
Abstract
Traumatic brain injury (TBI) causes structural and functional damage to the central nervous system including the visual pathway. Defects in the afferent visual pathways affect visual function and in severe cases cause complete visual loss. Visual dysfunction is detectable by structural and functional ophthalmic examinations that are routine in the eye clinic, including examination of the pupillary light reflex and optical coherence tomography (OCT). Assessment of pupillary light reflex is a non-invasive assessment combining afferent and efferent visual function. While a assessment using a flashlight is relatively insensitive, automated pupillometry has 95% specificity and 78.1% sensitivity in detecting TBI-related visual and cerebral dysfunction with an area under the curve of 0.69–0.78. OCT may also serve as a noninvasive biomarker of TBI severity, demonstrating changes in the retinal ganglion cell layer and nerve fiber layer throughout the range of TBI severity even in the absence of visual symptoms. This review discusses the impact of TBI on visual structure and function.
Introduction
Traumatic brain injury (TBI) disrupts central nervous system (CNS) function and is a nondegenerative brain insult, potentially causing temporary or permanent impairment of physical, visual, and cognitive functions. 1 Current consensus defines TBI as “an alteration to brain function or other evidence of brain pathology, caused by an external force.” 2 Globally, 10 million persons annually are affected by TBI, with a reported incidence rate of 106 per 100,000. 3 It was estimated by the World Health Organization that by 2030, TBI may exceed other types of neurological disease as the major cause of death and disability. 4
The pathophysiology of TBI includes primary and secondary injuries. Primary injury is the mechanical event causing neural and vascular structural damage. This primary injury triggers a cascade of cellular and tissue events, including oxygen free radical generation, calcium toxicity, neuroinflammation, and raised intracranial pressure (ICP). These events are known as secondary injury and can significantly amplify the initial damage. 5
Surgical intervention may be required to remove hematoma, reduce ICP, and preserve the viability of remaining brain tissue (preventing secondary injury). Diffuse lesions (including diffuse axonal injury) are caused by rapid accelerative, decelerative, or rotational forces such as in motor vehicle collisions, assaults, and falls. 6 Primary injury is irreversible, but secondary injury prevention improves outcomes. 7
In general, TBI impacts all aspects of life including physical, cognitive, behavioral, social, and/or emotional function. The eye is commonly injured directly in association with TBI, with eye injuries comprising 10% of military major trauma 8 and affecting 20% of the civilian population at some point in their life. 9 Injury to the optic nerve may be associated with eye injury or TBI, being a severe and debilitating manifestation. Subclinical injury to the optic nerve may pass unnoticed in TBI but may also serve as a biomarker or correlate of injury severity.
This review aims to detail afferent visual functional and structural changes after TBI to highlight the extent to which patients with TBI have visual dysfunction, as well as the extent to which afferent visual changes may indicate TBI severity and prognosis.
Methods
A literature search was performed in the PubMed database by using the keyword combinations: [‘traumatic brain injury’ OR ‘head injury’ OR ‘head concussion,’ OR ‘head contusion’] AND {[‘visual status’ OR ‘visual function’ OR ‘visual problem’] OR [‘ocular structure’ OR ‘eye structure’ OR ‘eye injuries’ OR ‘ocular trauma’]}. The search terms were used to collect all publications reporting eye/visual problems related to TBI and identified 2440 articles that were screened by abstracts. All reports were then screened to remove cases with efferent visual manifestations, and confined to English language only. The reference lists of the relevant reports were thoroughly reviewed to identify other related reports.
Classification of TBI
There are several methods available to classify TBI symptoms and severity. They are important in providing prognostic information and guiding treatment strategies. The Glasgow Coma Scale (GCS) has been used routinely in Emergency Departments to assess conscious level in patients with TBI, covering eye opening, verbal and motor responses. Based on the score obtained in each component, they can be combined into a single index score and categorized as either mild, GCS 13–15; moderate, GCS 9–12, or severe, GCS 3–8. 10
In addition, GCS Pupil Score (GCS-P) has been introduced recently combining GCS and pupil reactivity to assess conscious level in the presence of focal (brainstem) dysfunction. 11 The pupil reactivity is divided into three scoring systems: 2 for both pupils unreactive, 1 for only one pupil reactive, and 0 if neither pupil is unreactive. The total GSC-P score is then calculated by subtracting the pupil reactivity score from the GCS total score.
