
Abstract
Sports-related concussion (SRC) can exert serious acute and long-term consequences on brain microstructure, function, and behavioral outcomes. We aimed to quantify the alterations in white matter (WM) microstructure and global network organization, and the decrements in behavioral and cognitive outcomes from pre-season to post-concussion in youth athletes who experienced SRC. We also aimed to evaluate whether wearing a jugular compression neck collar, a device designed to mitigate brain “slosh” injury, would mitigate the pre-season to post-concussion alterations in neuroimaging, behavioral, and cognitive outcomes. A total of 488 high school football and soccer athletes (14-18 years old) were prospectively enrolled and assigned to the non-collar group (n = 237) or the collar group (n = 251). The outcomes of the study were the pre-season to post-concussion neuroimaging, behavioral, and cognitive alterations. Forty-six participants (non-collar: n = 24; collar: n = 22) were diagnosed with a SRC during the season. Forty of these 46 athletes (non-collar: n = 20; collar: n = 20) completed neuroimaging assessment. Significant pre-season to post-concussion alterations in WM microstructural integrity and brain network organization were found in these athletes (corrected p < 0.05). The alterations were significantly reduced in collar-wearing athletes compared to non-collar-wearing athletes (corrected p < 0.05). Concussion and collar main effects were identified for some of the behavioral and cognitive outcomes, but no collar by SRC interaction effects were observed in any outcomes. In summary,
Introduction
Mild traumatic brain injury (mTBI) is common in competitive sports and recreational activities, with 1.6 to 3.8 million sports-related concussions (SRCs) reported annually in the United States. 1 In youth athletes, high school football and soccer have the highest concussion incidence rates in male and female athletes, respectively. 2,3 While SRC can exert serious acute and long-term consequences on brain microstructure and functional outcomes, the underlying mechanism and the progression of change from pre-injury baseline to post-injury are lacking. Such prospective longitudinal outcomes are critical to inform interventions that can help prevent and possibly support the reversal of neurologic injury. 4
Neuroimaging studies of mTBI, including SRC, have revealed alterations in widespread white matter (WM) regions. 5 –14 Diffusion tensor imaging (DTI) measures can differentiate concussed from non-concussed subjects by quantifying differences in WM regions throughout the brain 9,15 -17 ; however, findings have been inconsistent in the diffuse location of affected regions and their associations with neuropsychological functioning. 5,18 Graph theory-based network connectivity analysis of DTI and tractography has recently emerged as a promising approach to characterize brain connectivity at global levels. 19,20 When applied to mTBI, this approach has revealed altered WM structural integrity characteristics, with reduced brain network connectivity similar to that seen in neurological disorders with global network pathologies. 6,21 -23
The majority of prior DTI studies investigating WM alterations among high school athletes have utilized cross-sectional designs or longitudinal designs that compared WM alterations at different stages post-concussion. 24 No study has reported prospective longitudinal DTI data delineating post-concussion microstructural and connectivity changes relative to pre-injury baseline in youth athletes with SRC. The lack of such longitudinal neuroimaging data comparing the pre- and post-concussion WM alteration has limited the discovery of clinically valid and sensitive biomarkers of SRC and impeded the development of effective interventions and/or preventive strategies. Current concussion prevention strategies (e.g., helmets) have only demonstrated limited efficacy for preventing open head injury. 25 -27 We have evaluated a novel prevention strategy to protect WM integrity against repetitive, sub-concussive head impacts by using a jugular venous compression collar device.
The jugular vein compression collar was designed to capitalize on existing fluid dynamics in the brain and promote cerebral vein filling by “taking up” the compensatory reserve volume, fashioned off the diagnostic Queckenstedt's maneuver. 28 The collar device supports mild, physiologically-safe increases in intracranial pressure and volume, generating similar or less pressure/volume changes to lying prone or performing a Valsalva maneuver. In theory, the collar may mitigate brain movement (“slosh”) in the skull during repetitive concussive head trauma 29 -31 and/or redistribute intracranial shear and strain energy absorption depending on impact magnitude and intensity. 32 This novel strategy offers promising results in mitigating structural and functional alterations related to sub-concussive head impacts, 33 –36 but whether it can protect against WM alterations following SRC is unknown.
Using a prospective longitudinal study design, we aimed to test two hypotheses: 1) There will be significant pre- to post-concussion alterations in WM microstructure and global network organization, as well as pre- to post-concussion decrements to behavioral and cognitive outcomes; 2) Wearing the jugular compression neck collar would reduce pre- to post-concussion alteration in neuroimaging and behavioral and cognitive outcomes.
