
Abstract
Agitation is a common behavioral problem following traumatic brain injury (TBI); however, the precise proportion of patients who experience agitation in the early stages of recovery is unknown. The aim of this systematic review and meta-analysis was to evaluate the prevalence of agitation in TBI patients undergoing inpatient care, and whether this prevalence differed by post-traumatic amnesia (PTA) status and setting (acute and rehabilitation). We also aimed to describe the prevalence of sub-types of agitated behavior (disinhibited, aggressive, and emotionally labile). We searched five databases and one clinical trials register, with additional review of websites and key journals to identify any relevant records up to July 2020. We included studies describing the proportion of hospitalized TBI patients age 16 years or older demonstrating agitated behavior. We included comparative studies with and without concurrent controls, randomized controlled trials, pseudo-randomized controlled trials, and case series. Methodological quality was critically appraised using a Joanna Briggs Institute checklist. Sixteen studies met eligibility criteria, with a total of 5592 participants. The pooled prevalence of agitation was 31.73% (95% confidence interval [CI], 25.25%-39.00%) during inpatient care (acute and rehabilitation), 32.23% (95% CI, 27.13%-37.80%) during rehabilitative care and 44.06% (95% CI, 36.15%-52.28%) for inpatients in PTA specifically. Disinhibited behaviors were the most common. There was substantial heterogeneity between studies. Additional high-quality research featuring large samples, frequent and long-term measurement of agitation, use of validated scales, and consideration of variables such as PTA status will further improve estimates of agitation prevalence following TBI.
Introduction
Agitation is a common sequela in the early stages of recovery following traumatic brain injury (TBI), and is characterized by an excess of behavior, including restlessness, aggression, disinhibition, and emotional lability. 1 The precise proportion of patients who experience agitation following TBI is unclear, with reported figures ranging widely from 6 to 96%. 2 –9 These behaviors place the patient and caregivers at risk of harm, are distressing to clinical staff and family members, and pose a significant barrier to the attainment of rehabilitation goals. 2,10,11
The considerable variability in reported agitation prevalence estimates likely stems from between-study heterogeneity in methodology, setting, and samples. The measurement of agitation varies between studies, including choice of measure, frequency of measurement, and use of retrospective or prospective designs. The use of pharmacological and non-pharmacological agitation management practices varies between inpatient settings 12 and may influence estimated prevalence depending on the efficacy of the chosen interventions. For example, the use of pharmacological interventions to manage agitation may serve to heighten or prolong these behaviors by exacerbating confusion, disorientation and drowsiness and in turn prolonging post-traumatic amnesia (PTA). 13,14 Differences in sample characteristics such as injury severity, time post-admission, age, and presence of frontal lobe damage may also contribute to variability in reported prevalence of agitation. 7,15,16
Agitation is thought to be most common during PTA, a transient period of recovery following emergence from coma characterized by confusion, disorientation, inattention, and impairment in the ability to store and retrieve new memories. 5,17,18 A patient is considered to have emerged from PTA when continuous memory for ongoing events is restored. 13 The cognitive difficulties present during PTA are theorized to interfere with the patient's ability to process and contextualize internal and external stimuli, leading to an inappropriate response in the form of agitation. 5,19,20 A temporal relationship between agitation and PTA has been demonstrated, whereby agitation tends to improve with the recovery of orientation, memory, and attention, and ultimately resolve prior to PTA clearance. 7,17,18,21 It appears that agitation may persist beyond emergence from PTA in some patients 6,18 ; however, the precise prevalence of agitation during PTA and following PTA emergence is unknown.
Differences in environmental characteristics, use of agitation management strategies, and time since injury may result in a higher prevalence of agitation in an acute setting compared with during rehabilitation hospitalization. 6,22 Although high-quality evidence to support the use of pharmacological and non-pharmacological interventions for the management of agitation is lacking, 22 –25 experts recommend the avoidance of pharmacological agents and adoption of non-pharmacological strategies in the early stages of recovery following TBI. 13,26 -28
Non-pharmacological methods of agitation management include environmental modifications (e.g., provision of familiarizing information, allocation to a single room, minimizing noise levels), behavioral strategies, and staff and family education. 13,14,22,26,28 -30 Certain recommended environmental modifications may be impractical in an acute environment (e.g., minimizing noise levels in the context of noisy but necessary alarms, use of dim lighting, allocation to single rooms) or of lower priority in the context of critical medical care. Patients may also be deeper in PTA within an acute setting due to the recency of their injury and may be more easily overwhelmed by a confusing or overstimulating environment, resulting in agitated behavior. 6,13 The presence of pain and infection resulting from new injuries 7,28,31 may additionally increase the prevalence of agitation found in the acute setting. In contrast, behavioral management and consequent engagement with multi-disciplinary therapy is of greater focus in the rehabilitation setting. A specialized rehabilitation department may feature non-pharmacological management strategies designed to minimize overstimulation and prevent the development of agitation, and potentially employs staff more likely to have specialized training in agitation management.
Agitated behaviors may be described as disinhibited (e.g., distractibility, impulsivity), aggressive (e.g., violence, oppositional behavior) or emotionally labile (e.g., excessive laughing and crying, excessive talking) in nature. 32 Of the wide spectrum of behaviors that constitute agitation, disinhibited behaviors seem to be reported most frequently, while violent behaviors are relatively rare. 7,17,22 Despite this, medical professionals tend to emphasize physical aggression and explosive anger as the behaviors most typical of agitation. 12,19 Further research is required to rectify this discrepancy and clarify which sub-behaviors of agitation are most likely to present in the early stages of recovery following TBI.
As estimates of the prevalence of agitation following TBI vary widely, it is presently unclear what proportion of patients are likely to develop agitation, in what stage of recovery and setting they are at greatest risk of developing these behaviors, and which behaviors they are most likely to exhibit. Clarifying how and when agitation is most likely to present itself will promote a better clinical understanding of factors that contribute to the development of agitated behavior, allow for accurate assessment of agitation, enhance resource allocation and patient management, and ultimately improve patient prognosis. The review questions evaluated in this systematic review and meta-analysis were therefore: What is the prevalence of agitated behaviors during inpatient care? What is the prevalence of agitated behaviors in patients in PTA and out of PTA, and does this differ significantly between these groups? What is the prevalence of agitated behaviors during acute inpatient care and rehabilitative inpatient care, and does this differ significantly between these settings? What is the prevalence of disinhibited, aggressive, and emotionally labile agitated behaviors during inpatient care and does this differ between behavior types?
Methods
This systematic review and meta-analysis was conducted and reported in line with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, 33 Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 34 and those specified by the Observational Studies in Epidemiology (MOOSE) group. 35 This review was registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42020201604). There were eight deviations from the protocol (Table 1).
Deviations from Protocol
E.g., if the proportion of patients age over 16 was not explicitly reported but supporting information such as age mean and standard deviation was available, this study was retained by author consensus.
E.g., studies including only patients who received a certain treatment, studies excluding patients receiving antipsychotics, studies including only patients with specific medical ailments.
CENTRAL, Cochrane Central Register of Controlled Trials; COVID, corona virus disease; TBI, Traumatic brain injury; WHO ICTRP, World Health Organization International Clinical Trials Registry Platform Search Portal.
