
Abstract
The lack of well-performing prognostic models for early prognostication of outcomes remains a major barrier to improving the clinical care of patients with mild traumatic brain injury (mTBI). We aimed to derive a prognostic model for predicting incomplete recovery at 1-month in emergency department (ED) patients with mTBI and a presenting Glasgow Coma Scale (GCS) score of 15 who were enrolled in the HeadSMART (Head Injury Serum Markers for Assessing Response to Trauma) study. The derivation cohort included 355 participants with complete baseline (day-of-injury) and follow-up data. The primary outcome measure was the Glasgow Outcome Scale Extended (GOSE) at 1-month and incomplete recovery was defined as a GOSE <8. At 1-month post-injury, incomplete recovery was present in 58% (n = 205) of participants. The final multi-variable logistic regression model included six variables: age in years (odds ratio [OR] = 0.98; 95% confidence interval [CI]: 0.97-1.00), positive head CT (OR = 4.42; 95% CI: 2.21-9.33), history of depression (OR = 2.59; 95% CI: 1.47-4.69), and self-report of moderate or severe headache (OR = 2.49; 95% CI: 1.49-4.18), difficulty concentrating (OR = 3.17; 95% CI: 1.53-7.04), and photophobia (OR = 4.17; 95% CI: 2.08-8.92) on the day-of-injury. The model was validated internally using bootstrap resampling (1000 resamples), which revealed a mean over-optimism value of 0.01 and an optimism-corrected area under the curve (AUC) of 0.79 (95% CI: 0.75-0.85). A prognostic model for predicting incomplete recovery among ED patients with mTBI and a presenting GCS of 15 using easily obtainable clinical and demographic variables has acceptable discriminative accuracy. External validation of this model is warranted.
Introduction
Traumatic brain injury (TBI) is a major public health challenge that results in 4.8 million emergency department (ED) visits each year, 1 of which 80-90% are classified as mild TBI (mTBI) 2 based on having a Glasgow Coma Scale (GCS) score of 13-15 shortly after injury. 3 For over 50% of patients with mTBI, limitations including persistent injury-related symptoms, cognitive dysfunction, and difficulties in day-to-day functioning occur up to a year after injury. 4 However, clinicians lack accurate prognostic tools to identify the subset of patients at high risk for incomplete recovery who may benefit from follow-up and monitoring post-injury. This gap in knowledge represents a major barrier to improving the clinical care for patients with mTBI.
ED clinicians are on the frontlines of brain injury care and are faced with quickly determining injury severity in order to initiate the most effective course of intervention. With moderate and severe TBI, the signs and symptoms of injury are more obvious than in mTBI. Determining injury severity in mTBI is significantly more challenging and clinicians must rely on information available at the time of ED presentation (e.g., whether loss of consciousness occurred, presence of neurologic deficits). In the absence of these types of symptoms, ED clinicians must make a diagnosis and determination of whether follow-up care is needed based upon very limited information. To make this decision, many ED clinicians rely more heavily on the GCS, which ranges from 3 (worst) to 15 (best), with TBI patients divided into the crude categories of mild (GCS 13-15), moderate (GCS 9-12), and severe (GCS 3-8). 3 However, when an individual presents with a head injury but limited signs and symptoms of a TBI and a GCS of 15, they often do not receive TBI educational material or referral to follow-up services, 5 and are frequently discharged directly from the ED. Whereas patients who present with a GCS of 13 or 14 have a 2-fold increase in odds of hospital admission and more than 4-fold increase in odds of intensive care unit admission. 6
The prevailing attitude of many ED clinicians is that most mTBI patients who present with a GCS of 15 will recover quickly and do not require referral to subspecialty care. 7 However, in a study of 217 patients with mTBI of which 89% had a presenting GCS of 15, treating ED clinicians predicted that 96% would have a complete recovery at 3-months when in fact only 47% had a complete recovery at 3-months. 7 These findings provide clear evidence that there is a need to arm clinicians with tools that can aid in accurately predicting the prognosis of mTBI, especially in those presenting with a GCS of 15.