Methods
Participants
Participants were enrolled as part of a large, prospective neuroimaging study of high school athletes in contact sports (
Group assignment for all athletes at baseline
All athletes were allocated at the team level to a non-collar (eight teams; 237 athletes) or collar group (eight teams; 251 athletes) before the season onset. See details in Supplementary Appendix S1.
Intervention
For those athletes assigned to the intervention group, a lightweight collar device was worn during all the games and practices. The collar applied mild jugular compression according to the principle of Queckenstedt's maneuver and was designed to mitigate the slosh energy during head impact. 29,30,33 –37
Outcomes
The outcomes of the study were the pre-season to post-concussion microstructural changes in WM based on DTI, the alterations in network integrity based on DTI tractography and graph theory, and the degradation in behavioral and cognitive outcomes based on King Devick (KD) Test, the Near Point Convergence Test (NPC), the Trail Making Test (TMT), and the Flanker Test.
Athlete surveillance, head impact tracking, and concussion diagnosis
Athletes' attendance, participation, and collar compliance were recorded by research staff for each athletic exposure (i.e., practice and game). All athletes wore an accelerometer device (CSx Systems Ltd, Auckland, New Zealand) throughout the season to track head impacts (see Supplementary Appendix S1 Methods). 38 School athletic trainers/physicians were responsible for evaluating athletes with suspected concussion. Post-concussion return-to-play decisions were made by the school medical team based upon standard guidelines.
Magnetic resonance imaging acquisition, processing, and analysis
Magnetic resonance images were acquired on three 3-Tesla Phillips scanners (Achieva, Ingenia, and Elition) using identical scan sequence specifications. All participants completed pre-season and post-concussion testing on the same scanner. The protocol included DTI (using a spin echo-planar imaging sequence with 61 non-colinear diffusion directions), T1-weighted, T2-weighted, susceptibility-weighted, resting-state functional magnetic resonance imaging (fMRI), and magnetic resonance spectroscopy sequences. Anatomic imaging data were reviewed by a board-certified radiologist. DTI data were processed with the Functional MRI of the Brain (FMRIB) Software Library (FSL) package. The tract-based spatial statistics (TBSS) approach was used to localize microstructural alteration in WM in response to SRC. Graph theoretical analysis was performed to quantify global changes in brain network organization. See the Supplementary Appendix S1 Methods for additional details.
Behavioral and cognitive outcome assessment
Participants performed the KD, NPC, TMT, and the Flanker Test at both pre-season and post-concussion on the same day as the MRI scan. Data for previous attention deficit-hyperactivity disorder (ADHD) diagnosis and/or treatment, based on parent and/or athlete report were collected during the pre-season visit. To evaluate the symptoms of ADHD, data for the Strengths and Weaknesses of ADHD Symptoms and Normal Behavior Scale (SWAN) were also collected. See details in Supplementary Appendix S1.
Statistical analysis
In the analysis of demographic and clinical data, head impact exposure, and concussion outcomes, within-group pre-season to post-concussion changes were tested using paired samples t-tests. Between-group differences of the changes of pre-season to post-concussion alterations were tested using two-sample t-tests.
For TBSS analysis, voxel-wise comparisons of DTI measures including fractional anisotropy (FA) and mean, axial, and radial diffusivity (MD, AD, and RD, respectively) were conducted comparing pre-season and post-concussion in athletes with SRC. A difference map between the two time-points was calculated and used in a one-sample t-test to assess within-group longitudinal changes. General linear modeling (GLM) was used to identify significant group differences (collar vs. non-collar) in the pre-season to post-concussion changes. Potential confounding factors, including age, baseline DTI (for potential scanner difference), number of head impacts experienced before concussion, and time interval between concussion and post-concussion MRI were included as covariates (tested separately). The randomize function in FSL was used to test statistical significance. Threshold-free cluster enhancements 39 with 5000 permutations were used to correct multiple comparisons errors. From WM regions with significant group difference of DTI changes, DTI values were extracted and used to calculate pre-season to post-concussion percentage changes in the two groups separately.
In the graph theoretical analysis, potential pre-season to post-concussion alterations were first tested for each global network measure using paired t-tests for the two study groups separately. The effect of collar wearing was tested based on the group difference of pre-season to post-concussion changes using two-sample t-tests. To avoid influence of an arbitrarily selected network density, each network matrix was thresholded over a density range of 0.18 to 0.25 at intervals of 0.01. The area under the curve (AUC) was calculated and used for group comparisons (see Supplementary Appendix S1 Methods).