Data sources and searches
The review search strategy was developed by an information specialist using key words (linked with Boolean operators) and controlled vocabulary. This strategy included terms relating to the population (TBI and agitated behaviors) and setting (initial inpatient hospitalization). Full search strategies for all searches are provided in Supplementary Appendix I. All human studies fulfilling eligibility criteria were eligible for inclusion regardless of publication date or status. The search strategy was restricted to articles available in English; however, we attempted to translate articles in languages other than English through Cochrane TaskExchange. The following databases were searched: MEDLINE, OVID SP interface (1946 to July 17, 2020); Cumulative Index to Nursing and Allied Health Literature (CINAHL; 1937 to July 19, 2020); Embase (Excerpta Medica Database) excluding MEDLINE, OVID SP interface (1974 to July 10, 2020); PsycINFO, OVID SP interface (1806 to July 17, 2020); and CENTRAL (until July 19, 2020). This search was supplemented through searches of
Inclusion criteria
Studies were selected for inclusion based on study design, participant characteristics and outcomes.
Study design
Broad study design inclusion criteria were employed as it was expected that relevant outcomes would be reported in studies that did not explicitly aim to report the prevalence of agitation. For this reason, the aim of included studies did not need to be to determine the prevalence of agitated behavior if other inclusion criteria were met. We included epidemiological studies of incidence and prevalence, descriptive cross sectional studies, randomized controlled trials, controlled non-randomized clinical trials, quasi-randomized controlled trials, controlled before and after studies, interrupted time series with a control group, interrupted time series without a parallel concurrent control group, analytical observational studies (including cohort and case-control studies), comparative studies without concurrent controls, cluster clinical trials, studies of treatment preferences, case series, and single arm studies. We excluded case reports, protocols, methodological papers, mechanism-based reasoning studies, qualitative research and reviews. For interventional studies, the proportion of patients exhibiting agitated behavior was required to be reported prior to the administration of any intervention.
Participants
This review accepted studies reporting the prevalence of agitation in adults who had sustained a penetrating or non-penetrating TBI by any mechanism and were hospitalized in an acute hospital or inpatient rehabilitation facility. We excluded studies where: <50% of participants had sustained a moderate-to-severe TBI (as determined by established criterion such as Glasgow Coma Scale score, PTA duration, duration of loss of consciousness, or qualitative descriptors of TBI severity) or outcome data for moderate and/or severe TBI was not presented separately; < 80% of participants had sustained a TBI or outcome data for TBI patients was not presented separately; < 80% of participants were inpatients or outcome data for inpatients was not presented separately; or <80% of participants were age 16 years or older or outcome data for participants age at least 16 years was not presented separately. Studies in which these characteristics were not explicitly stated were retained if the study appeared to meet criteria according to author consensus based on related information that provided insight into the missing information. For example, if the age range of included participants was not stated but mean and standard deviation suggested that patients were adults and the setting in which the study took place was not a pediatric facility, it was assumed that the study's sample was made up predominantly of adults and that the review's age criterion was met.
Where study inclusion criteria were employed, these could not impinge upon the validity of the study's reported prevalence estimate for that study to be included in the review. That is, studies were excluded if their stated eligibility criteria were too narrow (e.g., including only patients who received a certain drug during their admission), as this may impact the representativeness of the sample in these studies and therefore influence the validity of the reported prevalence estimate. Sampling was required to include all available cases at a single time-point, between two points in time, or to employ a random sampling method. No sample size restrictions were applied.
Outcomes
The outcome of interest was the proportion of patients who exhibited agitated behavior. Acceptable outcomes included agitation measured as a global construct or as sub-behaviors encompassed within the definition of agitation (e.g., inattention, restlessness, low frustration tolerance, disinhibition, perseveration, impulsivity, emotional lability, aggression). 1,36 To be considered for inclusion, agitated behavior was required to be measured prospectively using a clearly defined scale during inpatient hospitalization (e.g., Agitated Behavior Scale [ABS], 36 Neurobehavioral Rating Scale, [NRS] 37 ). Author-designed measures were accepted if the scale and its items were adequately described in the manuscript, as determined by author consensus. Need for intervention such as medication administration or restraint use was not considered an adequate measure of agitation. Measures were required to be completed by clinical staff based on behavioral observation of the patient. Self- and caregiver-report measures were not included as these were considered subject to bias in the context of recent TBI and unlikely to accurately capture agitation in the inpatient environment. Studies employing retrospective measures completed by a healthcare professional also were excluded, as these were deemed subject to recall bias or limited by the nature of qualitative medical record entries. If multiple relevant prevalence estimates were reported within a single study, all relevant outcomes were included in the review.
Outcome data was considered acceptable where this was reported as a percentage, number of patients or otherwise calculable from available data. Studies were ineligible if the outcomes of interest were not reported, although efforts were made to obtain missing information from study authors where possible.
PTA status was determined based on the use of PTA rating scales (e.g., Westmead Post Traumatic Amnesia Scale); use of terms synonymous with PTA such as post-traumatic confusional state; use of qualitative patient descriptors such as confusion, disorientation and amnesia; and time post-injury and study setting. We defined the acute setting as including both the intensive care unit (ICU) and any other inpatient setting providing initial stabilization of injury before transfer to a specialized rehabilitation facility. The rehabilitation setting was defined as inpatient hospitalization focusing on multi-disciplinary rehabilitation immediately following initial stabilization of injury in an acute facility and prior to discharge to the community. If the study sample were drawn from both acute and rehabilitation facilities, setting was classified as mixed.
Setting was determined by descriptions of setting (e.g., rehabilitation, ICU, trauma); the research environment (e.g., engagement with interdisciplinary rehabilitation services); participant characteristics (e.g., time post-injury, description of previous acute inpatient hospitalization); and the name of the hospital in which data was collected or hospital affiliation of the study's authors. Sub-behaviors of agitation were classified as disinhibited, emotionally labile, or aggressive based on the use of rating scales, terms used to label the behavior of interest, definitions of agitated behavior, and patient descriptors. These were matched against author-created descriptions of disinhibited, aggressive and emotionally labile behavior, based on the three factors of the Agitated Behavior Scale 36 and supplemented with terms used to describe agitated behavior (Supplementary Appendix II).
Study selection
Study selection for inclusion in this review, data extraction, risk of bias assessment, and selection of studies for inclusion in meta-analyses were carried out by two independent reviewers (R.K.P. and S.L.C.). Disagreements at all stages of study selection were resolved by authors J.L.P, A.M., and A.J.H. Articles in languages other than English were listed for translation on Cochrane TaskExchange. Reviewers were not blinded to journal title, study authors, or institutional affiliation.
Data extraction and risk of bias assessment
For included studies, authors R.K.P. and S.L.C. independently extracted data using a pre-piloted customized data extraction tool based on the Joanna Briggs Institute data extraction form for prevalence studies. 38 We extracted information pertaining to basic identifying information, study methodology, details of TBI, details of PTA, details of agitation, study sample, recruitment, and results. Our data extraction form is provided in Supplementary Appendix III. Authors were contacted via email when key study characteristics were not reported or were unclear (n = 18). Details of author contact are provided in Supplementary Appendix IV.
Methodological assessment
For each study, risk of bias was independently assessed by R.K.P and S.L.C. according to the Joanna Briggs Institute checklist for prevalence studies. 38 This nine-item tool rates: 1) appropriateness of the sample frame; 2) sampling method; 3) sample size; 4) description of study subjects and setting; 5) coverage of the study sample in data analysis; 6) validity of methods used for the identification of the condition; 7) whether the condition was measured in a standard and reliable way; 8) appropriateness of statistical analysis; and 9) adequacy of response rate. Each item is appraised as “yes” (met), “no” (not met), “unclear,” or “not applicable.” Any discrepancies in appraisal were settled by J.L.P., A.J.H., and A.M. No study was excluded based on degree of bias.
