
Abstract
Although post-traumatic stress disorder (PTSD) has been associated with worse cognitive outcomes after mild traumatic brain injury (TBI), its impact has not been evaluated after more severe TBI. This study aimed to determine whether PTSD symptoms are related to cognition after complicated mild, moderate, severe, and penetrating TBI. Service members (n = 137) with a history of complicated mild/moderate TBI (n = 64) or severe/penetrating TBI (n = 73) were prospectively enrolled from United States Military Treatment Facilities. Participants completed a neuropsychological assessment one year or more post-injury. Six neuropsychological composite scores and an overall test battery mean (OTBM) were considered. Participants were excluded if there was evidence of invalid responding. Hierarchical linear regressions were conducted evaluating neuropsychological performance. The interaction between TBI severity and PTSD Checklist-Civilian version total score was significant for processing speed (β = 0.208, p = 0.034) and delayed memory (β = 0.239, p = 0.021) and trended toward significance for immediate memory (β = 0.190, p = 0.057) and the OTBM (β = 0.181, p = 0.063). For each of these composite scores, the relationship between PTSD symptoms and cognition was stronger in the complicated mild/moderate TBI group than the severe/penetrating TBI group. Within the severe/penetrating TBI group, PTSD symptoms were unrelated to cognitive performance. In contrast, within the complicated mild/moderate TBI group, PTSD symptoms were significantly related to processing speed (R2Δ = 0.077, β = -0.280, p = 0.019), immediate memory (R2Δ = 0.197, β = -0.448, p < 0.001), delayed memory (R2Δ = 0.176, β = -0.423, p < 0.001), executive functioning (R2Δ = 0.100, β = -0.317, p = 0.008), and the OTBM (R2Δ = 0.162, β = -0.405, p < 0.001). The potential impact of PTSD symptoms on cognition, over and above the impact of brain injury alone, should be considered with service members and veterans with a history of complicated mild/moderate TBI. In addition, in research comparing cognitive outcomes between patients with histories of complicated-mild, moderate, severe, and/or penetrating TBI, it will be important to account for PTSD symptoms.
Introduction
Post-traumatic stress disorder (PTSD) and traumatic brain injury (TBI) are common consequences of recent military operations 1 –6 and are frequently comorbid in military samples. A recent meta-analysis revealed PTSD was present in 48.8% of service members and veterans (SMVs) who had sustained a military-related TBI. 7 Similarly, another recent meta-analysis concluded that SMVs with a history of TBI were more than four times more likely than those without TBI history to have a diagnosis of PTSD. 8
It has been well-established 9 –14 that PTSD symptoms explain the preponderance of the variance in self-reported outcomes after mild TBI, the most common severity of TBI. 6,15 For example, Hoge and associates 11 elegantly demonstrated that the strong relationship between mild TBI and post-concussion symptoms/physical health outcomes was dramatically attenuated after adjustment for PTSD.
There has also been a large amount of literature demonstrating that PTSD is associated with cognitive performance after mild TBI in military samples, 16 –23 although some studies have found this not to be the case. 24,25 Despite the strong evidence suggesting PTSD symptoms negatively impact cognition after mild TBI, to our knowledge, no studies have investigated the influence of PTSD symptoms on cognitive performance in complicated mild, moderate, severe, or penetrating TBI.
While it is possible that the relationship between PTSD symptoms and cognition after complicated mild, moderate, severe, and penetrating TBI is similar to that between PTSD symptoms and cognition after uncomplicated mild TBI, it is also possible that more severe brain damage amplifies the negative impact of PTSD (i.e., it may be that the more vulnerable brain is more susceptible to the negative impact of PTSD symptoms), or attenuates such a relationship (i.e., it may be that in the context of severe neurological insult, PTSD adds little to the clinical picture).
This study aimed to determine whether the presence of PTSD symptoms in individuals who sustained a complicated mild, moderate, severe, or penetrating TBI is related to worse cognitive performance. Based on the existing literature within mild TBI samples, it was hypothesized the PTSD symptoms would be inversely associated with cognitive performance within the overall sample. It was further hypothesized that when dividing the sample into two groups based on injury severity, PTSD symptoms would be negatively related to cognitive performance within each of these groups.