Although there are number of prognostic models that have been derived for predicting outcomes post-mTBI, 8 –11 none of them are specifically focused on mTBI patients with a presenting GCS of 15, only a few of them are based on symptoms and clinical features obtained on the day of injury, and the majority of models have variable discriminative accuracy and poor calibration. 12 In addition, existing mTBI prognostic models generally predict 3-month or 6-month outcomes. However, especially in mTBI patients with a presenting GCS of 15, it is important to identify those who will have injury-related disabilities within 1-month post-injury, as receipt of expedited subspecialty care may be associated with improved long-term outcomes. 13 -15
Therefore, the objective of the current study was to derive and internally validate a prognostic model for predicting incomplete recovery at 1-month among ED patients with mTBI and a presenting GCS of 15 using easily obtainable clinical and demographic variables collected on the day of injury.
Methods
This study was conducted and reported according to the criteria of the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) statement. 16
Participants and study design
HeadSMART (Head Injury Serum Markers for Assessing Response to Trauma) was an observational, prospective cohort study that enrolled adults 18 years of age and older who presented to the Johns Hopkins Hospital or Johns Hopkins Bayview Medical Center for evaluation of blunt head trauma within 24 h of injury and who received a non-contrast head CT scan as part of clinical care. Additionally, all HeadSMART participants met the American College of Emergency Physicians 17 criteria for evaluation of blunt head trauma with a non-contrast head computed tomography (CT) scan in the ED. HeadSMART enrolled participants from June 2014 through June 2017. The study was approved by the Johns Hopkins Institutional Review Board. Trained research staff collected demographic and clinical information from participants in the ED using structured data collection forms. Assessments included the Rivermead Post Concussion Symptom Questionnaire (RPQ) 18 and the GOSE 19,20 as recommended by the interagency TBI Outcomes Workgroup. 21 Patients enrolled in HeadSMART, or their legally authorized representative, provided written consent. Patients were excluded from HeadSMART if they could not communicate in English, had no working telephone number, were pregnant, or had a past medical history of intracranial surgery, intracranial hemorrhage, brain tumor, or dementia. Details regarding the design and methods of HeadSMART have been described previously. 22
mTBI inclusion criteria
