
Abstract
Substantial clinical data support an association between superior neurological outcomes and early (within 24 h) surgical decompression for those with traumatic cervical spinal cord injury (SCI). Despite this, much discussion persists around feasibility and safety of this time threshold, particularly for those with a complete cervical SCI. This study aims to assess clinical practices and the safety profile of early surgery across a large sample of North American trauma centers. Data were derived from the Trauma Quality Improvement Program database from 2010–2016. Adult patients with a complete cervical SCI (American Spinal Injury Association [ASIA] A) who underwent surgery were included. Patients were stratified into those receiving surgery at or before 24 h and those receiving delayed intervention. Risk-adjusted variability in surgical timing across trauma centers was investigated using mixed-effects regression. In-hospital adverse events including death, major complications, and immobility-related complications were compared between groups after propensity score matching. There were 2862 patients from 353 North American trauma centers included; 1760 (61.5%) underwent surgery within 24 h. Case-mix and hospital-level characteristics explained only 6% of the variability in surgical timing both between centers and within centers. No significant differences in adverse events were identified between groups. These findings suggest a relatively large proportion of patients are not receiving surgery within the recommended time frame, despite apparent safety. Moreover, patient and hospital-level characteristics explain little of the variability in time-to-surgery. Further knowledge translation is needed to increase the proportion of patients in whom surgery is performed before the 24-h threshold so patients might reach their greatest potential for neurological recovery.
Introduction
Acute traumatic spinal cord injury (SCI) leads to debilitating damage to motor, sensory, and autonomic function. Moreover, the consequences of SCI affect almost every aspect of a patient's life—psychological, economic, social, among others. 1 Substantial clinical evidence has mounted to support superior neurological outcomes with early (<24 h) compared to late (≥24 h) decompression for cervical SCI. 2 –4 In accordance with these findings, practice guidelines recommend decompressive surgery within 24 h for patients with acute cervical SCI. 5 Moreover, survey data suggest a strong preference within the surgical community to decompress the cervical spinal cord within 24 h. 6,7
While practice guidelines and surgeon preference support surgical decompression within a 24-h threshold, little data are available to assess real-world clinical practices. The aim of this study is threefold: (1) to assess recent clinical practices regarding surgical timing for patients with complete cervical SCI (American Spinal Injury Association [ASIA] A) across a large sample of North American trauma centers; (2) estimate variability in time-to-decompressive surgery between and within trauma centers; and (3) compare the risk of complications in early (<24 h) versus delayed surgical treatment (≥24 h). This should serve to provide clinicians and healthcare decision-makers with a better understanding of current practices and a more in-depth understanding of factors that may delay surgical intervention.
Methods
Data source
This study used data from the Trauma Quality Improvement Program (TQIP) between 2010 and 2016. 8,9 The TQIP was developed by the American College of Surgeons (ACS) Committee on Trauma with the goal of benchmarking trauma centers and improving quality of care. Nearly 500 American College of Surgeons- and state-verified Level I and II adult trauma centers across North America each collect more than 100 patient- and hospital-level variables that contribute to TQIP. Each center employs trained data abstractors and undergoes internal and external audits to ensure data reliability. 8,10 Patients are excluded from the TQIP database if arriving without signs of life, are discharged from the Emergency Department (ED), have a pre-existing do-not-resuscitate order, or have severe burns.
Research ethics board approval
This study was approved by the Sunnybrook Health Sciences Center research ethics board (Toronto, Ontario, Canada).
Study eligibility
Adult patients (≥16 years) with a diagnosis of acute complete (ASIA A) cervical SCI were identified using Abbreviated Injury Scale (AIS) codes (Supplementary Table 1). Patients with a non-survivable (AIS score of 6 in any body region) or penetrating injury were excluded, as were those who did not undergo surgical intervention or in whom timing of intervention was not available. Surgical procedures were identified using the International Classification of Diseases, 9th/10th revision, Procedure Classification System (ICD-9-PCS and ICD-10-PCS) codes (Supplementary Table 2).
