
Abstract
Civilian traumatic brain injury (TBI) guidelines recommend resuscitation of patients with hypotensive TBI with crystalloids. Increasing evidence, however, suggests that whole blood (WB) resuscitation may improve physiological and survival outcomes at lower resuscitation volumes, and potentially at a lower mean arterial blood pressure (MAP), than crystalloid after TBI and hemorrhagic shock (HS). The objective of this study was to assess whether WB resuscitation with two different MAP targets improved behavioral and histological outcomes compared with lactated Ringer's (LR) in a mouse model of TBI+HS. Anesthetized mice (n = 40) underwent controlled cortical impact (CCI) followed by HS (MAP = 25–27 mm Hg; 25 min) and were randomized to five groups for a 90 min resuscitation: LR with MAP target of 70 mm Hg (LR70), LR60, WB70, WB60, and monitored sham. Mice received a 20 mL/kg bolus of LR or autologous WB followed by LR boluses (10 mL/kg) every 5 min for MAP below target. Shed blood was reinfused after 90 min. Morris Water Maze testing was performed on days 14–20 post-injury. Mice were euthanized (21 d) to assess contusion and total brain volumes. Latency to find the hidden platform was greater versus sham for LR60 (p < 0.002) and WB70 (p < 0.007) but not LR70 or WB60. The WB resuscitation did not reduce contusion volume or brain tissue loss. The WB targeting a MAP of 60 mm Hg did not compromise function versus a 70 mm Hg target after CCI+HS, but further reduced fluid requirements (p < 0.03). Using LR, higher achieved MAP was associated with better behavioral performance (rho = -0.67, p = 0.028). Use of WB may allow lower MAP targets without compromising functional outcome, which could facilitate pre-hospital TBI resuscitation.
Introduction
Polytrauma and second insults adversely impact outcome after traumatic brain injury (TBI). Second insults are common—they occurred in 53% of patients with TBI transported by critical care air transport teams in the Iraq and Afghan wars. 1,2 In addition, hypotension occurs in up to 25% of patients with TBI necessitating intensive care; this is often caused by hemorrhage. The increased morbidity and mortality with post-TBI hypotension 1,2 may, in part, be related to insufficient cerebral blood flow relative to metabolic demands during the hypotensive episode when cerebral autoregulation may be impaired. 3,4 This makes optimization of early resuscitation crucial.
Current clinical practice in civilian trauma favors crystalloid resuscitation in patients with TBI, and the Brain Trauma Foundation (BTF) guidelines do not recommend the use of whole blood (WB). 5,6 This contrasts with the emerging use of fresh WB in hemorrhagic shock (HS) in some trauma centers, rather than the traditional use of large volumes of crystalloid and/or fractionated blood products. 7 –10 In military TBI resuscitation, The Joint Trauma System Current Tactical Combat Casualty Care Guidelines specify WB as the most preferred fluid for resuscitation of a patient with HS. 11 The Clinical Practice Guideline for prolonged field care of those with TBI also recommends WB transfusion to achieve hemodynamic stability. 12
The optimal blood pressure target during TBI resuscitation is also uncertain. The BTF guidelines recommend a systolic blood pressure >100–110 depending on patient age. 6 The guidelines also recommend a cerebral perfusion pressure (CPP) between 60 and 70 mm Hg and state that optimal CPP may depend on the patient's autoregulatory state. It remains unclear whether these targets differ during the acute resuscitation versus intensive care unit care or depending on the resuscitation fluid administered.
Previously, we reported that early WB versus lactated Ringer's (LR) resuscitation of TBI plus HS in mice markedly reduced resuscitation fluid requirements and improved multiple physiological parameters. 13 The WB resuscitation improved mean arterial blood pressure (MAP), brain tissue oxygenation (PbO2), and many blood chemistries. Even when the MAP resuscitation target was reduced from 70 mm Hg to 60 mm Hg, PbO2 was not compromised. That study, however, did not include behavioral or histopathological outcomes, key indicators of therapeutic translatability. If the MAP target for resuscitation of TBI plus HS or hypotension can be reduced below 70 mm Hg by using WB, then this could have a meaningful impact on how TBI resuscitation is performed. Indeed, studies addressing the optimal blood pressure targets for TBI resuscitation using different resuscitation fluids are limited.
Thus, we tested the following hypotheses in our mouse model of TBI plus HS: (1) WB mitigates behavioral deficits assessed over 21 days after injury versus LR; (2) WB resuscitation reduces contusion volume and overall brain tissue loss versus LR; (3) reducing the MAP target from 70 to 60 mm Hg worsens behavioral and histological outcomes in LR resuscitation; and (4) behavioral and histological outcomes are similar in WB resuscitated mice regardless of whether a MAP of 60 or 70 mm Hg is chosen.
Methods
Regulatory approval and animal care
The Institutional Animal Care and Use Committee of the University of Pittsburgh approved this study in accordance with the guidelines established by the National Institutes of Health in the Guide for the Care and Use of laboratory Animals. Adult (12–15-week-old), male C57BL/6J mice (n = 45) (Jackson Laboratories, Bar Harbor, ME) were given standard chow and water ad libitum and were group housed until injury, and single housed thereafter (12-h day-night cycles). Animal health and welfare were assessed at least daily by laboratory personnel and veterinary staff, and after injury animals were assessed daily by the surgeon to ensure that the animals regained catheterized limb function and did not have ischemic complications of catheterization.
