
Abstract
Loss of upper extremity function following spinal cord injury (SCI) can have devastating consequences on quality of life. Peripheral nerve transfer surgery aims to restore motor control of upper extremities following cervical SCI and is poised to revolutionize surgical management in this population. The surgery involves dividing an expendable donor nerve above the level of the spinal lesion and coapting it to a recipient nerve arising from the lesional or infralesional segment of the injured cord. In order to maximize outcomes in this complex patient population, refinements in surgical technique need to be integrated with principles of spinal cord medicine and basic science. Deciding on the ideal timing of nerve transfer surgery is one aspect of care that is critical to maximizing recovery and has received very little attention to date in the literature. This complex topic is reviewed, with a focus on expectations for spontaneous recovery within upper motor neuron components of the injury, balanced against the need for expeditious re-innervation for lower motor neuron elements of the injury. The discussion also considers the case of a patient with C6 motor complete SCI in whom myotomes without electrodiagnostic evidence of denervation spontaneously improved by 6 months post-injury, thereby adjusting the surgical plan. The relevant concepts are integrated into a clinical algorithm with recommendations that consider maximal opportunity for spontaneous clinical improvement post-injury while avoiding excessive delays that may adversely affect patient outcomes.
Introduction
Upper extremity paralysis from spinal cord injury (SCI) can have devastating consequences on function and quality of life. 1 –4 SCI often produces simultaneous, but physiologically distinct lesions within both the upper motor neuron (UMN) and lower motor neuron (LMN) circuits. 5,6 The LMN circuit extends from the anterior horn cell to the distal neuromuscular junction. If the LMN is disrupted by the injury to the anterior horn cells as part of the SCI, or with concomitant peripheral nerve injury, the peripheral targets are said to be denervated. For the purpose of distinction within this discussion, if the LMN fibers remain intact but are no longer receiving descending input because of a more cephalad UMN lesion, the peripheral target is referred to as paralyzed.
The emergence of peripheral nerve transfers as a reconstructive option has the potential to revolutionize treatment and functional recovery for debilitating cervical SCI. The surgical technique to restore upper limb function with a peripheral nerve transfer involves mobilizing an expendable/functionally redundant, intact motor nerve and coapting it to a recipient nerve close to its denervated or paralyzed peripheral target muscle. 7,8 Individuals who have undergone nerve transfers in tetraplegia show significant improvement in muscle strength and functional outcome measures. 9,10 There are many established nerve transfer options for managing complex peripheral nerve injury, but the mainstay nerve transfers to restore function in SCI include: (1) brachialis branch of the musculocutaneous nerve or extensor carpi radialis brevis branch of the radial nerve to the anterior interosseous nerve (AIN), to restore digit flexion; (2) supinator branch of the radial nerve to the posterior interosseous nerve (PIN), for digit extension; (3) posterior deltoid or teres minor branches of the axillary nerve to triceps nerve, to restore elbow extension. 11 –13
Whether for UMN or LMN injury, the primary advantage of performing a nerve transfer close to the denervated or paralyzed recipient target is that it dramatically shortens the distance and time required for re-innervation of motor endplates. If the period of denervation for LMN injury is too long (i.e., >18 months), functional re-innervation will not occur, because of the irreversible resorption of motor endplates, loss of myocyte progenitor (satellite) cells, and fibrofatty replacement of muscle tissue. 14 –18 This principle applies to injury at any position along the length of the LMN and has led to a prevailing philosophy that earlier surgical intervention avoids the harmful effects of chronic denervation. 8 However, this conflicts with our current understanding of the natural history of spontaneous recovery in SCI within the lesional and infralesional spinal segments, in which clinical improvements can be observed for ≥1 year following injury. 19 –23 This apparent conflict and its impact on the timing of surgical intervention requires careful consideration to optimize outcomes following peripheral nerve transfers in SCI.
The timing of peripheral nerve surgery in SCI patients, while balancing the considerations for UMN and LMN lesions alone or in combination, has not been thoroughly examined. UMN considerations for surgical timing include the fact that although LMNs are not disconnected from their target muscle in the context of isolated UMN injury, they do undergo significant alteration at the neuromuscular junction and muscle composition over time. 24 In addition, there is a reduction in the spinal motoneuron pool available to support denervated muscle via “transsynaptic degeneration.” 25 Third is the consistent potential for limited, albeit meaningful spontaneous recovery of motor function through a variety of mechanisms over the first 6–12 months post-injury. 19 –23 The purpose of this review is to outline a conceptual framework around the ideal timing of nerve transfers in SCI that considers maximal opportunity for spontaneous clinical improvement post-injury, but also avoidance of excessive delays that adversely affect patient outcomes. These considerations will be discussed around a case example and a timing algorithm presented to facilitate surgical decision making in patients with cervical SCI.
