
Abstract
Traumatic acute subdural hematoma (aSDH) is associated with a high mortality rate caused by post-operative cerebral infarction. Recently, brain natriuretic peptide (BNP) was considered a reliable biomarker in the acute phase of traumatic brain injuries. We therefore aimed in this study to analyze BNP levels on admission, identify the predictors of their elevation, and assess the relationship between BNP and the risk of post-operative cerebral infarction. Patients with isolated, unilateral, traumatic aSDH who were admitted to our department between July 2017 and May 2020 were enrolled in this study. On admission, cranial computer tomography (CCT) and BNP sampling were simultaneously performed. Additionally, the time between head trauma and BNP sampling (TTS) was assessed. Admission radiographic variables included hematoma volumes, midline shift, and degree of brain edema. Cerebral infarction was detected on postoperative CCT. In total, 130 patients were included in this study. Surgical treatment was performed in 82.3% (n = 107) of cases. The multiple regression analysis showed that larger hematoma volumes (p = 0.032) and advanced age (p = 0.005) were independent predictors of elevated BNP when TTS <24 h. The binomial logistical regression analysis identified BNP with a cutoff value of <29.4 pg/mL (TTS = 3–12 h, adjusted odds ratio [aOR] = 16.5, p = 0.023) as an independent predictor of post-operative cerebral infarction. Elevated BNP levels in the first 24 h post-trauma were related to larger hematoma volumes and advanced age. Further, an increased risk of post-operative cerebral infarction was identified in patients with lower BNP levels in the post-traumatic period 3–12 h.
Introduction
Traumatic acute subdural hematoma (aSDH) is the most common mass lesion in severe traumatic brain injury (TBI), 1,2 which is often complicated by the co-occurrence of diffuse injuries. Recently, brain natriuretic peptide (BNP) was considered a reliable biomarker in the acute phase of TBI. BNP is a peptide-structured neurohormone, which can be rapidly synthesized by cardiomyocytes in large quantities, and released in response to volume or pressure overloads. 3 BNP is a widely available, rapidly processed, and inexpensive biomarker whose elevation correlates with the severity of the trauma, 4 elevated intracranial pressure (ICP), 5 and poor outcomes. 6 However, the clinical and predictive value of BNP concentrations on admission in the setting of traumatic aSDH as well as their relationship with the initial radiological findings have not yet been addressed.
Because of its complicated pathophysiology, traumatic aSDH still carries the highest mortality rate among comatose patients with TBI, ranging between 60% and 90%. 7 –9 This high mortality rate has previously been attributed to the primary brain damage that often accompanies aSDH. 10 However, post-mortem studies have suggested that ischemic brain damage is the most common neuropathological finding among aSDH patients, which occurs more frequently in TBI with aSDH than in TBI without aSDH. 11 Cerebral infarction is the leading pathophysiological mechanism associated with the development of secondary brain damage following traumatic aSDH, 12 and plays an important role in the high mortality rate. 13 However, cerebral infarction is infrequently addressed in a systematic manner in the clinical setting. 14 Ischemia-reperfusion injuries are complex and multifactorial processes. 15 Disturbances in cerebral blood flow (CBF) autoregulation during surgery may initiate reperfusion injury, 16 in which ischemia-induced cellular dysfunction is followed by reperfusion-induced free radical production, 17,18 and the peak of neuronal injury typically occurs during the early reperfusion phase of aSDH. 19
During the last two decades, several studies have reported on the role played by BNP in the prediction of acute ischemic stroke (AIS) severity and outcomes. 20 –33 BNP has been demonstrated to be an important tool for guiding the management of AIS. 28 However, only a few studies have examined the role played by BNP in the prediction of AIS risk in healthy individuals, 34,35 and the role of BNP in the prediction of the risk of cerebral infarction following surgical treatment in brain injured individuals with aSDH has not yet been addressed.
Therefore, the aim of the present study was to analyze BNP serum levels on admission, assess their variability with regards to the exact time of head trauma, and identify the radiological predictors of their elevation. Moreover, we investigated the relationship between BNP and the risk of cerebral infarction following surgical treatment for traumatic aSDH.