Statistical analysis
Authors R.K.P. and S.L.C. determined whether the following criteria were met for inclusion in meta-analysis: 1) sample frame appropriate to address the target population, as determined by question 1 of risk of bias assessment; 2) valid methods used for the identification of agitated behavior, as determined by question 6 of risk of bias assessment; 3) sample size of at least 10 participants with TBI (to minimize outlier estimates); 4) if the study included a mixed acquired brain injury sample, prevalence of agitated behavior reported separately for TBI patients; and 5) if the study involved a mixed setting, prevalence of agitated behavior reported separately for inpatients. For studies meeting these criteria, the nature of study-level variables—including PTA status (in or out of PTA) and setting (acute or rehabilitation)—were also classified to determine eligibility for inclusion in subgroup analyses. Any disagreements between reviewers were settled by J.L.P., A.J.H., and A.M.
Where studies reported multiple statistics that could be included in meta-analyses, we selected one outcome for inclusion by prioritizing outcomes that employed validated clinical cut-offs, measured agitation longitudinally, and defined significant agitation in the same way as other included studies.
Pooled proportions were estimated using the metapreg command, 39 which implements the DerSimonian and Laird procedure, within Stata Version 17.0. 40 The exact method was used to calculate confidence intervals for each estimate. A random-effects model was run to estimate the overall prevalence of agitation following TBI and the subgroup analysis of agitation prevalence in a rehabilitation setting, as the true prevalence was assumed to vary from study to study. 41 A fixed-effects model was used to calculate the subgroup analysis of prevalence of agitation in patients in PTA due to the small number of studies included in this analysis. Pooled proportions were reported together with 95% confidence intervals (CIs). Heterogeneity was evaluated using the chi-squared statistic of likelihood ratio, the I2 statistic and prediction intervals generated from the tau-squared statistic. Publication bias was assessed visually using funnel plots and statistically using Egger's method.
Sensitivity analyses were carried out to assess the impact of arbitrary or unclear decisions on the results of the meta-analysis of overall prevalence of agitation. We examined the impact of: 1) excluding studies that did not explicitly provide information pertaining to sample characteristics (e.g., age range, TBI severity breakdown) but were included in this review based on the availability of information suggesting that these criteria were met; 2) including studies with higher risk of bias in meta-analysis; and 3) using an alternate prevalence figure in studies reporting the prevalence of agitation according to multiple definitions. Reviewers chose the second most representative outcome for inclusion in sensitivity analysis in place of the estimate chosen for inclusion in the primary meta-analysis. This choice was made based on the same principles as choice of estimate for inclusion in the primary meta-analysis.
Results
Literature search
The literature search produced 16,889 articles; 16,747 from bibliographic databases and registries and 142 from additional search sources (Fig. 1). After removal of 5631 duplicates, 11,258 records were screened for inclusion. Following screening of title and abstract, 470 records were reviewed at full text. Of these, 18 of 29 studies published in languages other than English were translated via the Cochrane TaskExchange platform. The remaining 11 studies were unable to be translated due to a lack of applicants. Excluded studies are presented in Supplementary Appendices V and VI. Percentage agreement between reviewers at full-text screening was 99.79% and Cohen's K was 0.97.

Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) diagram. APA, American Psychological Association; CENTRAL, Cochrane Central Register of Controlled Trials; CINAHL, Cumulative Index to Nursing and Allied Health Literature; MEDLINE, Medical Literature Analysis and Retrieval System Online. TBI, traumatic brain injury.
Description of included studies
We identified 16 studies (19 records) meeting inclusion criteria published between 1981 and 2020. Of these, 13 studies met criteria for inclusion in meta-analyses (Table 2). Most studies were conducted in the United States (n = 8), 9,18,42 –47 followed by single studies in the United Kingdom, 48 Australia, 7 Canada, 49 Denmark, 8 the Netherlands, 16 Sweden, 50 Switzerland, 51 and a multi-site study within the United States and Canada. 31 Sample size varied widely, ranging from 1818 to 2130 31 participants, with a total sample size of 5592 participants across studies. Males outnumbered females in all studies reporting sex (n = 14) 7 -9,18,31,42 –47,49 -51 and average age ranged from 21 46 to 64 49 years.
Characteristics of Included Studies
Information obtained from author.
Prevalence estimates not explicitly reported in terms of PTA status but PTA status was able to be abstracted from text.
Proportion of patients demonstrating agitation as measured longitudinally was able to be abstracted from text.
Although not explicitly stated, this measure was determined not to be self- or caregiver-report in nature as the authors described use of direct clinical observation of the patient when completing the ABS.
Although not explicitly stated, this measure was determined not to be self- or caregiver-report in nature as the employed measure rated whether patients were comatose (making self-report impossible) and appeared to rely on formal clinical assessment.
Inclusion criteria as published elsewhere. 54
Data published in multiple forms including conference abstracts and full publications. Information for the purpose of this review and meta-analysis were obtained from the full publication.
ABS, Agitated Behavior Scale; CI, confidence interval; CSI, Comprehensive Severity Index; CT, computed tomography; DRS, Disability Rating Scale; FIM, Functional Independence Measure; GCS, Glasgow Coma Scale; GOAT, Galveston Orientation and Amnesia Test; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; ICU, intensive care unit; IQR, interquartile range; M, mean; N, no; N/A, not applicable; NRS, Neurobehavioral Rating Scale; OGMS, Orientation Group Monitoring System; O-Log, Orientation Log; PTA, post-traumatic amnesia; RASS, Richmond Agitation Sedation Scale; RLAS, Rancho Los Amigos Scale; RoB, risk of bias; SD, standard deviation; TBI, traumatic brain injury; U, unclear; USA, United States of America; WPTAS, Westmead Post Traumatic Amnesia Scale; Y, yes.
Study design and setting
Most studies employed a longitudinal cohort design (n = 14), 7 -9,16,18,31,42 -44,47 –51 and one study was cross-sectional in nature. 45 The design of one study was unclear. 46 Most studies were conducted in a rehabilitation setting (n = 13) 7 -9,18,31,42 –48,51 followed by acute (n = 2) 16,49 and mixed acute and rehabilitation settings (n = 1). 50
Sample characteristics
All studies included only patients who had sustained a TBI (i.e., there were no studies of mixed acquired brain injury populations). Severity of TBI ranged from mild to severe. Time post-injury ranged from the day of acute hospital admission 16 to a median of 10.5 weeks. 46
The proportion of the sample in PTA was reported in six studies 7,16,18,43,47,50 ; three studies reported prevalence in a pure PTA sample, 7,16,18 while the remaining three studies reported prevalence in a mixed sample of patients who were in and out of PTA, with proportion of PTA patients ranging from 40 to 64%. 43,47,50 Two studies also reported the prevalence of agitation following all patients' PTA emergence. 16,18 Post-traumatic amnesia was measured using a variety of tools, including the Orientation Group Monitoring System, 18 Orientation Log, 43, 47 Galveston Orientation and Amnesia Test, 47 Westmead Post Traumatic Amnesia Scale, 7 author-designed questionnaire, 16 and qualitative classification. 43,50 Post-traumatic amnesia status was measured prospectively by clinical staff in all studies.