Case Presentation
A 20-year-old male sustained a C5 American Spinal Injury Association Impairment Scale (AIS) A SCI (complete injury) following a motor vehicle accident. He underwent acute spinal stabilization with instrumented fusion from C5 to T2. Imaging at the time of injury demonstrated significant compression and displacement, vasogenic edema extending from C5 to T2 and the hydromyelia cavity into the lower thoracic cord and upper cervical cord (Fig. 1A). He was first evaluated in an interdisciplinary peripheral nerve injury clinic 2.5 months following injury. Motor examination, as per Medical Research Council (MRC) scale, demonstrated the following levels of strength (right and left): shoulder abduction 5 and 5, elbow flexion 5 and 5, elbow extension 4 and 4, wrist extension 5 and 5, wrist flexion 4 and 2, and finger extension (extensor digitorum communis [EDC]) 1 and 0. Digit flexion and intrinsic function were absent bilaterally (grade 0). Pinprick sensation was intact to C6 on the right and C5 on the left, with no sharp or dull discrimination below this level.
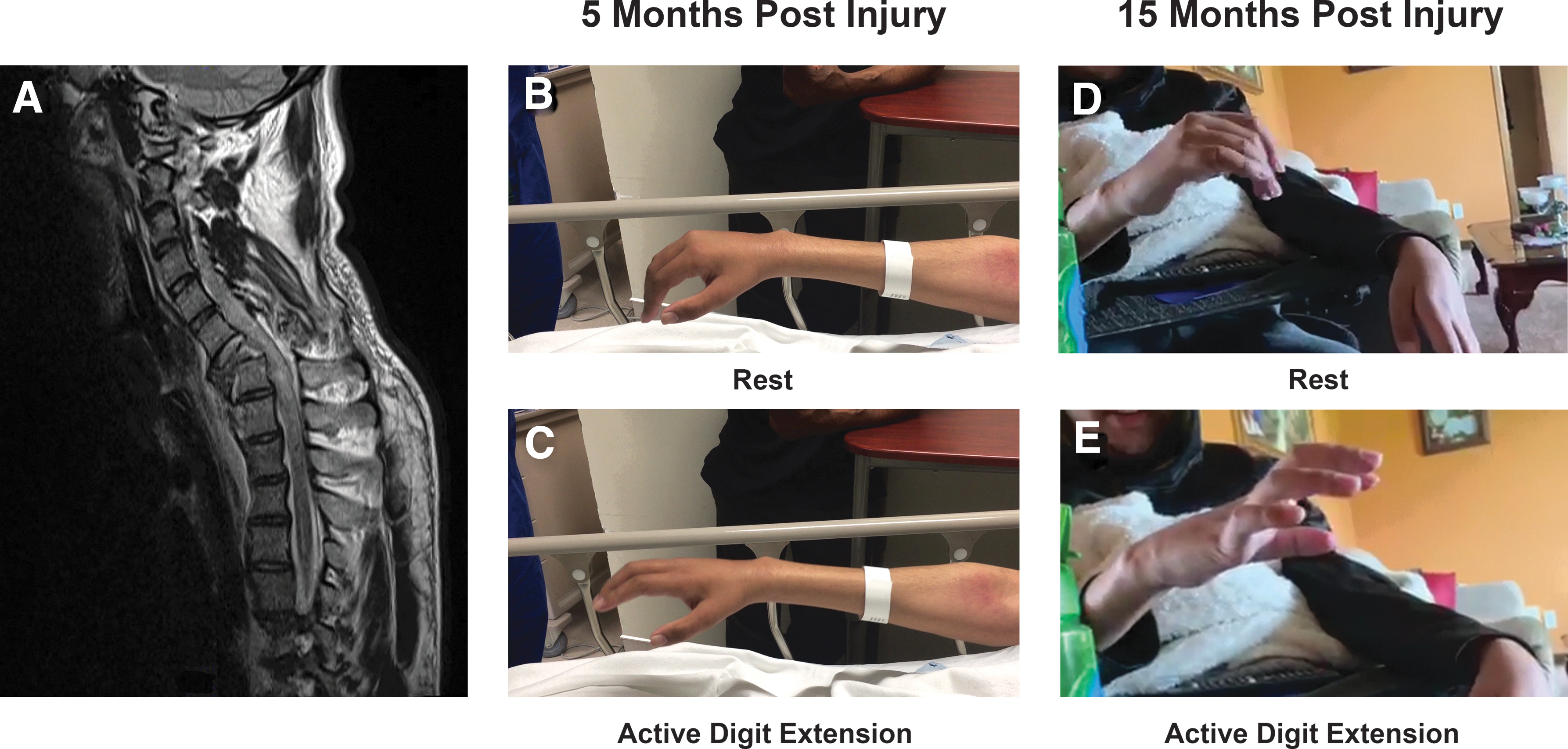
Recovery of right hand digit extension. Case of a 23-year-old male with C5 American Spinal Injury Association Impairment Scale (AIS) A SCI (complete spinal cord injury).
Electrodiagnostic (EDX) studies were performed 2.5 months post-injury including nerve conduction studies (NCS) to evaluate parameters such as conduction latency/velocity and signal amplitude, and electromyography (EMG) to assess muscle resting membrane activity and voluntary activation (Table 1). Pre-operative EDX is an essential element of the planning stages of nerve transfers in cervical SCI, with both NCS and EMG each providing useful information on donor and recipient nerve integrity. 5,26,27 There was evidence of an infralesional LMN injury involving C8-T1 based on the muscles examined. EDC did not demonstrate evidence of significant denervation, despite only a flicker of palpable voluntary activation on clinical examination (grade 1), raising the possibility of a UMN lesion to this myotome. Potential supralesional donors did not demonstrate any evidence of denervation. Note that EDX of several neuromuscular units was limited in this patient because of significant intolerance, for both NCS and needle EMG, and prominent autonomic dysreflexia.
