
Abstract
Concussion is a major health concern, making it critical to identify factors that influence risk and resilience. The salience network (SN) likely plays a key role in concussion risk, given its roles in orienting attention, functional adaptability, and interoceptive awareness. The SN's functions are thought to be mediated through causal control of other networks, including the default mode network (DMN) and executive control network (ECN). It was therefore hypothesized that the SN of at-risk individuals would have altered functional and structural connectivity with the DMN and ECN. For this prospective study, 167 university athletes had baseline clinical assessments and magnetic resonance imaging scans and were monitored for the rest of their varsity career, with any concussions recorded. Athletes concussed in the same season as imaging (CSS; n = 17) and those concussed in later seasons (CLS; n = 15) were matched to controls that were not concussed after imaging. Functional connectivity and white matter fractional anisotropy (FA) were compared between concussed and control groups. Prior to injury, CSS athletes had significantly elevated total symptom severity scores, elevated SN-DMN functional connectivity and reduced FA of connecting white matter tracts, whereas CLS athletes showed no significant clinical or imaging effects. These findings provide new insights into the neurobiology of concussion risk and resilience, as indices of SN-DMN network connectivity are associated with short-term but not long-term concussion risk.
Introduction
Concussion is a major health concern in sport and recreation, with an estimated 3.8 million cases annually in North America. 1 There is also growing recognition that concussion can have long-term consequences, including emotional and cognitive disturbances 2,3 and increased neurodegenerative risk. 4 -6 The identification of factors that determine an individual's risk of concussive injury is important, as it may assist in developing strategies to mitigate this risk. At present, we cannot answer one of the major conundrums of sport-related concussion: For athletes playing the same sport, with similar demographic and clinical profiles, why do some go on to sustain a concussion and others play an entire career without a single concussive injury?
Research examining concussion risk has mainly focused on practical issues such as the impact of new rules and regulations. 7 To date, this has not been well examined from a neurobiological perspective, which is major knowledge gap. To avoid concussive blows in sport, the brain must quickly integrate sensory information, select a response and execute the appropriate action, while filtering out irrelevant information; this requires interaction between brain networks subserving different domains. 8,9 If a blow occurs, whether or not it results in concussion may also depend on pre-injury network interactions, with more adaptable networks better compensating for physiological perturbations. 10,11 In addition, a key component of concussion diagnosis is symptom reporting, and the detection of post-concussion symptoms likely depends on interactions between distributed brain networks. 12 It is presently unclear, however, whether there are consistent pre-injury differences in the network connectivity of concussion-prone and concussion-resilient athletes.
The salience network (SN) is a promising target for investigating the neural correlates of concussion risk. Anchored by nodes in the anterior insula and dorsal anterior cingulate, it has dense functional and structural connectivity and is implicated in a diverse array of sensory, affective, and cognitive processes. 13 It plays a key role in orienting towards stimuli that threaten homeostasis, assigning salience in the presence of ambiguity, and monitoring internal bodily state (i.e., interoception). 14,15 This underscores the potential importance of the SN in the components of concussion risk, including injury avoidance, functional adaptability and symptom self-appraisal. The SN's role is achieved by feeding information to other networks. In particular, it exerts causal control over the default mode network (DMN), which is implicated in internally-directed cognition (e.g., self-referential thought and memory consolidation), and the executive control network (ECN), which is implicated in externally-directed cognition (e.g., working memory and decision making). 16,17 Hence, SN-mediated toggling between the DMN and the ECN is thought to modulate attentional orienting, adaptability, and interoception. 18,19 The functional and structural connections of these networks may therefore distinguish concussion-prone individuals from those who are concussion-resilient.
The present study examined this issue using a prospective design. A large cohort of university athletes had magnetic resonance imaging (MRI), including resting-state functional MRI (rs-fMRI) and diffusion tensor imaging (DTI). The athletes were then monitored for the remainder of their careers and any concussions were recorded. Athletes concussed in the same season as imaging (CSS) and those concussed in later seasons (CLS) were compared with matched controls that were not concussed afterwards (NCA) during the remainder of their varsity career. It was hypothesized that CSS and CLS groups would have altered pre-injury functional connectivity of the SN to the DMN and ECN, indicating associations with both short-term and long-term concussion risk. It was also hypothesized that CSS and CLS groups would have altered pre-injury fractional anisotropy (FA) in fiber tracts connecting networks, indicating a structural basis for the altered functional connectivity.