Methods
Study participants
Between July 2017 and May 2020, 165 patients ≥18 years of age with isolated unilateral aSDH who were admitted to our institution were evaluated for study eligibility. Patients with a history of chronic cardiac or renal failure, brain surgery, or intracranial tumor, and patients who presented with a bilateral or interhemispheric aSDH, an aneurysmal subarachnoid hemorrhage, or a non-traumatic aSDH were excluded from the study. The study flow chart summarizes the main exclusion criteria in detail (Fig. 1). This prospective study was performed in accordance with the Declaration of Helsinki and the ethical standards of the institutional review board that approved this study (Medical Faculty, University of Duisburg-Essen, Registration number: 15-6632-BO). Written informed consent was obtained from the patients, or in cases of altered states of consciousness, from the next of kin. All supporting data are available within the article and associated online supplementary files.

Study flow chart.
Data management
The primary end-points of the study were: The analysis of BNP serum levels on admission The assessment of their variability with regards to the exact time of head trauma The identification of the radiological predictors of their elevation
The secondary end-point of the study was the investigation of the relationship between BNP and the risk of post-operative cerebral infarction.
Routine care and treatment protocol for traumatic aSDH
According to local policy, all patients were neurologically assessed on admission and underwent cranial computer tomography (CCT). Additionally, a cranial and cervical CT-angiography were performed to rule out/diagnose any vascular abnormalities (stenosis, dissection). Patients with a Glasgow Coma Scale (GCS) score <15 or the presence of a midline shift (MLS) received an immediate hematoma evacuation under general anesthesia with a decompressive craniectomy or craniotomy, depending on presence of brain edema. Prior to surgery, a single dose of cefazolin was administrated prophylactically. Post-operatively, patients spent at least 24 h in the intensive care unit and remained on bed rest. A postoperative CCT was performed in all cases to rule out a secondary bleeding. Patients with a GCS score of 15 without MLS were neurologically monitored for 24 h in the ICU, then received a control CCT 6 h after the first imaging, or in response to neurological deterioration. Patients with initially non-reactive and wide pupils for >2 h were not operated on because of worse prognosis. Pre-existing antiplatelet/anticoagulant therapy (AAT) was discontinued upon hospital admission and re-established 3 weeks after surgery, in cases of complete hematoma resolution.
BNP sample collection
In all patients, BNP was assessed on admission (3–5 min before the initial CCT) by electrochemiluminescence immunoassay (Siemens, ADVIA Centauer®, USA). The detection range provided by the manufacturer was 2 − 5000 pg/mL.
Patient data collection
Patients' characteristics were prospectively assessed by the first author (M.C.) using a study questionnaire, which included age, sex, and comorbidities, such as cardiac history (atrial fibrillation [AF] and coronary heart disease [CHD]), AAT, and the presence of dementia. Patients' neurological conditions on admission were also assessed, using the GCS score and pupils' size and their reaction to light (medium-sized reactive pupils vs. anisocoria with wide non-reactive pupil ipsilaterally to the aSDH vs. wide non-reactive pupils). Further, the exact time at which head trauma and BNP sampling occurred was prospectively documented, and the time between head trauma and BNP sampling (TTS) was calculated in minutes, then split into five categories (< 3 h, 3–6 h, 6–12 h, 12–24 h, and >24 h [median: 43.6 h]). Among the surgically treated cohort, the occurrence of post-operative complications such as re-bleeding, cerebral infarction, early post-operative seizures, myocardial infarction, cardiac arrest, acute renal failure, and sepsis was assessed during the hospital stay.
Definition of post-operative cerebral infarction
Cerebral infarction after surgical treatment was defined as a focal hypodensity ± sulcal effacement on non-contrast CCT, which was diagnosed following the occurrence of a new post-operative neurological deficit, and did not regress on the final control CCT before discharge.
Radiographic measurements
Hematoma volume on the initial CCT was measured in all patients using computer-assisted volumetric analysis. Hematoma volume margins were traced using iPlan Software (BrainLab, Munich, Germany) on each axial CT slice, and the volume was automatically calculated by the software in cubic centimeter (equivalent to milliliter [mL]). MLS was measured in millimeter (mm) at the level of the insular cortex, in a slice showing the basal ganglia and the thalamus above the basal cisterns. The midline was traced vertically from the frontal crest to the internal occipital crest. A perpendicular horizontal line was traced from the septum pellucidum to the midline, and this distance was considered to be the MLS. Early brain edema was assessed using the Subarachnoid Hemorrhage Early Brain Edema Score (SEBES), 36 then dichotomized into no/mild edema (SEBES ≤2) and severe edema (SEBES >2).