Controlled Cortical Impact (CCI) and HS
Mice underwent our previously described murine model of CCI and severe HS (Fig. 1). 14 –16 This model simulates the clinically relevant scenario of moderate-severe TBI and comorbid HS seen in patients with polytrauma. It consists of CCI followed by an initial “shock” phase, a prolonged “pre-hospital” resuscitation, and a definitive-care “hospital” phase, outlined in greater detail in subsequent sections.

Experimental protocol. Intervals between black dots represent 5-min epochs from time of controlled cortical impact (CCI). Red dots represent times at which arterial blood gases and chemistries were withdrawn. Vertical dashed lines represent horizontal separation between protocol phases. After a pressure controlled (25–27 mm Hg) hemorrhagic shock, mice were first bolused with 20 mL/kg of either autologous whole blood (WB) or lactated Ringer's (LR). They were subsequently bolused with an additional 10 mL/kg of LR for mean arterial pressures (MAPs) below randomized target (60 or 70 mm Hg). Remaining shed blood from shock was reinfused in all animals after the pre-hospital phase.
Monitoring and initial injury
Mice were randomized to five groups (n = 8/group) before catheter insertion: initial LR resuscitation with MAP target 60 mm Hg (LR60), initial LR resuscitation with MAP target 70 mm Hg (LR70), initial WB resuscitation with MAP target 60 mm Hg (WB60), initial WB resuscitation with MAP target 70 mm Hg (WB70), or sham. Anesthesia was induced with 4% isoflurane in a gas mixture of 2:1 N2O:O2 (FiO2 = 0.33) and maintained with 1.5% isoflurane in that gas mixture for catheter insertion.
After inguinal cutdown and administration of local anesthesia (1% lidocaine hydrochloride, 0.1 mL), femoral venous and arterial catheters (modified PE-50 tubing) were inserted under sterile conditions. Mice were placed in a stereotactic frame (Kopf, Tujunga, CA), and a left scalp incision was made. A dental drill was used to make a 5-mm craniotomy over the left parietal cortex, and the bone flap was removed. A temperature probe (1-cm length, 0.33-mm diameter [Physitemp, Clifton, NJ]) was inserted in the left temporalis muscle to approximate brain temperature, which was maintained at 37.0 ± 0.5°C using a heat lamp. A rectal probe recorded body temperature. Isoflurane was reduced to 1% after catheter placement, and FiO2 was reduced to 0.21 for 10 min before CCI.
Sham mice had catheters inserted, were anesthetized and monitored as above, but did not undergo craniotomy, CCI, or HS. Mice were enrolled in the protocol until n = 8/group completed behavioral testing.
The CCI was performed with a pneumatic impactor (Bimba, Monee, IL) with a flat 3-mm tipped impounder on the left parietal cortex (velocity of 5 m/sec; depth of 1.2 mm). After CCI, the bone flap was replaced, and the skin was sutured closed with local analgesia provided at the time of skin closure (0.25% Sensorcaine/bupivacaine, 0.1 mL). At 5 min after CCI, mice began the “shock” phase of our model. Blood (12 mL/kg of body weight) was removed manually over 5 min via venous canula into a tuberculin syringe containing 0.07 mL of citrate anticoagulant (Cardian BCT, Lakewood, CO). An additional 12 mL/kg of venous blood was removed over 5–15 min into the same syringe, for a total blood loss of ∼30% of mouse blood volume.
The MAP was maintained at 25–27 mm Hg for the 35 min “shock” phase, initiated at the start of blood removal, by continued removal and/or reinfusion of 0.05 mL aliquots between the citrated syringe and the venous catheter. Blood was kept at room temperature between removal and reinfusion in either the pre-hospital or hospital phase. During shock, anesthetic was decreased from 1% isoflurane in room air to 0.5% isoflurane in room air.
Pre-hospital and hospital resuscitation
After shock, mice received an initial 20 mL/kg bolus of autologous WB or LR depending on randomized treatment. The surgeon could not be blinded to treatment given the immediate difference in MAP response between LR and WB resuscitation. All mice received 10 mL/kg boluses of LR every 5 min for MAP below target, for up to 170 mL/kg of additional LR. After the 90 min pre-hospital phase, mice entered a 15 min hospital phase where remaining shed blood was reinfused and anesthetic was increased to 1% isoflurane in 100% oxygen to mimic the resuscitation of a severe TBI victim with polytrauma and HS.
Physiological outcomes
The MAP was recorded every 5 min throughout the experiment. Arterial blood gases and chemistries were measured pre-injury and after each of the three injury phases. Total LR volume administered subsequent to the initial bolus was tabulated.
Morris Water Maze (MWM) testing
We used the MWM hidden platform task on post-injury days 14–18 to assess spatial learning, followed by probe trial as described previously. 16 Performance in the MWM was quantified by daily latency to locate a hidden platform, and the probe trial was quantified as percent time in the target quadrant. Visible platform testing on days 19–20 after TBI confirmed that latencies were not confounded by visual impairments. All behavioral testing was performed by research technicians blind to treatment and injury status.
