
Abstract
Traumatic brain injury (TBI) is a risk factor for later-life dementia. Clinical and pre-clinical studies have elucidated multiple mechanisms through which TBI may influence or exacerbate multiple pathological processes underlying Alzheimer's disease and Alzheimer's disease–related dementias (AD/ADRD). The National Institutes of Health hosts triennial ADRD Summits to inform a national research agenda, and the 2019 ADRD Summit was the first to highlight “TBI and AD/ADRD Risk” as an emerging topic in the field. A multidisciplinary committee of TBI researchers with relevant expertise reviewed extant literature, identified research gaps and opportunities, and proposed draft research recommendations at the 2019 ADRD Summit. These research recommendations, further refined after broad stakeholder input at the Summit, cover four overall areas: 1) Encourage crosstalk and interdisciplinary collaboration between TBI and dementia researchers; 2) Establish infrastructure to study TBI as a risk factor for AD/ADRD; 3) Promote basic and clinical research examining the development and progression of TBI AD/ADRD neuropathologies and associated clinical symptoms; and 4) Characterize the clinical phenotype of progressive dementia associated with TBI and develop non-invasive diagnostic approaches. These recommendations recognize a need to strengthen communication and build frameworks to connect the complexity of TBI with rapidly evolving AD/ADRD research. Recommendations acknowledge TBI as a clinically and pathologically heterogeneous disease whose associations with AD/ADRDs remain incompletely understood. The recommendations highlight the scientific advantage of investigating AD/ADRD in the context of a known TBI exposure, the study of which can directly inform on disease mechanisms and treatment targets for AD/ADRDs with shared common pathways.
Introduction
Dementia is a syndrome characterized by chronic progressive deterioration of cognitive function (e.g., attention, memory, language, visuospatial skills, executive function) that is often accompanied (and sometimes preceded) by changes in emotions and behavior; these changes impact one's ability to function independently. Traumatic brain injury (TBI) has for decades been recognized as one of the strongest environmental risk factors for dementia, 1 and associations of TBI with all-cause dementia, Alzheimer's dementia (AD), and other neurodegenerative diseases have been reported in large- scale epidemiological studies, 2 –5 meta-analyses and systematic reviews. 6 -8 Nonetheless, not all studies support this conclusion, 9 –14 and important questions remain about person-specific risk (i.e., for whom does TBI confer elevated risk for the subsequent development of AD/Alzheimer's disease–related dementias (ADRDs). 11,12,15,16 The National Institute of Neurological Disorders and Stroke (NINDS)–hosted 2019 ADRD Summit was the first to include as an emerging topic a committee on TBI and AD/ADRD risk based on the contributions of TBI to neurocognitive decline and dementia diagnoses along the spectrum of AD/ADRD syndromes.
Alzheimer's dementia accounts for an estimated 60-80% of all dementia diagnoses 17 and typically presents as an amnestic multi-domain syndrome. Although the hallmark neuropathological features of AD are thought to significantly contribute to dementia, as noted in ADRD summits, mixed pathologies (i.e., AD with another pathology) are extraordinarily common in both early and late-onset Alzheimer's dementia, 18 often referred to as mixed etiology dementias. Other common forms of late-life dementia, collectively referred to as Alzheimer's disease-related dementias (ADRDs), include frontotemporal dementia, Lewy body dementia, and vascular contributions to cognitive impairment and dementia. The total number of people in the world with dementia is projected to be 82 million by 2030, and 152 million by 2050. 19 There is an urgent need to accelerate research to identify preventable contributors, treatment targets, and effective interventions. The 2012 National Plan to Address Alzheimer's Disease set an ambitious goal of preventing and effectively treating ADRDs by 2025. In so doing, the National Plan serves to coordinate federal, private, and state-level efforts to address AD/ADRD, including clinical care, support services, and research.