Post-traumatic amnesia (PTA) is a period of confusion after TBI, which also includes the duration of unconsciousness or medicated coma until the patient is oriented and able to recall memories. 12 A PTA of up to 24 h is considered as mild TBI, while between one and seven days and more than seven days are considered as moderate and severe TBI, respectively. Loss of consciousness (LOC) may occur, and its duration can be used to classify TBI severity. Alteration of consciousness/mental state is similar but not identical to LOC classification. 13 Table 1 summarizes the classification of TBI based on its severity.
Classification of Traumatic Brain Injury Severity
GCS, Glasgow Coma Scale.
The Glasgow Outcome Scale (GOS) measures neurological outcome in patients recovering from TBI in five categories: death; persistent vegetative state; severe disability (conscious but disabled); moderate disability (disabled but independent); and good recovery. 14 Although GOS has been implemented widely, it has been criticized as being insufficiently sensitive in patients with good outcomes, and the score tends to plateau at SIX months, although patients have not completed recovery by this time point. 15 Hence, the extended GOS (GOSE) was introduced and subdivides the favorable three categories (good recovery, moderate disability, and severe disability) into two levels—upper and lower levels—through structured interview. 16,17
The Mayo Classification System is also useful in classifying the TBI severity retrospectively and addressing post-trauma clinical evaluations. 18 It uses multiple criteria including GCS score, loss of consciousness, PTA, neuroradiological abnormalities, cerebral and hemorrhagic contusion to confirm diagnosis of either definite moderate-severe TBI, mild TBI, or symptomatic TBI. 18 This system showed better results in classifying TBI with an estimated 89% sensitivity and 98% specificity for moderate-severe TBI. 18
Injuries Associated with TBI
Eye Injuries
Eye injuries are generally categorized as open and closed globe injuries, of which open-globe injuries routinely necessitate rapid surgical intervention. Closed globe injuries may also be time critical with optic nerve compression or ischemia and raised intraocular pressure. 19 According to The Birmingham Eye Trauma Terminology classification, open-globe injury is defined as eye penetration with a full-thickness wound of the eye wall, and closed-globe injury is defined as no full-thickness wound of the eye wall. 20,21
In a sample of 594 patients with TBI who had ocular signs, 28.0–51.8% had eyelid ecchymosis, followed by subconjunctival hemorrhage (38.6–44.4%), chemosis (43.1%), lid edema (41.4%), lacerated wound (22.5%), and other injuries. 22 –25 Other injuries including corneal edema, vitreous hemorrhage, retinal detachment, and optic neuropathy were also described in association with TBI. 19,26
The causes of eye injury are varied. Sports-related injuries are common among young persons. 27,28 In the United States, 30% of ocular injuries in youths younger than 16 years were sports related. 29 In a retrospective, cross-sectional study of sports-related ocular injuries, Haring and colleagues 30 documented eyelid/adnexal injury as the most common ocular injury especially in basketball players, contusions as the second most common such as in baseball and air gun sports, and then superficial wounds and orbital fractures.
In a retrospective, cross-sectional study of combat ocular trauma, 31 66% (101 of 152 ) patients also had TBI. While specific neuro-ophthalmic manifestations were less common than other ocular injuries, the combination of globe and neuro-ophthalmic injury carried a poor prognosis for visual recovery. 32 A recent retrospective study reviewed the Walter Reed Ocular Trauma Database (WROTD) and reported that optic nerve injury was the main cause of neuro-ophthalmic injury and was significantly associated with TBI and poor visual outcome. 33 Another recent study of WROTD documented one-third of combat ocular trauma had either a single or multiple orbital fractures with approximately 40% legally blind after injury. 34
Traumatic optic neuropathy
Optic nerve damage caused by trauma is termed traumatic optic neuropathy (TON). Historic data suggest that the prevalence of TON is between 0.5% and 8% in cases of TBI overall. 35 –40 Recent case series suggest that subtle retinal and visual changes after TBI may be much more frequent, being present subclinically in many elite athletes after head injuries in sport activities. 41 –43 In the United Kingdom, Lee and coworkers 44 estimated the incidence of TON was 1 per million population on the basis of a survey of consultant ophthalmologists (using the British Ophthalmic Surveillance Unit; BOSU), with adult males (79–85%) in their early thirties comprising the bulk of the cohort and falls (25.6%), road traffic accidents (21.5%) and assaults (20.7%) being the top three causes.