Measures
Agitation was most frequently measured using the ABS 36 (n = 13). 7 -9,18,31,42 -44,47 –51 In studies rating the presence of agitation using the ABS, agitation was consistently defined as a total score of >21, in line with established clinical guidelines. 36 The number of scores >21 required for a patient to be considered agitated and the time-frame within which this threshold must be met varied (e.g., one score >21 at any time during hospital admission, ≥6 scores >21 within 48 h). Other methods of agitation measurement included author designed measures (n = 2), 16,46 the Neurobehavioral Rating Scale (NRS; n = 1) 45 and the Richmond Agitation Sedation Scale (RASS: n = 1). 49 Agitation measured using the NRS and RASS was also classified according to established clinical criteria. 37,55 Agitation was rated most often by nurses (n = 13), 7 -9,16,18,31,42 -44,47 -49,51 followed by neuropsychologists (n = 3), 7,45,48 physiotherapists (n = 2), 8,51 occupational therapists (n = 2), 8,51 psychometricians (n = 1), 45 physicians (n = 1), 16 and medical staff (n = 1). 48 The rater was unclear in two studies. 46,50 Eleven studies 7 -9,16,18,31,42,44,47 -49 reported the proportion of patients presenting with agitation as measured longitudinally. Six studies reported the proportion of patients presenting with agitation at a single time-point, 18,43,45,46,50,51 despite five of these studies measuring agitation longitudinally. 18,43,46,50,51 Start and stop rules for agitation monitoring varied in those studies measuring agitation over time. Agitation was measured each nursing shift (n = 8), 8,9,16,31,42,44,47,49 daily (n = 3), 7,43,48 weekly (n = 1), 18 at multiple pre-defined time-points (n = 1), 50,51 and at a single point in time (n = 1). 45 Frequency of measurement was unclear in one study. 46
Prevalence
Overall prevalence of agitation
Fifteen studies reported prevalence of the general construct of agitation in their sample. 7 -9,16,18,31,43 –51 The proportion of patients demonstrating agitation ranged widely from 0 16,46 to 57% 49 (Fig. 2).
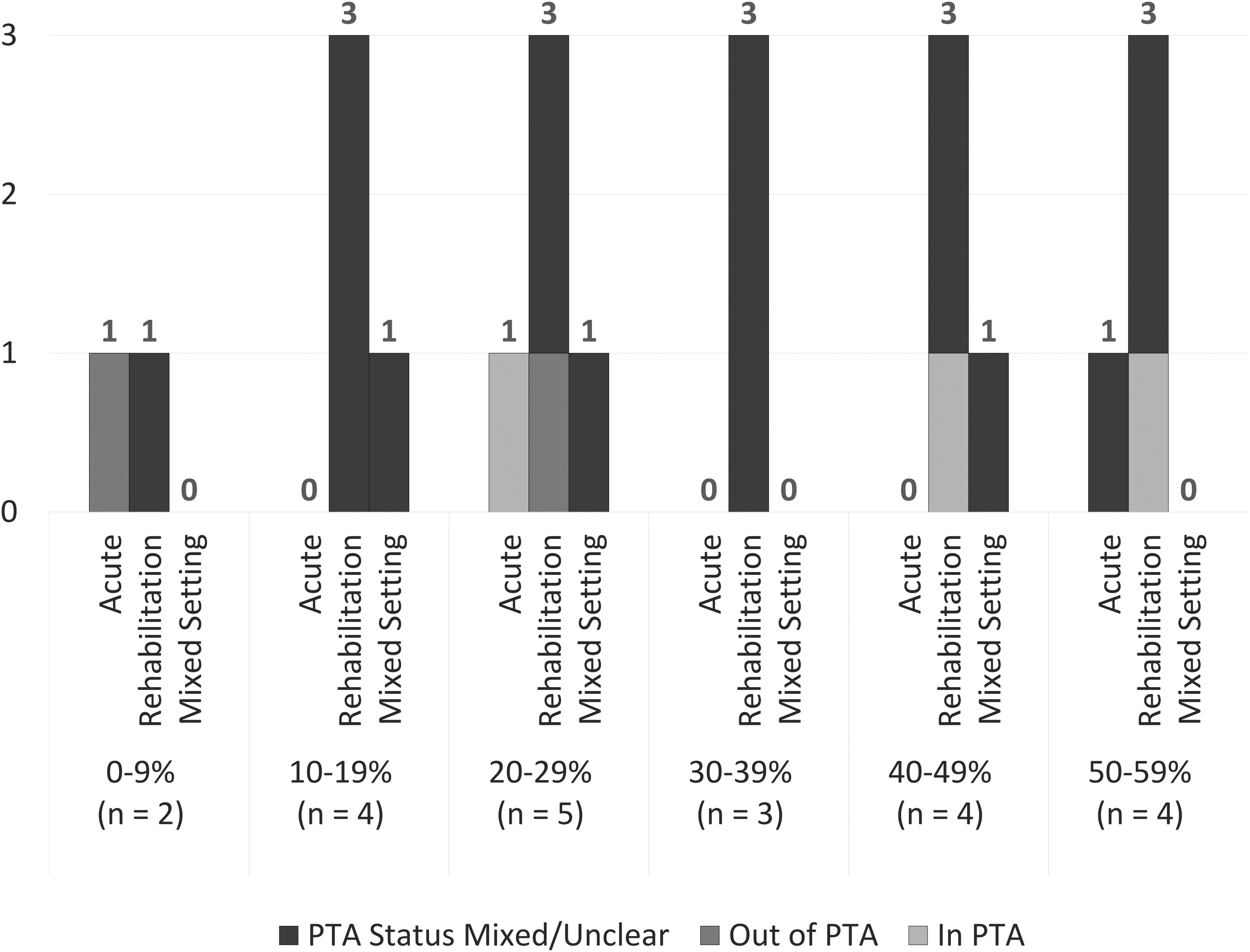
Distribution of reported prevalence by setting and PTA status. PTA, post-traumatic amnesia.
Prevalence of agitation by PTA status
Only three studies presented the overall prevalence of agitation in a sample comprising only patients in PTA, 7,16,18 with estimates ranging from 2516 to 56%. 18 One of these studies also reported the overall prevalence of agitation at the point that patients emerged from PTA to be 22%, 18 and another noted that agitation resolved prior to emergence from PTA in all patients, indicating a prevalence of 0% following PTA emergence. 16
Prevalence of agitation by setting
In the two studies conducted in an acute setting, prevalence was reported to be 25% 16 and 57%. 49 Of the 12 studies focused on inpatient rehabilitation settings, 7 -9,18,31,43 –48,51 the prevalence of agitation ranged from 016 to 42%. 7 One study reported the prevalence of agitation to be between 12 and 47% in a mixed acute and rehabilitation setting, with estimates varying according to the definition of agitation used. 50
Prevalence of agitation by sub-behavior
Six studies described the prevalence of agitated sub-behaviors. 7,16,42,45,46,49 Disinhibited behaviors were most frequently measured (n = 6), 7,16,42,45,46,49 followed by emotionally labile (n = 4) 7,42,45,49 and aggressive behaviors (n = 3). 7,42,49 Three studies reported the proportion of patients displaying individual agitated behaviors on the ABS, 7,42,49 while other studies utilized the NRS 45 and self-constructed measures.16 46
Prevalence ranges for each ABS item are displayed in Table 3. Disinhibited items tended to be the most commonly endorsed, followed by emotionally labile and aggressive behaviors. However, the reported proportion of patients demonstrating each behavior varied substantially. Studies not employing the ABS reported disinhibited behaviors occurring at a prevalence of 0 to 63% 16,45,46 and emotionally labile behavior occurring at a prevalence of 22%. 45 One study reported a prevalence of disinhibition of 63% during PTA and 0% following PTA emergence. 16
Prevalence of Agitated Behavior Scale Items
-not measured.