There is no clear consensus regarding which set of criteria to use to diagnose mTBI. With the goal of including the range of clinical presentations of mTBI, we applied the diagnostic criteria from four of the main approaches: Department of Veterans Affairs/Department of Defense (VA/DoD), 23 American Congress of Rehabilitation Medicine (ACRM), 24 Mayo Clinic, 25 and World Health Organization (WHO). 26 All study participants evaluated for inclusion met the diagnostic criteria of at least “possible” mTBI according to the Mayo Clinic criteria, with most participants clearly meeting criteria for a diagnosis of mTBI. Figure 1 describes the flow diagram of HeadSMART participants meeting criteria for at least “possible” mTBI with a presenting GCS of 15 and complete data. Missing data was handled via list-wise deletion.
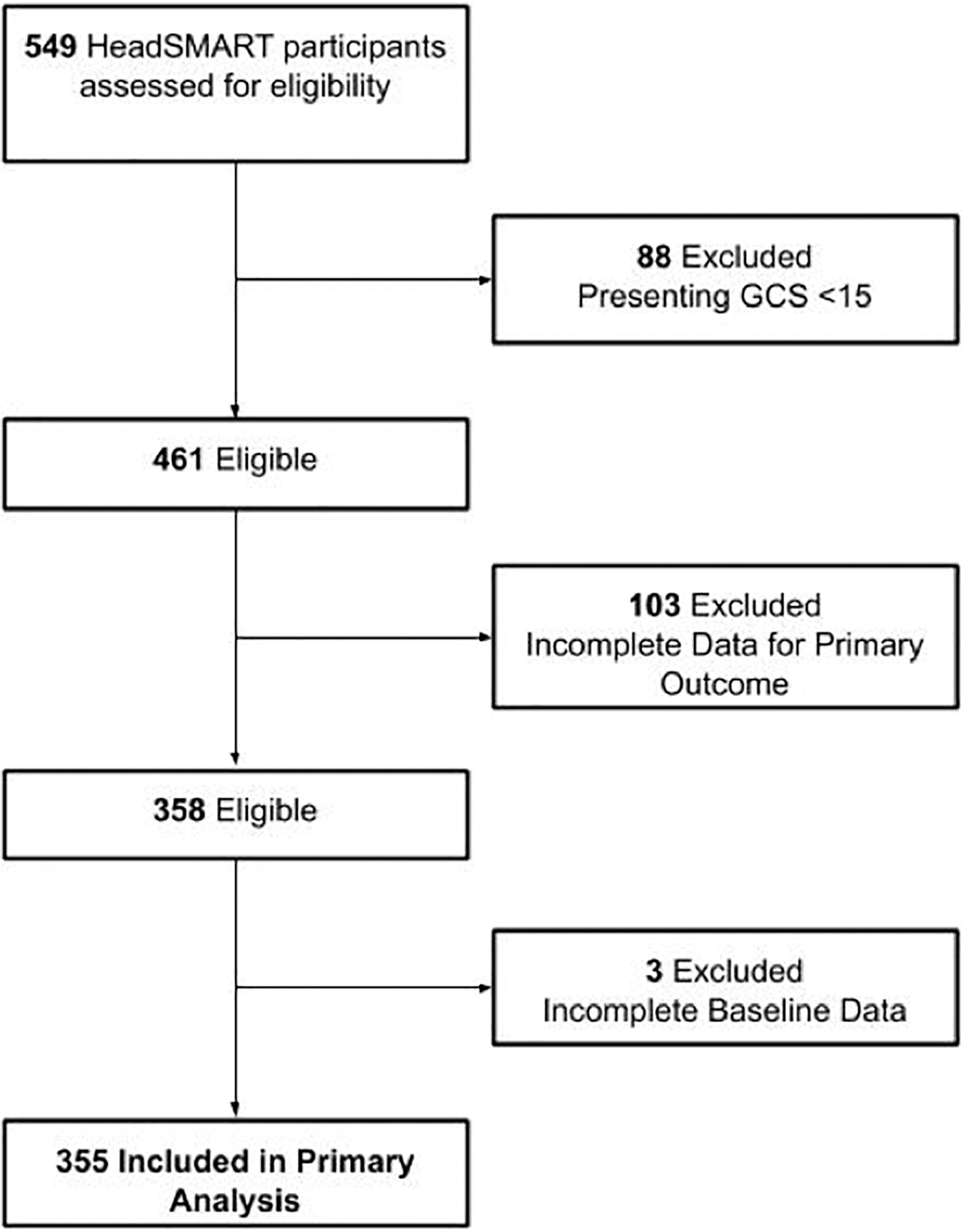
A total of 549 participants with acute TBI were enrolled in the completed prospective cohort study, HeadSMART (Head Injury Serum Markers for Assessing Response to Trauma). The final sample size for the primary analysis included 355 HeadSMART participants who met criteria for mTBI and had a presenting Glasgow Coma Scale score of 15 with complete data at baseline (day-of-injury) and at 1-month follow-up.
Data collection
Collection of demographic and clinical information occurred in accordance with the National Institute of Neurological Disorders and Stroke common data elements for TBI (CDE v.2). 27 Study data were collected and managed using the Research Electronic Data Capture (REDCap) tool hosted by the Johns Hopkins University Bloomberg School of Public Health. 28
Predictor variables
Clinical variables including mechanism of injury, past medical history (e.g., hypertension, history of depression), loss of consciousness, post-traumatic amnesia, altered mental status, memory deficits, focal neurologic deficits, acute drug and/or alcohol intoxication, extracranial injuries, patient-reported symptoms on the RPQ and demographic data including age, sex, race, ethnicity, years of education, marital status, and employment status collected in the ED on the day of injury were included as candidate predictor variables (Supplementary Table S1). Headaches, fatigue or tiring more easily, feeling frustrated or impatient, being irritable or easily angered, and restlessness were coded as positive responses if the patient reported them as moderate or severe on the RPQ due to their non-specificity and prevalence in the general population. All other symptoms on the RPQ were coded as positive if the patient reported them as mild or worse. A positive head CT scan was defined as the presence of an acute intracranial hemorrhage and/or skull fracture, or other acute intracranial abnormality. A board-certified neuroradiologist independently read all head CT scans. Age and years of education were modeled as continuous predictor variables and all other predictor variables were dichotomized.