The TON may be classified as direct or indirect, with indirect the most common. 45 Direct TON is usually associated with an open wound caused by a projectile or object that directly injures the optic nerve, causing severe and immediate visual loss. 37 Direct TON may also cause 46 optic nerve avulsion after rotational force applied to the globe and injury associated with displaced fractures compressing or transecting the optic nerve. 47
Indirect TON typically occurs after non-penetrating impact trauma, including concussion to the head and orbital areas, hemorrhage, and edema, 45 with transmitted forces to the optic canal. 48,49 In the optic canal, the blood supply to the nerve is pial, and transmitted forces damaging the pial vessels causing ischemia may therefore contribute to the optic neuropathy. 47 In addition, secondary release of inflammatory mediators, blood–brain barrier breakdown, oxidative stress, and the activation of apoptotic signaling pathways may cause progressive injury. 19
Visual Manifestations of TBI
Visual dysfunction secondary to TBI is common and often involves multiple aspects of visual function with varying severity, including afferent and efferent pathways. 50 Significant visual dysfunction greatly affects patients' quality of life after TBI, 51 and that includes deficits in visual acuity (VA), visual fields, and color vision. Structural deficits are demonstrable on optical coherence tomography (OCT) and brain imaging.
VA
The VA at baseline, shortly after TBI, is one of the prognostic factors predicting final outcome. 52 Visual acuity worse than or equal to 6/60 in patients with moderate to severe TBI fits with the classical description of TON, 53 and the prevalence is low, being reported as between 0 and 3.2% of patients with head injury. 54 Among elite athletes, concussion is common in contact sports such as football, baseball, and boxing, and most patients retain VA equal to or better than 6/18, with very few cases worse than 6/30, 55 but any reduction in VA may impair balance and reaction time in sportsmen and women. 56
Reported military VA outcomes after TBI range from 6/6 to 6/38 in both blast and nonblast mild TBI. 57,58 Recent studies reported 36% of neuro-ophthalmic injury cases and 40% of orbital fracture cases among those with combat ocular trauma with an outcome of legally blind (VA of 6/60 or less with best correction or widest visual field of no greater than 20 degrees, both in the better eye). 33,34
Head injury-associated lesions of the occipital cortex, either hemorrhage or edema, cause cortical visual impairment (CVI), 59,60 which may be transient or permanent. Transient visual loss is found in several case reports involving mostly children who eventually regained pre-traumatic VA one day to five months after injury. 61,62 Permanent visual loss also occurs. 63
Systemic and/or ocular signs at presentation may predict visual outcome. The presence of blood within the posterior ethmoidal cells, age over 40 years, LOC associated with TON and absence of recovery after 48 h associate with no recovery in VA. 36
Visual field
Injury to the optic nerve and visual pathway may cause visual field defects. Visual fields are usually assessed using either manual Goldmann or automated Humphrey perimetry. These techniques can accurately detect visual field loss, and any changes can be monitored over time. Other methods such as the confrontation technique are commonly used for screening and are useful in detecting severe visual field loss. 36
Occipital lobe lesions display retinotopic organization on magnetic resonance imaging (MRI), correlating with visual field mapping in patients with homonymous hemianopia, homonymous quadrantanopia, and homonymous scotomas. 64 Thinning of the retinal ganglion cell and inner plexiform layers after transsynaptic degeneration over months after injury associates with primary gray matter degeneration in the temporal and occipital lobes and corresponding visual field defects. 65 Lesions anterior to the lateral geniculate injure optic nerve axons directly and cause more rapid retrograde degeneration and retinal ganglion cell loss.