Electrodiagnostic Data of 20-Year-Old Patient with Complete C5 ASIA A Spinal Cord Injury, Demonstrating Electrodiagnostically Normal EDC at 2.5 Months Despite MRC Grade 1 Power
ADM, abductor digiti minimi; amp, amplitude; APB, abductor pollicis brevis; ASIA, American Spinal Injury Association; config, configuration; decr, decreased; dig, digit; dur, duration; ECRB, extensor carpi radialis brevis; EDC, extensor digitorum communis; EPL, extensor pollicis longus; fasc, fasciculations; fib, fibrillations; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; incr, increased; IA, insertional activity; MRC, Medical Research Council; MU, motor unit; MUAP, motor unit action potential; NR, no response; PSW, positive sharp wave.
The patient was booked for staged bilateral nerve transfers, including brachialis branch of the musculocutaneous nerve-to-AIN and the nerve to supinator-to-PIN. When the patient presented for his initial right-sided procedure at 5 months post-injury, the supinator-to-PIN nerve transfer was aborted given that he had managed to recover satisfactory anti-gravity metacarpophalangeal (MCP) joint extension (grade 3) at this early time point, an improvement from MRC grade 1 at 2.5 months, and no evidence of denervation on EMG (Fig. 1B, C). He would later go on to recover grade 4 MCP extension of second to fifth digits spontaneously on examination at the 15-month mark (Fig. 1D, E). Ultimately, the patient underwent right sided brachialis-to-AIN nerve transfer, followed by dual transfers on the left side 8 weeks later (brachialis-to-AIN and supinator-to-PIN).
This case illustrates a number of important points in the surgical decision making for nerve transfers in SCI. First, serial examination is essential given the changes in the clinical examination findings within myotomes arising from the lesional segment of the injured cord over the first 6 months following SCI. Second, it demonstrates the important role of early EDX evaluation to distinguish between UMN and LMN patterns of injury. For those myotomes demonstrating UMN involvement, surgery should be delayed for 6 months, as much of the spontaneous recovery typically occurs within this time frame. 19 As seen in this case example, we observed that EDC, with reported C7 (greater than C8) predominant innervation, 28,29 improved from grade 1 (2.5 months post injury), to grade 3 (5 months), and later to grade 4 (15 months post injury). This compares with extensor pollicis longus (EPL) with reported C8 (greater than C7) predominant innervation, 28,30 which was grade 0 at 15 months.
Literature Review
UMN lesion (“paralysis”) influence on timing for peripheral nerve transfers
Consideration of the anatomy of a spinal cord lesion and its relationship to peripheral nerve transfer illustrates several important concepts. The injured spinal cord can be divided into three distinct segments: supralesional, lesional or injured metamere, and infralesional (Fig. 2). 6,31 –33 The supralesional segment of the spinal cord is located cephalad to the level of injury and contains intact, uninjured UMN and LMNs (Fig. 2A). It is from this supralesional segment that expendable donor motor nerves can be mobilized, divided distally, and coapted to recipient nerves within the lesional or infralesional segments to restore function. 