Multilevel Mixed-Effects Logistic Regression Model for Patient- and Hospital-Level Covariates in Odds of Undergoing Early (<24 h) Surgical Intervention
ISS, Injury Severity Scale; GCS, Glasgow Coma Scale; AIS, Abbreviated Injury Scale; MVC, motor vehicle collision.
Statistically significant.
Baseline Characteristics of Study Cohort
SMD, sample mean difference; SD, standard deviation; ISS, Injury Severity Scale; GCS, Glasgow Coma Scale; ED, emergency department; AIS, Abbreviated Injury Scale; MVC, motor vehicle collision.
Patient- and hospital-level characteristics
For all patients, we collected demographic, injury, and hospital-level characteristics. Demographic variables including age, sex, race, insurance status, and comorbidities were evaluated using the modified Charlson Comorbidity Index (mCCI) (Supplementary Table 3). Injury characteristics were comprised of total Injury Severity Score (ISS), highest AIS for each body region, mechanism, presenting Glasgow Coma Scale (GCS) score, shock on arrival (defined as an ED systolic blood pressure <90 mm Hg), the need for mechanical ventilation in the ED, alcohol and drug tests, as well as whether the patient was transferred from another institution. Characteristics of the treating facility included trauma center level, teaching status, the number of adult beds, year of injury, and case volume (defined as the number of yearly surgeries for acute cervical SCI).
Outcomes after Propensity Score Matching
OR, odds ratio; CI, confidence interval.
For early compared with delayed.
Outcomes
Time-to-surgery was defined as the total time (in hours) from ED arrival at the treating center to arrival in the operating room. Patients were categorized as undergoing early (<24 h) or delayed (≥24 h) surgery.
The primary outcome was occurrence of a major in-hospital complication. This is a composite outcome defined by TQIP as any of: acute kidney injury, acute respiratory distress syndrome (ARDS), cardiac arrest (with cardiopulmonary resuscitation), decubitus ulcer, deep or organ space surgical site infection, myocardial infarction, pneumonia or ventilator-associated pneumonia, pulmonary embolism, stroke, catheter-related bloodstream infection, unplanned return to the operating room, unplanned admission to the intensive care unit (ICU), or severe sepsis. Secondary outcomes included complications of immobility defined as a composite of decubitus ulcer, pneumonia, or pulmonary embolism and death.
Statistical analysis
Baseline cohort characteristics were reported as counts and percentages for categorical variables and as medians and interquartile ranges (IQR) for continuous variables. All analyses were performed using SAS statistical software version 9.4 (SAS Institute, Cary, NC) and R version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria) with an a priori specified significance level of p = 0.05 (two-tailed).
The variability in timeliness of cervical SCI intervention across trauma centers was assessed using mixed-effects regression models. To control for differences in case-mix and trauma center level characteristics, a “null model” was compared with a “full model,” For both, time-to-surgery dichotomized at 24 h was the outcome, with a random intercept for each individual trauma center to account for the clustering of patients within individual trauma centers. The full model also specified fixed-effect covariates for all patient- and hospital-level characteristics. The risk-adjusted mean difference and 95% confidence interval (CI) for time-to-surgery was identified for each trauma center from the full model, and outliers were identified.
The variance among individual hospitals was calculated using median odds ratios (MORs), a method that expresses between-hospital variance on the odds ratio (OR) scale.
11
It is defined as the median value of the set of ORs comparing the odds of early surgery in a patient from one randomly selected trauma center to another patient with equivalent covariates selected from a different randomly selected trauma center. Therefore, the MOR can be conceptualized as the median increase in the odds of early surgery when an individual moves from a longer wait-time trauma center to a shorter one. The larger the MOR, the greater the variation between hospitals (a value of 1 indicates no variation).
12,13
The MOR formula may be found in equation (1), where τ is the square root of the hospital-level variance.
To assess uncertainty of the estimate, a 95% CI was computed for the MOR using a parametrical bootstrap with 1000 replications. Further, the proportional change in variance (PCV) was calculated between the null and full model to determine the influence of case-mix and hospital characteristics on the timeliness of surgery.