A recent systematic review including 2106 TBI estimated the prevalence of visual field defects at 18.2% (95% confidence interval 10.6%–27.1%). 54 Of that, hemianopia was the most common visual field defect followed by quadrantopia, tunnel vision, and central or paracentral scotoma. Visual field loss was more common in moderate than mild TBI (39.8% vs. 6.6%). Elsewhere, of 112 TBI patients with homonymous hemianopia corresponding to injuries in the optic tracts, chiasm, radiations, and occipital lobe on MRI and computed tomography (CT), 44 (39.3%) had a complete homonymous defect. 63,66
In traumatic chiasmal syndrome, bitemporal hemianopia is associated with cranial nerve lesions, diabetes insipidus, and other endocrine disturbances, 67,68 although some reports include no neurological deficits. 69,70
Most patients with blast-related TBI displayed some abnormality on visual field testing, including abnormal global indices (mild TBI) and homonymous defects such as hemianopia (moderate and severe TBI), 71,72 although one study reported no difference in the frequency and type of field defects between blast and non-blast TBI. 73
Pupillary function
The pupillary light reflex (PLR) is an important prognostic factor predicting final outcome. 74 The PLR assesses the functional integrity of the anterior visual pathway. Abnormal or absent pupil responses may indicate defects in the afferent and efferent arms of the pathway. A TON may be detected acutely using a simple swinging-flashlight test to detect a relative afferent pupillary defect (RAPD). 75 –77
Use of a neutral density (ND) filter to quantify a RAPD is performed by placing ND filters of increasing density in front of the non-affected eye while performing the swinging-flashlight test until the RAPD is neutralized, which results correlate well with retinal nerve fiber layer (RNFL) thickness. 78 Such bedside examination, however, is not sensitive to the range of subtle changes in the PLR that occur after TBI.
A modern pupillometer, on the other hand, provides an objective, quantitative, automated assessment of PLR. Typically, a flash stimulus configuration elicits the PLR, which may be assessed either monocularly or binocularly. A study reported, on average, a delay/reduction in four PLR parameters (constriction latency, average constriction velocity, dilation velocity, and 75% recovery time) among 20 military service members with blast-induced mild TBI compared with matched control patients (n = 20) using a monocular infrared pupillometer (PLR-200™). 79 Similar findings were also reported in 17 chronic nonblast-induced patients with mild TBI when compared with 15 visually normal controls, indicating the potential application of PLR in optimizing the diagnosis of mild TBI. 80
Of four studies evaluating 32 patients with non-blast mild TBI and 40 normal controls using binocular pupillometry (Neuroptics DP-2000), one found no difference in pupil size (static), but on dynamic testing showed differences in constriction latency, maximum and minimum pupil diameters, average and peak constriction velocities, peak dilation velocity, and 6 sec post-stimulus diameter (Fig. 1), across a variety of stimulus conditions; dim pulse, dim step, bright pulse, bright step, bright red step, and bright blue step. 81 The study noted peak dilation velocity yielded high specificity (95%) and sensitivity (78.1%) with area under the curve 0.69–0.78 when combined with latency, showing that it can be a good biomarker to identify patients with suspected mild TBI. 81
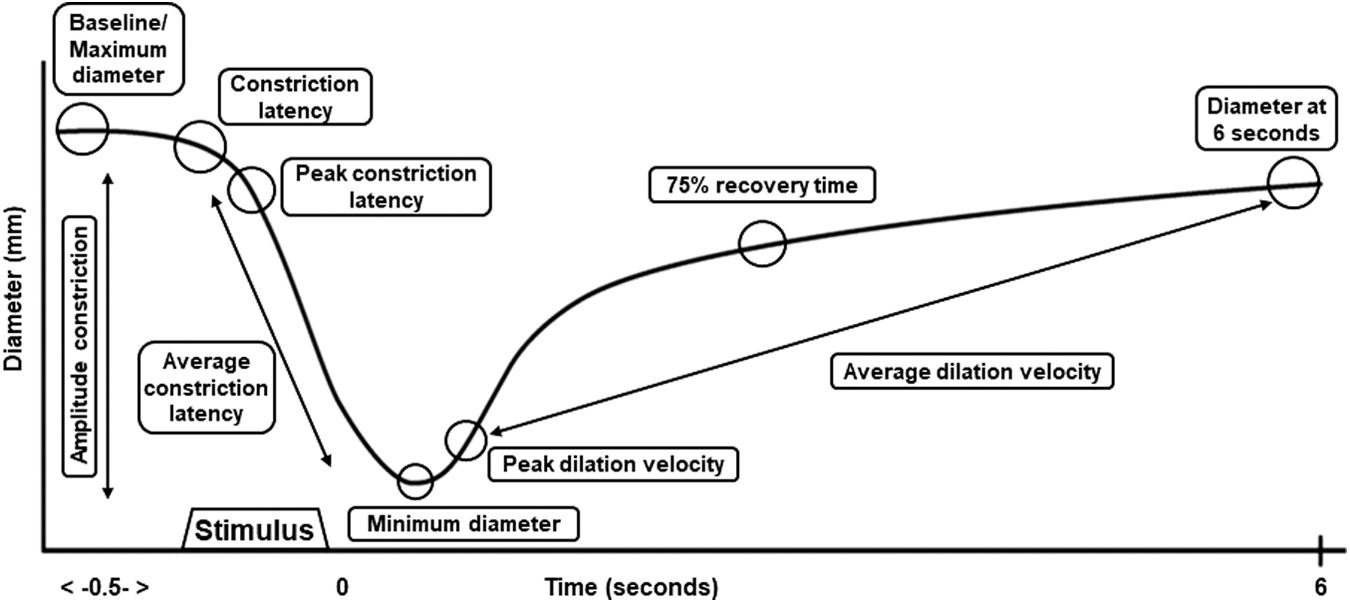
Schematic representation of dynamic pupil response measured using automated pupilometer. Pupil diameter at pre- and post-stimulus for each parameter indicated by the open circles. The size of each circle corresponds to the size of pupil diameter. Pre-stimulus time is 0.5 sec and the post-stimulus time is 6.0 sec.