Meta-analyses
Selection of studies and outcomes for inclusion in meta-analysis
For inclusion in meta-analysis studies were required to report the prevalence of agitation within an appropriate sample frame, identify agitation using valid methods and employ a sample size of at least 10 hospitalized TBI participants. A total of 13 studies with these characteristics met criteria for inclusion in meta-analyses.
Three studies 18,44,50 reported multiple outcomes meeting criteria for inclusion in meta-analyses. The most robust estimate was selected for inclusion by prioritizing outcomes that employed validated clinical cut-offs, measured agitation longitudinally, and defined significant agitation in the same way as other included studies. Two studies 9,45 did not provide numerators for prevalence estimates; therefore, these values were calculated using the provided denominator and percentage figures.
Overall prevalence of agitation
Pooled prevalence was determined for the overall prevalence of agitation. Thirteen studies met criteria for inclusion in meta-analysis of the overall prevalence of agitation. 7 -9,18,31,43 -45,47 –51 The overall pooled prevalence of agitation during inpatient care following TBI was 31.73% (95% CI, 25.25%-39.00%; z = -4.71; p < 0.001; z-test for proportion = 0.5; Fig. 3). Heterogeneity statistics (χ 2 = 52.16, p < 0.001, I2 = 76.68%, τ 2 = 0.28) indicated considerable variability in the prevalence of agitation across studies. The funnel plot seemed to suggest that study specific proportions were distributed symmetrically (Supplementary Appendix VII) and the Egger test was non-significant (p = 0.084), suggesting the absence of small sample bias.

Forest plot of overall pooled prevalence of agitation in 13 studies.
Prevalence of agitation by PTA status
When considered alone, the pooled prevalence of agitation within the two studies meeting criteria that were conducted during PTA 7,18 was 44.06% (95% CI, 36.15%-52.28%; z = -1.42; p = 0.16; z-test for proportion = 0.5; Fig. 4). Although planned, the prevalence of agitation outside of PTA was not calculable as only one study met criteria for inclusion in this analysis. Formal comparison of the difference in pooled prevalence of agitation between patients in and out of PTA was therefore also not possible.
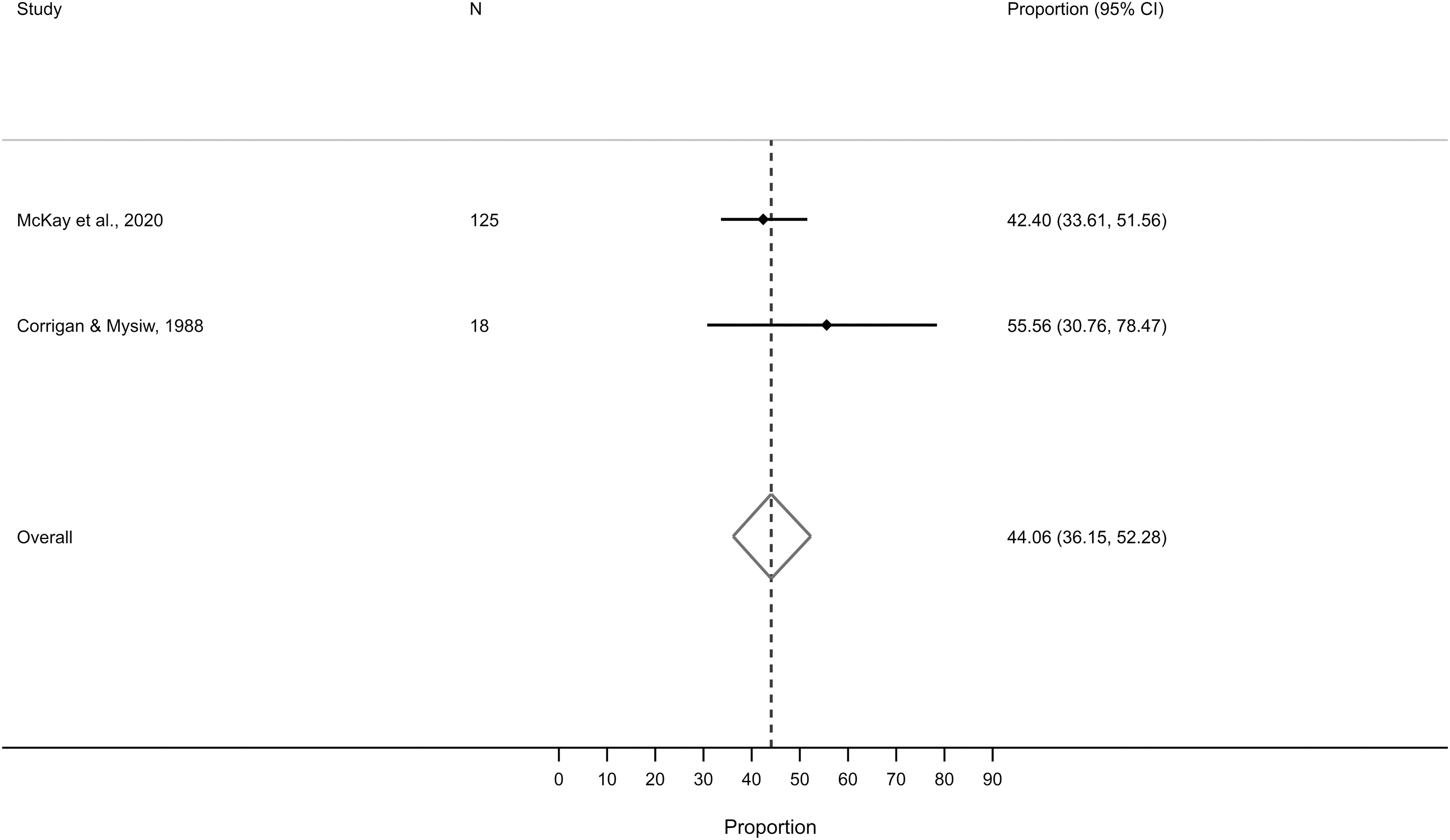
Forest plot of pooled prevalence of agitation during post-traumatic amnesia in two studies.
Prevalence of agitation by setting
The estimated prevalence of agitation during rehabilitative care in 11 studies meeting criteria for inclusion in meta-analysis 7 -9,18,31,43 -45,47,48,51 was 32.23% (95% CI, 27.13%-37.80%; z = -5.95; p < 0.001; z-test for proportion = 0.5; Fig. 5). Heterogeneity statistics (χ 2 = 41.13, p < 0.001, I2 = 62.85%, τ 2 = 0.12) indicated that there was substantial variability in the prevalence of agitation across studies conducted in a rehabilitation setting. Although planned, the prevalence of agitation during acute care was not calculable as only one study met criteria for inclusion in this analysis. Statistical comparison of the difference in pooled prevalence of agitation between patients in an acute and rehabilitation setting was therefore unable to be carried out.