Methods
Study participants
One hundred sixty-seven university athletes were imaged for this study, recruited consecutively from teams at a single institution through the academic sport medicine clinic, during mandatory pre-season baseline clinical assessments. Athlete recruitment and data collection were carried out between October 2014 and March 2019. Participants had no history of neurological or psychiatric diseases or sensory/motor impairments, based on self-report during physician assessment, and were not recovering from a prior concussion at the time of imaging. The study was carried out in accordance with the Canadian Tri-Council Policy Statement 2 and approval of University of Toronto and St. Michael's Hospital research ethics boards, with participants giving free and written informed consent.
MRI
Athletes were imaged using a 3 Tesla MRI system (Magnetom Skyra, Siemens Healthineers, Erlangen, Germany) with standard 20-channel head coil. Imaging and preprocessing sequences have been previously published 20 -22 and details are in the Supplementary Material, Supplementary Appendix SA1. Anatomical imaging included Magnetization Prepared Rapid Acquisition Gradient Echo (MPRAGE; sagittal acquisition, 0.9 × 0.9 mm in-plane, 0.9 mm slice thickness), fluid attenuated inversion recovery imaging, and susceptibility-weighted imaging. The scans were inspected by an MRI technologist and later reviewed by a neuroradiologist, to verify that participants had no structural abnormalities. Resting brain function was evaluated using rs-fMRI (3.25 × 3.25.4.5 mm voxels, 2000 msec repetition time, 6.5 min acquisition) and functional networks obtained from a template-based procedure, outlined in the “Functional connectivity” section below. White matter was evaluated using DTI (2 × 2 × 2 mm voxels, 30 diffusion encoding directions, b = 700 sec/mm2) and FA was analyzed within white matter tracts, as described in the “White matter microstructure” section below.
Demographic and clinical data
Participant demographics were recorded, including age, sex, history of concussion (HOC), participation in collision sports (i.e., having routine body-to-body contact) 23 and year of varsity eligibility. Participants completed baseline testing using C3 Logix, an iPad-based application that assesses symptoms, cognition (Standardized Assessment of Concussion), and balance (Modified Balance Error Scoring System) aligned with the most recent Concussion in Sport Group's Sport Concussion Assessment Tool (SCAT3/5). Per evolving guidelines, 68/167 athletes were evaluated with SCAT3 and 99/167 were evaluated with SCAT5. For symptoms and balance, analyses are based on the full sample, whereas analysis of cognitive scores are restricted to SCAT5, which used 10-word lists. C3 Logix also includes computerized neurocognitive testing, with good test-retest reliability and validity. 24,25 The administered tests included Simple and Choice Reaction Time, Processing Speed, along with Trail-Making Tests A and B, which were assessed for 121/167 athletes.
Whole–group demographic and clinical summary statistics are reported, along with summary statistics for the NCA, CSS and CLS groups. The mean difference in demographic and clinical variables was calculated per concussed group, relative to the NCA cohort. Two-sample bootstrapping was conducted on the mean differences (1000 iterations), obtaining non-parametric two-tailed percentile 95% confidence intervals (95% CIs), bootstrap ratios (BSRs; standardized effect size, calculated as the mean/standard error) and p values as the proportion of resamples that do not overlap zero, with significance determined at a false discovery rate (FDR) of 0.05. To control for demographic heterogeneity, CSS and CLS athletes also were matched to individual NCA athletes. For each concussed athlete, a matched control was obtained by restricting the pool of NCA athletes to the same sport, sex, and HOC status, based on evidence that these variables significantly affect athlete brain function. 26 -28 From this pool, the control nearest in eligibility year was chosen, to ensure comparable sport exposure. The difference in mean clinical values was obtained for CSS and CLS groups, relative to their matched NCA subgroups. Paired-measures bootstrap resampling was conducted (1000 iterations), where resampling units consisted of a concussed athlete and matched control. This produced 95% CIs, BSRs, and p values evaluated at an FDR of 0.05.