A primary barrier to advancing understanding the dementia risk incurred by prior history of TBI involves the lack of a common nomenclature for this area of research, propagated perhaps by varying levels of collaboration between researchers from multiple disciplines. For example, some prior studies have failed to distinguish the acute effects of TBI from those of a delayed degenerative process, and others have inadequately addressed concerns of reverse causation; as such, the committee conceptualized post-traumatic neurodegeneration as clinical decline relative to a previously achieved post-TBI level of function.
A wide range of neuropathological processes present potential mechanisms through which TBI may elevate the risk for subsequent development of AD/ADRD (Fig. 1). Some of these processes begin at the acute stage of injury and evolve chronically, while others may develop and progress years after TBI. Repetitive concussion and moderate or severe single TBI commonly induce diffuse axonal injury, which has been implicated in the rapid genesis of amyloid-beta peptides and diffuse plaques within hours after injury. 15,20 In addition, TBI can trigger phosphorylation and accumulation of tau in axons, neuroinflammation, blood–brain barrier disruption and cavum septum pellucidum. 15,21 Multiple pathological processes commonly co-exist in the brain tissue of those who survived many years following TBI; these include neurofibrillary tangles, tau astrogliopathy, diffuse and senile amyloid plaques, alpha-synuclein pathology, TAR DNA-binding protein 43 pathology, persisting neuroinflammation, 22,23 vascular changes, 24 progressive axon degeneration and brain atrophy 25 –28 to a greater extent than age-matched controls. 29,30
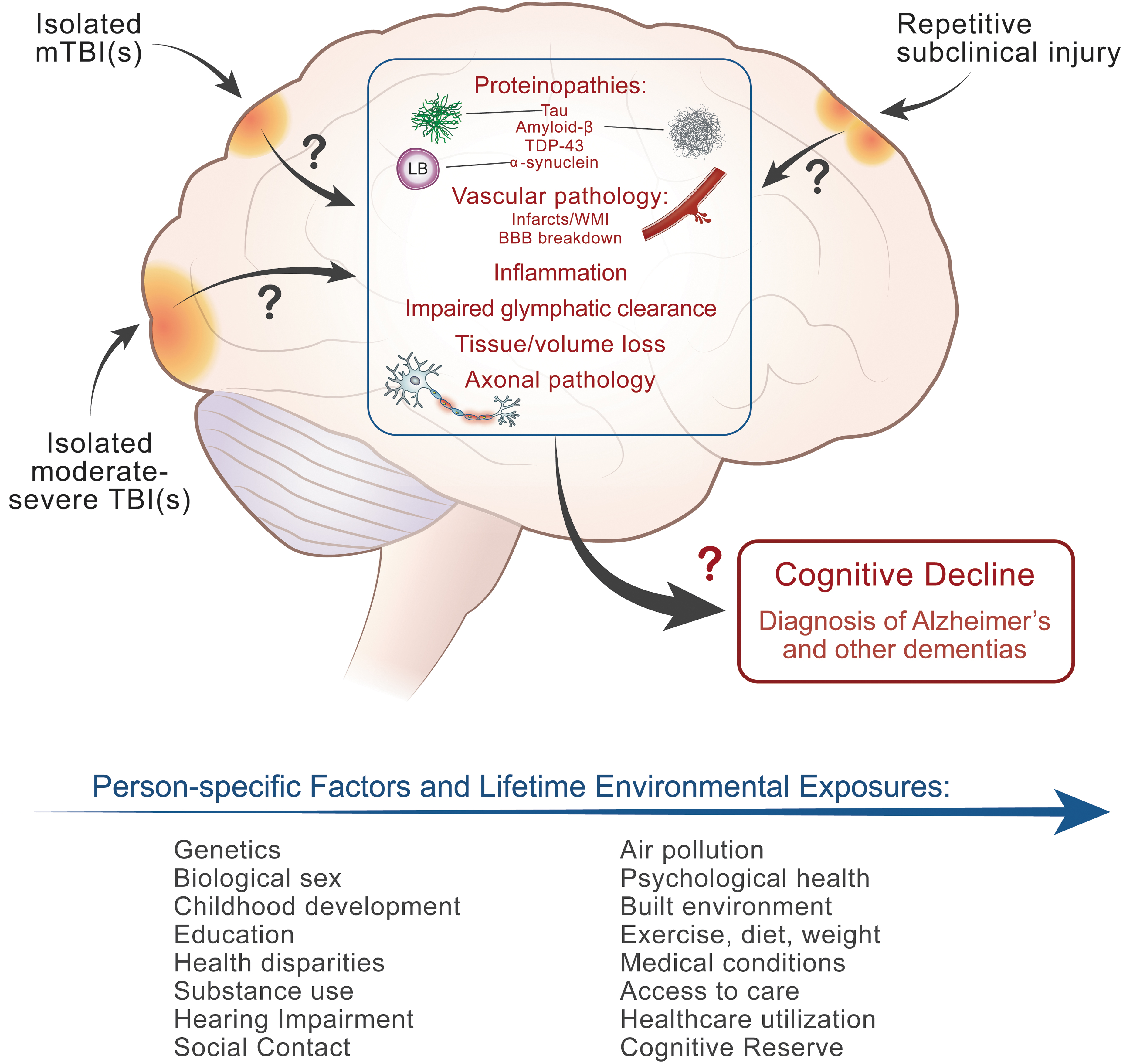
Knowledge is rapidly evolving regarding the neuropathological implications of isolated mild traumatic brain injuries (TBIs), isolated moderate-to severe TBIs, and repetitive subclinical head traumas, and their associations with cognitive decline and AD/ADRD. Clinical and neuropathological consequences of brain trauma are overlaid upon the effects of other known dementia risk factors that accumulate across the life course. Methodologically rigorous