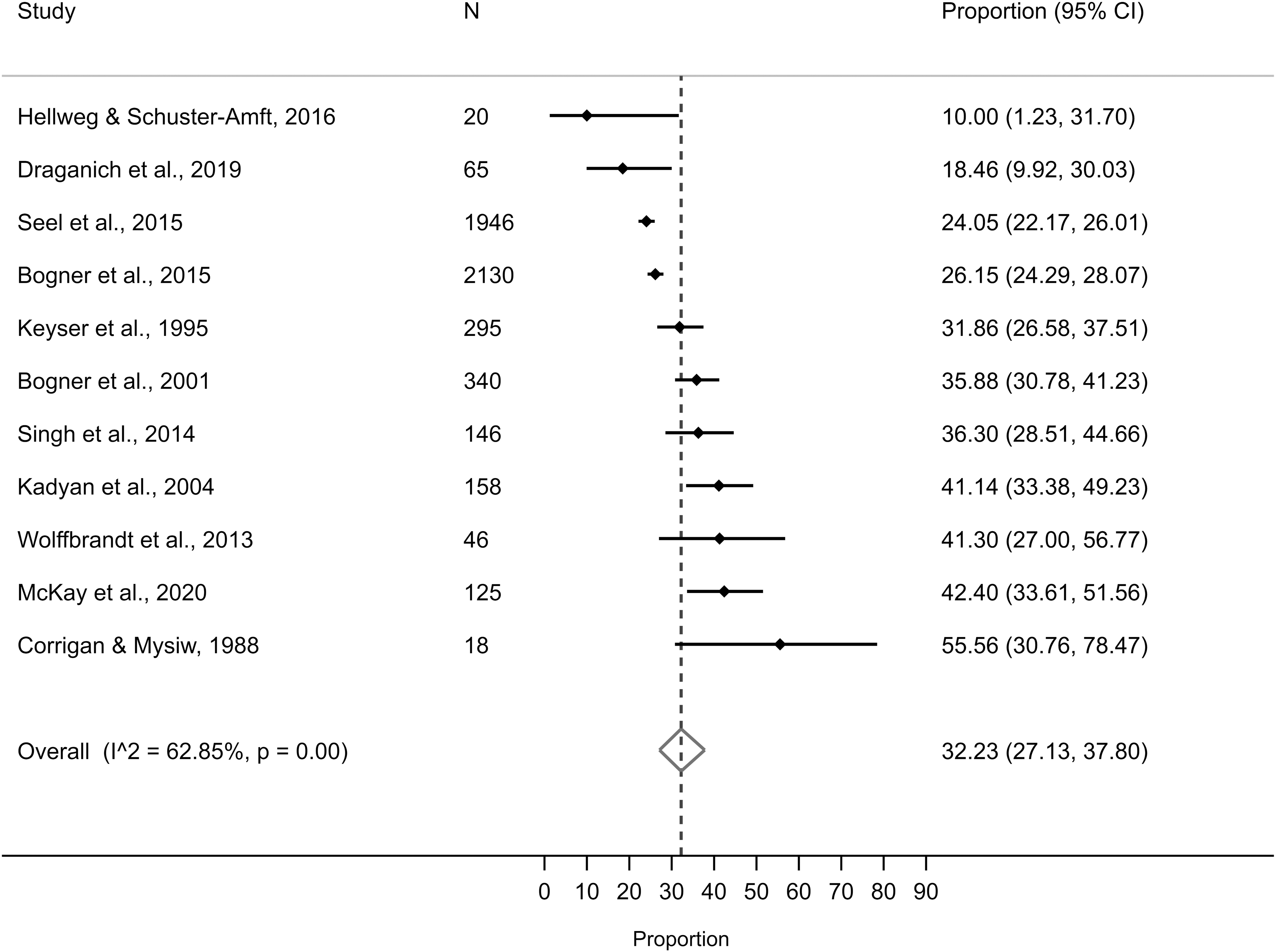
Forest plot of pooled prevalence of agitation during rehabilitative care in 11 studies.
Sensitivity analyses
We used sensitivity analyses to assess the impact of arbitrary or unclear decisions on the results of meta-analysis of prevalence of overall agitation. As previously described, the pooled prevalence of overall agitation over 13 studies was 31.73% (95% CI, 25.25%-39.00%). Estimates were removed from or added to this analysis for the purpose of sensitivity analysis.
We examined the impact of excluding studies that did not explicitly provide information pertaining to sample characteristics (e.g., age range, TBI severity breakdown) but were included in this review based on the availability of information suggesting that these criteria were met. Nine studies 7,8,18,43,45,47 -49,51 were included in this analysis following removal of four studies, 9,31,44,50 resulting in a similar pooled prevalence of 33.65% (95% CI, 25.72%-42.62%).
To assess the impact of our decision to exclude studies with a higher risk of bias from meta-analysis we re-ran meta-analysis including these two studies. 16,46 The overall prevalence of agitation across the 15 studies was 29.82% (95% CI, 23.58%-36.92%), only negligibly decreasing the pooled prevalence estimate.
Finally, we examined the impact of choice of outcome for inclusion in meta-analysis where studies reported multiple prevalence figures employing different definitions of agitation. Two studies were identified as meeting this criterion 44,50 and two alternate estimates were chosen and substituted for those included in the initial analysis of overall prevalence. Where multiple options were available, the second most representative estimate was chosen for inclusion based on the same principles as choice of estimate for inclusion in the meta-analysis of overall agitation. Analysis indicated a prevalence of 34.08% (95% CI, 27.97%-40.76%), again similar to the initial analysis. Detailed results for each of these sensitivity analyses are available in Supplementary Appendix VIII.
Methodological quality
All included studies
Quality assessment revealed limitations in the included studies (Supplementary Appendix IX). Several studies adopted problematic eligibility criteria that may have swayed the prevalence estimate, including inclusion of mild TBI patients if these patients displayed severe agitation, 8,51 exclusion of patients with the most severe injuries, 16,49 -51 exclusion of patients with disorders of consciousness, 43,47 and exclusion of older patients. 16,50 This is despite evidence to suggest a relationship between greater injury severity and agitation, 6,56 the possibility of developing agitation in a minimally conscious or vegetative state, 57 and research indicating an association between younger age and presence of agitation. 7 Only three studies excluded patients presenting with conditions that might independently cause agitation 16,46,49 and only one study excluded patients in whom agitation could not be accurately monitored. 49 Study sampling frames were generally considered appropriate to establish the prevalence of agitation following TBI; however, one study excluded severe TBI patients, 16 exposing this study to bias.
Several threats to coverage of the sample were observed, including the need for consent, 7,9,31,47,49 -51 exclusion of patients who were not recruited within 48-h of admission, 49 and use of a once-weekly sampling procedure. 50 Response rate and coverage bias were often unclear. Two studies employed unvalidated author-designed measures to assess agitation, threatening the validity of findings. 16,46 One study only monitored patients who demonstrated the potential for agitation as ordered by their physician, 9 thereby failing to measure agitation in a standard fashion across patients. Inadequate sample size constituted a considerable threat to the accuracy of prevalence estimates, with only three studies meeting or exceeding the minimum sample size criterion of 340 participants 9,31,47 as calculated in accordance with the formula provided by Daniel (1999). 58 No study that explicitly aimed to establish the prevalence of agitation following TBI conducted a formal sample size calculation. Three studies did not provide the precise number of patients considered agitated 9,16,45 and only one study provided confidence intervals to accompany their reported prevalence estimate. 49
Studies included in meta-analyses
Thirteen studies were considered at a lower risk of bias and included in meta-analyses. 7 -9,18,31,43 -45,47 –51 Selective monitoring of only those patients demonstrating the potential for agitated behavior may have increased the reported prevalence of one study included in meta-analyses of overall prevalence of agitation and prevalence of agitation in a rehabilitation setting, 9 and exposed these calculations to bias. Two studies included in meta-analyses of the overall prevalence of agitation and prevalence in a rehabilitation setting did not report the precise number of patients considered agitated. 9,45 Sample size was considered inadequate in 10 of the 13 studies included in meta-analysis of prevalence of overall agitation, 7,8,18,43 -45,48 –51 both studies included in meta-analysis of agitation during PTA, 7,18 and eight of 11 studies included in meta-analysis of agitation within a rehabilitation setting, 7, 8,18,43 -45,48,51 introducing error to the reported estimates and analyses.