The same authors also found the interocular pupillary effects of mild TBI appear to be symmetrical, 82 while several PLR parameters exhibited differences in patients with and without photosensitivity. 83 Thus, the authors suggested that besides being a potential biomarker to detect mild TBI, dynamic pupillary parameters could also be used to test photosensitivity in this specific population. Nevertheless, high refractive error may confound PLR, and correction for refractive error may therefore be necessary when using PLR in a clinical setting. 84 Table 2 summarizes the pupillometry data between normal controls and patients with mild TBI.
Summary of Pupillometry Parameters Data between Normal Controls and Patients with Mild Traumatic Brain Injury
TBI, traumatic brain injury.
Indicates p < 0.05; **indicates p < 0.0001
Color vision
A TBI may affect color perception by damaging the retina, optic nerve, the parvocellular pathway through the optic tract, and radiations or visual area V4. 85 In the 2010 BOSU study, only 63/121 TON had color vision tested using a 17-plate Ishihara test, of whom 10 patients had full color vision, 32 read 12 or fewer plates, and 21 patients were unable to see the test plate, 44 while others reported reductions in the mean number of Ishihara plates read in affected eyes. 86,87 In contrast, a more recent study found normal color vision in young veterans who had either blunt or blast mild TBI greater than six months prior, 88 but not clinically manifest TON, associating abnormal color perception with TON specifically rather than TBI in general.
A detailed discussion of color vision testing is beyond the scope of this review, but for context, a brief description is provided. While they are commonly available in eye clinics, Ishihara and other pseudo-isochromatic plates are limited in a number of ways: they are specifically designed to assess congenital red-green color vision defects; are therefore unable to classify the types of color vision defects; are not a quantitative assessment of severity of color vision deficiency. 89
Panel tests such as Farnsworth Panel D-15 and Farnsworth-Munsell 100 hue may be more useful and suitable for acquired visual dysfunction. For clinical use, Farnsworth Panel D-15 is simpler and quicker, while the 100 hue test is more accurate and detailed but also time-consuming. A case report compared Farnsworth Panel D-15 and Fransworth-Munsell 100 hue tests on a patient who sustained TBI to the occipital region over three visits of four months apart and found both tests were consistent and reliable in demonstrating the type of color vision defect. 90
Alternatives in color vision testing include the Color Assessment and Diagnosis tool and the ChromaTest, both of which provide detailed assessment of defects on red-green and blue-yellow axes in comparison with normative databases but have not been reported in TBI. 89
Contrast sensitivity
A TON secondary to TBI may impair contrast sensitivity, which patients may express as blurred vision with normal VA. Singh and associates 87 reported lower contrast sensitivity scores at presentation in patients with mild TBI compared with controls, as measured with the Pelli-Robson Letter contrast chart. The symptoms improved and showed no difference compared with normal controls more than three months after injury, suggesting that contrast sensitivity recovers over time and also (because it affected most patients with mild TBI) that deficits in contrast sensitivity do not directly relate to afferent visual function.