11,12 The lesional segment describes the multi-level zone of injured spinal tissue that can involve the descending corticospinal tracts (UMN) and/or the anterior horn cells (LMN). 6 A mixed UMN and LMN pattern of injury is often observed within the lesional segment (Fig. 2B). 32 This zone may extend over several levels cephalad and/or caudad from the location of primary injury as a consequence of the secondary injury cascade caused by edema, venous stasis, compromised blood supply, inflammation, excitotoxins, and other factors. 6,34,35 The infralesional segment features a structurally intact LMN circuit that lacks the descending input/volitional control as a result of an UMN lesion (Fig. 2C). 31 Within the infralesional segment, corticospinal tract axons are functionally disconnected from the LMN and will not undergo spontaneous reconnection. 36 Transferring a donor nerve from a supralesional to an infralesional segment restores volitional control via elongation of donor axons that will re-innervate recipient muscle motor endplates. 11
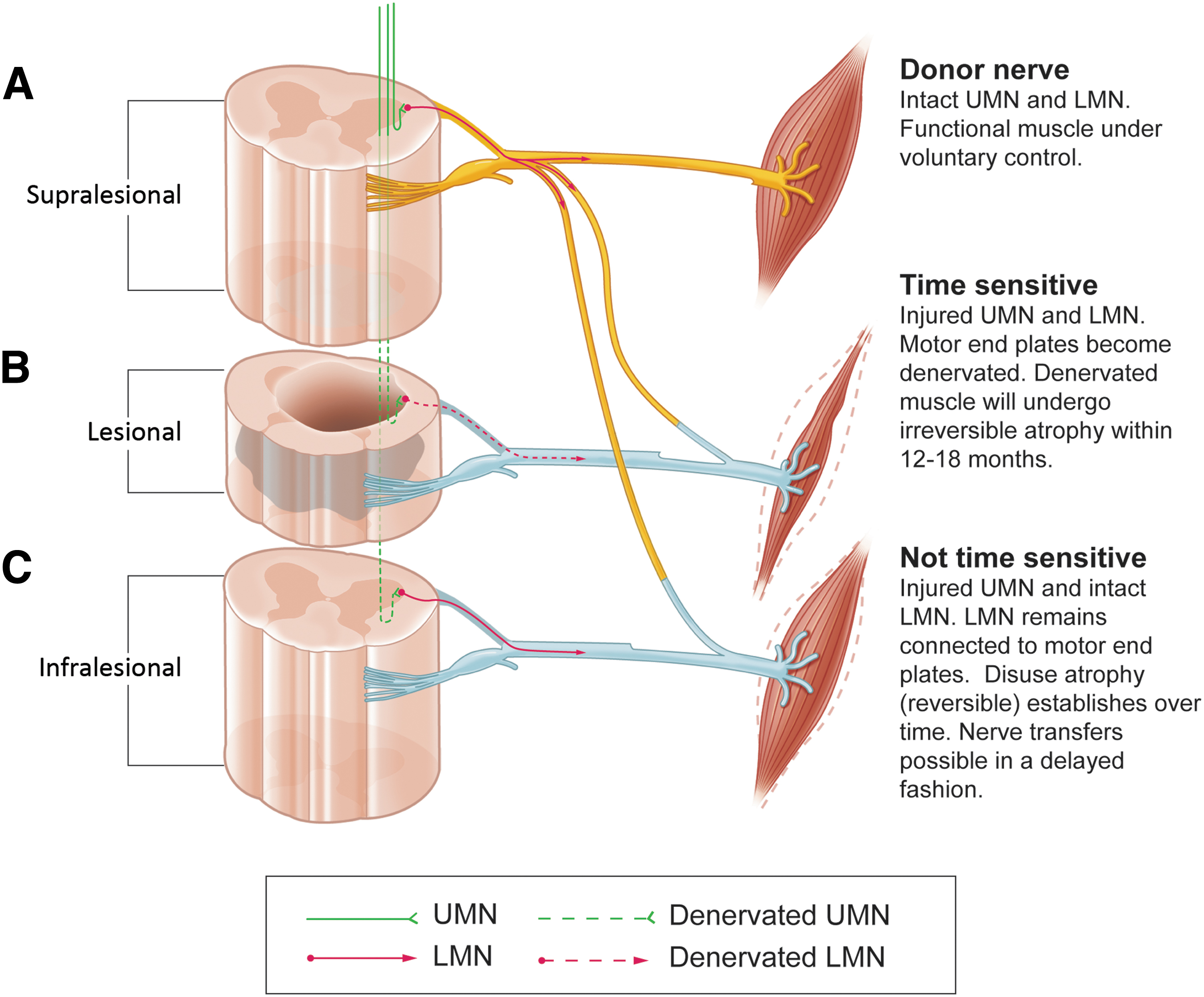
Levels of spinal cord injury and timing considerations.
Delayed peripheral nerve transfers are theoretically possible for UMN lesions given that the integrity of LMNs and motor endplates is maintained for an extended period of time. Muscles remain innervated and do not undergo the rapid irreversible atrophy and fibrosis, as seen in LMN lesions. 31,37,38 In a study of long-term outcomes of people with complete paraplegia, it was found that after an initial phase of rapid muscle atrophy, subsequent atrophy occurred slowly and muscle fibers maintained normal striated appearance after 15–20 years. 38 Consequently, restorative nerve transfers into the infralesional segment may be performed many years post-injury and have historically been considered “not time-sensitive.” 11,32,39,40
Despite the conventional notion that peripheral nerve transfers into the infralesional segment are not time-sensitive, there is an abundance of evidence demonstrating time-related changes in candidate recipient muscles within the infralesional segment. First, motor endplate numbers diminish over time with a subsequent gradual denervation of the corresponding muscle fibers. 38,41 –43 Also, predominant type II fiber atrophy is seen within the first several months along with a gradual decrease in oxidative enzymatic activity. 24 This is later followed by type I fiber atrophy. Muscle fiber type transitions toward the predominantly fast glycolytic type IIX fibers until the steady state is reached ∼70 months post-SCI. 24 The cumulative effect of these time-dependent changes diminishes muscle performance through progressively declining force-output and endurance of muscles. 24,38,42 Although there are currently no data relating to the impact of these changes on muscle performance post-nerve transfer, earlier intervention may be justified for the reasons cited. In summary, preservation of LMN integrity caudal to the level of the spinal injury allows for delayed nerve transfers to restore functional control into the chronic time frame. However, earlier intervention may prove worthwhile by avoiding the changes in recipient muscle that have been noted. The previously described case features a mixture of UMN and LMN lesions within the affected myotomes. Here, the duration in which to observe the UMN injury to EDC is constrained by the adjacent LMN pattern of injury to C8 and T1 levels.