Statistical analyses
All analyses were performed using IBM SPSS Statistics version 25, for Windows (Chicago, IL, USA). Categorical data are presented as the frequency and percentage. Non-normal distributed continuous variables are expressed as the median and interquartile range (IQR). The Mann–Whitney U test was used to determine differences between two groups of a categorical variable on non-normally distributed continuous variables (i.e., BNP). Associations between categorical variables were determined using the χ 2 test or Fisher's exact test (when the expected cell frequency was <5). The Kruskal–Wallis Test was used to determine an association between an ordinal variable (TTS) and a continuous variable (BNP). In the case of two continuous variables, the Spearman rank correlation was used. Factors found to be significantly associated with BNP and cerebral infarction during the univariate analyses with p values <0.1, were included in the multivariate analyses. Multiple regression and binomial logistical regression were used to determine the predictors of elevated BNP and the risk of cerebral infarction following surgery, respectively. In the binomial logistical regression, an adjusted odds ratio (aOR) and 95% confidence intervals (95% CI) were calculated for each predictor. A receiver operating characteristic (ROC) curve analysis was conducted to determine the cutoff value for BNP to predict the risk of cerebral infarction. P values <0.05 in two-sided testing were considered significant.
Results
Patients' characteristics and post-operative complications
In total, 130 patients (median age: 74.5 years, IQR: 28 years, female/male: 1.5/1) were enrolled in the study. Surgical treatment was performed in 82.3% (n = 107) of cases, 14.6% (n = 19) were conservatively treated, and only 3.1% (n = 4) were not operated on because of worse prognosis (Fig. 1). Female patients were significantly older than male patients (median age: 81 vs. 63 years, respectively, p = 0.0005). Head trauma under the influence of alcohol occurred significantly more frequently in younger individuals (median age: 52 vs. 78 years, p = 0.0005). Supplementary Table S1 summarizes all patient characteristics and post-operative complications in detail.
Relationship between BNP and TTS
Higher BNP was significantly associated with longer TTS (p < 0.001). Figure 2 shows a consistent increase in median BNP with a period of stagnation when TTS ranged from 3 to 12 h (medians: 58.9–72.6 pg/mL).

Relationship between brain natriuretic peptide levels (BNP) and the time between head trauma and BNP sampling (TTS).
Relationship between BNP and radiographic findings
On initial CCT, larger hematoma volumes were significantly associated with a higher BNP (p < 0.01). In contrast, MLS showed no statistical association with BNP. Severe early brain edema (SEBES >2) was associated with lower BNP when TTS was <24 h (25.7 vs. 76.4, p = 0.001). However, BNP in patients with severe brain edema significantly increased from TTS >6 h (99.5 vs. 19.9 pg/mL, p = 0.011) reaching a maximum median value of 238.1 pg/mL when TTS was >24 h (Fig. 3). On the post-operative CCT, a significant association between new cerebral contusions and higher BNP values (p = 0.021) was observed. Further, an association between post-operative cerebral infarction and lower BNP values was found when TTS was <24 h (p = 0.039) (Table 1).