For behavioral and cognitive outcomes, separate 2 between-subject (group: collar, non-collar) × 2 within-subject (time: pre-season, post-concussion) mixed effect GLM models were conducted for each variable. While the group by time interaction is the term of particular relevance for determining the potential differential impact of SRC on the two groups, we will also present the main effect of time as this reflects a change in functioning from pre-season to post-concussion and may provide some information about post-concussion changes (see Supplementary Appendix S1 Methods).
Results
Number of concussions and concussion incidence rate
A total of 46 athletes, including 32 male football athletes and 14 female soccer athletes, experienced a SRC during the season: 24 in the non-collar group, and 22 in the collar group. Among these, six athletes could not undergo MRI due to metal orthodontics. In the present study, all the imaging related data analyses were based on the 40 athletes with SRC who completed both pre-season and post-concussion imaging. We will report the findings first based on the intent-to-treat design in which data are analyzed with participants kept in the group as initially assigned, regardless of compliance level or premature drop-outs (non-collar: n = 20; collar: n = 20, initial group assignment; Supplementary Appendix Fig. S1). The four per-protocol scenarios, which require full compliance and thus involves excluding or reassigning participants, and the results are reported in Supplementary Appendix Figure S1.
The risk of concussion for the overall cohort was 9.43% (46/488) with no significant difference between the non-collar (10.13%, 24/237) and collar groups (8.76%, 22/251, p = 0.64; Table 1 intent-to-treat). In the Per-Protocol analyses, significant group difference was only found in the Per-Protocol 4 analysis, in which a significantly higher concussion risk was observed in the non-collar group (p = 0.031; Table 1). With a total number of athletic exposures (AE) of 19,877 for the entire season (9487 in the collar group; 10,390 in the non-collar group), the overall concussion incidence rate was 2.31 per 1000 AE. Incidence rate was comparable between the two study groups in all five analysis scenarios (Table 1).
Number of Concussions and Concussion Incidence Rates in Collar-Wearing and Non-Collar-Wearing Athletes by Five Different Analytic Designs