11
Specifically, between-center and within-center variability were determined by computing the PCV using hospital-level and individual-level variances, respectively. The PCV formula is available in equation (2), where Vnull is the variance of a model with no explanatory variables and Vfull is the variance of a model that includes fixed-effect covariates for case-mix and hospital characteristics. The higher the PCV between the null and the full model, the more variability in surgical timing is explained by the case-mix and hospital level characteristics.
Patients were categorized into early and delayed surgery using a threshold of 24 h. 6 Propensity score matching was conducted over all measured characteristics to evaluate the effect of surgical timing while mitigating covariate imbalance between early and delayed surgical groups. 14 Both groups were matched 1:1 without replacement 15 using nearest neighbor matching with a caliper width of 0.2 on the logit of propensity scores. 16 To ensure appropriate balancing, the standardized mean differences of all covariates between matched groups were calculated, with values greater than 0.1 indicating imbalance. 17 On successful matching, the average treatment effect of surgical timing for all outcomes was determined via unadjusted logistic regression. 18
Sensitivity analyses
Two post hoc sensitivity analyses relating to propensity score matching were conducted. The first analysis was performed to account for potential data loss using 1:1 matching. Here, we used propensity score weighting as an alternative. 19 Unadjusted logistic regression was used to calculate the average treatment effect on those treated with early surgery for all outcomes. Robust standard errors were used to adjust for the propensity score weights. 20,21 Second, we tested whether unobserved time spent at a referring hospital impacted surgical timing. Here we performed propensity score matching using the same specifications as in the main analysis, applied to the subset of the cohort that was not transferred between hospitals.
Results
Study population
A total of 3018 subjects met eligibility criteria (Fig. 1). After excluding records with missing values (n = 156, 5.2%), 2862 patients treated at 353 trauma centers were eligible for analysis (Table 1). The median age was 45 years (IQR: 28–60), and 79.7% (n = 2280) were male. The median time-to-surgery was 17.2 h (IQR: 7.0–41.0) from ED admission for the entire cohort; 8.8 h (IQR: 4.9–15.3) for those in the early group, and 56.9 h (IQR: 35.9–108.9) for those in the delayed group (Supplementary Fig. 1). Most patients were injured in a motor vehicle collision (MVC) (47.8%, n = 1367) or a fall (41.6%, n = 1191).

CONSORT flowchart illustrating assembly of the study cohort. TQIP, Trauma Quality Improvement Program; AIS, Abbreviated Injury Scale.
Early and delayed surgery groups
Fewer than two-thirds of patients (61.5%, n = 1760) received early surgery. An unadjusted comparison revealed that those receiving delayed surgery were older with more comorbidities and were more likely to present with lower GCS scores, require mechanical ventilation, have severe head, thoracic, or abdominal injuries (Table 1).
Variability in timeliness of surgery
The complete results of the null and full mixed-effects regression models can be found in Table 2. After adjustment, we found that at an individual patient level, black race, having a concurrent severe head or abdominal injury (by AIS scoring criteria), or having a GCS less than 13 resulted in a significantly lower odds of receiving early surgery. At a hospital level, we found that being admitted to a non-teaching hospital resulted in significantly higher odds of early surgery. In addition, there was a significant association between early surgery and admission occurring in 2015 and 2016 compared with 2010.
We identified 18 hospitals with significantly higher odds of performing early surgery, and six hospitals with significantly lower odds after adjusting for case mix and hospital characteristics (Fig. 2). There was evident variability in timeliness of surgery between trauma centers, with a MOR of 1.16 (95% CI: 1.15–1.17). In other words, the odds of receiving early surgery are 16% higher if admitted to a trauma center that typically performs early surgeries compared with a center that typically does not. The hospital PCV between the null and full model was 6.3%, while the individual PCV was 5.6%. This indicates that case-mix and hospital-level covariates from the full model explain only 6% of the variability in probability of early versus late surgery both between-centers and within-centers.