Expectations for recovery following SCI
The potential for meaningful partial recovery during the 1st year post-injury is a concept not often discussed, yet it is highly relevant to the timing of peripheral nerve transfers in tetraplegia, particularly within the lesional segment of the injured cord. This recovery profile is summarized in the Paralyzed Veterans of America (PVA) clinical practice guidelines, 44 which outline the observed incidence of spontaneous recovery of MRC grade 3 upper extremity power in the SCI population, defined as full range of motion against gravity. 45 The extent of motor recovery in complete SCI is greatest in the first 3 months post-injury, declining until 6 months post-injury, and plateauing at ∼9–12 months. 19,45,46 Spontaneous recovery is stratified by spinal level in reference to the lowest spinal level demonstrating at least grade 3 power on initial examination, within 3 days post-injury. This level corresponds to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) level of motor injury, hereafter referred to as the “motor level.” One spinal level below this motor level, 82% of grade 1–2 muscles will reach grade 3 power or better at 6 months post-injury, with 90% reaching antigravity power at 1 year post-injury. 20,44 In comparison, only 36% of grade 0 muscles at this spinal level will reach grade 3 power or better by 6 months and only 45% will reach this level by 12 months. 20,23,44 The likelihood of MRC grade 0 muscles gaining antigravity power at 1 year that are located ≥2 levels below the motor level is close to 1%. 19,44 Although neurological recovery beyond 1 year has been described, 47 it is likely unreliable for the purposes of timing nerve transfer surgery and should be considered on a case-by-case basis. The mechanisms responsible for this spontaneous recovery after SCI include both passive processes such as resolution of spinal shock and re-myelination, as well as active processes such as spinal circuit reorganization and sensorimotor cortex adaptation. 48 –50 Several of these pathophysiological mechanisms are reviewed in more detail in Figure 3, but are otherwise beyond the scope of this discussion.
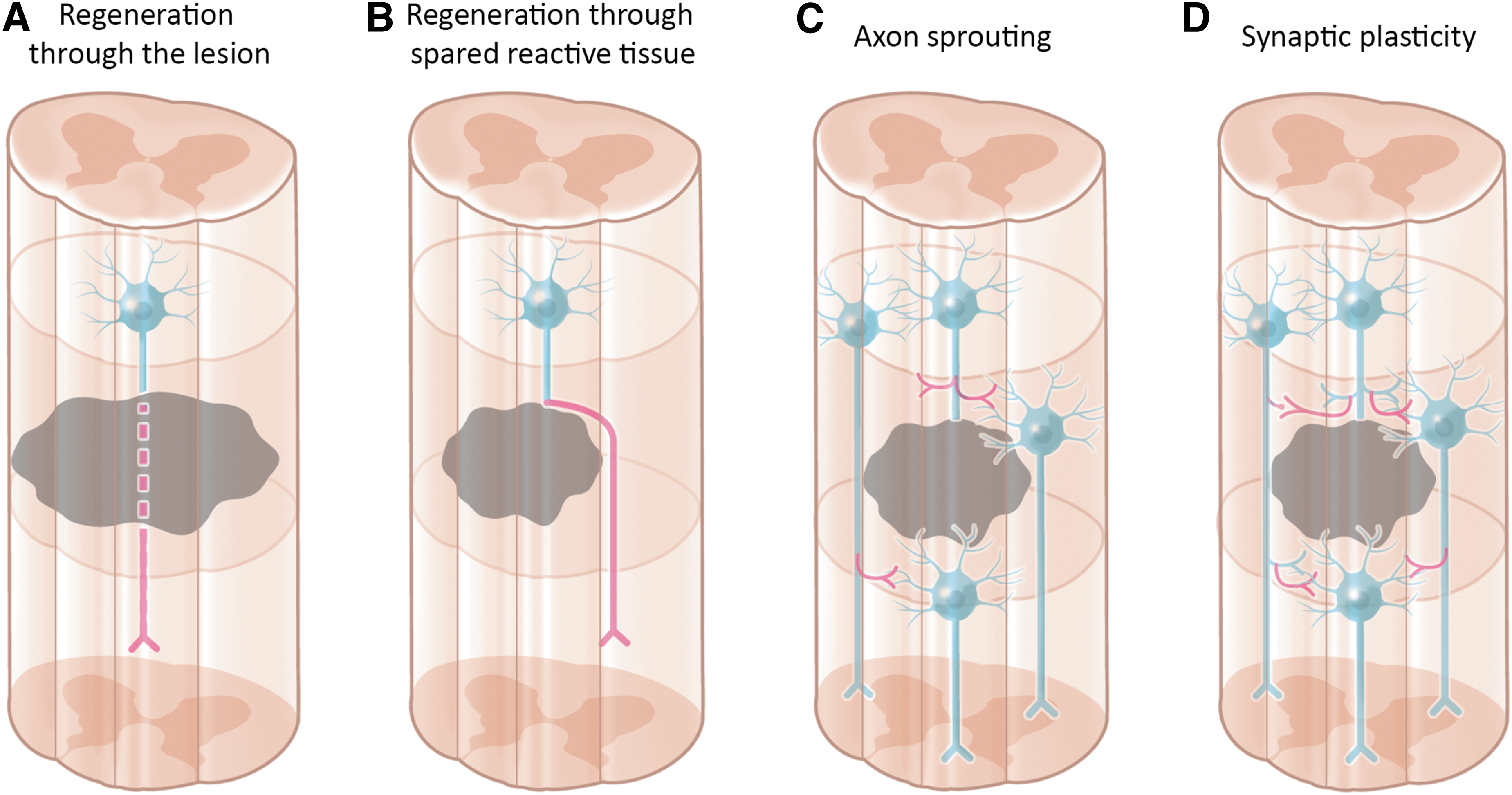
Mechanisms of spontaneous recovery in spinal cord injury (SCI). Initial short-term improvement in neurological function is attributed to processes that do not rely on neuronal elongation or re-connectivity. These include the resolution of spinal shock and/or focal conduction block, as edema decreases and re-myelination of viable axons occurs.