Incidence rate was calculated as number of concussions per 1000 athletic exposures (AEs). p Value calculated based on Fisher's exact test.
White matter microstructural changes
Based on intent-to-treat scenario, TBSS analysis revealed a significant pre-season to post-concussion increase in MD and/or AD in extensive WM regions within the non-collar group (corrected p < 0.05; Fig. 1A, 1B), but not in the collar group (Fig. 1C, 1D). Pre-season to post-concussion MD, AD, or RD increases were significantly greater in the non-collar group than in the collar group (all corrected p < 0.05, Fig. 2A-L), with the differences located primarily in the genu and body of corpus callosum, bilateral anterior and superior corona radiata, and in left cerebral peduncle, external capsule, and anterior and posterior limb of internal capsule. Demographic information used in imaging analysis is summarized in Supplementary Table S1.
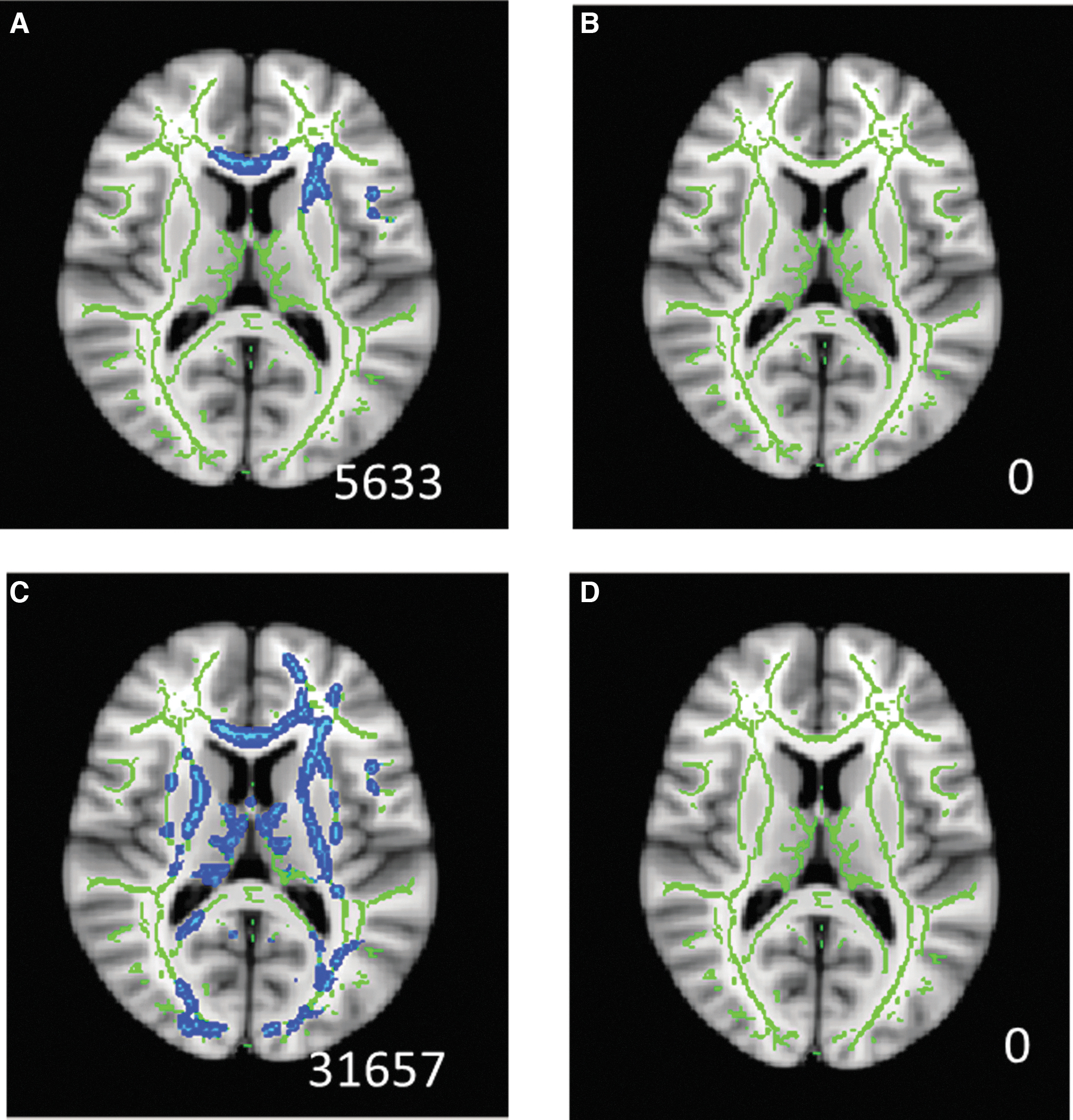
Within-group pre-season to post-concussion diffusion tensor imaging (DTI) alteration using intent-to-treat analysis (non-collar: n = 20, collar: n = 20). White matter (WM) regions with significant increase in mean diffusivity
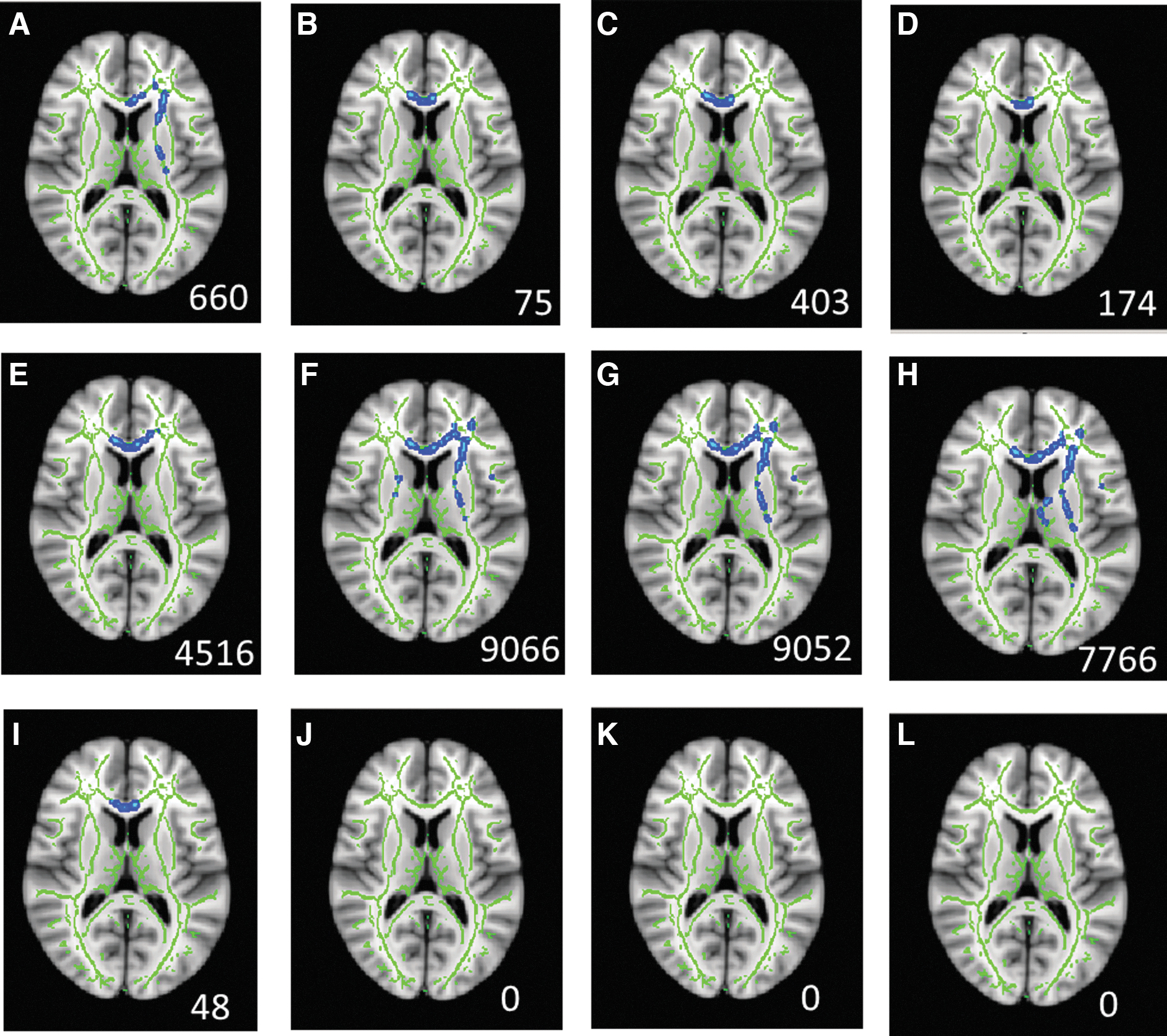
Between-group difference of pre-season to post-concussion diffusion tensor imaging (DTI) alteration using intent-to-treat analysis (non-collar: n = 20, collar: n = 20). White matter regions with significantly greater increase in mean diffusivity (1st row,
Within WM regions exhibiting significant group differences, the percentage DTI change from pre-season to post-concussion in the non-collar group was −0.47 ± 2.88%, 3.70 ± 4.13%, 4.07 ± 3.78%, 3.85 ± 5.66% for FA, MD, AD, and RD, respectively, based on intent-to-treat (Table 2). By contrast, the percentage change in the collar group was smaller in magnitude (Table 2). Per-Protocol analyses produced similar results (Table 2; Supplementary Appendix Fig. S2-S9).
Percentage DTI Change at Post-Concussion from Pre-Season by Different Analytic Designs
The four per-protocol analyses were performed to address compliance issue for collar wearing at the time of concussion.
DTI, diffusion tensor imaging; FA, fractional anisotropy; MD, mean diffusivity; AD, axial diffusivity; RD, radial diffusivity.
White matter network integrity alterations