Variable selection
A total of 43 candidate predictor variables were considered for inclusion in the final model. Backward elimination was used for variable selection and implemented by the fastbw function available in the rms package 29 developed for R 30 (4.0.2, R Foundation for Statistical Computing, Vienna, Austria, 2020) with a stopping rule of p < 0.05.
Outcome measure
The GOSE is a measure of the impact of TBI on various aspects of daily functioning 20 and was used to assess recovery at 1 month. GOSE quantifies functional outcome on an ordinal scale (1-8) defined as follows: 1) dead; 2) vegetative state; 3) lower severe disability; 4) upper severe disability; 5) lower moderate disability; 6) upper moderate disability; 7) lower good recovery; and 8) upper good recovery. While previously published prognostic models for mTBI have used variable GOSE cutoffs to define complete versus incomplete recovery in mTBI, 12 recent work suggests that patients with a GOSE of 8 (upper good recovery) and a GOSE of 7 (lower good recovery) may differ substantially across multi-dimensional outcome domains. 31 Compared with patients with a GOSE of 8, patients with a GOSE of 7 reported a higher prevalence of memory impairment, executive dysfunction, emotional distress, poor satisfaction with life, and persistent TBI symptoms beyond 1-month. 31 Thus, for this study, complete recovery was defined as GOSE = 8 (full return to pre-injury level of functioning) and incomplete recovery as GOSE <8.
Statistical analysis
All analyses were performed using R 4.0.2 and RStudio Version 1.2.5033. 30,32 Descriptive statistics were used to summarize the baseline (day-of-injury) demographic and clinical characteristics of the study population. The association between predictors and clinical outcome was modeled using logistic regression. Bootstrap resampling (1000 resamples) was used for internal validation of the model and the mean over-optimism value and optimism-corrected area under the receiver operating characteristic curve and 95% CI were reported.
Model calibration following internal validation was assessed using a calibration plot
(mean observed vs. mean predicted outcomes) and graphically using the calibration intercept and slope. 33 Collinearity was assessed using the variance inflation factor (VIF).
Results
A total of 461 participants enrolled in HeadSMART with mTBI had a presenting GCS of 15. Of those, 77% (n = 355) had a GOSE score at 1-month and were included in the derivation cohort. A flow diagram of participants evaluated for inclusion in the current analysis is presented in Figure 1. A total of 16% (n = 88) of all enrolled participants were excluded from analysis due to a presenting GCS <15, 29% (n = 103) did not have a GOSE score at 1 month, and 0.6% (n = 3) were excluded because of incomplete day-of-injury data. The baseline demographic and clinical characteristics of the final cohort of 355 participants appear in Table 1. The median age was 45.0 years (interquartile range: 28.0-64.0) and 47% (n = 168) were female.
Baseline Demographic and Clinical Patient Characteristics
Rated as moderate or severe on the Rivermead Post Concussion Symptoms Questionnaire.
Rated as mild or worse on the Rivermead Post Concussion Symptoms Questionnaire.
Demographic and clinical characteristics of HeadSMART participants with Glasgow Coma Scale score 15 traumatic brain injury included for analysis. Age and years of education were modeled as continuous predictor variables and all other variables were dichotomized.
IQR, interquartile range, MVC, motor vehicle collision; MCC, motorcycle collision; CT, computed tomography.
Incomplete recovery (GOSE <8) at 1-month was reported in 58% (n = 205) of participants and complete recovery (GOSE = 8) was reported in 42% of participants (n = 150). The candidate predictor variables of participants with complete and incomplete recovery at 1 month post-injury appear in Supplementary Table S1. Age, history of depression, positive head CT, and self-report of injury of moderate or severe headache, difficulty concentrating, and photophobia on the day of injury were selected for inclusion in the model using backward elimination with a stopping rule of p < 0.05. All variables had a VIF <3, indicating a lack of multicollinearity between predictor variables. The predictor variables and their adjusted odds ratios (ORs) and 95% confidence interval (CI) are available in Table 2 and include: 1) age (OR = 0.98; 95% CI: 0.97-1.00); 2) depression (OR = 2.59; 95% CI: 1.47-4.69); 3) positive head CT (OR = 4.42; 95% CI: 2.21-9.33); 4) moderate or severe headache (OR = 2.49; 95% CI: 1.49-4.18); 5) difficulty concentrating (OR = 3.17; 95% CI: 1.53-7.04); and 6) photophobia (OR = 4.17; 95%CI: 2.08-8.92).