Methods
Participants
Participants were 137 U.S. military SMVs prospectively enrolled in the Defense and Veterans Brain Injury Center (DVBIC)/TBI Center of Excellence (TBICoE) 15-Year Longitudinal TBI Study. Participants were recruited and consented to the larger study via (a) community events, (b) inpatient wards, (c) outpatient clinics, or (d) intensive treatment programs at four Military Treatment Facilities. Participants were enrolled in the larger study if they were an active-duty service member or other Defense Enrollment Eligibility Reporting System-eligible (i.e., eligible to receive military benefits) veteran who provided informed consent to participate.
General exclusion criteria included: a lack of proficiency in conversational English, a history of significant neurological conditions (e.g., meningioma, pre-injury epilepsy, stroke, artery dissection, multiple sclerosis), a history of formal psychiatric diagnosis before the military that did not represent a response to isolated events (e.g., major depressive disorder was generally exclusionary, but not if it occurred after a family member's death and resolved), a history of psychotic disorder, personality disorder, or bipolar disorder diagnosed at any time. Participants with a diagnosis of attention deficit/hyperactivity disorder or learning disability in childhood or adulthood were only excluded in the event of pervasive impact on academic functioning (e.g., necessitating multiple years of special education and/or tutoring).
This research was approved by the Institutional Review Board of Walter Reed National Military Medical Center and in accordance with the guidelines of the Declaration of Helsinki.
For the purposes of this study, participants were selected from a larger sample of SMVs who had sustained a complicated mild, moderate, severe, or penetrating TBI at least 11 months before their study visit and had completed neuropsychological testing (n = 163). Patients were selected for inclusion in the final sample if they passed performance validity tests (PVTs) and symptom validity tests, described below. This resulted in a final sample of 137 participants divided into two groups: complicated mild/moderate TBI (n = 64) and severe/penetrating TBI (n = 73).
TBI evaluation and classification
Diagnosis and classification of TBI has been described in detail previously. 26 Briefly, a comprehensive interview including the Ohio State University TBI identification method and an extended semi-structured clinical interview was conducted and combined with medical records for classification of TBI severity by consensus during case conferencing. For this study, TBI severity was classified as follows:
(A) complicated mild TBI (mTBI) (n = 42): (1) Glasgow Coma Scale (GCS) score = 13–15, post-traumatic amnesia (PTA) <24 h, loss of consciousness (LOC) <30 min, and/or alteration of consciousness present, and (2) trauma-related intracranial abnormality on computed tomography or magnetic resonance imaging (MRI). (B) Moderate TBI (n = 22): LOC 30 min–24 h, PTA 1–7 days, and/or lowest reliable GCS score (e.g., not intubated/sedated/intoxicated) >30 min post-injury of 9–12. (C) Severe TBI (n = 30): LOC >24 h, PTA >7 days, and/or lowest reliable GCS score >30 min post-injury of <9. (D) Penetrating TBI (n = 43): a breach of the cranial vault and/or dura mater by an external object (e.g., bullet, shrapnel) and/or skull fragment (i.e., depressed skull fracture).
Penetrating TBI was confirmed with neuroimaging and/or surgical medical records. As part of the study, all participants underwent MRI, unless contraindicated.
Measures and procedure
Neuropsychological tests
Available index scores from the Wechsler Adult Intelligence Scale-IV (WAIS-IV) 27 and Wechsler Memory Scale-IV (WMS-IV) 28 were used, including Processing Speed (PSI: Coding and Symbol Search; Cronbach α = 0.833), Working Memory (WMI: Digit Span and Letter-Number Sequencing; Cronbach α = 0.847), and Perceptual Reasoning (PRI; Visual Puzzles and Block Design; Cronbach α = 0.790). The WMS-IV Index Scores included Immediate Memory (IMI: Logical Memory I, Visual Reproduction I and California Verbal Learning Test-II (CVLT-II) 29 Total Learning; Cronbach α = 0.684) and Delayed Memory (DMI: Logical Memory II, Visual Reproduction II, and CVLT-II Long Delay Free Recall; Cronbach α = 0.701).