Volumetrical analyses
Isoflurane anesthetized mice were euthanized 21 days after injury by thoracotomy, left ventricular cannulation, and heparinized saline/10% buffered formalin solution perfusion until atrial outflow cleared, followed by decapitation. Brains were extracted, the cerebellum and brainstem were removed, and 10-mm coronal frozen sections were cut on a cryostat at 0.5-mm intervals. Sections were stained with hematoxylin and eosin, and per slice contusion area and ipsilateral and contralateral hemisphere areas were quantified using MCID Elite Software (MCID Imaging Research, St. Catharines, ON) by technicians blind to experimental group status.
Per previously published methods, slice volumes were calculated by multiplying per slice area by slice interval thickness. 14 Slice volumes were summed to calculate contusion volume and right and left hemisphere volumes. Hemisphere volumes were summed to obtain remaining brain volume.
Statistical analysis
Based on previous experiments, we expected cumulative MWM latency to increase from approximately 100 sec in the sham group to 200 sec in the LR70 group, with a standard deviation (SD) of approximately 10 sec. 14 Because our previous report suggested that WB60 resuscitated mice had the lowest brain edema, lowest fluid requirements, and double the PbO2 as LR70, 13 we hypothesized that this group would likely have the best performance in MWM, with intermediate latencies for WB70 and LR60 based on LR requirements and PbO2. Assuming that WB60 could reduce the latency deficit by 75 sec (75%), then n = 8 mice/group would give 80% power to detect a statistically significant (a = 0.05) marginal difference between LR70 and WB60 mice in post hoc testing.
Body weight, mean MAP, LR volume post-initial bolus, and blood chemistries data are presented as mean ± SD. Other parameters were compared using one-way analysis of variance (ANOVA), with post hoc comparisons performed with two-tailed Student t test. Between-group differences in MAP throughout the pre-hospital period were assessed by random coefficient linear mixed models (LMM). The LMM results are presented as b coefficients. The MWM data were assessed by repeated measures ANOVA and presented as mean ± standard error of the mean.
Sham mice were excluded from ANOVA comparisons of average MAP per period, but were included in the LMM of MAP over time. Volumetric data were not normally distributed and are presented as median and interquartile range. The Tukey test was used for post hoc comparisons. All p values are adjusted, and a = 0.05. Analysis was performed using Stata 16.1 (StataCorp, College Station, TX).
Results
A total of 45 mice underwent surgical procedures to achieve n = 8 mice/group for completion of behavioral testing—one LR70 mouse died during shock and was not analyzed. One mouse each from LR60 and LR70 and two mice from WB70 died between injury and behavioral testing. Physiological parameters, body weight, hematology, and chemistries were assessed in these mice, but behavior and histology were not. Body weights did not differ between groups (Table 1).
Physiological Characterization of Sham, Lactated Ringer's, and Whole Blood Resuscitated Mice
LR, Lactated Ringer's; WB, whole blood; ANOVA, analysis of variance; SD, standard deviation; MAP, mean arterial pressure; HS, hemorrhagic shock; Hgb, Hemoglobin.
LRx, lactated Ringer's resuscitation, MAP target X; WBx, whole blood resuscitation, MAP target X.
ANOVA excluded sham group.
Physiology
Pre-hospital LR requirements were highest in LR70, followed by LR60, WB70, and then WB60 (Fig. 2A). All differences were significant (p < 0.05). All groups had similar MAPs at baseline and during the shock period (except sham, Fig. 2B). The MAPs in the two LR resuscitated groups did not differ significantly from one another during the pre-hospital phase (b = 1.95, p = 1.00), but were lower than MAPs in WB groups (p < 0.01, all comparisons). The MAP in WB70 was higher than in WB60 (b = 3.86, p = 0.03). The MAP in sham mice remained higher versus other groups during the pre-hospital and hospital phases (p < 0.05, all comparisons), but MAP in the four TBI groups equalized in the hospital phase (Table 1, Fig. 2B).