interdisciplinary research that leverages existing knowledge and infrastructure is needed to better understand the relative contributions of multiple dementia risk factors, including TBI, to cognitive impairment and dementia. mTBI, mild TBI; TDP-43, TAR DNA-binding protein 43; WMI, white matter injury; BBB, blood–brain barrier. Color image is available online.
The study of TBI offers a unique opportunity for uncovering mechanisms of AD/ADRD. Indeed, unlike other causes of neurodegeneration and dementia of unknown etiology, “time zero”—the moment of the initiating event or events—is known in those with a history of TBI. This allows for a temporal examination of the evolving clinical changes and pathological processes triggered by TBI. Conversely, we also can leverage and learn from decades of research on AD and ADRDs to inform and refine our methods. Here, we describe the proposed research priorities as recommended and refined by stakeholder input for investigation of TBI and AD/ADRD risk.
Methods
The TBI-ADRD committee followed methods deployed in the 2013 ADRD Conference 31 and 2016 ADRD Summit 32 as described below.
Pre-summit activities
Starting in late summer 2018, NINDS and National Institute on Aging (NIA) leadership and staff convened with the ADRD Summit 2019 Scientific Chair (JS) to develop an overall strategy. Together, they defined topic areas corresponding to seven summit sessions and selected scientific chairs for each session. The session chair of the TBI-ADRD committee (KDOC), together with National Institutes of Health (NIH) session leads, formed a committee by selecting from a roster of experts with broad expertise in post-traumatic neurodegeneration (DS), TBI and dementia epidemiology (MP), and TBI and dementia biomarkers (HZ). The committee met regularly via teleconference between October 2018 and March 2019 to develop and refine scientific recommendations. Because this was the first time TBI-ADRD was part of the Summit, these committees did not assess progress on the 2016 ADRD research recommendations, 32,33 but rather reviewed the scientific literature to identify gaps and priorities for formal consideration by the NINDS and National Alzheimer's Project Act (NAPA) Councils.