Graph theoretical analysis for intent-to-treat revealed a significant pre-season to post-concussion decrease in mean local efficiency in the non-collar group (AUC in density range 0.18–0.25, p = 0.036; Table 3) and a significant increase in mean local efficiency in the collar group (p = 0.017). The between-group difference of the pre-season to post-concussion change was statistically significant (p = 0.0024; Table 3; Supplementary Appendix Fig. S10). No significant within-group pre-season to post-concussion change or between-group difference of the change was found in any other global structural network measures (Eglob, MOD, γ, λ, σ). Findings were consistent and similar in the four Per-Protocol analyses (Supplementary Appendix Tables S2–S5 and Fig. S11).
Comparison of Change in mean Eloc according to Intent-to-Treat Design (Non-Collar: n = 20, Collar: n = 20) at Different Network Density Levels and Area Under Curve

SD, standard deviation; AUC, area under curve for mean Eloc curve across density range (0.18-0.25).
Alterations in behavioral and cognitive assessment
The baseline comparison of behavior and cognitive assessment in the Intent to Treat and the four Per-Protocol analyses are included in the Supplementary Appendix Tables S6–S10. Based on intent-to-treat analysis, there was a significant main effect of collar in KD test: the collar wearing is associated significantly with the reduction in KD Time average (p = 0.003; Table 4). In the Flanker test, there was a significant main effect of time: the concussion was significantly associated with the increase in the Alerting network score (p = 0.006; Table 4). There was also a significant main effect of both collar and time on the Flanker test: concussion was associated with the decrease of Conflict score (p = 0.001, Table 4), while collar wearing was associated with higher Conflict score (p = 0.01, Table 4). No significant main effect was found in either collar or time in any other dependent variables among those assessed. There was no significant collar by time interaction in the model for any behavioral or cognitive outcomes. More specifically, the SRC did not show significant impact to differentiate the alterations in any variables derived from the KD test, NPC test, SWAN, Flanker test, or TM test between the collar wearing and the non-collar wearing group. The Per-Protocol analyses generated similar results (Supplementary Appendix Tables S11–S14).