Adjusted Odds Ratios (95% CI) for Selected Predictors for Final Multi-Variable Logistic Regression Model
The adjusted odds ratios and 95% CIs for the six variables selected by backward elimination with a stopping rule of p < 0.05, which were included in the final multivariable logistic regression model.
CI, confidence interval; CT, computed tomography.
The six variable model was validated internally using bootstrap resampling (1000 resamples), which revealed a mean over-optimism value of 0.01 and an optimism-corrected area under the curve of 0.79 (95% CI: 0.75-0.85; Fig. 2). Model calibration was assessed graphically using the calibration slope and intercept. The calibration plot for the final multi-variable logistic regression model after internal validation by bootstrapping appears in Figure 3. The calibration intercept of our derived model was 0.007 with a calibration slope of 0.935, suggesting good model calibration.

The final multi-variable model included six predictor variables: age, history of depression, positive head computed tomography (CT) scan, and self-report of moderate or severe headache, difficulty concentrating, and photophobia on the day-of-injury. The optimism-corrected area under the curve (AUC) after internal validation by bootstrap resampling was 0.79 (95% CI: 0.75-0.85). The x-axis is the false positive rate (1-Specificity), and the y-axis is the true positive rate (Sensitivity).
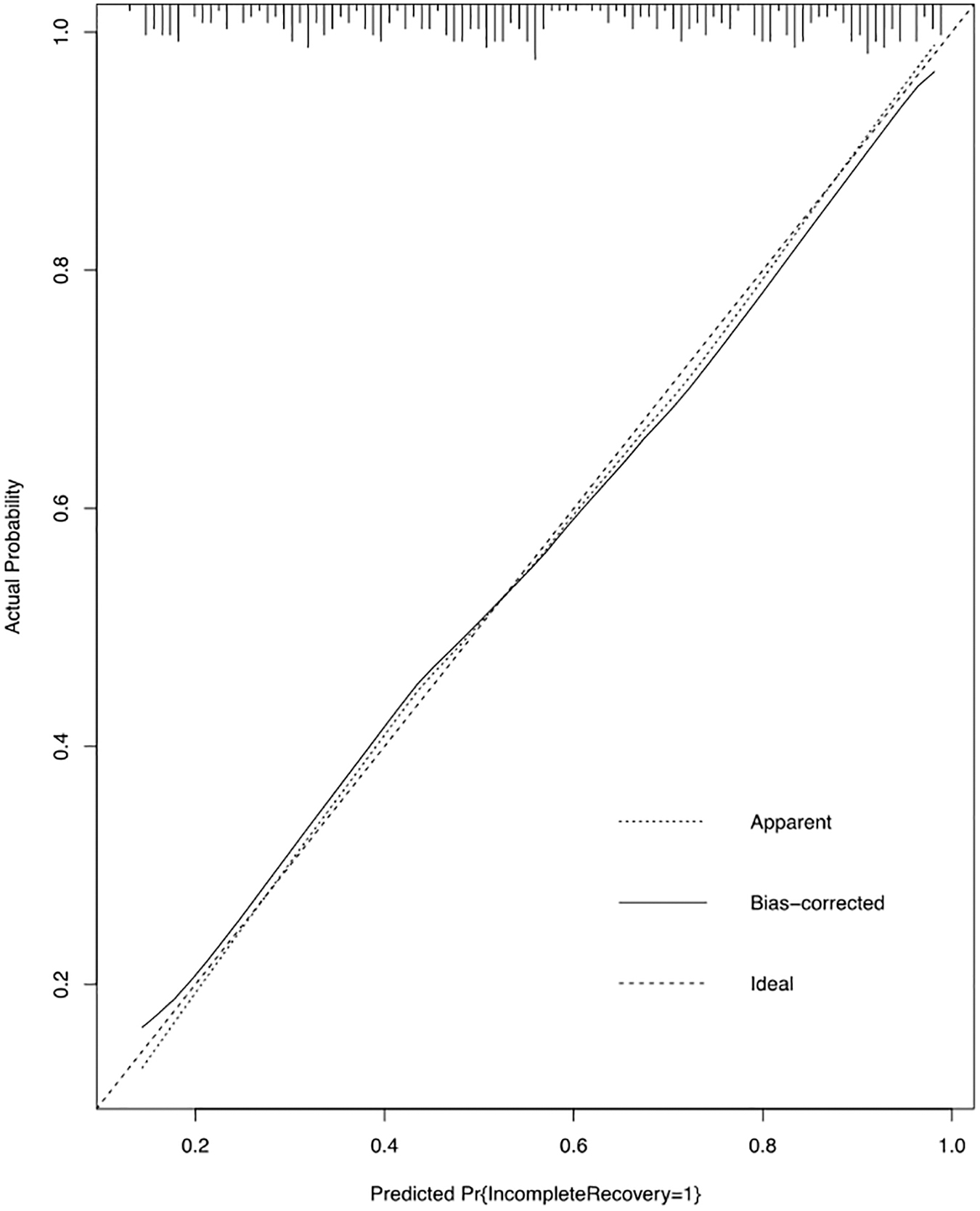
Calibration plot for the final prognostic model for predicting incomplete functional recovery at 1-month using data from HeadSMART (Head Injury Serum Markers for Assessing Response to Trauma) participants with Glasgow Coma Scale (GCS) 15 MTBI. The apparent (in sample) and bias-corrected (after internal validation with 1000 resamples) calibration curves are plotted against the 45° line (ideal; intercept = 0, slope = 1) to assess the calibration accuracy of our final model following internal validation using bootstrap analysis. 1000 bootstrap repetitions were performed with the calibration intercept = 0.007 and the calibration slope = 0.935. Areas of the calibration plot where the slope >1 represent areas of model underfitting and areas where the slope <1 represent areas of overfitting. The distribution of the data is visualized by tick marks at the top of the plot.
Discussion