An executive functioning composite standard score was also computed from WAIS-IV Similarities Scaled Score, and Trail Making Test 30 Part B Scaled Score, 31 Delis-Kaplan Executive Functioning System 32 Verbal Fluency Letter Fluency and Color Word Interference Test Inhibition Scaled Scores (Cronbach α = 0.671). An overall test battery mean (OTBM) was calculated from averaging these six indices together (Cronbach α = 0.902). The Test of Premorbid Functioning (TOPF) 33 predicted standard score was used as a proxy for pre-morbid intelligence.
Patients were also administered at least one stand-alone PVT (Medical Symptom Validity Test (MSVT), 34 Test of Memory Malingering (TOMM), 35 or Advanced Clinical Solutions Word Choice Test (WCT) 33 and multiple embedded measures of performance validity (WAIS-IV Reliable Digit Span, Logical Memory, and Visual Reproduction). Failure of either the stand-alone PVT and/or of at least two embedded measures resulted in exclusion from the neuropsychological analyses. For the WCT and all embedded measures, failure was defined as performance below the 10%ile. 33 For the MSVT, failure was defined by cutoffs in the manual. For the TOMM, failure on Trial 2 was defined by the cutoff in the manual, and failure on Trial 1 was defined using the cutoff recommended by Denning. 36
Self-report questionnaires
The PTSD Checklist-Civilian version (PCL-C), 37 Combat Exposure Scale (CES), 38 and Minnesota Multiphasic Personality Inventory-2nd Edition-Restructured Format (MMPI-2-RF) 39 were also administered. The PCL-C total score was used to quantify PTSD symptoms. In addition, responses to individual items were mapped onto Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) 40 criteria for PTSD. Individuals who satisfied criteria based on mild or greater endorsement of the requisite symptoms were classified as PTSD-Present. Participants were excluded from the sample if MMPI-2-RF was considered invalid (i.e., VRIN ≥80T, TRIN ≥80T, F-r = 120T, or Fp-r ≥100T), or if they skipped too many items (i.e., Cannot Say >14)
Statistical analyses
Descriptive statistics and group comparisons were conducted with analyses of variance (ANOVAs), chi-square, and Mann-Whitney tests. Post hoc comparisons were conducted with Fisher least significant difference, chi-square, and Kruskal-Wallis. Effect sizes were computed with Cohen d for continuous variables. Hierarchical linear regression predicting performance in the six cognitive domains and OTBM were run in the overall sample
Pearson and Spearman correlations were calculated to investigate the relationship between demographics (i.e., age, sex, race, time since injury), TOPF predicted standard scores (SS), MMPI-2-RF depressive symptoms (from the Low Positive Emotions [RC2] Scale), and cognitive scores. Based on the identification of differences between the injury groups and correlations with outcome measures, TOPF predicted SS was centered and entered as a covariate in the first step of all models, time since injury was entered as a covariate in all models, and race (White vs. Non-white) was entered as a covariate in the models investigating PRI, IMI, DMI, and OTBM.
The TBI severity (complicated mild/moderate vs. severe/penetrating), centered PCL-C total score, and the interaction between TBI severity and centered PCL-C total score were entered in the second step. Additional hierarchical linear regressions were run within each of the two TBI severity groups, with the same covariates mentioned above entered in step 1, and centered PCL-C total score entered in step 2. For these two additional sets of hierarchical regressions, the Benjamini-Hochberg False Discovery Rate 41 correction was used to keep the false discovery rate at 0.05, correcting separately within each TBI group (i.e., correcting for seven analyses within the complicated mild/moderate TBI group and seven analyses within the severe/penetrating TBI group).
Results
Demographics, military characteristics, and injury characteristics are presented for each TBI group in Table 1. Time since injury was significantly greater in the severe/penetrating TBI group (M = 103.4 months; standard deviation [SD] = 55.2) compared with the complicated mild/moderate TBI group (M = 63.8; SD = 52.1, p < 0.001, d = 0.74). Combat exposure was also significantly higher in the severe/penetrating TBI group (Mean CES = 19.6; SD = 9.3) compared with the complicated mild/moderate TBI group (M = 14.9, SD = 12.9, p = 0.015, d = 0.43).