The divergence between objectively assessed afferent visual function and deficits in contrast sensitivity is further supported by the fact that Corning Photochromic Filter lenses enhanced binocular contrast sensitivity by two-fold (0.3 log units), and increased reading rate, compared with performance in the absence of any filter lenses. 91 A recent study, however, showed no significant difference in reading performance between three different types of tinted lenses despite reporting greater comfort while wearing them. 92 Tinted lenses may therefore be more useful to improve comfort by reducing photophobia.
Retinal structure in TBI
Structural imaging including scanning laser polarimetry (SLP) and OCT document defects in the visual pathways associated with TBI. In most TBI studies, the RNFL, ganglion cell layer (GCL), macular and ganglion cell complex [GCC [combination of GCL, and inner plexiform layer]) are the main metrics evaluated for the retinal structure after trauma. Figure 2 shows a cross-sectional image of normal healthy retina imaged using OCT.
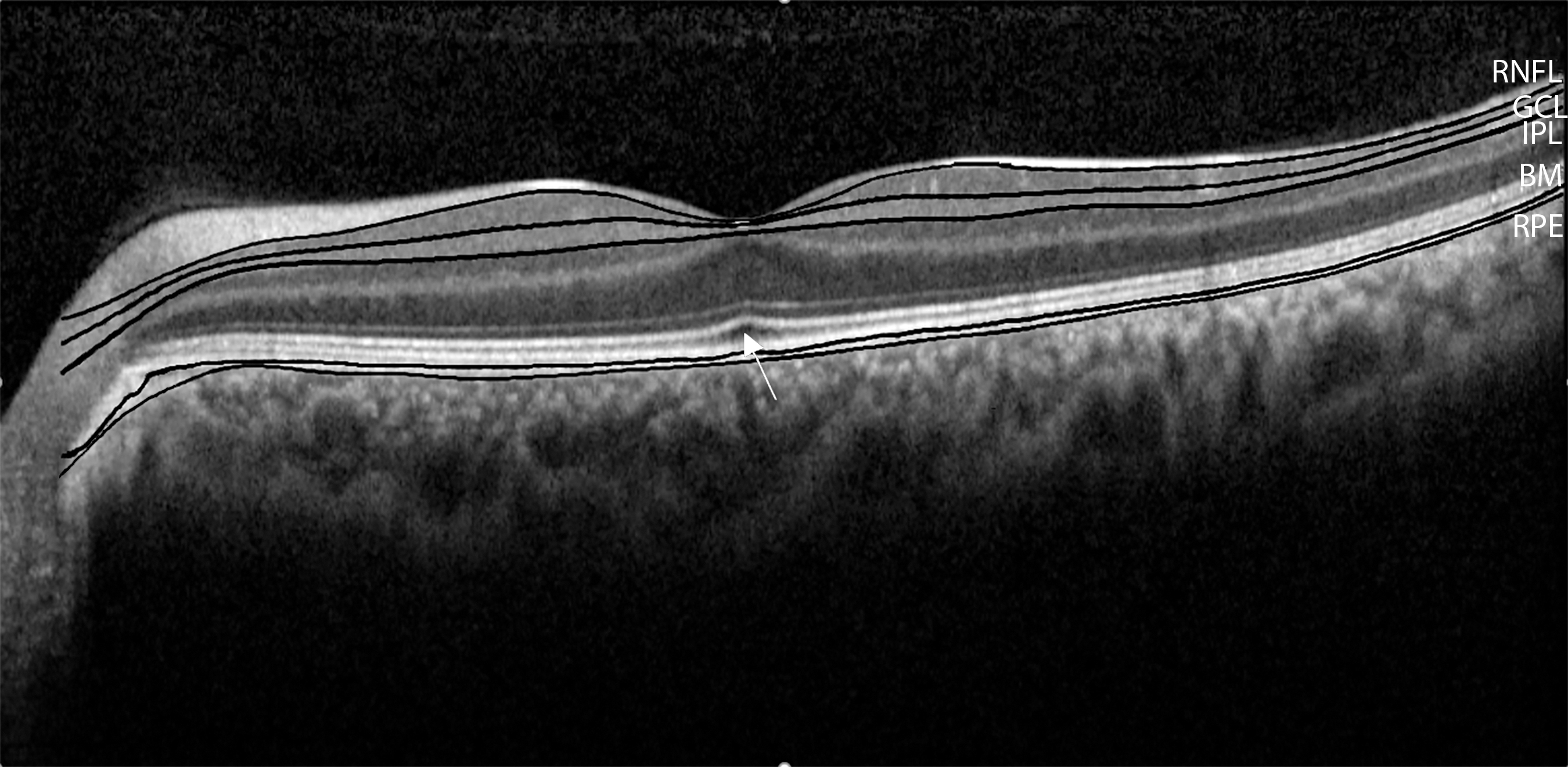
Cross-sectional image of the retina scanned using OCT. The common two layers investigated in TBI studies are the retinal nerve fibre layer (RNFL; top black line) and ganglion cell layer (GCL; second black line). Some studies reported the GCC which comprises GCL and inner plexiform layer (IPL; third line), because of the difficulty in segmenting these two layers. The bottom two lines indicate the retinal pigment epithelium (RPE) and Bruch s membrane (BM). The white arrow shows the interdigitation zone at the fovea centralis, where the outer segment of photoreceptors located.