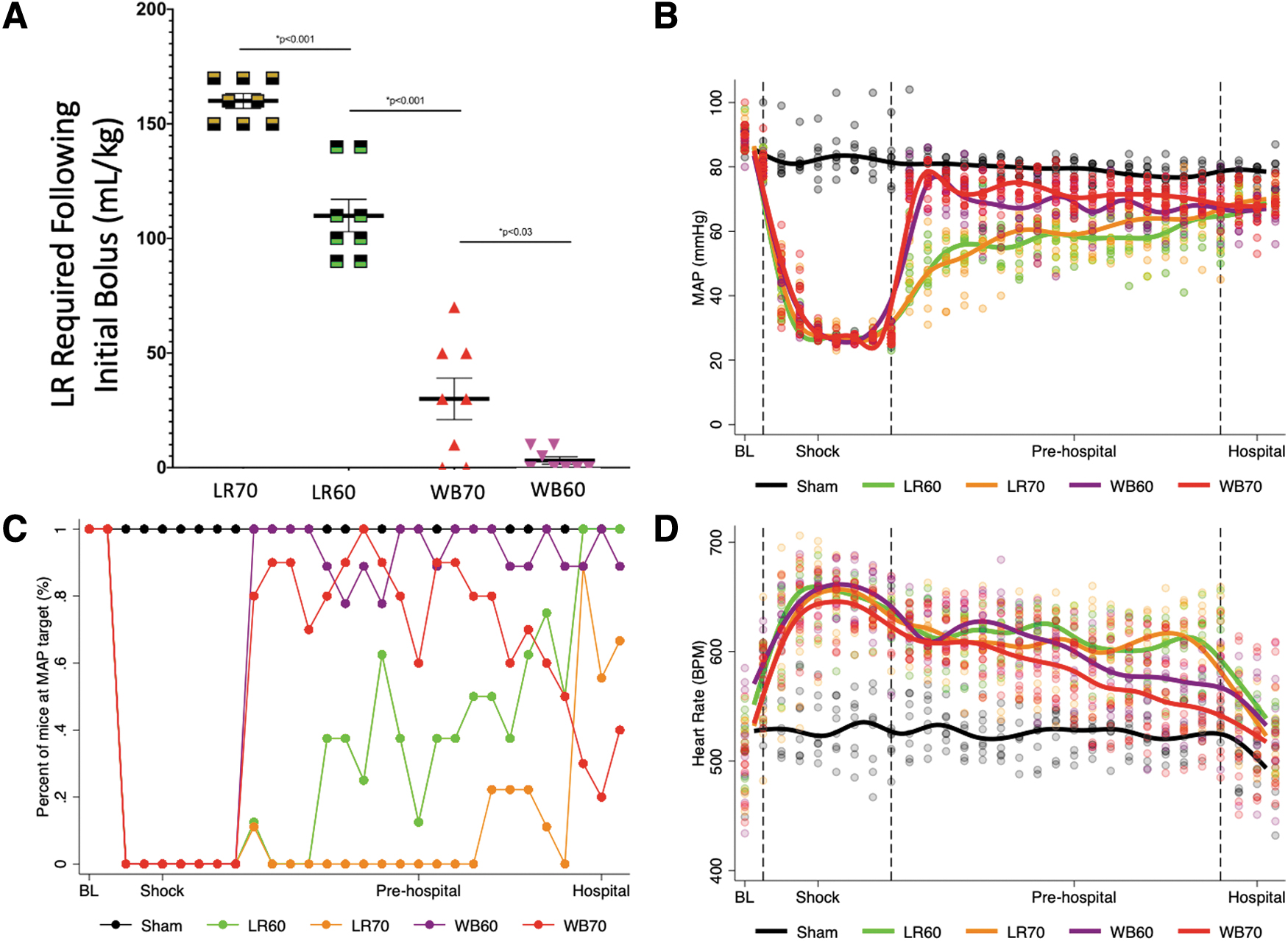
Whole blood (Wreduces crystalloid volume infused and rapidly normalizes mean arterial pressure (MAP). (
Figure 2C demonstrates the proportion of mice reaching their MAP target per 5-min epoch: while an increasing proportion of LR60 mice met their target over the resuscitation period, the same was not true for LR70 mice, where consistently few mice met target. Similarly, MAP target was achieved at all time points in almost all WB60 mice, but a decreasing proportion of WB70 mice as the procedure went on. Heart rate was faster in all injured groups than in sham injured animals (Fig. 2D). While heart rate began to recover toward baseline during the pre-hospital phase in WB resuscitated mice, it did not do so until reinfusion of blood in the hospital phase in LR resuscitated mice (Fig. 2D).
Arterial blood gases and chemistries
Early WB resuscitation rapidly normalized multiple blood gases and chemistries after combined TBI and HS versus LR including hemoglobin, sodium, ionized calcium, lactate, and blood osmolality (Supplementary Table S1).
MWM testing
When MWM latency to platform was compared across groups, shams performed better than both LR60 and WB70 (Fig. 3A, p < 0.05), but not LR70 (p > 0.10) or WB60 (p > 0.10). In pairwise comparisons (Fig. 3B,C), there was a trend to decreased latency in LR70 versus LR60 mice, although this was not significant after Tukey adjustment (p = 0.08). The WB70 and WB60 resuscitated mice performed similarly (p > 0.10).