Assessment of Main Effect in Behavioral and Cognitive Outcome Based on Intent-to-Treat Analysis
NPC, Near Point Convergence Test; Avg, average; KD, King Devick Test; SWAN Strengths and Weaknesses of ADHD Symptoms and Normal Behavior Scale; IN, inattention score; HI, hyperactive/impulsive score; TMT, Trail Making Test.
Discussion
This study contributes the largest prospective longitudinal DTI datasets collected at both pre- and post-concussion in youth athletes with SRC. These data are scarce in the field but of critical importance in fully delineating WM alterations in the pediatric population. Performing longitudinal comparisons in concussed subjects relative to their own pre-injury data allows for minimizing the confounding effects of inter-subject differences inherent in cross-sectional comparisons. Several SRC studies reported longitudinal comparisons using DTI data acquired at different stages after concussion, all using region of interest (ROI)-based or voxel-based analysis approach. 8,10,13,15,24 Only two studies reported longitudinal changes in SRC with baseline and post-injury DTI data in college athletes or young adults with limited sample (n = 13 and n = 10, respectively). 7,40 Our DTI data were acquired prospectively in 40 athletes at both pre-season and post-concussion, and the results using voxel-based TBSS analysis corroborate the findings of Cubon and colleagues in location and direction of change in diffusion indices. 7 This inter-study agreement is encouraging, but such longitudinal data remain rare.
Brain injury is often diffuse in children after TBI. 6,22,23,41 While the conventional ROI-based analysis or voxel-based TBSS approach aim to test and localize injuries, graph theoretical analysis allows for characterizing SRC consequences based on alterations that affect global level organization in the entire brain network. This complementary approach has revealed altered structural connectivity measures following TBI in adults and children. 22,41 The present study provides the first prospective longitudinal neuroimaging application of graph theoretical analysis in high school athletes with SRC. Mean local efficiency, an index reflecting network wiring redundancy (or how efficiently information is transferred among nodes in network) and tolerance to attack, 19 decreased in the non-collar group after SRC, suggesting a disruption in network organization. Thus, our data may reveal an early manifestation of the consequence of SRC suggesting that the concussion negatively affected the brain network's robustness, potentially making it more vulnerable to future insults. However, since no athlete in our study experienced more than one SRC during the season, the potential association between concussion event and propensity for additional concussion could not be tested.
A primary goal of our study was to evaluate whether the collar device can limit WM alterations following SRC, which may protect athletes' short- and long-term brain health. Previous studies of the collar provided encouraging evidence for a protective effect against sub-concussive head impacts. 33 –37 The present study for the first time yielded sufficient numbers of concussion injuries to enable meaningful statistical analyses of those with SRC. While incidence rate was similar between groups, one of the per protocol analyses (Per-Protocol 4) indicated that athletes wearing the collar had a lower concussion risk than the non-collar group when the non-compliant cases were re-assigned to the non-collar group. However, the current project was not powered to detect differences in concussion risk or incidence rates so these data should be interpreted with caution. Collar wearing did show promising evidence for reducing alterations in WM microstructural integrity and network organization in athletes with SRC. The study adds to prior literature that collar device may not only protect athletes' brains against “mild” sub-concussive head impacts 33 -35,37,42 but may also mitigate potential changes resulting from concussive events. The jugular compression collar was designed to induce an “internal cushion” that might reduce slosh-mediated energy transfer during head impacts. 29,30 This putative protection mechanism is distinct from traditional protective devices using helmets and/or headgear that are designed to externally cushion the head. If confirmed by further large-scale longitudinal studies, our findings could initiate a fundamental change in research focused on prevention strategies for participants in sports and also for personnel in occupations with high risk for mTBI (e.g., military and police professionals with frequent exposure to blast injury).
Our assessment of behavioral and cognitive outcomes did not indicate significant collar × time interaction effects in any test, suggesting a lack of differential effect of concussion in the collar and non-collar groups with these outcomes. A closer examination showed that there was a main effect of collar in KD average response time driven by the lower average KD time in the collar group at both pre-season and post-concussion. However, the faster reading speed in the collar group could be just an implication of relatively better performance at pre-season but without any clinical significance. In line with our expectations, both Alerting network and Conflicting network from the Flanker task were negatively impacted by concussion, regardless of group. However, counter intuitively, we also found that Conflicting network improved following concussion. Since the impact of SRC was consistent across groups, this unexpected finding could be attributed to practice effects, but further research is needed in order to support the use of these outcomes clinically in SRC assessment. It is noteworthy that the lack of significant collar effect in mitigating behavioral/cognitive changes is incongruent to the significant findings of the collar effect in ameliorating neurophysiological changes based on neuroimaging data. It is possible that the behavioral/cognitive response may be changes occurred further downstream change, and since we are only assessing changes occurred soon after the concussion, the alterations detected were just the first layer of change (physiology) prior to the more overt behavioral/cognitive changes that may emerge after multiple seasons/concussions.