SLP
SLP measures tissue thickness using polarized near-infrared light (780 nm), making use of the birefringent properties of ocular tissues such as cornea, lens, and retinal nerve fibers. In the retina, polarized light passing through the microtubules of ganglion cell axons is retarded in proportion to the RNFL thickness. 93
SLP has been used to assess, diagnose, and monitor the RNFL and optic nerve head of eyes with glaucomatous optic neuropathy. 94 –97 SLP detected progressive RNFL loss after TON between weeks nine and 13 post-injury with no progression of RNFL loss recorded after week 13 post-injury, consistent with the ophthalmoscopic optic nerve pallor/atrophy at this time point, 98,99 while others documented increased RNFL thicknesses within the first week after the injury, before subsequent atrophy, 93,100 potentially related to axonal edema in the early stages. The pattern of visual field loss corresponds to RNFL atrophy, although field loss precedes RNFL loss. Table 3 summarizes the studies evaluating SLP in patients with TON.
Studies of Retinal Changes in Patients with Traumatic Optic Neuropathy Using Scanning Layer Polarimetry
RNFL, retinal nerve fiber layer.
OCT manifestations of TBI
OCT is ubiquitous in its application to detect physiological and pathological changes in the retina. 101,102 In comparison with SLP, OCT was better at revealing RNFL thickening from edema. 103 There is no gold standard for ophthalmic examinations evaluating TBI severity, but OCT may provide detail on both severity and pathogenesis. It is therefore of interest to review the range of OCT findings in patients with TON/TBI.
There are two historic types of OCT: time domain and spectral domain. Time domain OCT scans 400 axial measurements per second with approximately 10 μm axial resolution, being limited by the need to physically move the reference mirror to determine path length. Spectral domain OCT are now more widely used and allows faster scanning acquisition of 18,000 axial measurements per second with consequent higher—approximately 5 μm—axial resolution thanks to the incorporation of a spectrophotometer, with Fourier transform of the spectral signal (and no need to move a reference mirror). 104
Spectral domain OCT is therefore much more sensitive in detecting changes in retinal layer thickness with fewer artefacts compared with time domain OCT, 104,105 across ocular diseases such as glaucoma 106 and age-related macular degeneration. 107,108 Swept-source OCT uses Fourier domain detection in addition to a longer wavelength tunable laser to improve visualization of deep structures.