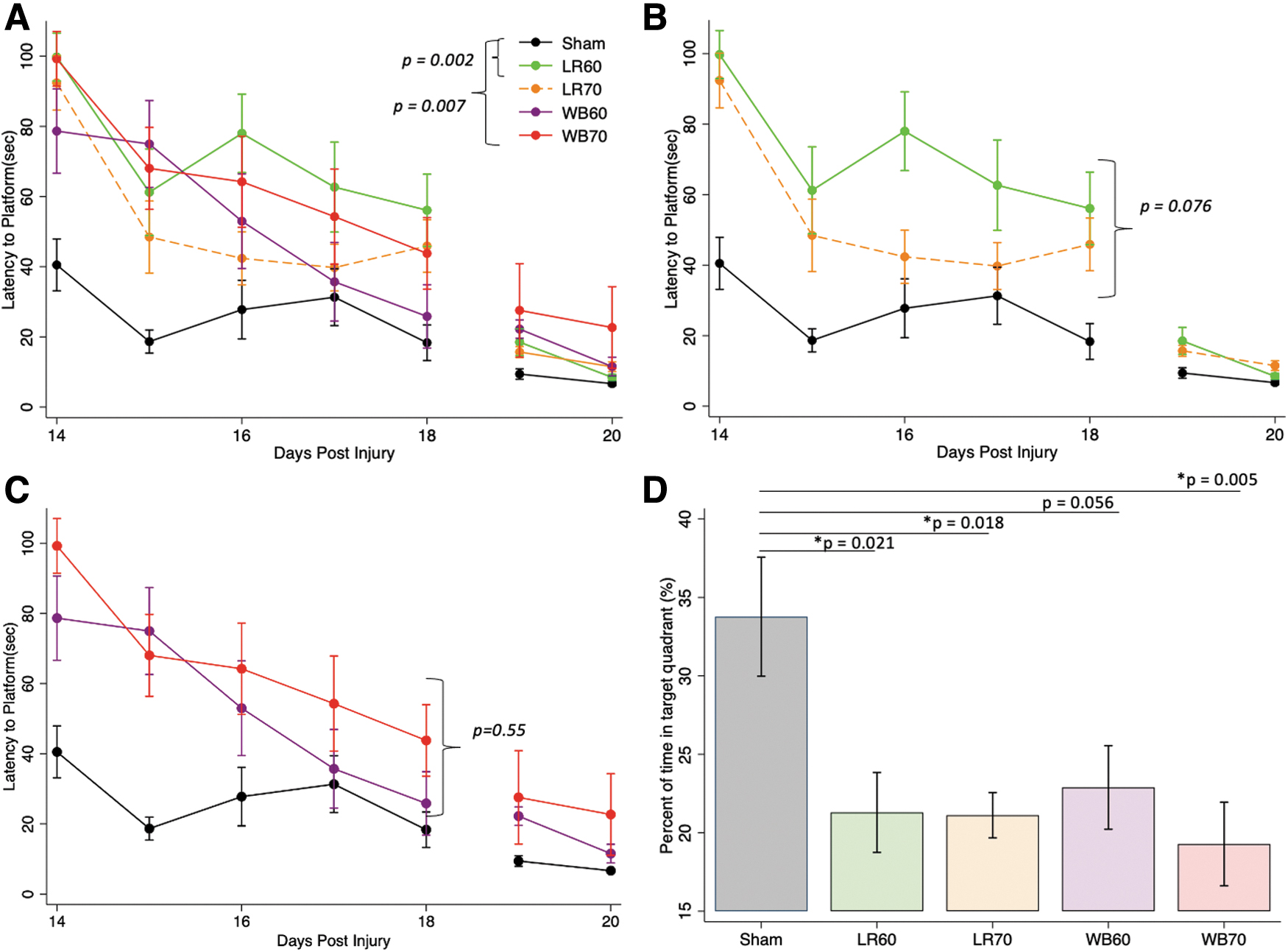
Whole blood (WB) resuscitation to a mean arterial pressure (MAP) of 60 mm Hg ameliorates behavioral deficits after traumatic brain injury plus hemorrhagic shock. (
In the probe trial, sham mice outperformed (p < 0.05) all groups except WB60 (Fig. 3D), although there was a trend toward more time in the target quadrant versus WB60 (p = 0.056). Performance in the probe trial was similar in all injured groups.
Contusion and remaining brain volume
Contusion volumes were similar across resuscitation groups (Fig. 4A). Whole brain volume at euthanasia was significantly higher in sham than in any of the injured groups (p < 0.01, all comparisons), with no differences between injured groups (Fig. 4B). Representative examples of hematoxylin and eosin-stained sections through the lesion from each treatment group are provided in Supplementary Fig. S1.

Neither whole blood (WB) resuscitation nor lactated Ringer's (LR) resuscitation reduced tissue loss after traumatic brain injury plus hemorrhagic shock. (
Correlational analyses of MAP and behavioral outcome
The average MWM value across the five days of testing has been consistently used as a metric of overall MWM performance in our previous studies. 16,19 –25 Thus, we assessed the correlations between the average MAP during resuscitation and average latency across the five days of MWM testing for each mouse in each of the post-TBI treatment groups. A significant negative correlation was observed between average MAP during resuscitation and average MWM latency (Spearman rho -0.67, p = 0.028) indicating that higher MAP values are associated with favorable cognitive outcome when LR was used (Fig. 5). In contrast, the correlation between average MAP during resuscitation and average MWM latency was not significant for mice resuscitated with WB (Spearman rho 0.10, p > 0.10, Fig. 5).