Functional connectivity
Functional connectivity was assessed using the parcellation of Shirer and colleagues, 29 which subdivides the brain into 14 networks. The analyses focused on whole-network connectivity for the SN (combining anterior and posterior network templates), DMN (combining dorsal and ventral network templates), and ECN (combining left and right network templates). To account for cohort-specific variations in functional topology, voxel weights producing the most homogeneous network time series were computed at the group level. This was achieved by fitting a three-component Gaussian mixture model of type #2 as in Churchill and colleagues, 30 with fixed clusters given by template masks. To avoid over-fitting, this was done on a “training” sample of 35 NCA athletes that were not selected as matched controls. This sample was comparable in size to the concussed cohort and demographically comparable to both the concussed and complete samples (20.8 ± 1.8 years, 16/35 female (45%), 15/35 with HOC (43%); p ≥ 0.116), with representation from all sports in the concussed cohort. For each participant, the three network timeseries were then obtained as weighted averages of the voxel timeseries within each template, and inter-network connectivity was measured as the Pearson correlation between timeseries.
To evaluate the first hypothesis, connectivity of the SN to the ECN and DMN was assessed for both CSS and CLS groups, relative to their matched NCA subgroups. Group differences in whole–network connectivity were evaluated with paired-measures bootstrap analyses, producing mean differences, 95% CIs, BSRs, and p values evaluated at an FDR of 0.05. For network pairs showing global effects, secondary analyses visualized the spatial pattern of affected brain regions. This was achieved by measuring the functional connectivity of individual voxel within network 1 to the whole-network timeseries of network 2, and vice versa. Group differences in voxel-wise connectivity were assessed via paired-measures bootstrap analyses, and BSR values were plotted after thresholding at |BSR| > 2 (approximately p < 0.05, uncorrected).
White matter microstructure
White matter diffusivity was assessed for tracts connecting significantly affected networks. First, tracts were mapped between significant network pairs identified in the rs-fMRI analyses. To avoid over-fitting, this was conducted on the same “training” sample of 35 NCA athletes in the rs-fMRI analysis, which were not selected as matched controls. For this sample, FSL bedpostx calculated the diffusion parameter distributions at each voxel and probtrackx generated tract-following samples (5000 samples, 0.2 curvature threshold, modified Euler streamlining, 0.1 mm step length, distance correction), using the network masks as seed and target points. Tractographic maps were warped into Montreal Neurological Institute (MNI) space and binarized at the 95th percentile, then averaged to obtain a probabilistic group map. The map was thresholded to include voxels identified for the majority of athletes in the training sample (i.e., p ≥ 0.50).
To evaluate the second hypothesis, FA values for CSS and CLS groups were compared with matched NCA subgroups. Group difference in whole–tract FA were evaluated with paired-measures bootstrap analyses, producing mean differences, 95% CIs, BSRs, and p values. Secondary analysis visualized the spatial pattern of effects within white matter tracts. Group differences in voxel-wise FA were assessed via paired-measures bootstrap analyses, and BSR values were plotted after thresholding at |BSR| > 2 (approximately p < 0.05, uncorrected).
Results
Clinical and demographic data
Table 1 summarizes demographic data. From the initial sample of 167 athletes, 32 were subsequently concussed, including 17 in the same season (CSS) and 15 in later seasons (CLS). A remaining 133 athletes were not concussed afterwards (NCA), from which subgroups of 17 and 15 athletes were matched to CSS and CLS groups. Comparing demographic and clinical data of CSS and CLS groups to the full NCA group, there were no significant differences at an FDR of 0.05. At uncorrected threshold p < 0.05, CLS athletes tended to be imaged earlier than NCA athletes (mean and 95% CI: -0.6, [-1.2, 0.0] years, BSR = -2.06, p = 0.044), but effects for age, sex, HOC, collision sport participation, and eligibility year did not reach this threshold (|BSR|
Demographic and Clinical Assessment Data
Age is reported as the mean ± standard deviation, and all other distributions are summarized by the median and interquartile range (Q1, Q3). Standard clinical scales include Total severity (i.e., summing all symptom severity scores), Total symptoms (i.e., counting all symptoms with non-zero severity scores), Standardized Assessment of Concussion total score (SAC total) and Modified Balance Error Scoring System total errors (M-BESS errors). Neurocognitive test scores include Simple and Choice Reaction Time (RT), Processing Speed, and Trail-Making Test (TMT) A and B completion times.