The study findings provide further evidence that individuals with mTBI and a presenting GCS of 15 may be at risk for poor outcomes. Our findings support the accuracy and validity of a prognostic model for identifying those at risk for poor outcomes by 1-month post-injury. Our prognostic model was derived using easily obtainable demographic and clinical data that can be collected on the day of injury in the ED. These include age, positive head CT, history of depression, and self-report of moderate or severe headache, difficulty concentrating, and photophobia. Although the prognostic model requires external validation in an independent cohort, the findings provide preliminary evidence that it has the potential to help inform clinical decision making in the acute care setting by identifying those at risk of incomplete recovery. Further, the model may provide future additional benefits by increasing the efficiency of clinical trials of novel mTBI therapeutics and supporting precision medicine efforts. 34
Strengths of this study include the incorporation of post-injury symptoms evaluated in the acute phase of mTBI (day-of-injury). None of the previously published mTBI prognostic models of functional outcome (GOSE) that met at least one of the criteria for inclusion in the large external validation study by Mikolic and colleagues 12 (sample size >500, > 10 events per candidate predictor variable, use of some form of shrinkage and/or external validation) included acute mTBI-related symptoms as predictor variables. 9 -11 In models predicting persistent post-concussive symptoms (PPCS), the inclusion of post-injury symptoms measured days to weeks after injury substantially improved discriminative accuracy. 12 However, the clinical utility of models containing predictors measured after discharge is particularly low when the objective is to make an accurate prognosis in the ED. Further, existing prognostic models predicting functional outcome do not account for the substantial heterogeneity that characterizes GCS 13-15 mTBI, resulting in models with highly variable discriminative accuracy and poor calibration. In focusing on the subgroup of patients with mTBI and a presenting GCS of 15, a population for whom accurate prognosis may be especially difficult in the absence of overt clinical signs such as loss of consciousness, presence of neurologic deficits, and abnormal clinical findings, we were able to successfully derive a well-calibrated prognostic model with acceptable discriminative accuracy.