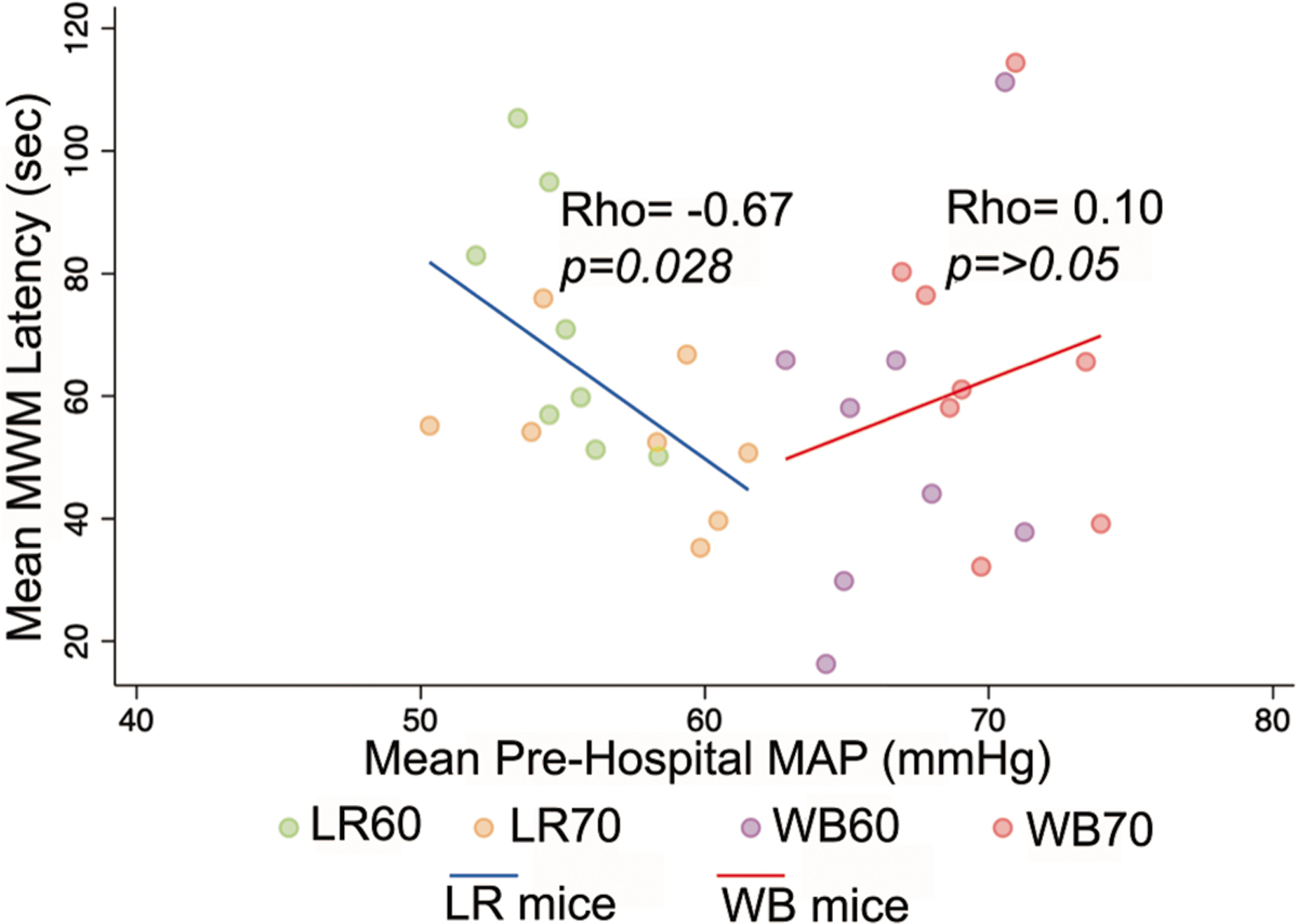
Correlation between average mean arterial blood pressure (MAP) during resuscitation and average Morris Water Maze (MWM) latency in mice resuscitation with lactated Ringer's (LR) solution or whole blood (WB) after traumatic brain injury plus hemorrhagic shock. A significant negative correlation was observed between average MAP during resuscitation and average MWM latency over the five days of hidden platform testing (Spearman rho -0.67, [blue line] p = 0.028) indicating that higher MAP values are associated with favorable cognitive outcome when LR (green and orange circles) was used. In contrast, the correlation between average MAP during resuscitation and average MWM latency was not significant for mice resuscitation with WB (Spearman rho 0.10, p = 0.42) (purple and red circles).
Discussion
Our study provides early evidence that the relationship between MAP target and functional outcome may be modified by the choice of resuscitation fluid. After TBI plus HS, behavioral outcome in mice resuscitated with WB targeting a MAP of 60 mm Hg or LR targeting a MAP of 70 mm Hg did not differ from sham, contrasting more pronounced MWM deficits seen with WB70 and LR60.
There were four major findings. (1) When WB was used, a MAP target of 60 mm Hg outperformed 70 mm Hg in fluid requirement without compromising behavioral outcome. (2) When LR was used, MWM performance was positively correlated with MAP during resuscitation, but this was not the case with WB. (3) WB resuscitation to target MAP of 70 mm Hg did not outperform LR at the same MAP target. (4) Resuscitation strategy did not have a significant effect on brain tissue loss or contusion volume.
Optimized resuscitation with WB after TBI plus HS
The WB resuscitation to target MAP of 60 mm Hg necessitated the least resuscitation fluid without any evidence of behavioral compromise. In our previous report examining PbO2 levels and brain edema in separate mice using an identical injury and treatment protocol, the WB60 group reached the same brain oxygenation levels during resuscitation as WB70, with both groups having significantly higher PbtO2 than LR resuscitated mice. 13 The WB60 group also had lowest brain water content at 3 h post-injury.