50,53,72
Neuronal regeneration and mechanisms of spinal cord plasticity also contribute to observed recovery. Local astrocyte proliferation and cellular activity create a dense capsule around the lesion, effectively isolating it from the surrounding tissue.
In contrast to complete SCI, incomplete injuries typically have a more favorable prognosis, and recover more quickly and to a greater extent. 46,51,52 The time frame for observed changes in motor recovery for incomplete injuries is similar, and the rate of improvement is still greatest within the first 3 months and mostly complete by 6 months. 53 Mange and coworkers 21 reported that the median time to reach grade 3 power is 2 weeks for individuals with motor incomplete injuries, versus 2 months for those with complete injuries. 44 Despite having greater potential, individuals with incomplete SCI may still experience insufficient spontaneous recovery and would be candidates for nerve transfer surgery. Candidacy, timing, and execution would be guided by the same principles as for nerve transfers in complete SCI, as demonstrated in previous case reports. 54
Given the foregoing discussion outlining spontaneous recovery reaching a maximum at 12 months, nerve transfers for a pure UMN lesion could be delayed until after 1 year post-injury (Fig. 4A). However, in practice, cervical SCI presents with a heterogeneous and complex pattern of UMN and LMN injury; 5,55 therefore, purely UMN injury patterns are rarely encountered. This section highlights the inherent capacity for limited spontaneous recovery within the 1st year after SCI. This fact needs to be balanced against the priority for early surgical intervention to address the LMN components of the injury.

Recommended timing for nerve transfer surgery.
LMN lesion (“denervation”) influence on timing for peripheral nerve transfers
Injury to the LMN as part of SCI has its own considerations for the timing nerve transfer surgery, including time from injury and distance for donor axons to reach their target muscle after reconstruction. 33,39 Whether at the level of the anterior horn cell or more distally within the peripheral nerve, injury to the LMN leads to Wallerian degeneration and subsequent denervation of motor endplates. 17,56 As a consequence, within 1 month of denervation, muscle loses >60% of its mass and 90% of its maximal force as a result of atrophy. 8 Irreversible muscle atrophy and fibrosis occurs within 12–18 months from denervation, defining the maximal time frame in which donor axons must reach their targets following nerve transfers. 39,57 –60 In the context of suspected concomitant peripheral nerve injury, an appropriate period of observation for spontaneous recovery is warranted given that spontaneous recovery is often functionally superior than that achieved with nerve transfer surgery. 61 However, once a decision to perform nerve transfers is made, there is evidence that outcomes are superior if surgery is performed within 6 months from the time of injury. 61,62 It follows that a reasonable time frame for surgical intervention for an isolated LMN injury is between 3 and 6 months, with earlier transfers for more proximal injuries (Fig. 4B).
Two additional points bear consideration related to the timing of nerve transfers in the context of LMN injury. First, partial spontaneous recovery may plateau after an appropriate period of observation. In the event that the degree of recovery is not sufficient for function, nerve transfers may be desired, but without compromising the recovery already achieved. In these circumstances, an end-to-side nerve transfer may be employed, whereby the donor nerve is coapted to the side of the recipient nerve via an epineurial window. This technique spares disruption of partially retained or recovered motoneurons and is a well-justified technique to augment native motor recovery. 39,63 –67 Second, given that the surgical technique involves complete axotomy of the recipient nerve, the design of the nerve transfer must avoid a prohibitively long distance from the location of the nerve transfer to the target musculature. The most common nerve transfers performed for cervical SCI described in the introduction typically allow motor endplate re-innervation within 1 year post injury. Relating back to the case presented, the LMN injuries to C8 and T1 levels dictate a preferred time frame of 6 months within which to perform the brachialis to anterior interosseous nerve transfers.
Mixed UMN and LMN lesions and considerations for peripheral nerve transfer timing
As discussed, cervical spinal cord lesions present with a heterogenous pattern of UMN and LMN involvement throughout the lesional and infralesional segments. Accordingly, selecting the ideal timing for nerve transfers in SCI requires balanced consideration of potential spontaneous recovery of UMN components and expeditious re-innervation for LMN components of the injury. For example, if a given muscle manifesting paralysis exhibits grade 0 power at 6 months, the likelihood of gaining meaningful functional recovery is very low, and therefore surgery is indicated. 31,68,69 The upper time limit in a mixed pattern of injury is bounded by the time frame for irreversible denervation, 12–18 months, while taking into account the anticipated time required by donor axons to reach their target. The lower limit of timing is defined by the window of expected spontaneous recovery in SCI; namely, 6–9 months. Blending these considerations defines an ideal window of nerve transfers of 6–9 months, and ideally no later than 12 months if an associated LMN pattern exists (Fig. 4C). 42,43,60,70 The case presented here highlights the importance of a reasonable period of observation for myotomes arising from the lesional segment of the injured spinal cord. Had the supinator to posterior interosseous nerve transfer been performed at an earlier time point on the right side, the eventual native spontaneous digit extensor function would have been sacrificed along with the resulting natural, intuitive control that the patient has now recovered.