Demographics, Military, and Injury Characteristics by Traumatic Brain Injury Group
TBI, traumatic brain injury; SD, standard deviation; PCL-C, Post-traumatic Stress Disorder Checklist-Civilian Version, Minnesota Multiphasic Personality Inventory-2nd Edition-Restructured Format (MMPI-2-RF; TOPF, Test of Premorbid Functioning; IQR, interquartile range; PTA, post-traumatic amnesia; LOC, loss of consciousness; RA, retrograde amnesia; PTSD, post-traumatic stress disorder.
Service branch was also significantly different between the groups, with the severe/penetrating TBI group more likely to be in the Marines (20.5%) than the complicated mild and moderate TBI group (4.7%, p = 0.010). The severe/penetrating TBI group was more likely to have LOC and/or PTA compared with the complicated mild/moderate TBI group, but less likely to have retrograde amnesia (RA). When present, PTA, LOC, and RA, tended to be longer for those with severe/penetrating TBI than those with complicated mild/moderate TBI. There were no other differences in demographics, military, or injury characteristics between the two groups. Neuropsychological test scores, by TBI severity and PTSD status, are presented in Figure 1.
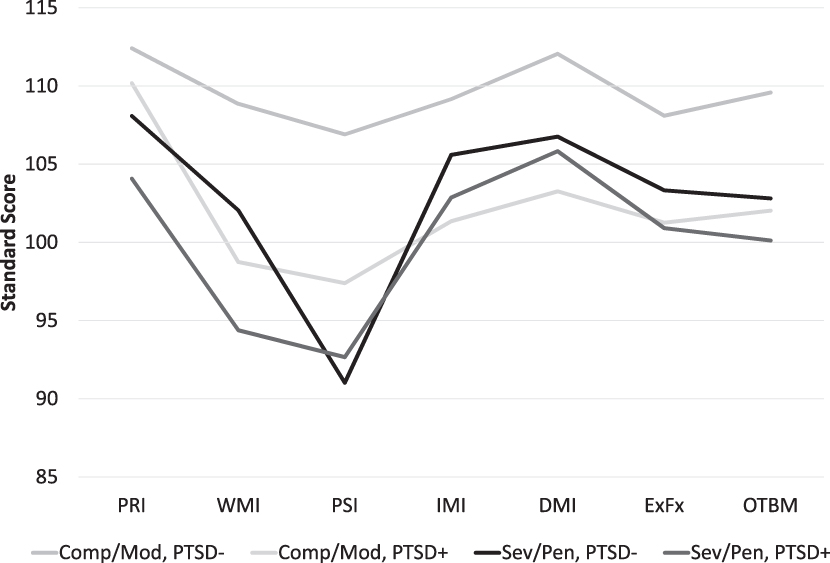
Cognitive domain scores by traumatic brain injury (TBI) severity and post-traumatic stress disorter (PTSD) status based on mild or greater endorsement of Diagnostic and Statistical Manual of Mental Disorders, 4th edition, criteria. Comp/Mod, complicated mild/moderate TBI; DMI, Delayed Memory Index, EFI, Executive Functioning Index, IMI, Immediate Memory Index; OTBM, Overall Test Battery Mean; PRI, Perceptual Reasoning Index; PSI, Processing Speed Index; Sev/Pen, severe/penetrating TBI; WMI, Working Memory Index.
Hierarchical linear regressions conducted within the overall sample indicated that the interaction between TBI severity and PCL-C was significant for processing speed (β = 0.208, p = 0.034) and delayed memory (β = 0.239, p = 0.021) and trended toward significance for immediate memory (β = 0.190, p = 0.057) and the OTBM (β = 0.181, p = 0.063). For each of these composite scores, the relationship between PTSD symptoms and cognition was stronger in the complicated mild/moderate TBI group than the severe/penetrating TBI group (Fig. 2). Executive functioning was significantly related to PCL-C total score (β = -0.252, p = 0.017) only, while working memory was predicted by TBI severity (β = -0.228, p = 0.011) and trended toward an association with PCL-C total score (β = -0.211, p = 0.055), but was not related to the interaction of TBI severity and PCL-C total score (Table 2).