For the subset of athletes with history of concussion.
The SAC scores are based on the subset of 99/167 athletes that had Sport Concussion Assessment Tool 5 administered
The C3logix neurocognitive test data were collected for 121/167 athletes
Comparison of Athletes Concussed Same Season (CSS) to Their Matched Control Subgroups, Drawn from the Not Concussed Afterwards (NCA) Cohort
For neurocognitive tests, there were insufficient samples where both CSS and matched NCA athletes had Sport Concussion Assessment Tool 5 data (all with n ≤ 7), hence these group differences were not analyzed statistically.
BSR, bootstrap ratio; SAC, Standardized Assessment of Concussion; M-BESS, Modified Balance Error Scoring System; RT, reaction time; TMT, Trail-Making Test.
Comparison of Athletes Concussed Later Season (CLS) to Their Matched Control Subgroups, Drawn from the Not Concussed Afterwards (NCA) Cohort
For neurocognitive tests, there were insufficient samples where both CLS and matched NCA athletes had SCAT5 data (all with n ≤ 7), hence these group differences were not analyzed statistically.
BSR, bootstrap ratio; SAC, Standardized Assessment of Concussion; M-BESS, Modified Balance Error Scoring System; RT, reaction time; TMT, Trail-Making Test.
Functional connectivity data
Figure 1 compares the whole–network connectivity of CSS and CLS groups to matched NCA subgroups, for the functional networks in Figure 1A. For the SN-DMN connection (Fig. 1B), CSS athletes had elevated mean connectivity relative to matched controls (mean and 95% CI: 0.165, [0.071, 0.277], BSR = 3.13, p < 0.001) but effects for CLS athletes were nonsignificant (-0.01, [-0.235, 0.226], BSR = -0.05, p = 0.979). These results did not depend on cohort matching, as CSS athletes were also significantly elevated relative to the full NCA cohort (0.100, [0.005, 0.192], BSR = 2.13, p = 0.033) but CLS athletes were not (0.008, [-0.128, 0.137], BSR = 0.11, p = 0.900). For the SN-ECN connection (Fig. 1C), effects were nonsignificant for both CSS athletes (0.089, [-0.028, 0.211], BSR = 1.45, p = 0.142) and CLS athletes (0.029, [-0.154, 0.222], BSR = 0.31, p = 0.742). The differences remained nonsignificant when compared with the full NCA cohort, for both CSS athletes (0.055, [-0.016, 0.125], BSR = 1.49, p = 0.146) and CLS athletes (0.030, [-0.080, 0.146], BSR = 0.53, p = 0.608). Figure 2 displays regional analyses of SN-DMN connectivity, comparing CSS athletes with matched controls. For the SN, connectivity increases were spatially limited, with supra-threshold effects in bilateral ventral insula and right anterior insula, along with the left middle frontal gyrus and medial superior frontal cortex. For the DMN, connectivity increases were more extensive, with greatest effects in the ventral anterior cingulate and smaller effects in the ventromedial prefrontal cortex, posterior cingulate and left angular gyrus.