Timing for nerve transfers in the setting of chronic SCI, in which LMN considerations no longer factor into surgical timing, can be performed at the discretion of the reconstructive team. That said, the impact of chronic structural and physiological changes in the recipient muscle and surrounding soft tissues (such as joint contractures, for example) ought to be considered. 5 Further, general patient-related factors such as age, medical comorbidities, associated injuries, and soft tissue characteristics may also impact surgical candidacy and should factor into timing and decision making. The impact of chronic changes in muscle and the LMN on outcomes following nerve transfers has yet to be defined.
Recommendations
The goal of peripheral nerve transfer surgery in SCI is to restore function to the upper extremities when meaningful spontaneous recovery is unlikely to occur. Optimizing outcomes requires thoughtful decision making around the timing of surgery. Operating too early on recipient nerves destined for meaningful spontaneous recovery exposes patients to unnecessary surgical risk and in the event of a failed nerve transfer, compromises their functional outcome. Delaying a nerve transfer too long for LMN components of the SCI, or concomitant peripheral nerve injury, limits the potential for re-innervation, because of irreversible muscle atrophy and lost motor endplates. The following recommendations are based on the reasonable assumptions that meaningful recovery in this population includes at least antigravity power and that for a given level of power, spontaneous recovery is preferred over that gained by a nerve transfer. Accordingly, the following proposed algorithm considers: (1) the central role of the ISNCSCI intake examination within 3 days post injury, as the most uniformly accepted prognostic parameter for predicting neurological recovery post-SCI; 71 (2) the importance of electrodiagnostic studies to distinguish between paralyzed and denervated muscles, as defined previously; and (3) the need for expeditious timing of nerve transfers for denervated muscles.
All patients being screened for candidacy for peripheral nerve transfer should have an ISNCSCI examination performed, ideally within the first 3 days following injury, consistent with current clinical guidelines. If the ISNCSCI examination is outside of this time frame, then the time from injury must be taken into account to judge expected spontaneous recovery, but ultimately, decision making in this case is reliant on serial examination.
EDX studies should be conducted within an 8–12 week time frame post-injury, which accounts for practical issues such as recovery from other major injuries, improvement in general medical status, intensive care unit (ICU) discharge, and resolution of spinal shock. EDX studies should not be performed earlier than 6–8 weeks post-injury so that LMN injury associated denervation changes can be detected.
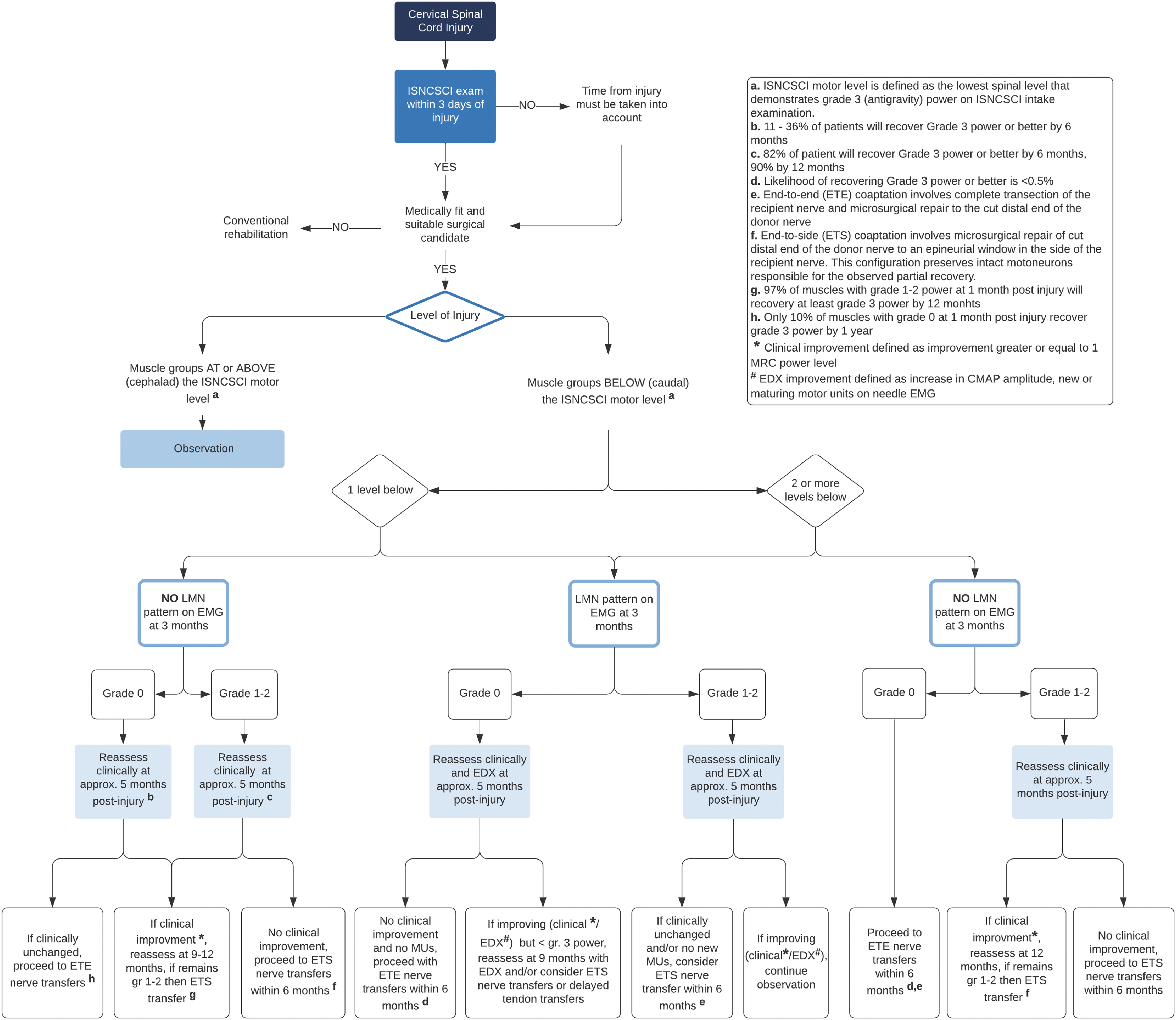
The following flow chart incorporates these varying concepts to facilitate decision making around the timing of peripheral nerve transfer surgery in SCI (Fig. 5). In this algorithm, certain principles are emphasized:
○ Observation for 6 months post-injury is indicated for all muscle groups at and above (cephalad) the motor level, as identified at the intake ISNCSCI examination.
○ For muscle groups one level below the motor level, the following should be considered in the context of the EDX findings:
▪ For muscle groups demonstrating grade 1–2 power with no features of denervation/LMN pattern on EDX, clinical reassessment is indicated at 3 and 5 months post-injury given that the UMN component of these injuries is likely to recover antigravity power spontaneously.