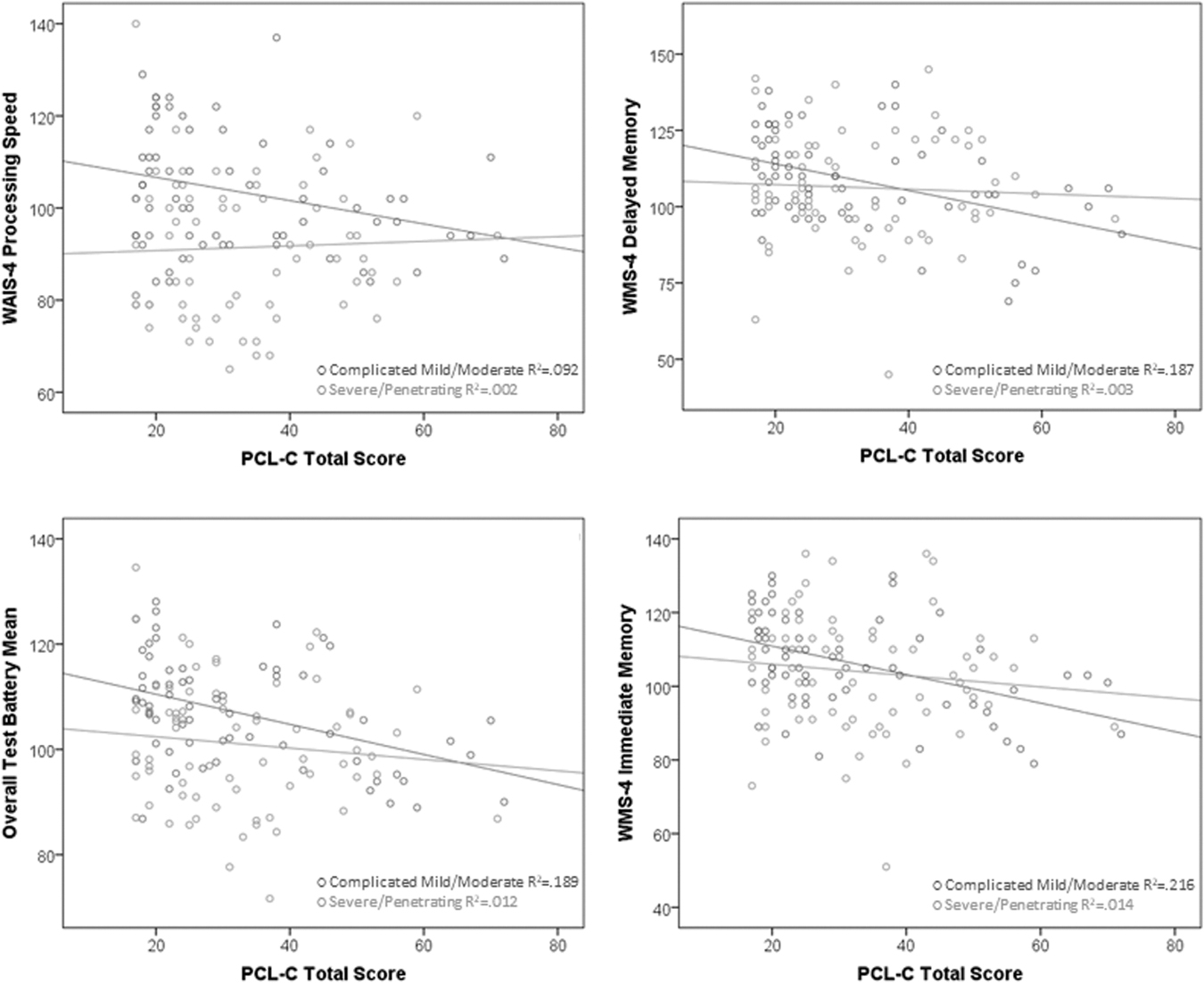
Group by post-traumatic stress disorder (PTSD) symptoms on cognition scatterplots for processing speed, delayed memory, overall test battery mean, and immediate memory. PCL-C, Post-traumatic Stress Disorder Checklist-Civilian Version; WAIS-4, Wechsler Adult Intelligence Scale-IV; WMS-4, Wechsler Memory Scale-IV.
Summary of Regression Model Investigating How Traumatic Brain Injury Severity and Post-Traumatic Stress Disorder Checklist-Civilian Version Total Score Relate to Cognitive Performance within the Entire Traumatic Brain Injury Sample
TBI, traumatic brain injury; PCL-C, Post-traumatic Stress Disorder Checklist-Civilian Version; OTBM, overall test battery mean.