A joint NINDS/NIA request for information solicited public input on updating the ADRD research priorities, and NIH staff provided the committee with responses for review. Cross-committee coordination was facilitated by monthly teleconferences of the Summit Organizing Committee which consisted of scientific committee chairs; the Summit Scientific Chair (JS); NIH and other federal officials including NINDS/NIH Summit lead (RC); and the Steering Committee. 34
As an Emerging Topic session, the TBI committee had the option of proposing up to four prioritized recommendations. The committee was asked to provide an estimated timeline for initiation and establishment of fully operational status after work is initiated, which would serve to guide planning and implementation logistics. The ADRD Summit 2019 agenda and draft recommendations were then posted online and distributed to ADRD Summit registrants to gather input from stakeholders.
Summit
More than 810 individuals registered for the ADRD Summit 2019: 481 joined in person on March 14-15, 2019, and over 2,000 viewed the Summit online during or after the conference. As with the other six Topic Committees, the TBI-ADRD Chair (KDOC) provided a brief introduction to the topic area and then presented a summary of scientific rationale and draft recommendations for investigating TBI as a risk factor for common dementias. She also provided a summary of the input that was submitted by members of the research community, healthcare providers, and other stakeholders. The primary goal of these presentations was to seek public input on recommendations; thus, attendees were invited to pose questions and engage in real-time discussion after the presentation.
Post-summit follow-up
Following the summit proceedings, NINDS led a closed executive session with session chairs, NIH and other federal officials, Steering Committee members, 34 and the Scientific Chair to review the proposed revisions and edit the draft recommendations. Over teleconference, the TBI-ADRD committee met to further refine the content, prioritization, and proposed timelines for research recommendations. The final recommendations were approved and submitted to the Assistant Secretary for Planning and Evaluation at the Department of Health and Human Services. 34
Results
The committee took a holistic and interdisciplinary approach to evaluating the current state of science. As an Emerging Topic, research on TBI had not been highlighted as a specific ADRD topic area at prior Summits. The committee's recommendations were informed by decades of research on TBI, AD/ADRD and combined studies of TBI and AD/ADRD. As an Emerging Topic, in the development of its research recommendations, the TBI and AD/ADRD risk committee was asked to: 1) propose research recommendations that will be impactful in advancing the science of TBI related to AD/ADRD, especially as it relates to addressing research goals of the National Plan, and 2) encourage cross-talk and interdisciplinary collaboration between TBI and dementia researchers.
Knowledge synthesis
Results of large-scale national epidemiological and smaller cohort studies largely support an association of TBI with AD and/or ADRDs. 35 –38 The committee carefully considered many studies with contradictory findings and their inherent limitations that preclude meaningful synthesis. There are considerable methodological differences across studies, including significant concerns about inconsistent definitions for, and validity of, TBI ascertainment, injury severity, and AD/ADRD diagnosis. 39 Although some studies suggest dementia risk is greater following more severe TBIs, 8,40 methods for defining TBI severity differ considerably across studies, 12 and TBI researchers have begun to question whether traditional injury severity metrics serve their intended purpose. 41 Most of these studies do not include in vivo biological markers of post-traumatic neurodegeneration or postmortem neuropathology. Few TBI cohort studies span more than 1 year post-injury, and even fewer include control comparisons or ADRD consensus diagnostics. However, evidence suggests that up to a third of those who survive beyond 5 years post-injury experience a decline relative to a previously achieved post-injury level of function 42 and/or cognitive ability. 43 -45
There is substantial overlap in the chronic deficits that often result from moderate-severe TBI and the clinical diagnostic characteristics of AD and other ADRDs, which further underscores the importance of distinguishing the stable effects of TBI from post-traumatic neurodegeneration. Secondary analyses that use data from large prospective studies to investigate clinical symptoms in those with and without TBI suggest that TBI may alter the age of onset 46 and clinical presentation of AD/ADRDs. 38,47,48 Thus, significant questions remain, especially regarding the role of mild TBI, 49,50 and how the clinical presentation and underlying pathology of post-traumatic neurodegeneration overlap with those of AD/ADRDs.