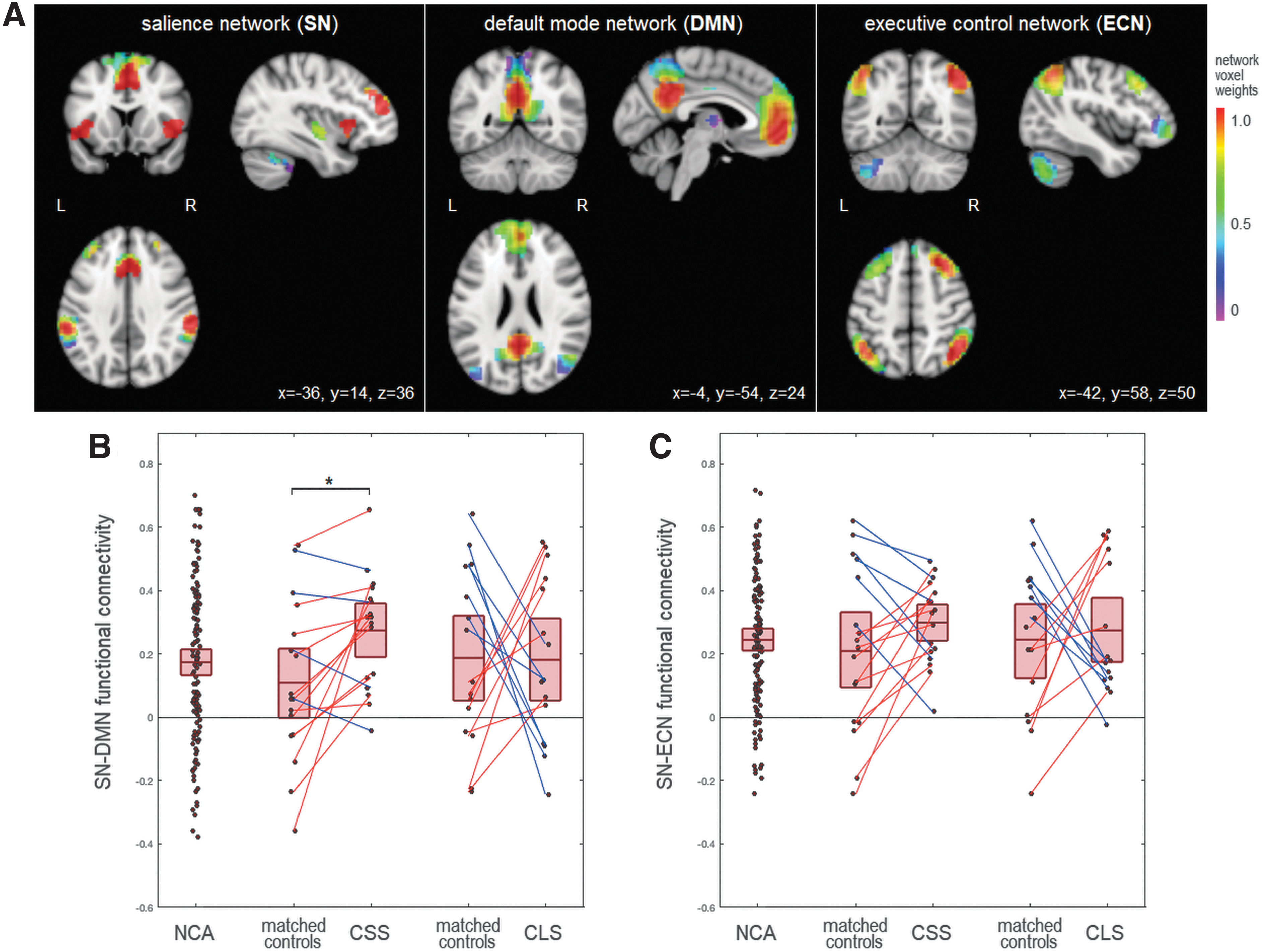
Global between-network functional connectivity and concussion risk.

Regional between-network functional connectivity and concussion risk, for the significant SN-DMN connection of athletes concussed same season (CSS) shown in Figure 1. Maps depict bootstrap ratio (BSR) values reflecting z-distributed standardized effect sizes of the difference between CSS athletes and their matched controls, drawn from the not concussed afterwards (NCA) cohort, thresholded at |BSR| > 2 (approximately p < 0.05 uncorrected). The Montreal Neurological Institute (MNI) space coordinates of the axial slices are listed on the bottom of the figure. Color image is available online.