When examining the relationship between PCL-C total score and neurocognitive outcomes within each injury severity group separately, there were no significant relationships between PCL-C total score and performance on individual cognitive domains in the severe/penetrating TBI group (βs: -0.166 to 0.115, ps > 0.15) (Table 3). Within the complicated mild and moderate TBI group, PCL-C total score was significantly related to processing speed (R 2 Δ = 0.077, β = -0.280, p = 0.019), immediate memory (R 2 Δ = 0.197, β = -0.448, p < 0.001), delayed memory (R 2 Δ = 0.176, β = -0.423, p < 0.001), executive functioning (R 2 Δ = 0.100, β = -0.317, p = 0.008), and OTBM (R 2 Δ = 0.162, β = -0.405, p < 0.001). All of these survived the Benjamini-Hochberg False Discovery Rate correction.
Standardized Regression Coefficients and Percent Variance Explained in Each Cognitive Domain by Post-Traumatic Stress Disorder Checklist-Civilian Version Total Score for Each Traumatic Brain Injury Group
TBI, traumatic brain injury; PCL-C, Post-traumatic Stress Disorder Checklist-Civilian Version; OTBM, overall test battery mean,
Although not statistically significant, PCL-C total score also trended toward a significant relationship with perceptual reasoning (R 2 Δ = 0.033, β = -0.183, p = 0.093) and working memory (R 2 Δ = 0.054, β = -0.234, p = 0.064).
Discussion
This study demonstrated that PTSD symptom severity was significantly related to neuropsychological performance in SMVs with complicated mild, moderate, severe, and penetrating TBI. This relationship appeared to be most strongly driven by the complicated mild/moderate TBI group, because when looking at the two severity groups separately, PTSD symptoms were significantly related to neuropsychological performance within the complicated mild/moderate TBI group, but not the severe/penetrating TBI group.
Within the complicated mild/moderate TBI group, PTSD symptoms were related to decreased processing speed, immediate and delayed memory, executive functioning, and OTBM, with PTSD symptoms uniquely explaining roughly 8–20% of the variance on each of these indices. These findings are largely consistent with previous research showing that PTSD symptoms are related to worse performance on tests of processing speed, 17 –19,23,42 learning and memory, 18,19,21,42,43 and executive functioning 16 –19,23,44 after mTBI.
Taken together, the available literature suggests that PTSD symptoms are important to consider when assessing cognitive outcomes in patients with mild or moderate TBI. In addition, when comparing individuals across different injury severities (e.g., moderate vs. severe TBI), PTSD will be an important factor, because in our sample, individuals with complicated mild/moderate TBI who met DSM-IV criteria for PTSD based on mild endorsement of symptoms often performed at or below the level of patients with severe or penetrating TBI.
That PTSD symptoms were associated with cognition in complicated mild/moderate TBI will be especially important to keep in mind with older patients. Both PTSD 45,46 and TBI 47 –49 have been associated with increased risk of cognitive decline and dementia. The PTSD may increase risk of dementia through cerebrovascular mechanisms, because it also has been associated with coronary artery disease and atherosclerosis. 50 –52 It will be important to longitudinally study individuals with and without each of these risk factors to better understand the mechanisms driving cognitive decline and dementia to best target interventions.
Notably, the relationship between PTSD symptoms and cognitive performance was much weaker in the severe/penetrating TBI group. This suggests that the cognitive impairments secondary to a severe or penetrating TBI are less likely to be negatively impacted by PTSD symptoms. Interestingly, combat exposure was higher in the severe/penetrating TBI group, but PTSD symptoms did not differ between the two groups. It is possible that the severe/penetrating TBI group was more likely to have anosognosia, making some individuals in this group less likely to endorse PTSD symptoms. It seems possible that the most severe cases may experience both anosognosia and severe cognitive impairment, which may have attenuated any relationship between PTSD symptoms and cognition in the severe/penetrating TBI group.