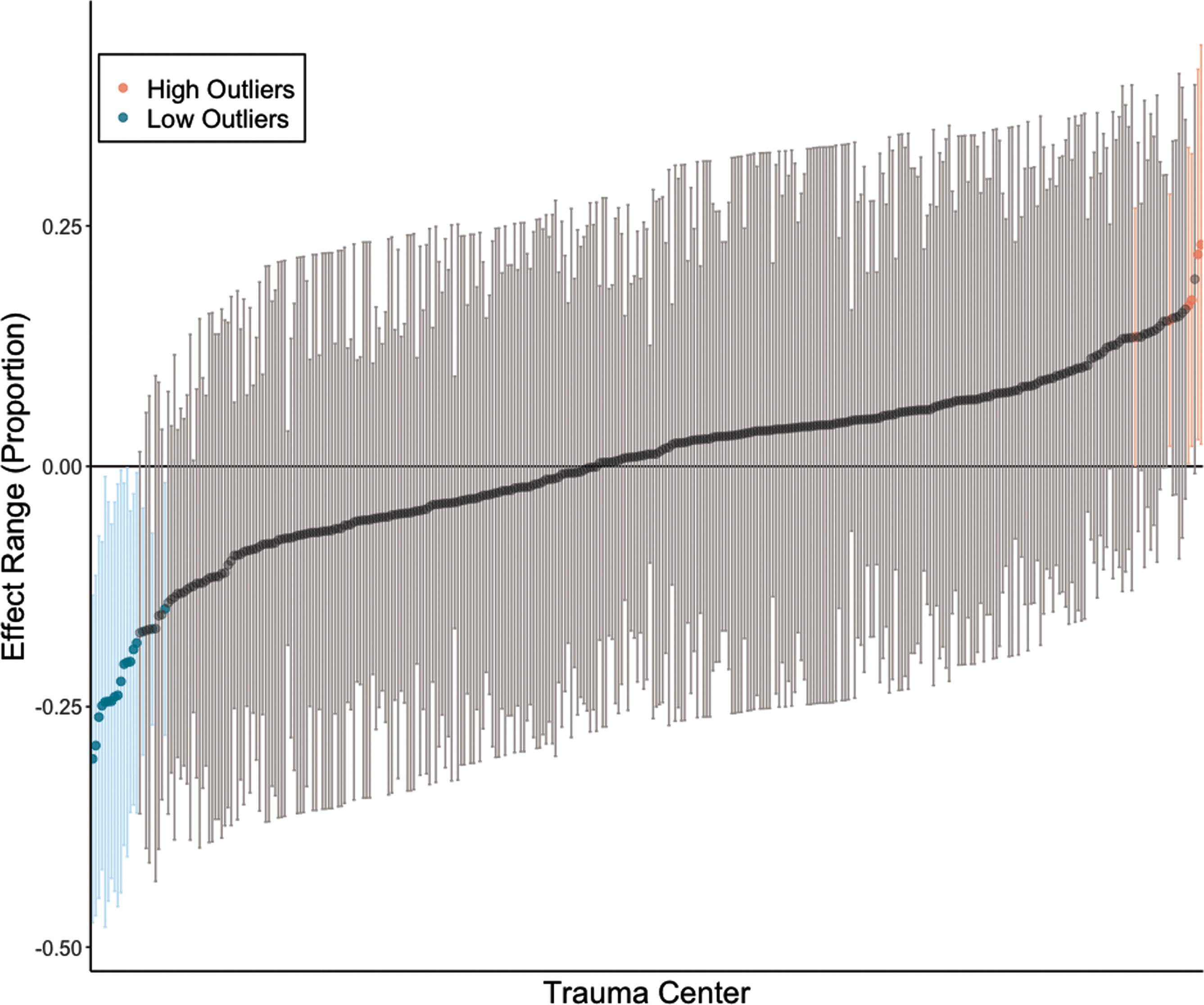
Caterpillar plot of trauma center mean differences and 95% confidence intervals (CIs) for time to surgery, risk-adjusted for patient- and hospital-level characteristics. Hospitals that have significantly shorter times to surgery than average (upper limit of the 95% CI is below 0) are low outliers (blue), whereas those with significantly longer times to surgery than average (lower limit of 95% is above 0) are high outliers (red).