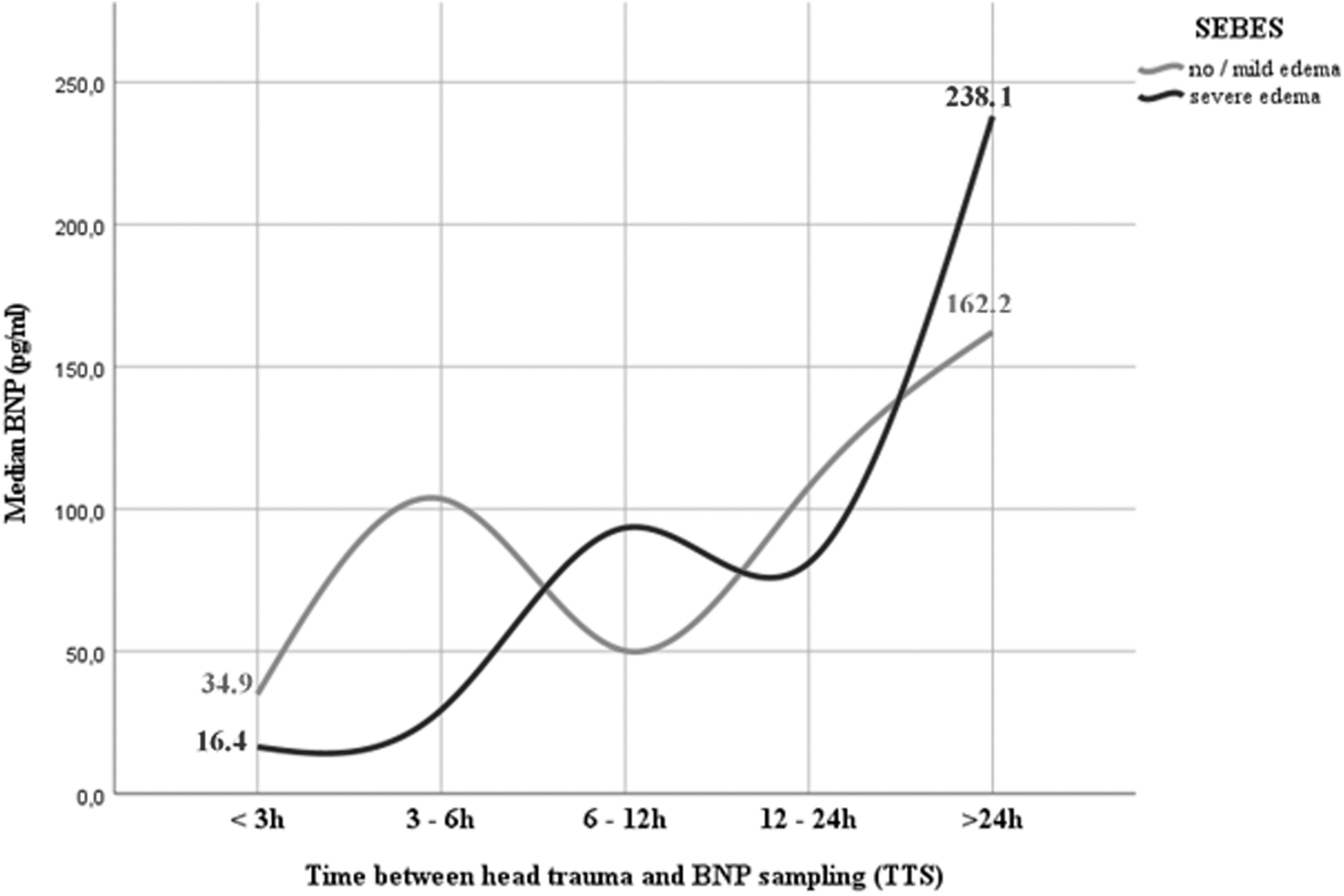
Variation of brain natriuretic peptide levels (BNP) depending on degree of early brain edema (using the Subarachnoid Hemorrhage Early Brain Edema Score [SEBES]) and time between head trauma and BNP sampling (TTS).
Relationship between BNP and the Radiographic Findings
BNP, brain natriuretic peptide; CCT, cranial computer tomography; MLS, midline shift; SEBES, Subarachnoid Hemorrhage Early Brain Edema Score; TTS, Time between head Trauma and BNP Sampling
Predictors of elevated BNP in the first 24 h after trauma
The univariate analysis is summarized in the Supplementary Table S2. After adjusting for TTS, age, sex, cardiac history, atrial fibrillation, coronary heart disease, AAT, and GCS score at admission, the multiple regression analysis revealed that larger hematoma volumes (p = 0.032) and advanced age (p = 0.005) were independent predictors of elevated BNP (Table 2).
Predictors of Elevated Brain Natriuretic Peptide (BNP)
AAT, antiaggregant/anticoagulant therapy; CI, confidence interval; GCS: Glasgow Coma Scale; SEBES, Subarachnoid Hemorrhage Early Brain Edema Score; TTS, Time between head Trauma and BNP Sampling.