Alternatively, the more severe brain injury may in some way be protective from exacerbation of potential PTSD symptoms, which could similarly reduce the strength of the relationship between PTSD symptoms and cognitive performance in the severe/penetrating TBI group. Perhaps, as some have argued, reduced memory of the injury event is protective against PTSD, because it reduces ability to re-experience symptoms. 53 –56 Most data, however, supports that PTSD can occur even if the memory of the traumatic event is disrupted. 57 –60
Focal damage to the brain itself can modify PTSD expression. In Vietnam veterans with a history of penetrating TBI, left-sided cortical and/or limbic system damage was associated with increased anxiety, 61 yet, none of the 15 patients in the study with amygdala damage had a lifetime history of PTSD, and damage to the left or right ventromedial pre-frontal cortex (vmPFC) was associated with reduced likelihood of lifetime PTSD. 62 The latter finding is particularly surprising given the theory that the vmPFC provides inhibition to the hyperactivity of the amygdala in PTSD, and damage to the vmPFC should thereby reduce inhibition and increase PTSD occurrence. Nonetheless, damage to specific brain areas can reduce the expression (and reporting) of PTSD symptoms.
It is important to consider that PTSD can develop secondary to events entirely unrelated to the event causing the TBI. We did not assess whether PTSD symptoms were related to the injury event that caused the TBI, to events before or after the TBI, or to a combination of these events.
Other limitations include that the participants in this study are likely not representative of all SMVs with complicated mild, moderate, severe, and penetrating TBI, because this study required the participants to travel and participate in multiple days of in-person assessments, precluding those with the most severe impairments from participating. This, in particular, may have impacted findings in the severe/penetrating TBI group. Similarly, individuals with the most severe PTSD symptoms would have been less likely to participate in this study. In addition, PTSD symptoms were assessed with a self-report measure, rather than a clinician administered interview.
Despite these limitations, our results suggest that the impact of PTSD symptoms should be considered as a significant confounding factor that may, perhaps temporarily, exacerbate cognitive decline from neurological insult after complicated mild to moderate TBI, consistent with the mild TBI literature. In addition, in research comparing cognitive outcomes between patients with histories of complicated-mild, moderate, severe, and/or penetrating TBI, it will be important to account for PTSD symptoms. Although PTSD symptoms were not significantly related to neuropsychological performance within the severe/penetrating TBI groups, future research is needed to confirm these findings and evaluate any potential impact of PTSD symptomatology longitudinally.
Conclusions
Post-traumatic stress symptoms were significantly related to neuropsychological performance in our overall sample of SMVs with complicated mild and more severe TBI. When participants were separated by injury severity, PTSD symptomology was significantly related to cognitive performance only within the complicated mild/moderate TBI group, and not the severe/penetrating TBI group. As with patients with a history of uncomplicated mild TBI, PTSD symptoms should be considered when evaluating patients with a history of complicated mild to moderate TBI.
Footnotes
Acknowledgments
The views expressed in this manuscript are those of the authors and do not necessarily represent the official policy or position of the Defense Health Agency, Department of Defense, or any other U.S. government agency. This study is part of the larger Defense and Veterans Brain Injury Center (DVBIC) 15-Year Longitudinal TBI Study designed to respond to a Congressional mandate (Sec721 NDAA FY2007). The authors would like to thank the service members and veterans for their time and commitment to participating in the research. The authors would also like to acknowledge the efforts of the larger team of research coordinators, research associates, research assistants, program managers, and senior management who contribute to the DVBIC 15-Year Longitudinal TBI Study.
Authors' Contributions
Sara Lippa designed and conceptualized the study, collected data, analyzed the data, drafted the manuscript for intellectual content, approved the final version of the manuscript, and agrees to be accountable for all aspects of the work; Louis French, Tracey Brickell, Angela Driscoll, Megan Glazer, Corie Tippet, Jamie Sullivan, and Rael Lange collected data, revised the manuscript for intellectual content, approved the final version of the manuscript, and agree to be accountable for all aspects of the work.
Funding Information
This work was prepared under Contract HT0014-19-C-0004 with DHA Contracting Office (CO-NCR) HT0014 and, therefore, is defined as U.S. Government work under Title 17 U.S.C.§101. Per Title 17 U.S.C.§105, copyright protection is not available for any work of the U.S. Government. For more information, please contact dha.TBICOEinfo@mail.mil.
Author Disclosure Statement
No competing financial interests exist.