Association between surgical timing and outcomes
After propensity score matching, there were 1062 patients in the early surgery group (60.3% of original size) matched with 1062 patients in the delayed group (96.4% of original size). All patient- and hospital-level factors were balanced successfully between groups, as indicated by standardized mean differences of less than 0.1 (Supplementary Table 4). Density plots of the propensity score distributions before and after matching (Supplementary Fig. 2) suggest sufficient common support.
Outcome comparisons after matching are shown in Table 3. We found no significant differences in any outcome measures between early and delayed surgery. Of those undergoing early surgery, 45.5% (n = 483) experienced a major complication compared with 48.7% (n = 517) in the delayed group. The lack of an association was also evident for complications of immobility, which were experienced by 39.5% (n = 419) and 41.7% (n = 443) of patients in the early and delayed groups, respectively. Overall mortality rate in the matched patient cohort was 11.6% (n = 246), with 12.2% (n = 130) in the early group versus 10.9% (n = 116) in the delayed group.
The results of our sensitivity analysis using propensity score weighting reiterated non-significant differences between early and delayed surgery groups for all measured outcomes (Supplementary Table 5). Excluding patients who were transferred between trauma centers again showed similar results for all outcomes (Supplementary Table 6).
Discussion
Our analysis of this multi-center North American database from 2010 to 2016 suggests that fewer than two-thirds of patients with a complete cervical SCI undergo surgery within 24 h. These real-world clinical practices contrast with expressed surgeon preference. Glennie and associates 7 reported that 93% of surgeons surveyed believe surgery within 24 h is ideal for patients with a complete or motor complete cervical SCI; similarly, Fehlings and colleagues 6 found that more than 80% of surgeons held a similar view in a separate survey.
Despite this general preference for early surgery and supporting guidelines, there may be factors limiting access to surgical management within this time frame. 2 –5 We found a number of patient-level factors associated with significantly higher odds of undergoing delayed surgery. These included black race, as well as severe head and abdominal injuries. While severe injuries to the head or abdominal injuries may expectedly delay intervention, the identification of racial differences in surgical timing demonstrates potential implicit biases. There is much research suggesting disparities in access to surgical care based on race despite adjustment for covariates such as age, insurance status, and geographic region 22 –25 Our study similarly shows that race may impact patient care in the emergent setting. Surgeons should thereby be mindful of any implicit biases that may affect provision of just and high-quality care.
Despite the statistical significance of certain patient characteristics, only 6% of the overall variability in surgical timing was explained by case-mix and hospital-level characteristics. Thus, most variability is a result of unobserved factors. Some may come from center specific practice patterns, because we found 18 hospitals with significantly shorter wait times and six hospitals with significantly longer wait times after controlling for case-mix differences. Moreover, we found a MOR of 1.16 (95% CI: 1.15–1.17) suggesting significant contextual effects at the trauma center level that impact the probability of early surgery. These unobserved factors may include timely access to imaging modalities, access to operating room resources, and local hospital practice patterns. 26 –28
Certainly comorbidities, concurrent injuries, and other patient related factors do contribute to the timeliness of surgery, and some of these factors may unavoidably delay surgery, but the low explained variance suggests that implementation of process level changes may result in earlier surgery.