Current knowledge about mechanisms through which TBI may initiate or exacerbate the subsequent development of AD/ADRDs (i.e., post-traumatic neurodegeneration) come largely from investigations of brain tissue collected from acute decedents and long-term survivors of TBI. Investigation of brain tissue from decedents after acute TBI has shown the rapid accumulation of neurodegenerative proteins similar to those seen in AD. 51 Whether these acute accumulations persist and/or progress to explain a later onset dementia is much less clear, as is the association of TBI with AD pathology. A clinical-pathologic epidemiologic study of TBI showed an increase in Lewy bodies and parkinsonism but no increase in hallmark AD pathology 10 ; subsequent investigations have similarly found no associations with AD neuropathology. 52
Brain autopsy is, by definition, a cross-sectional study, making it difficult to draw inferences about the associations of multi-faceted clinical symptoms with brain pathology, or to evaluate how pathology may have evolved over time. AD/ADRD risk factor studies often lack detailed information on TBI, which TBI studies have typically focused on either repetitive mild TBI 53,54 or single moderate-to-severe TBI, 55,56 rather than carefully characterizing lifetime exposure to repetitive and isolated head trauma. Studies of repetitive head trauma have been particularly vulnerable to selection bias and have focused primarily on a tauopathy described as chronic traumatic encephalopathy, despite the documented presence of numerous additional neurodegenerative, white matter, and vascular pathologies. 25 –28,57,58 Finally, few studies attempt to examine potential correlations of specific neuropathological changes with risk factors and clinical outcomes, such as dementia. There is a critical need for well-designed prospective studies including dementia outcomes and autopsy. Conversely, the neuropathology associated with single TBI and dementia requires an integrated approach with the heterogeneity of TBI as a risk factor properly interrogated.
Considerable advancements have been made in the quantification of blood-based biomarkers for TBI, which provide a clinically accessible window to investigate disease mechanisms and progression. Methods with improved analytical sensitivity compared with standard immunoassays are increasingly utilized; however, most of this work has focused on acute TBI diagnostics. The major non-metabolic cascade injury mechanisms in concussion are thought to be neuroaxonal injury followed by astrocytic and microglial activation. The best-established blood biomarkers for neuroaxonal injury are microtubule-associated protein tau (tau), which increases within hours and decreases within days after TBI, 59 ubiquitin carboxy-terminal hydrolase L1 (UCH-L1), which has similar turnover kinetics as tau, 59 and axonal neurofilament light (NfL) or neurofilament heavy, which are slow biomarkers that increase within days and plateau around 1-2 months following TBI or stroke, 60,61 with an apparent half-life of 2-3 months. 62 Chronic NfL increase after TBI may indicate TBI-induced long-term neurodegeneration. 63
The best-established blood biomarker for astrocytic activation is glial fibrillary acidic protein (GFAP). Biphasic increase of blood GFAP concentration acutely and then after months could reflect acute astroglial injury and astrogliosis, respectively. 63 Another astrocytic protein that has been extensively studied in TBI is S100B. However, extracerebral expression of this protein limits its interpretability. There is currently no established blood biomarker for microglial activation or neuroinflammation; to study such processes in biofluids, cerebrospinal fluid analysis is needed. Using these accessible candidate biomarkers, we now need to investigate them in longitudinal studies in relation to AD/ADRD clinical phenotypes and also in relation to in vivo and ex vivo AD/ADRD pathologies.
Current gaps in knowledge regarding TBI as a risk factor for AD/ADRD largely reflect practical obstacles that can be overcome with investments in research infrastructure, thoughtful approaches to study design, and analytic methods. At the time of the 2019 ADRD Summit, there were very few TBI brain tissue archives, a paucity of detailed clinical data available, and no standardization of protocols for neuropathological examination or clinical data harmonization. The largest TBI and repetitive head trauma brain archives 64,65 are limited by poor clinical characterization and/or selection bias in that participation in brain donation may be associated with head trauma exposure severity and/or pre-mortem neuropsychiatric symptomatology. Rapidly evolving blood biomarker technologies were underutilized in chronic TBI studies, and cross-talk between TBI and AD/ADRD researchers, biostatisticians, and epidemiologists was lacking. It remains clear that sensitive and specific biomarkers in prospective cohort studies with autopsy endpoints, combined with experimental models that accurately replicate the human condition are both essential and attainable.