Predictors of cerebral infarction after surgical treatment
Cerebral infarction was diagnosed in 10.8% (n = 14) of cases (median time of diagnosis: 3 days, IQR: 1 day). No vascular stenosis was observed on the pre-operative cranial CT-angiography of any of the 14 patients. As BNP was significantly associated with post-operative cerebral infarction in different periods of TTS (Table 1), corresponding ROC curves analyses for the prediction of cerebral infarction were performed, and the ROC curve with the best discrimination capacity (area under the curve [AUC] of 0.833, 95% CI: 0.63–1.00, p = 0.027), and corresponding time window (TTS = 3–12 h) was selected (Supplementary Fig. S1). The corresponding ROC curve analysis revealed a BNP cutoff value of 29.4 pg/mL (sensitivity: 84.6% and specificity: 75%). Post-operative cerebral infarction was significantly associated with BNP (p = 0.027) and the pupils' size and their reaction to light (p = 0.034) when TTS = 3–12 h (Supplementary Table S3). A binomial logistical regression analysis was performed, and identified BNP (< 29.4 pg/mL, aOR = 16.5, p = 0.023) as an independent predictor of cerebral infarction following surgery for traumatic aSDH (Table 3).
Predictors of Post-Operative Cerebral Infarction
BNP, brain natriuretic peptide; CI, confidence interval.
Discussion
This study is the first to investigate variability in BNP levels in terms of TTS, the relationship between BNP and the radiological findings on initial and post-operative CCT, and the role of BNP in predicting the risk of post-operative cerebral infarction in traumatic aSDH patients. We found that BNP levels continuously increased during the post-traumatic period, stagnated when TTS = 3–12 h, and then continued to increase when TTS was >12 h (p = 0.0005). BNP levels on admission were related to hematoma volumes and patient's age. During the 3–12 h post-traumatic period, BNP <29.4 pg/mL (aOR = 16.5, p = 0.023) was an independent predictor of post-operative cerebral infarction.
Variability of BNP levels with regard to TTS
In TBI patients, elevated BNP reflects brain–heart crosstalk, which involves the post-traumatic dysfunction of the autonomic nervous system and can result in sympathetic hyperactivity. 37 The subsequent hypersecretion of noradrenaline might generate cardiac wall abnormalities, causing BNP to increase, 37 relative to the extent of myocardial injury. 24 However, the timing of this process and the BNP concentrations within the first 24 h following head trauma have not yet been investigated. To date, no published data have examined the timing between head trauma and BNP sampling. Our data suggest that BNP begins to increase after brain injury (median: 25.4 pg/mL), remains slightly elevated (medians: 58.9–72.6 pg/mL) during the post-traumatic period between 3 and 12 h, and then continues to increase starting 12 h post-trauma (median: 107.8 pg/mL), reaching elevated levels >24 h after brain injury (median: 162.2 pg/mL).
BNP and radiological findings
The association between BNP and hematoma volumes in traumatic aSDH has not yet been addressed. The relationship between hematoma volumes and levels of BNP or N-terminal (NT)-pro hormone BNP (NT-proBNP) (a non-active prohormone which is released with BNP) was first described in patients with hypertensive intracerebral hemorrhage (ICH), 38 in which significantly higher levels of NT-proBNP were observed in patients with a hematoma volume >30 mL and increased ICP. 38 In another study, NT-proBNP on admission was independently associated with hematoma size. 39 Accordingly, our findings revealed that hematoma volume was an independent predictor of elevated BNP in aSDH patients during the first 24 h post-trauma. Larger prospective studies are needed to validate our findings.
The relationship between BNP and early brain edema was previously evaluated in patients with subarachnoid hemorrhage (SAH), which revealed significantly higher BNP levels in patients who experienced early brain edema within 72 h of SAH onset. 40 Accordingly, our results showed that BNP levels in patients with severe early brain edema (SEBES >2) significantly increased within the first 24 h post-trauma reaching significantly higher concentrations >24 h post-trauma (Fig. 3). Interestingly, the analysis of BNP concentrations within the first 24 h of trauma with regard to the exact time of brain injury revealed that patients with severe early brain edema (SEBES >2) presented with significantly lower BNP levels than patients with no/mild early brain edema (SEBES ≤2). These results were concordant with the clinical findings, as patients with poor GCS scores (≤ 8) had significantly lower BNP serum levels than patients with better state of consciousness. Nonetheless, the degree of brain edema using SEBES could not independently predict elevated BNP levels on admission. This may be explained by the inadequacy of SEBES to assess early brain edema in traumatic aSDH.