We observed that more than one-third of patients admitted to a North American TQIP trauma center between 2010 and 2016 had a delayed surgical intervention. This compares favorably with studies of earlier time periods. A 1999 study by Tator and coworkers 29 concluded that only 23.5% of patients admitted to North American centers with SCI underwent surgery within 24 h. An assessment of a multi-center Canadian SCI database from 2004–2014 found only 51.5% of patients with a cervical complete or motor complete SCI underwent surgery within 24 h. 7 In addition, a study of the National Trauma Data Bank from 2011 to 2012 reported only 57.0% of the patients with complete SCI had undergone surgical intervention within 24 h. 26
The improvement in timeliness of surgical intervention may be explained at least in part by increasing awareness of the benefit of early decompressive surgery. 2,3,30 –32 In fact, within our dataset, we noted that 2015 and 2016 were associated with a significantly higher likelihood of undergoing early surgery when compared with 2010 as the base year. This encouraging finding signals that knowledge translation efforts may further improve the proportion of patients undergoing early surgery.
As the growing evidence about the neurological benefit of early surgery in cervical SCI is broadly acknowledged, the inherent risks of early surgery for these severely injured patients are still discussed. 33,34 Encouragingly, we found no significant differences in major complications, complications of immobility, or in-hospital death between early and delayed surgical groups for patients with traumatic cervical SCI. This agrees with a prospective observational study of surgical timing for traumatic cervical SCI that found no significant differences in post-operative complications and 30-day deaths between the early and delayed surgery groups. 3
A recent nationwide retrospective cohort in Japan revealed no significant differences in length of critical care and in-hospital death after early surgery for cervical SCI when compared with delayed surgery. 35 As such, our findings add to the current body of evidence supporting the relative safety of early surgical treatment.
The findings of this study are strengthened by high-quality data from more than 350 North American trauma centers, supporting generalizability. Further, the inclusion of more than 3000 patients permitted regression adjustment for many covariates and allowed us to account for the clustered nature of the data. There are notable limitations, however. First, it is worth mentioning that propensity score matching does not account for unobserved latent variables that may remain after matching and confound results. Moreover, we do not have data on the nature of the osseous spinal column injury, the degree of spinal cord compression of the specifics of the surgical intervention. To some degree, these may impact surgical timing, even for those with a complete neurological injury.
We also could not include transport time and time spent in a referring hospital, nor could we include the time from arrival at the treating hospital to spine surgery consultation. Given that a little more than 25% of our cohort was transferred from another institution, this could impact our findings. The raw difference in transfer status between the early and delayed groups, however, was minimal (27.1% and 24.1%, respectively). Moreover, excluding patients who were transferred did not impact our findings on sensitivity analysis. This is in accordance with previous work, which has shown that, for patients transferred from an outside hospital, most pre-surgical time is spent between arrival at the treating hospital and arrival in the operating room. 36
In addition, a study of the National Trauma Data Bank research data set from 2011 to 2012 demonstrated that for patients with traumatic SCI, 90% of the time between emergency medical services dispatch and surgical intervention occurred after arrival at the treating hospital. 26 Thus, it seems the probability of early surgery is not largely influenced by transfer and transport time and more likely relates to policies and practices at the treating center.
Conclusion
Our findings from a large sample of North American trauma centers suggests surgical intervention for patients with complete cervical SCI occurs within 24 h in fewer than two-thirds of patients. Further, observed patient- and hospital-level characteristics explain little of the variability in surgical timing. Encouragingly, surgery within 24 h does not increase the risk of adverse events compared with delayed surgery (≥24 h). These findings support the need for further work to enhance knowledge translation surrounding timeliness of surgery with a goal to improve surgical care pathway efficiency.
Footnotes
Acknowledgments
The authors would like to thank Melissa Tom for her assistance with database management. Avery B. Nathens is the Medical Director, Trauma Quality Programs, American College of Surgeons.
Authors' Contributions
MB, study design, data analysis, manuscript preparation and revisions; PP, manuscript preparation; LN, manuscript preparation; ASJ, manuscript revisions; GL, manuscript revisions; JHB, manuscript revisions; LdC, manuscript revisions; ABN, data acquisition and manuscript revisions; MGF, manuscript revisions; JRW, manuscript revisions; CDW, study design, data analysis, manuscript preparation and revisions.
Funding Information
This study was funded by a Young Investigator Award from AOSpine North America.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.