Frequent predictors of outcome in mTBI include age, 8 –12 pre-injury mental health, 8,11,12,35 –43 acute neuroimaging abnormalities, 4,8 –12,44 –46 and post-concussion symptoms, 11,12,42,43,46 –49 which are consistent with our overall findings. Older age was found to be slightly protective (OR = 0.98), which is consistent with previously published analyses of the HeadSMART cohort demonstrating that older adults had equivalent or better functional outcomes at 1-month post-injury compared with younger individuals. 50,51 However, a number of studies have demonstrated worse functional outcomes in older adults with mTBI. 52 –55
Participants with mTBI and a presenting GCS of 15 with a history of depression were 2.59 times more likely to experience injury-related limitations at 1-month post-injury. Depression is the most common psychiatric complication following TBI and is associated with decreased cognitive performance, disability, decreased quality of life, and suicidal ideation. 56,57 Estimates of the prevalence of depression following TBI are as high as 50%. 56,58 –62 The finding that a history of depression is a predictor of incomplete recovery at 1-month may suggest that patients with a pre-injury history of depression may experience an exacerbation of their symptoms following injury, leading to worse outcomes at 1-month. This finding requires further research.
Patients who self-reported symptoms including moderate or severe headache, difficulty concentrating, and photophobia on the day of injury were significantly more likely to experience incomplete recovery at 1-month post-injury. Headache occurs frequently following mTBI, and was significantly associated with mTBI in a study examining associations between post-traumatic stress disorder, depression, physical health symptoms, and mTBI. 63 Photophobia is another common symptom following mTBI; however, the pathophysiology remains incompletely understood. 64 Other work has identified dizziness, nausea, and trouble concentrating as being associated with post-concussion symptoms lasting longer than 1 week in a subset of athletes with concussion. 65
We examined the presence or absence of individual post-concussion symptoms reported on the RPQ. However, other work has suggested that overall symptom severity 66 and total symptom burden 40 are associated with incomplete recovery. The inclusion and development of symptom-based risk scores may be important directions for future analyses. Although beyond the scope of the current analysis, it will be important to examine the prognostic utility of blood-based biomarkers of brain injury and more sensitive neuroimaging modalities such as magnetic resonance imaging (MRI), compared with current models based only on clinical and demographic variables. In particular, MRI may play an especially important role in improving prognoses for patients with negative head CT scans. 45
We recognize that while our study has several strengths, there are limitations. First, the GOSE was used as the measure of functional recovery, and although it is the most commonly used primary outcome measure in TBI clinical trials, it may not be sensitive enough to capture persistent injury-related deficits in specific functional domains (e.g., cognitive, behavioral/emotional). Second, diagnosis of mTBI was not based upon a specific classification system but rather all the symptoms/signs that are included in four of the most used diagnostic criteria sets. Although this will help to apply these results to clinical situations faced day-to-day in EDs across the country, the results are not necessarily directly comparable to other studies in which a specific classification system is used. However, it should be recognized that there is marked overlap among the various classification systems and the evidence is mixed and quite limited that differences between systems are clinically meaningful. Future research needs to investigate which class of criteria leads to the most valid and reliable prognostication particularly with regard to mTBI. Third, it is important to note that our cohort of GCS 15 mTBI patients evaluated in the ED were more severely injured (57% with loss of consciousness, 41% with altered mental status, 18% with a positive head CT scan) than GCS 15 mTBI patients encountered in non-ED settings. In addition, we studied ED patients who were evaluated within 24 h following injury. Therefore, it is not known whether our study findings will be applicable to patients evaluated outside the ED or those who present to the ED >24 h following injury. Finally, our final model needs to be externally validated 12,33 prior to adoption in a clinical setting.
The results of our analysis and resulting prognostic model add to our knowledge of the day-of-injury variables that contribute to incomplete recovery in the subset of patients with mTBI and a presenting GCS of 15 and has the potential to aid in early identification of patients who are at high risk for incomplete recovery. Such a model fills an unmet clinical need and may be used to inform subject selection in therapeutic drug trials. Overall, having clinical indicators available at the time of ED presentation that could assist in identifying those individuals at risk for poorer outcomes represents a notable step in the advancement of mTBI care.
Footnotes
Funding Information
HeadSMART was supported by a grant from ImmunArray, Inc.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.