White matter microstructure data
Figure 3 compares the whole-tract FA of CSS and CLS groups to matched NCA subgroups, for the bilateral tracts connecting nodes of the SN and DMN in Figure 3A. Within these regions (Fig. 3B), CSS athletes had significantly reduced FA relative to matched controls (mean and 95% CI: 1.12 × 10−2, [-2.02, -0.14] × 10−2, BSR = -2.31, p = 0.022), but effects for CLS athletes were nonsignificant (-0.81 × 10−2 [-2.77, 0.10] × 10−2, BSR = -1.71, p = 0.075). These effects depended on cohort matching, as CSS athletes did not differ significantly from the full NCA cohort (-0.35 × 10-2, [-0.92, 0.20] × 10-2, BSR = -1.23, p = 0.217), nor did CLS athletes (-0.45 × 10-2, [-1.18, 0.26] × 10-2, BSR = -1.22, p = 0.215). Figure 4 displays regional analyses of FA in white matter tracts connecting SN and DMN networks, comparing CSS athletes to matched controls. The most extensive reductions in FA were seen in the genu of the corpus callosum and the cingulum, with sparser effects in the body of the corpus callosum and posterior corona radiata.
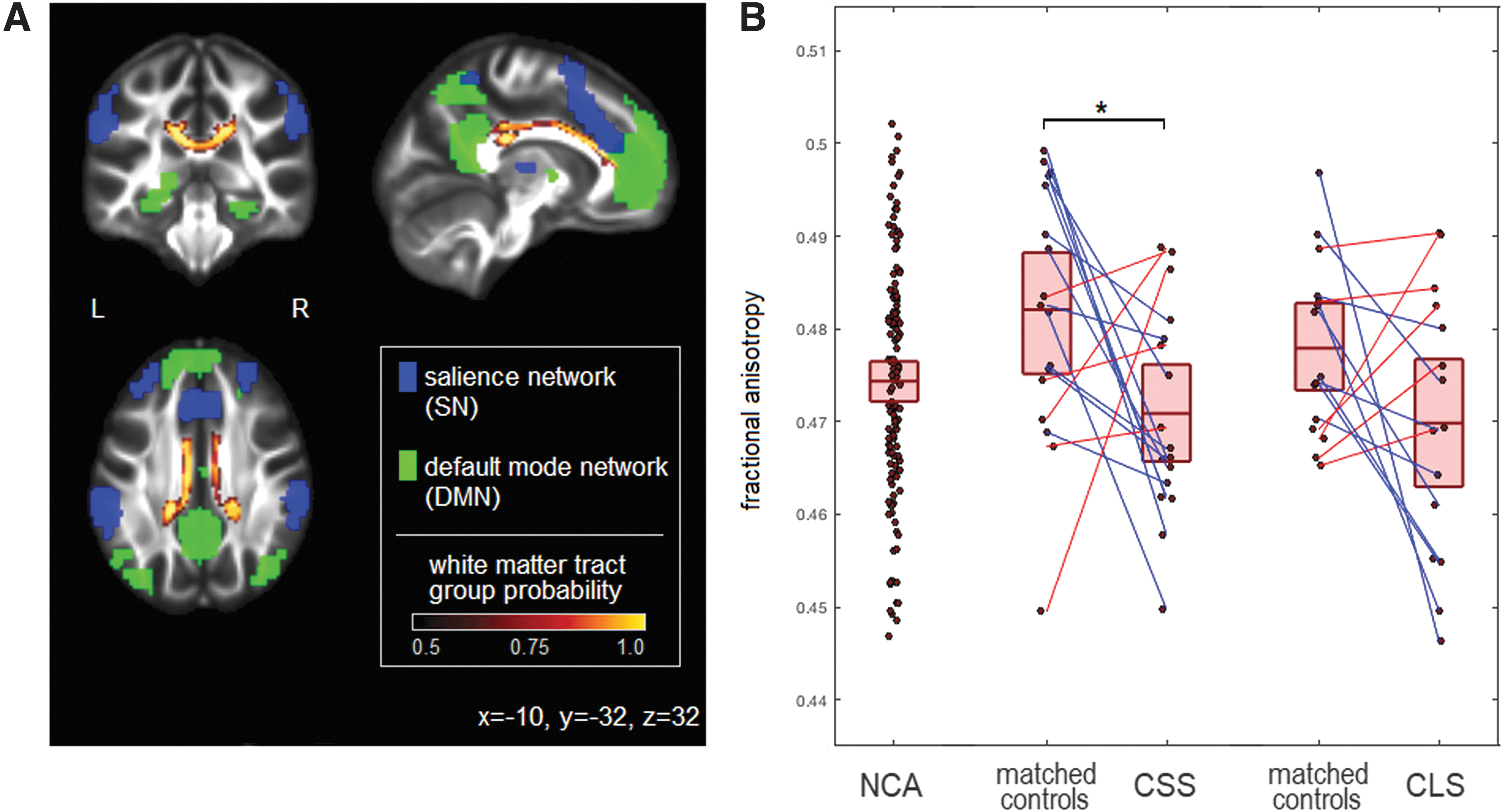
Global between-network white matter microstructure and concussion risk.