Studies reporting general prevalence not included in meta-analysis
Studies not included in meta-analyses were of poorer methodological quality than included studies. The main areas of bias identified in these studies included exclusion of severe TBI patients (possibly reducing the reported prevalence estimate), 16 use of unvalidated measures of agitation, 16,46 failure to report the precise number of patients considered agitated, 16 and inadequate sample size. 16,46
Studies examining prevalence of sub-behaviors of agitation
Of those studies reporting the prevalence of sub-behaviors of agitation, two studies used unvalidated author-designed measures of agitation, 16,46 one study excluded patients with severe TBI leading to an inappropriate sample frame, 16 two studies did not report the precise number of patients demonstrating agitated behaviors, 16,45 and no study's sample size was sufficient, exposing results to risk of bias.
Discussion
Agitation constitutes a significant barrier to rehabilitation following TBI and poses risks to the patient, staff and family members. The aim of this systematic review and meta-analysis was to establish the proportion of patients who develop agitation following TBI, what stage of recovery and setting they are at greatest risk of developing agitation and which behaviors they are most likely to exhibit. Sixteen studies met review inclusion criteria and 13 studies judged to have low risk of bias were synthesized in meta-analyses.
Overall prevalence of agitation
The reported overall prevalence of agitation following TBI ranged from 0 to 57%, with variability in reported figures due to methodological heterogeneity. Meta-analysis indicated a pooled prevalence of 31.73% in 13 studies with a lower risk of bias. The findings of this analysis suggest that agitation affects a significant proportion of TBI patients in the early stages of recovery following injury and represents a common challenge encountered by healthcare providers and family members.
Prevalence of agitation in PTA
In patients in PTA, the prevalence of agitation ranged from 25 to 56% and pooled prevalence was estimated to be 44.06%. Only two studies reported on the prevalence of agitation following PTA emergence, providing estimates of 0% and 22%. Two of the three highest prevalence estimates of agitation were reported in pure PTA samples within a rehabilitation setting (42% and 56%), 7,18 while the highest prevalence of 57% was reported in an intensive care unit setting where a large proportion of patients were likely in a state of PTA. 49 This analysis points to a relationship between PTA and agitation and lends support to previous research indicating a higher prevalence of agitation during the PTA period. 6,7,17,18,21 Agitation is therefore of particular clinical significance during this early phase of recovery following TBI and additional resources to facilitate agitation management during PTA are warranted in clinical practice.
Prevalence of agitation in rehabilitation
In studies conducted within a rehabilitation setting, the prevalence of agitation ranged from 0 to 42% and pooled prevalence was estimated to be 32.23%. This pooled estimate contrasts starkly with the one study with a lower risk of bias conducted within an acute setting, reporting the highest prevalence of included studies at 57%. 49
This analysis suggests that although agitation impacts a significant proportion of patients at any stage of recovery following TBI, it may be most likely to occur during acute hospitalization. These findings lend tentative support to previous research suggesting a higher prevalence of agitation within an acute hospital environment. 6 Several factors may underpin this relationship. Patients are earlier in their recovery during acute hospitalization and more likely to remain deep in PTA. They also may be more susceptible to other factors associated with the development of agitation, such as presence of pain and infection. 7,28,31 The rehabilitation unit's focus lies with engagement in multi-disciplinary therapy and therefore necessitates manageable levels of agitation to facilitate patient cooperation. Conversely, initial stabilization of the injury is of greatest focus in the acute environment. As such, while some rehabilitation settings are designed to limit stimulation to avoid overwhelming the patient and triggering agitation, acute environments are by necessity designed with a focus on preservation of life and feature bright lighting, noisy alarms, and frequent rounding. Although agitation management may become a greater focus of care during inpatient rehabilitation due to the impact of behavioral dysregulation upon engagement in therapy, environmental and patient characteristics during acute hospitalization place patients at risk of developing agitation.
Greater implementation of recommended non-pharmacological agitation management strategies 13,26 -28 may lead to a reduction in agitation prevalence, especially within the acute environment. A recent international survey found that most clinicians employed non-pharmacological interventions to manage agitation in the early phase of recovery following TBI. 12 However, only 52% of respondents reported feeling satisfied with agitation management practices in their facility, suggesting that there is room for improvement in the application of non-pharmacological agitation management strategies. This may be especially true in acute settings, where we found the highest prevalence of agitation, and in which one study found that only 20-30% of patients received non-pharmacological intervention for agitation. 22 Allocation of organizational resources, formalized training aimed at broadening the array of non-pharmacological strategies available to clinicians, and implementation of appropriate strategies across patients may lead to a reduction in agitation prevalence and severity and limit the use of potentially harmful pharmacological interventions with undesirable sedating effects. 12,13
Prevalence of sub-behaviors of agitation
In studies reporting the prevalence of sub-behaviors of agitation, disinhibited behaviors tended to be the most prevalent, followed by emotionally labile and aggressive behaviors. The highest estimates of prevalence of agitated sub-behaviors were reported in the one study conducted in a pure PTA sample. 7 The one study conducted in an acute setting 49 consistently reported the lowest proportions of patients presenting with agitated behavior according to individual ABS items, with the exception of “pulling on tubes and catheters,” the use of which might be expected to be higher in the intensive care unit.
Medical professionals tend to emphasize physical aggression and explosive anger as the most typical agitated behaviors following TBI. 12,19 The wide variety of behaviors endorsed in studies examining the presence of agitated sub-behaviors highlights the complex presentation of agitation and illustrates the importance of considering a broad range of behaviors when evaluating agitation, the utility of detailed tools such as the ABS in describing each patient's unique presentation, and the need for a broad range of interventions in the management of agitated behavior. Concurrently, the relative prevalence of disinhibited behaviors indicates that emphasis should be placed on behaviors such as distractibility, impulsivity, and repetitive behaviors when identifying the presence of agitation in the early stages of recovery following TBI. Successful identification and subsequent management of the wide spectrum of behaviors constituting agitation has direct implications for patient prognosis, given the link between agitation and poorer patient outcomes. 2,11
Variability in reported prevalence estimates
Together, differences in sample characteristics and setting, biases identified in formal risk of bias assessment, and variability in study methodology likely explain heterogeneity between studies.
Between-study variability in sample characteristics and setting likely contributed to differences in reported prevalence estimates. Sample characteristics related to the development of agitation including TBI severity, 6,16,3 age, 7 time post-injury, 7 PTA status, 7,31 pain, 28 infection, 7,31 and presence of frontotemporal lesions 16 varied between study samples and likely contributed to variability between prevalence estimates. The use of pharmacological and non-pharmacological interventions to manage agitation varies between settings, 12 impacting upon the development of agitation and ultimately producing variability in estimates of agitation prevalence. Studies were published over a 41-year time frame, over which time the management of agitation has undoubtedly advanced and the proportion of patients consequently exhibiting agitation would be expected to vary.
Formal risk of bias assessment identified factors likely to contribute to heterogeneity in reported prevalence estimates. Most included studies did not meet sample size requirements, leading to imprecise prevalence estimates. Several studies also featured problematic eligibility criteria (e.g., exclusion of patients with the most severe injuries). Few studies excluded patients with pre-morbid conditions that might independently cause agitation such as neurological disorders, psychiatric conditions, and a history of alcohol/substance abuse or in whom agitation could not be accurately monitored—likely falsely increasing or decreasing the prevalence estimate, respectively. Threats to sample coverage (e.g., the need for consent) also were observed. The use of unvalidated measures with narrow definitions of agitation may have resulted in the underestimation of agitation prevalence and studies that employed such measures tended to report a lower prevalence of agitation. One study did not measure agitation in a standard way between participants.