▪ Muscle groups demonstrating grade 1-2 power with features of denervation/LMN pattern on EDX should be reassessed clinically at 3 and 5 months post-injury. If no nascent motor units are seen, clinical improvements are less likely and end-to-side nerve transfer is indicated.
▪ Muscle groups demonstrating grade 0 power with features of denervation/LMN pattern on EDX warrant clinical reassessment at 3 and 5 months. Nerve transfers are indicated within 6 months if there is no clinical or electrodiagnostic improvement.
▪ Muscle groups demonstrating grade 0 power with no EDX features of denervation/LMN pattern should be considered for nerve transfers within 1 year.
○ For muscle groups greater than two spinal levels below the motor level:
▪ In these circumstances, without the expectation for meaningful functional recovery in UMN lesions at this level (< 1%), proceed with nerve transfers within 6 months in accordance with the ideal timing for any associated LMN injuries.
Algorithm for timing of peripheral nerve transfers in tetraplegia. Color image is available online.
Conclusion
Nerve transfers in tetraplegia have remarkable potential to restore function, yet there is a lack of guidance regarding the timing of peripheral nerve surgery given the balance between allowing spontaneous recovery from paralysis, while avoiding the irreversible effects of denervation. Thoughtful decision making around the timing of peripheral nerve transfers in SCI is critical to achieving good outcomes. The proposed algorithm begins this important discussion and serves as a framework based on existing evidence and conventional practices in SCI medicine and peripheral nerve surgery. In the case presented, serial examination revealed satisfactory spontaneous recovery of digit extensor function one level caudal to the INSCSCI motor level of impairment within 6 months from injury; therefore, the nerve transfer was aborted. This case example illustrates the importance of serial examination as well as carefully balancing spontaneous recovery after SCI with the time sensitivity of nerve transfer surgeries.
Future Directions
This study proposes a conceptual framework to inform the decision-making process when planning peripheral nerve transfers for functional reanimation in cervical SCI. Advancing the surgical care of these patients demands high-quality, prospective data from which these recommendations can be validated, and functional outcomes objectively compared. Comparisons within prospectively acquired natural history databases of cases with and without nerve transfer intervention, or well-executed meta-analyses are potential research designs that future work will explore pre- and post-implementation of this clinical algorithm.
Footnotes
Acknowledgments
The authors thank the Department of Surgery at Queen's University for supporting this publication.
Institutional Review Board Approval
Ethics approval was received from Queen's University's Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (#6030062).
Authors' Contributions
V.C. and J. M.H. were responsible for the study conception, design, manuscript drafting, and substantive revisions. M.B., B.R., and J.T. were responsible for critical analysis and substantive revisions of manuscript. All authors critically reviewed and approved the final manuscript.
Funding Information
The authors acknowledge funding from the Department of Surgery, Queen's University.
Author Disclosure Statement
No competing financial interests exist.