Early case reports showed progressive RNFL and macula thinning in patients with unilateral TON from two to 11 weeks post-injury, 75,76,109,110 with a later inclusion of GCC thinning noted between week two to week eight post-injury and all parameters measured plateauing by week 20, although there are conflicting reports of whether RNFL or GCL changes manifest first. 77,110
In 54 unilateral TON (28 no light perception [NLP]; 26 better than NLP), RNFL thickness in patients with better than NLP vision decreased two weeks after injury (similar most previous reports), but in patients with NLP vision, the RNFL thickness increased two weeks after injury, only decreasing at week four to week 12 likely reflecting a longer duration of more severe axonal edema in the patients with NLP. The greater reduction in RNFL thickness of the NLP group (52%) compared with the better than NLP group (38%) related axonal loss to function. 111
Two TON/TBI studies demonstrate focal thinning of the ganglion cell and the inner plexiform layers predominantly in the superior and inferior quadrants, which mimics the pattern of axonal loss seen in glaucomatous optic neuropathy and may relate to lesser connective tissue support in the superior and inferior lamina cribrosa leaving fragile arcuate fibers vulnerable to injury. 86,87
In repetitive concussion, studied in American football players with and without a history of concussion RNFL (106.8 μm vs. 103.7 μm) and GCC (98.1 μm vs. 96.7 μm) thickness was increased. 43 Similar findings were also reported for total macula thickness of Olympic boxers when compared between two follow-up visits (right eye: 270.5 μm vs. 275.6 μm, left eye: 268.3 μm vs. 275.8 μm). 112 Thickening of RNFL occurs in papilledema (where elevated ICP induces RNFL swelling), 113 but here may relate to an immune response with secondary gliotic scarring. 43
In conflicting reports, others have found that average RNFL (but not GCC) thickness was 4-4.8 μm thinner in contact sport athletes (boxers, American football, rugby, and hockey players) compared with age-, gender- and race-matched controls. 41,42 Between athlete groups, only boxers displayed significant GCC thinning by 5.0 μm. 42 Comparable findings are found in other neuropathological conditions such as Alzheimer disease 114 and multiple sclerosis. 115
Similar to other causes of TBI, 116 the average RNFL thinning in veterans with TBI compared with veterans without TBI was 14.8% for the right eye and 7.6% for the left eye, and the average thinning of GCC was 24.5% and 14.8% for right eye and left eye, respectively. In the long term after TBI, progressive RNFL degeneration is estimated at 1.47 μm per year in veterans with a history of TBI compared with 0.31μm per year in age-matched veterans with no history of TBI, associated with relative deficits in visual function including VA, visual field, and contrast sensitivity. 117 Table 4 summarizes OCT assessment in patients with TON and TBI.
Studies of Retinal and Visual Changes in Patients with Traumatic Optic Neuropathy and Traumatic Brain Injury
OCT, optical coherence tomography; TON, traumatic optic neuropathy; TD, time domain; RNFL, retinal nerve fiber layer; VA, visual acuity; SD, spectral domain; source; NLP, no light perception; GCC, ganglion cell complex; TBI, traumatic brain injury; EDTRS, early treatment diabetic retinopathy study; SS, Swept source; GCL, ganglion cell layer; RAPD, relative afferent papillary defect.
OCT as a Surrogate Marker for TBI Severity
While TON affects only 0.5–8% of patients with TBI, 35 –37 OCT abnormalities are detectable in up to 53% of patients with mild TBI with no detectable deficit in visual function. 88 The OCT is therefore able to detect subclinical damage to the afferent visual pathways. OCT, RNFL thinning also associates with cerebral white matter loss when observed using MRI, 118,119 suggesting that OCT could serve as a surrogate marker for neurodegeneration in TBI, even in the absence of clinically manifest afferent visual dysfunction. In addition, OCT has been shown to be useful in monitoring changes in retinal structure, even if they are acute, thus demonstrating potential value in predicting long-term severity of TBI.
OCT angiography (OCTA)
The OCTA uses OCT technology to noninvasively image retinal and choroidal blood flow. 120 To date, few studies report OCTA findings in TBI and TON. A case report of one patient with a diagnosis of unilateral TON (left eye) because of a vehicle collision three months before presentation showed reduced capillary density of 41.22% at the superonasal peripapillary compared with average peripapillary density of 53.92%, corresponding to RNFL thinning. 121 More recently, a study reported on the potential to achieve good OCTA images in an unconscious and intubated TBI patients. 122 While a very limited number of patient assessments are reported, these reports suggest potential for OCTA use in assessing patients with TBI.
Conclusion
Classically described TON affects a small minority of patients with TBI, causing clinically manifest, often severe, reductions in visual function that are usually symptomatic and detectable using standard subjective clinical testing. More detailed functional and structural assessments including pupillometry and OCT demonstrate that damage to the afferent visual pathway is more common than previously thought, affecting up to 53% of patients with TBI and is not always associated with detectable subjective clinical reductions in, for example, VA or visual fields. The presence of these subclinical manifestations and the association of OCT metrics with MRI brain imaging measures of neurodegeneration suggest that pupillometric and OCT assessments have the potential to serve as biomarkers for TBI severity in the months after injury.
Footnotes
Author Disclosure Statement
No competing financial interests exist.