Role of BNP in predicting the risk of cerebral infarction after surgery
The relationship between BNP levels and the risk of cerebral infarction in patients with TBI or traumatic aSDH has not yet been assessed. Many pathological mechanisms have been associated with cerebral ischemia and acute and delayed cell death in human and experimental studies, including (1) increased ICP, (2) increased focal pressure of the expanding mass on microcirculatory elements, (3) cerebral herniation, (4) vasospasm, (5) the elevated release of excitotoxic amino acids, such as glutamate, and (6) the immunological responses of neural tissue to blood degradation products. 41 –51 These events lead to global and local reductions in CBF, critical energy supply, ionic imbalance, edema formation, and widespread cell death. 52 Therefore, the early identification of patients at high risk of cerebral infarction in clinical practice facilitates the provision of adequate post-operative neurointensive care. Clinical and experimental evidence has suggested that cerebral ischemia is associated with increased catecholamine concentrations and myocardial damage. 53 –56 Ultimately, an increase in BNP is expected after myocardial tension. Many studies have confirmed the elevation of BNP levels following AIS. 20 –33 However, only a few studies have investigated the relationship between BNP and the risk of ischemic stroke in healthy individuals 34 as well as in patients with SAH (risk of delayed cerebral ischemia [DCI]) 55,56 before AIS occurrence. In TBI and aSDH patients, this issue has not yet been investigated. The Japanese study conducted on healthy individuals showed that high plasma BNP levels could predict the risk of AIS above a cutoff BNP concentration of 30 pg/mL in men. 34 The Framingham Heart Study identified an even lower threshold BNP concentration of 20 pg/mL. 35 In contrast to healthy individuals, in patients with aneurysmal SAH who frequently presented with early brain edema, BNP levels on admission were significantly lower among those patients who later developed DCI (mean: 25.81 vs. 95.07 pg/mL), 57 or symptomatic cerebral vasospasm (mean: 32.4 vs. 102.2 pg/mL), 58 and these levels increased during the period of hospitalization. 57,58 Interestingly, our findings are in line with the aforementioned results. Indeed, we found that unexpectedly lower BNP levels (cutoff <29.4 pg/mL) in patients with large hematoma volumes (median: 118.7 mL) independently predicted the risk of cerebral infarction following surgery for traumatic aSDH when BNP was sampled within 3–12 h after brain injury. Additionally, among the patients who were admitted >12 hours post-trauma and who later developed a cerebral ischemia, BNP levels were extremely elevated (median BNP: 753.4 pg/mL). Whether the predominance of post-traumatic severe early brain edema (SEBES >2) during the acute post-traumatic period of 3–12 h among the patients who developed cerebral infarction may be the reason behind the delay in BNP elevation is a subject that requires further investigations.
Limitations of the study
Our findings can be applied to only a limited number of patients who present without cardiac insufficiency and exhibit normal renal function. However, patients with multiple comorbidities and organ failure must be considered separately, because these patients require neurointensive care and management on a case-by-case basis. In addition, the small size of our cohort limits the generalizability of our results. However, our study is the first to investigate the role of BNP in predicting the risk of cerebral infarction in traumatic aSDH, and establishes a paradigm for use in future studies. Larger prospective studies must be performed to validate our results by sampling BNP during the acute post-traumatic period of 3–12 h, which may have an important impact on post-operative neurointensive management, especially among patients at high risk of cerebral infarction.
Conclusion
In patients with traumatic aSDH, BNP begins to increase after brain injury, remains slightly elevated during the post-traumatic period of 3–12 h, and then continues to increase >12 h post-trauma. Elevated BNP was accurately predicted by larger hematoma volumes and advanced age. In the acute post-traumatic period of 3–12 h, BNP <29.4 pg/mL could independently and accurately predict the risk of cerebral infarction following surgical treatment.
Footnotes
Authors' Contributions
Mehdi Chihi takes full responsibility for the data, analyses, interpretation, and conduct of the research, has full access to all of the data, and has the right to publish any and all data separate and apart from any sponsor. All authors have read and approved the submitted manuscript. This manuscript is original, has not been published, and is not under consideration for publication elsewhere.
Funding Information
No funding was secured for this study.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Text
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.