Limitations of this study include a sample size that precluded more comprehensive statistical analysis (e.g., testing covariates together and including more variable such as concussion history, duration of participation of contact sports, education achievement), lack of a control non-concussion group to account for developmental changes in DTI metrics and cognition or changes associated with sports participation, lack of standardized procedure across schools for concussion diagnosis, and potential that some athletes did not report concussion symptoms immediately or at all. The delay in reporting may lead to error in the quantification of head impact exposure prior to concussion, the interval between concussion and MRI, or even in the diagnosis of concussion itself. In the present study, the a priori definition of concussion relied on the diagnosis by team medical staff. Concussion diagnosis as a clinical endpoint was confirmed by school athletic trainer and physician based on subjective signs and symptoms per standardized state and school guidelines. Non-consistency may occur and therefore affects the interpretation of our current results; however, our approach was consistent in our protocol and between study conditions eliminating potential systematic bias between groups. The interval between concussion and post-concussion testing was 1 week on average, which could limit interpretations associated with temporal progression of WM alterations. In future large scale clinical trials, the psychological effect of collar wearing needs to be assessed for its potential influence on athletes' behavior during the participation of the sports.
Conclusion
This study provides initial data demonstrating longitudinal alterations in WM microstructural integrity, brain network organization, and cognitive outcomes among high school athletes who experienced SRC. Wearing a jugular vein compression collar mitigated WM alterations at both the regional and global level, suggesting a potentially protective effect against concussion-related changes. Behavioral and cognitive outcomes also demonstrated changes in response to concussion but no interaction of collar with concussion was found. Studies with larger sample sizes and with repeated concussion incidence are warranted to further delineate the effect of SRC and collar wearing on the behavioral and cognitive outcomes.
Footnotes
Acknowledgments
The authors would like to thank our outstanding collaborators and support staff that made this large-scale investigation possible. While it would be difficult to acknowledge all who contributed to the success of the project, there are those with specific contributions we would like to mention. At Cincinnati Children's Hospital Medical Center, we would like to thank faculty members Brian Coley, Charles Dumoulin, Kim Cecil, and Paul Gubanich; MRI technologists Lacey Haas, Brynne Williams, Matthew Lanier, Kaley Bridgewater, Elizabeth Fugate, and Marty Jones; MRI engineering and technical support Hui Wang, Zach Heeger, and Dennis Flage; staff members Staci Thomas, Sarah Orban, John Simon, Ryan MacPherson, Katie Kitchen, Katherine Kinsella, James Lynch, and Brooke Gadd. We also express our sincere gratitude to the University of Cincinnati medical student interns, Anna Saltman, Brent Waibel, Madeline Engeler, and Ramsey Sabbagh; undergraduate/graduate student interns from various universities, including Dan Braswell, Nicholas Slaboden, Emma Hansen, Ashley Doud, Lila Wright, Nicholas Zenger, Omar Brijawi, Austin Tiernan, Jennifer Shine, Sydney Hamilton, Saed Mustif, Bradley Jacobs, Enna Selmanovic, Kia Hreno, Emily Hornback, Meghan Swearingen, Kristen Jansen, Savannah Bacon, Nicole Veselitis, Samantha Simms, Cody McMillian, Daniel Riveros Molina, Morgan Froelich, Eric Schmitz, Jordan Maxwell, Philip Wienkamp, Teresa Rust, Courtney Johnson, Walker Engelhard, Kelsey Laizure, John Rizk, Victoria Colacicco, Megan Sloboda, Jessica Culbertson, Elizabeth Reddington, Dylan Kirby, Brady Tincher, Abby Odachowski, and Hima Devgan. Importantly, we want to acknowledge and thank student advisors Dan Carl and Susan Kotowski, who were critical to help manage and facilitate the student opportunities to participate on this project. We also express our thanks to the school athletic trainers Mike McCafferty, Craig Lindsey, Dan Forcum, Alex Popken, Katie Taylor, James Muncy, Nathalie Towchik, Alli King, Cindy Busse, Kayla Taske, Becky White, Rebecca Lemmel, Joe Lucas, Mike Gordon, Ken Rushford and Al Ducker; the school athletic directors Rob Heise, Mike Asbeck, Keith Pantling, Tony Hemmelgarn, Steve Ellison, Jan Wilking, Wendy Smith, Kim Gunning, Diane Redmond, Mark Schenkel, Eric Taylor, and Brian Reinhart; school coaches Mike Orlando, Doug Rosfeld, Patrick McLaughlin, Kevin Spraul, Gerry Beauchamp, Tino Mam, Aaron Hancock, Karen Wood, Marissa Wolf, Dave Ruehl, Keith Schaeper, Kiersten Johnson, Heather Vibberts, Mark Mueller, and Steve Spect; team physicians Dr. Stanfield, Dr. Kremcheck, Dr. Buerger, Dr. Argo, Dr. Rice, Dr. Altenau, Dr. Kevin Reilly, Dr. Eugene Reilly, Dr. Patrick Reilly, Dr. Noyes, Dr. Galloway, Dr. Cha, and Dr. Linz. We also express our thanks to Ed Lodge who helped with accelerometers and Jamison Float for neck collar fitting. Lastly, we express our appreciation to the football and soccer players and families from the high schools participating the study for being supportive of our mission to keep athletes safe during sport by engaging and participating in this research project.