Thus, our behavioral outcomes are consistent with the observed physiology. This suggests that a lower MAP target was not only tolerated, but surprisingly favored using WB resuscitation. Despite a significant positive correlation between MAP during resuscitation and favorable MWM performance in mice treated with LR, a higher MAP was not correlated with better cognitive outcome in WB treated mice; indeed the trend was in the opposite direction (Fig. 5).
While previous studies have demonstrated that WB resuscitation improves mortality and crude neurologic outcomes after combined injury, ours is the first to demonstrate that it may allow for lower MAPs than currently targeted without compromising outcomes. Although we did not measure intracranial pressure (ICP) in this study, we previously reported that ICP is near zero early in the HS phase in our model, and gradually rises to ∼15 mm Hg by the end of the resuscitation. 17 Thus, the CPP achieved using WB during resuscitation would be expected to be between 65 (early) and 50 mm Hg (late).
This suggests the intriguing possibility that acute resuscitation of TBI plus HS with WB may allow for safe, or even optimal, use of lower MAP/CPP targets—or that lower MAP targets should be studied in pre-clinical models and clinical TBI resuscitation when WB is used. This could be particularly important for TBI in austere environments, or complicated by penetrating bodily trauma, where a lower extra-cerebral MAP target may be desirable.
This finding could have several potential explanations. Rapidly normalizing MAP with WB early after CCI could theoretically acutely expand the contusion—at a time when it may still be perfused despite severe blood–brain barrier disruption. That could counteract any histological benefit produced by a reduction in ischemia by WB in the pericontusional regions. Our WB70 group numerically had the largest contusion volumes, although not statistically different from WB60.
A previous study found a U-shaped curve for the effect of cerebral perfusion pressure on contusion volume after CCI, supporting the notion that a higher MAP might be detrimental. 18 Similarly, a study in rats found that WB resuscitation at a MAP of 80 mm Hg after contusional TBI and HS was superior to 100 or 120 mm Hg. 19 A larger sample size is needed to appropriately test this hypothesis in our model. Whether optimal MAP with WB resuscitation after TBI and HS is influenced by the TBI endophenotype (i.e., contusion vs. diffuse injury) merits further study both in pre-clinical models and in patients.
Optimized MAP target with lactated Ringer's resuscitation
Contrasting the findings with WB, LR mice had greater behavioral impairment with lower MAP. Our model illustrates the classically described reduced tolerance to HS after TBI and MAP refractory to crystalloid administration. 20 –23 This has been suggested to result from loss of sympathetic tone and systemic vascular control and results in the need for substantial crystalloid usage. In our study, >160 mL/kg and >120 mL/kg of LR were required in the LR70 and LR60 groups, respectively. Despite those large resuscitation volumes, MAP did not consistently reach/maintain target in either group.
In our previous report, PbO2 was lower in both LR versus WB groups, although PbO2 and edema did not differ between LR groups. In our current study, however, targeting a higher MAP when using LR improved behavioral outcomes, although this did not translate into a histological benefit. Examination of hippocampal neuron counts in CA1, CA3, dentate, and hilus, however, should be performed in future studies, because those selectively vulnerable regions might more readily show differences than contusion volume or tissue volumes—particularly given that MWM performance can be hippocampally mediated.
Contrasting our findings, a previous study of TBI and HS in rats reported that resuscitation with 10 mL/kg/h of LR resulted in better Neurological Severity Scores (NSS) at 24 h versus resuscitation with 40 mL/kg/h of LR. 24 That study, however, used the dynamic cortical deformation model, which applies a negative pressure vacuum suction to the cortex, rather than CCI, and could represent a very different pathobiology. The NSS also does not assess cognitive function.
Choice of resuscitation fluid for TBI plus HS
Overall, our study suggests that early resuscitation with WB may outperform LR in this model, but that the MAP target may be important in maximizing benefit. The WB to a target MAP of 60 mm Hg reduced resuscitation fluid requirements versus all strategies, without compromise of either behavioral or histological outcomes, and, taken together with our previous report, 13 optimized PbO2 and limited brain edema. The rapid MAP improvement seen with WB is likely multi-factorial, potentially related to colloid properties of blood, proendothelial/glycocalyx properties of blood product administration, and possible other factors. 25,26
Clinical studies guiding blood product administration in TBI are largely observational. 27 –30 One randomized controlled trial found that a 10 mg/dL hemoglobin transfusion threshold did not improve outcomes versus 7 mg/dL, but did not specifically enroll hemodynamically unstable or bleeding patients. 31 In trauma patients with HS, transfusion of red blood cells, plasma, and platelets at a fixed ratio is standard of care, with lowest death at a 1:1:1 ratio. 32 –34 Even this, however, results in nonphysiological replacement. 34 Thus, there is increasing interest in fresh WB for trauma patients in HS. 7,10,35 –39 A trial comparing WB to component therapy, however, found that WB reduced transfusion requirements only in nonhead-injured patients, 7 suggesting no benefit of WB resuscitation in patients with TBI. 10
Our pre-clinical data comparing WB to crystalloid in TBI resuscitation favor WB and are consistent with a previous report showing that WB resuscitation mitigates NSS after TBI plus HS. 40 The Shock, WB, and Assessment of TBI (LITES TO 2 [SWAT]) study (NCT03402035) is an ongoing prospective cohort study of WB resuscitation in traumatic hemorrhage patients with and without TBI; we await those results. Our data also highlight the need to study carefully targeted blood pressures when WB is used in clinical TBI resuscitation.