Incorporation of stakeholder input
During open discussion at the ADRD Summit, participants discussed the potential role of subclinical concussions and repetitive head trauma in AD/ADRD risk. This supported a knowledge gap in how head trauma exposure patterns, injury severity, and injury etiology may impact AD/ADRD risk. There was discussion of the impact of neuroinflammation in AD/ADRD and how TBI-related chronic systemic and brain inflammation may interact with other pathological processes. Participants agreed that longitudinal studies with excellent injury exposure characterization and autopsy endpoints permitting pathological studies are needed to fill these gaps. There were also comments about the need to consider many other risk factors that often co-occur with TBI, such as post-traumatic stress disorder (PTSD) given its high prevalence in military populations, 66 -68 which underscored the need to utilize epidemiological methods for causal inference through interdisciplinary collaboration.
Priorities for the investigation of TBI and AD/ADRD risk
Final recommendations (Table 1) reflect gaps in scientific knowledge and research priorities as reported by the scientific and stakeholder communities. The committee identified opportunities for TBI researchers to learn from and collaborate with interdisciplinary investigators in the fields of aging and dementia, biostatistics and life course epidemiology, building on and expanding existing infrastructure. The use of common data elements is encouraged to facilitate data sharing and open science. Recommendations span pre-clinical and clinical methods to investigate underlying mechanisms and their clinical manifestations to define post-traumatic neurodegeneration and better understand its relationship to AD/ADRDs.
Recommendations for the Study of TBI and AD/ADRD Risk
TBI, traumatic brain injury; AD/ADRD, Alzheimer's disease and Alzheimer's disease-related dementias; PTSD, post-traumatic stress disorder.
Discussion
The Draft Prioritized Recommendations 34 were submitted to National Advisory Neurological Disorders and Stroke Council and the NAPA Council and were approved as research milestones in the National Plan to Address Alzheimer's Disease that will inform the Department of Health and Human Services, the NIH, and the entire national and international research community on high priority steps to advance TBI research related to AD/ADRD outcomes. Since the 2019 Summit, advancements consistent with these recommendations include the publication of consensus-based chronic traumatic encephalopathy 69 and traumatic encephalopathy syndrome 70 research diagnostic criteria, and the launch of an NIH/NINDS-supported effort to define common data elements (CDEs) for the postmortem neuropathologic investigation of brain tissue derived from decedents with a history of TBI, as well as CDEs for postmortem clinical characterization of TBI decedents per informant report. With a known exposure and tremendous opportunity to learn from and leverage decades of dementia research and expanding TBI research infrastructure, the final recommendations are expected to yield short-term and long-term advancements in our understanding of whether and how TBI initiates and/or accelerates AD/ADRD risk, while also informing upon the neurogenesis of AD/ADRDs.
Funding Information
The conference was supported by NINDS, organized in collaboration with NIA, with assistance from the NIH Office of Disease Prevention, the Foundation for the National Institutes of Health with support from their contributors: Alzheimer's Association; GHR Foundation; Biogen; Accelerate Cure/Treatments for Alzheimer's Disease (ACT-AD) Coalition; Alzheimer's Drug Discovery Foundation; American Stroke Association, a division of the American Heart Association; CurePSP; EIP Pharma; the John A. Hartford Foundation; and the WellMed Charitable Foundation.
Footnotes
Author Disclosure Statement
HZ is a Wallenberg Scholar and has served at scientific advisory boards for Eisai, Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, Nervgen, AZTherapies and CogRx, has given lectures in symposia sponsored by Cellectricon, Fujirebio, Alzecure and Biogen, and is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program.
MJP reports no disclosures relevant to the manuscript; her time was supported by VA Health Services Research and Development Service Research Career Scientist Award, (RCS 17-297, Award No IK6HX002608).
For the other authors, no competing financial interests were reported.