Regional between-network white matter microstructure and concussion risk, for the significant SN-DMN connection of athletes concussed same season (CSS), shown in Figure 3. Maps depict bootstrap ratio (BSR) values reflecting z-distributed standardized effect sizes of the difference between CSS athletes and their matched controls, drawn from the not concussed afterwards (NCA) cohort, thresholded at |BSR| > 2 (approximately p < 0.05 uncorrected). The Montreal Neurological Institute (MNI) space coordinates of the axial slices are listed on the bottom of the figure. Color image is available online.
Discussion
Concussion is a significant health concern, with evidence of acute and long-term effects on brain health. At present, however, little is known about the neurobiological factors that underlie concussion risk and resilience. The present study addressed this gap by prospectively imaging a cohort of university athletes and comparing those who were later concussed with those who were not subsequently injured. These data were used to probe the relationship of the SN with concussion risk, given its role in orienting attention, functional adaptability, and interoception. 14,15 The key finding was that same-season injury was associated with heightened pre-injury symptom severity, elevated SN-DMN functional connectivity and reduced FA of connecting white matter tracts. By contrast, concussion in later seasons showed no significant associations with clinical indices or with SN connectivity.
The fMRI results partially supported the primary study hypothesis. Although significant associations with concussion risk were identified, they were limited to SN-DMN connectivity of CSS athletes, with no significant effects for CLS athletes; in addition, no significant SN-ECN effects were identified for either cohort. These results suggest that elevated SN-DMN functional connectivity is related to short-term injury risk. Although cognitive interpretations remain speculative, given the SN's role in toggling internal and external states 19 and the DMN's role in internally-directed cognition, 31 the SN-DMN connectivity of at-risk athletes may reflect a predisposition for orienting towards internal stimuli. This is bolstered by voxel-wise analyses showing effects in anterior insular and cingulate cortices, which have roles in interoception and self-monitoring. 32,33 A tendency towards internally-directed cognition is congruent with the proposed mechanisms of risk, as it would affect athletes' ability to anticipate blows, adapt functionally following a blow, and self-monitor for symptoms. In contrast with the DMN results, the study failed to identify significant SN-ECN connectivity effects, hence there is a lack of evidence for frontoparietal involvement in concussion risk. The elevated SN-DMN functional connectivity was identified for CSS but not CLS athletes. An absence of long-term associations is consistent with literature showing substantial variations in functional connectivity over months to years 34 (e.g., due to maturation and normal functional reorganization).