Authors' Contributions
Weihong Yuan: Study concept and design; data processing, analysis, interpretation; drafting/revision of the manuscript.
Jed A. Diekfuss: Major role in the acquisition of data; data interpretation; revision of the manuscript.
Kim D. Barber Foss: Major role in the acquisition of data; data interpretation; revision of the manuscript.
Jonathan A. Dudley: Data processing and analysis; revision of the manuscript.
James L. Leach: Data interpretation; revision of the manuscript.
Megan E. Narad: Data analysis and interpretation; revision of the manuscript.
Chris DiCesare: Major role in the acquisition of data; data interpretation; revision of the manuscript.
Scott Bonnette: Major role in the acquisition of data; data interpretation; revision of the manuscript.
Jeffery N. Epstein: Data analysis and interpretation; revision of the manuscript.
Kelsey Logan: Data interpretation, revision of the manuscript.
Mekibib Altaye: Data processing; analysis, interpretation; revision of the manuscript.
Greg D. Myer: Study concept and design; data interpretation; revision of the manuscript.
Funding Information
Q30 Sports Innovations, LLC funded Cincinnati Children's Hospital Medical Center for the parent Clinical Trial testing the effects of the jugular vein compression on brain health outcomes.
Author Disclosure Statement
Weihong Yuan, Jed A. Diekfuss, Kim D. Barber Foss, Jonathan A. Dudley, James L. Leach, Megan E. Narad, Chris DiCesare, Scott Bonnette, Jeffery N. Epstein, Kelsey Logan, and Mekibib Altaye have no conflicts of interest to declare.
Gregory D. Myer has consulted with Q30 Innovations to support applications to the US Food and Drug Administration but has no financial interest in the commercialization of their products. Dr. Myer’s institution receives current and ongoing grant funding from National Institutes of Health/NIAMS Grants U01AR067997, R01 AR070474, R01AR055563, R01AR076153, R01 AR077248 and has received industry sponsored research funding related to brain injury prevention and assessment with Q30 Innovations, LLC, and ElMinda, Ltd. Dr. Myer receives author royalties from Human Kinetics and Wolters Kluwer. Dr. Myer is an inventor of biofeedback technologies (2017 Non Provisional Patent Pending- Augmented and Virtual reality for Sport Performance and Injury Prevention Application filed 11/10/2016 (62/420,119), Software Copyrighted.) designed to enhance rehabilitation and prevent injuries and has potential for future licensing royalties.
Supplementary Material
Supplementary Appendix Figure S1
Supplementary Appendix Figure S2
Supplementary Appendix Figure S3
Supplementary Appendix Figure S4
Supplementary Appendix Figure S5
Supplementary Appendix Figure S6
Supplementary Appendix Figure S7
Supplementary Appendix Figure S8
Supplementary Appendix Figure S9
Supplementary Appendix Figure S10
Supplementary Appendix Figure S11
Supplementary Appendix Table S1
Supplementary Appendix Table S2
Supplementary Appendix Table S3
Supplementary Appendix Table S4
Supplementary Appendix Table S5
Supplementary Appendix Table S6
Supplementary Appendix Table S7
Supplementary Appendix Table S8
Supplementary Appendix Table S9
Supplementary Appendix Table S10
Supplementary Appendix Table S11
Supplementary Appendix Table S12
Supplementary Appendix Table S13
Supplementary Appendix Table S14
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.