Strengths and limitations
Randomization reduced possible selection and allocation biases. Similarly, separate assessors of behavioral and histological outcomes, all of whom were blinded to treatment and injury status, reduced the probability of biased outcome assessment. Using an identical insult protocol and treatment groups as in our previous report on physiological effects of WB versus LR resuscitation allowed us to build on those findings, providing insight into the effects on neurobehavioral and neuropathological outcomes.
Our study has several limitations. One of our primary limitations is our relatively small sample size, with only eight mice completing the protocol per group; this underpowered our ability to detect modest differences, which may be the reason we found no significant differences between WB60 and sham behaviorally. Given the marked benefit of WB that we observed versus LR on the physiological outcomes that we assessed in our previous report using this exact protocol, we anticipated greater effects on behavior and powered the study on that basis. 13 This model, however, is highly complex, data-rich in the acute phase, and this work is one of the larger studies using this model and coupling it to long-term behavior. 13 –15,17,41 –44
Although mice were randomized to treatment groups and behavior and histology were assessed by technicians blind to group assignment, the time of randomization was such that the surgeon was aware of the group assignment at the time of injury, potentially allowing for bias at this time. Also, the magnitude of the difference in blood pressure response to WB versus LR, which has previously been established in multiple studies in this model, further limits the ability to blind the surgeon during resuscitation. Another limitation was that without a control group that did not receive catheters, we could not separate out possible effects of catheter placement on swim speed and MWM performance.
By transfusing recently shed, autologous blood, we bypassed concerns associated with cold-stored WB, 8 including transfusion reactions, storage lesions, and different lifespans of the components. 34 We did not target a pre-defined hemoglobin value, instead transfusing a fixed volume, preventing assessment of a dose-response. Resuscitation of those with acute hemorrhage, however, is not guided by hemoglobin clinically.
Similarly, because we gave fixed volume LR boluses for MAP below target, LR resuscitated mice received crystalloid volumes higher than what is often given clinically in the pre-hospital period. Despite this, pressors are not always available in the pre-hospital setting, and, if blood products are not available, then high-volume crystalloid may be used as a temporizing measure until a bleeding patient with severe TBI can reach definitive care. We also did not find adverse behavioral effects associated with these high volumes of LR, instead finding improved behavior associated with higher achieved MAPs.
Relatedly, because there was little to no overlap in MAPs achieved in WB versus LR resuscitated mice, it is difficult to know whether lack of improvement with higher MAP in WB is because of MAP >65 mm Hg having limited benefit after TBI + HS or if this phenomenon is intrinsically related to WB resuscitation.
Another limitation is that our study only assessed male animals, and both physiology and response to treatment may be different in males versus females. Including female mice would have added another layer of heterogeneity to the study, further reducing our power. Studying optimal resuscitation targets in females, however, where the baseline MAP and predisposition to injury may be different, is needed for full clinical translation.
Our study was limited by using LR for early resuscitation versus physiologic saline, which is likely superior to LR in TBI. 45,46 Current combat casualty care guidelines, however, recommend balanced crystalloid over physiologic saline for patients in HS when blood products or colloids are unavailable. 47 Balanced fluids like LR are recommended for other trauma patients, and the presence of TBI is often unclear. 48 Future studies should compare early WB resuscitation to NS in TBI plus HS. Finally, we recognize that using LR, the MAP targets were not consistently achieved and/or maintained during the resuscitation despite an aggressive approach to fluid administration. That scenario, however, is often encountered clinically, and the use of pressor agents is uncommon in pre-hospital care.
Conclusion
Low volume WB resuscitation blunted behavioral deficits in mice after TBI and HS versus LR resuscitation. This was evident even in mice that did not reach a MAP of 70 mm Hg, the current MAP floor recommended in TBI, with no correlation between achieved MAP and behavior. Surprisingly, with WB, the lower MAP target may outperform the higher MAP target of 70 mm Hg. In contrast, higher MAPs were associated with improved outcome when LR was used. Whether use of WB allows even lower MAPs deserves further study in the setting of TBI plus HS.
Footnotes
Acknowledgments
We thank Marci Provins for assisting in manuscript preparation and Linda T. Ryan for administrative support.
Material has been reviewed by the Walter Reed Army Institute of Research. There is no objection to its presentation and/or publication. The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or as reflecting true views of the Department of the Army, Uniformed Services University of the Health Sciences, the Department of Defense, or any other agency of the U.S. Government.
Authors' Contributions
All authors were involved in the conception or design of the work, critical revision of the article, and final approval. Benjamin E. Zusman, C. Edward Dixon, Ruchira M. Jha, Vincent Vagni, Jeremy Henchir, Keri L. Janesko-Feldman, and Patrick M. Kochanek were involved in data collection, analysis, and interpretation, and in drafting the article.
Funding Information
We would like to thank the DoD (W81XWH-17-C-006) for generous support. We also thank NIH NINDS (K23NS101036, R01NS115815 to R.M.J).
Authors' Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.