The DTI results also partially supported the secondary study hypothesis. Imaging showed significantly reduced FA of tracts connecting the SN and DMN for CSS athletes, but not for CLS athletes. Hence, SN-DMN structural connectivity is significantly related to short-term risk of injury, indicating a neuroanatomical substrate for the fMRI results. The interpretation of decreased FA is not straightforward, but may represent a combination of increased axonal diameter, decreased packing density and reduced myelination. 35 Overall, this suggests that heightened SN-DMN functional connectivity is at least partly due to less efficient direct signal transmission between networks, with greatest effects in major tracts of the cingulum and corpus callosum. The results are noteworthy, as stronger functional connectivity is typically associated with greater DTI indices of anatomical connectivity. 36,37 Nevertheless, inverse relationships between functional connectivity and FA have been identified in patient and healthy aging cohorts. 38 –41 In both cases, heightened functional connectivity has been interpreted as signifying reduced diversity of functional dynamics, with non-selective recruitment of regions during cognitive fluctuations to compensate for reduced anatomical connectivity. 38,40 Although study participants were young and in good health, the higher-risk athletes may similarly have subtle but consistent structural differences giving rise to heightened SN-DMN functional connectivity. Intriguingly, reductions in FA were identified for CSS athletes only, which reinforces that SN-DMN connections are relevant to short-term risk of injury. The absence of long-term associations may reflect structural plasticity in the young athlete cohort. Although DTI measures are more stable than fMRI over time scales of weeks to months, 42 there remains substantial yearly variability due to maturation, with the cingulum being particularly sensitive to change. 43
The neuroimaging effects were seen in the absence of significant differences in demographics or clinical assessments of symptoms, balance and cognition, relative to the broader cohort of NCA athletes. This is consistent with prior literature indicating limited ability of standard clinical batteries to predict concussion risk. 44 This is likely due to key domains not being well-captured, as testing usually focuses on speed of response, processing speed and working memory. 24,45,46 Based on the present results, tests of attentional switching between internally-directed and externally-directed tasks and interoceptive function may prove more sensitive to concussion risk. 47,48 However, comparisons of CSS and CLS athletes to matched controls yielded greater effect sizes for symptom measures, suggesting that self-reported symptoms are informative, if cohort matching is done appropriately. Significantly elevated baseline symptom severity for CSS athletes also supports the interpretation of heightened pre-injury SN-DMN connectivity correlating with a greater sensitivity to post-concussion symptoms.
Although this study provides a novel perspective on the neurobiology of concussion risk, there are some limitations that should be acknowledged. It was hypothesized that SN connectivity is related to concussion risk, based on its role in attentional orienting, adaptability and interoception. Although an association between SN connectivity and short-term concussion risk was identified, we lack direct evidence that the increased risk is due to deficits in SN-related cognitive domains. Future prospective imaging studies should therefore incorporate neurocognitive testing that is sensitive to these domains. 47,48 In addition, while the study findings are interpreted in terms of SN connectivity affecting cognition, this may represent reverse causation (i.e., SN connectivity may be modified by cognitive fluctuations). The relationship between functional connectivity, cognition and neuroplasticity remains an area of ongoing research. 49 There were also limitations in the techniques used to probe brain connectivity, with the relatively brief 6.5 min rs-fMRI sequence potentially contributing to variability in the functional connectivity measurements. 50
In addition, although robust FA effects were seen, the interpretation is ambiguous; studies using multi-shell diffusion imaging 51 and myelin water imaging 52 may yield greater insights. There are also demographic considerations. While subject matching controlled for baseline variation in sport, sex, HOC, and eligibility year, there may be uncontrolled factors that influence MRI parameter estimates. Differences in playing position and style may matter, along with HOC features (e.g., mechanism and severity of last injury). These issues should be addressed in larger cohort studies, as the present results were based on a limited sample of concussed athletes. For greater ecological validity, future studies should also include individuals with anxiety and mood disorders, as they are prevalent in the population and may influence concussion risk. Lastly, this study focused on the SN as a robustly detected network that is related to different aspects of concussion risk. However, there are likely other network interactions that play a role in concussion risk. Further work is needed to clarify the SN's role in the context of the whole-brain connectome.
In sum, this study provided evidence of pre-injury functional and structural correlates of concussion risk and resilience, with SN-DMN connections playing a key role. Given the health concerns associated with concussion, these findings highlight the importance of further research in this area. If validated in future studies, there is also potential for imaging and cognitive testing to develop strategies that improve concussion resilience, for example through cognitive and neuromodulatory interventions.
Footnotes
Authors' Contributions
NWC contributed to study design, analysis planning and execution, writing and interpretation of results. MGH contributed to study planning, interpretation of results and critical revision of the manuscript. SJG contributed to study design, interpretation of results and critical revision of manuscript. TAS contributed to study design, interpretation of results and critical revision of manuscript.
Funding Information
This work was supported by the Canadian Institutes of Health Research (CIHR) [grant numbers RN294001–367456, RN294001–367456]; the Canadian Institutes of Military and Veterans Health (CIMVHR) [grant number W7714-145967]; and funding from Siemens Canada Ltd.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix SA1