Differences in study methodology not captured by formal risk of bias assessment likely also contributed to heterogeneity in estimated prevalence. Presence of agitation was assessed using a wide array of measures, each of which employed different definitions of agitation. Agitation was rated by a wide range of medical professionals who likely interact differently with the patient over varying durations of time. Thresholds defining significant agitation (i.e., one or more scores above a set threshold within a certain period of time) also varied between studies, and studies requiring a single endorsement of agitation tended to report greater prevalence than those requiring multiple instances of significant agitation. Studies measuring agitation at a single time-point also tended to report lower prevalence than those reporting the prevalence of agitation as measured longitudinally, likely due to missing agitation demonstrated earlier or later in recovery. Of those studies that measured agitation longitudinally, the frequency of measurement varied between daily, multiple times daily and weekly. As agitation is known to fluctuate over the course of the day, 17,32 from one day to the next, 17,32,59 and throughout the patient's period of recovery, 7,17,18,21 differences in when agitation was measured likely led to variability in reported estimates. Finally, start and stop rules for agitation measurement varied between studies, likely also contributing to differences in reported prevalence.
Strengths and limitations
This review focused solely on the prevalence of agitation in adults age 16 years or older undergoing inpatient hospitalization and therefore cannot speak to the prevalence of agitation in children or adolescents, or longer-term behavioral change persisting beyond hospital discharge. We searched for studies published in English only. Although we did identify studies published in other languages, several studies were unable to be translated within the review time frame. One potentially eligible record could not be obtained.
Several studies failed to report important information, making comparison of study results and assessment of study quality difficult. We categorized studies as including patients in or out of PTA and conducted in an acute or rehabilitative setting. However, PTA status and setting cannot be separated entirely, as regardless of setting type each sample likely contained some proportion of patients who were in PTA. As the number of patients in PTA was infrequently reported, it is difficult to establish the impact that this may have had on reported prevalence estimates. In distinguishing acute and rehabilitative hospitalization, we have assumed a model of care in which patients receive initial stabilization of their injury in an acute setting, followed by intensive rehabilitation in a specialized care facility with behavioral management provisions until ready for discharge into the community. Although this model reflects practice in many of the studies included in this review, it may not represent the model of care found in many non-specialized settings and in situations where access to rehabilitation is unavailable.
This review is limited by the inability to run planned analyses of prevalence following PTA emergence and in an acute setting owing to a lack of high-quality primary studies. Caution must be exercised in interpreting findings in studies conducted during PTA due to the small number of studies included. Our estimate of agitation prevalence during rehabilitation hospitalization includes only two fewer studies than the overall pooled prevalence statistic and is therefore similar to the overall pooled prevalence of agitation following TBI. Substantial differences between studies resulted in significant heterogeneity, suggesting that results of meta-analyses should be interpreted with caution.
Despite these limitations, to the authors' knowledge, this review represents the only systematic review and meta-analysis of the prevalence of agitation following TBI. We examined the nature of agitation during inpatient hospitalization in detail, including the impact of PTA status and hospital setting and the behaviors most likely to be exhibited. The majority of identified studies were included in meta-analyses. Subjective reviewer decisions (whether to retain studies in which key characteristics were unclear, choice between multiple reported prevalence estimates for inclusion in meta-analyses) were supported by sensitivity analyses. Our search strategy included a comprehensive search of unpublished studies and we ultimately included a wide range of studies featuring a broad array of aims, reducing the risk of publication bias. We also employed a rigorous analysis of methodological quality.
Directions for future research
Only six studies included in this review explicitly aimed to identify the prevalence of agitation. 8,16,44,45,48,50 Future research should focus upon the areas in which the current literature is most lacking. Only two studies reported the prevalence of agitation in an acute setting, three in a pure PTA sample, and two in a sample of patients who had emerged from PTA. Further high-quality research is needed to estimate the proportion of patients who exhibit agitation in these circumstances. No study included in this review reported the prevalence of agitation within hospital units not specializing in the care of patients who have sustained a TBI. The prevalence of agitation within this setting also warrants investigation.
Future studies should measure agitation in large samples frequently and longitudinally from the time of injury until re-integration into the community. Agitation should be measured using validated scales that capture the full breadth of agitated behavior (e.g., the ABS). Important variables such as PTA, setting, and environmental characteristics should be captured to facilitate understanding of the contexts in which agitation is most prevalent. Further research in this area will allow patients, clinicians and family members to be better informed as to the likelihood of the patient developing agitation. A better understanding of the prevalence and nature of agitation will additionally allow for efficient assessment and resource allocation within the inpatient setting, ultimately improving patient outcomes.
Conclusions and recommendations for clinical practice
The findings of this systematic review and meta-analysis suggest that agitation affects approximately one-third of individuals following TBI, contributing to healthcare resource utilization and exposing patients, healthcare workers, and family members to risk of harm. Agitation is most likely to affect patients in an acute setting and during the PTA period, highlighting priorities for resource allocation. Greater organizational resourcing, formal staff training, and implementation of non-pharmacological agitation management techniques in line with expert guidelines 13,26 -28 may reduce the prevalence of agitation in the early stages of recovery following TBI. This is especially pertinent to acute care environments where agitation appears to be the most prevalent and non-pharmacological management strategies may be less utilized. Due to a lack of high-quality evidence, further research is required to support the use of pharmacological agents in the management of agitation following TBI. 23,24 Agitation is most likely to present as disinhibited behavior such as wandering, restlessness, and impulsivity, rather than emotional lability or aggression. While it is important to consider a broad range of behaviors when evaluating agitation, clinicians should remain particularly cognizant of these disinhibited behaviors. A formal, objective measure of agitation capturing a broad spectrum of behaviors (e.g., the ABS) should be utilized when assessing the presence of agitation.
Footnotes
Acknowledgments
We would like to acknowledge Dr. Farhad Shokraneh, information specialist, for input in the design of search strategies and Dr. Stella May Gwini, statistician, for her advice regarding statistical analysis. The authors would also like to acknowledge and thank those individuals who contributed to the translation of research studies that were published in languages other than English, including Aigerim Azamatova, MSc, Bart Pijls, MD, PhD, Corneliu Antonescu, MD, Gianna Kohl, BSc, MSc, Samriti Sharma, MEc, Joanne Ryan, BSc (Hons), MBiostat, PhD, Ka King Chan, BSc, MNSc, Marco Da Roit, MSc, Michał Kunicki, MD, PhD, Reto Bloch, and Signe Jakobsen, MSc. Finally, we would like to acknowledge the authors whose publications have been included in this systematic review and meta-analysis.
PROSPERO Registration: CRD42020201604.
Authors' Contributions
Authors R.K.P. and S.L.C. performed study screening for inclusion, data extraction, assessment of risk of bias, and selection of studies for inclusion in meta-analyses. Any disagreements were settled by J.L.P., A.J.H., and A.M. All authors contributed to the review protocol, methodological decisions and manuscript.
Funding Information
This is no funding to declare.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Appendix I
Supplementary Appendix II
Supplementary Appendix III
Supplementary Appendix IV
Supplementary Appendix V
Supplementary Appendix VI
Supplementary Appendix VII
Supplementary Appendix VIII
Supplementary Appendix IX
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.