
Abstract
Neurological examination in the acute phase after spinal cord injury (SCI) is often impossible and severely confounded by pharmacological sedation or concomitant injuries. Therefore, diagnostic biomarkers that objectively characterize severity or the presence of SCI are urgently needed to facilitate clinical decision-making. This study aimed to determine if serum markers of neural origin are related to: 1) presence and severity of SCI, and 2) magnetic resonance imaging (MRI) parameters in the very acute post-injury phase. We performed a secondary analysis of serological parameters, as well as MRI findings in patients with acute SCI (n = 38). Blood samples were collected between Days 1-4 post-injury. Serum protein levels of glial fibrillary acidic protein (GFAP), neuron-specific enolase (NSE), and neurofilament light protein (NfL) were determined. A group of 41 age- and sex-matched healthy individuals served as control group. In the group of individuals with SCI, pre-operative sagittal and axial T2-weighted and sagittal T1-weighted MRI scans were available for 21 patients. Serum markers of neural origin are different among individuals who sustained traumatic SCI depending on injury severity, and the extent of the lesion according to MRI in the acute injury phase. Unbiased Recursive Partitioning regression with Conditional Inference Trees (URP-CTREE) produced preliminary cut-off values for NfL (75.217 pg/mL) and GFAP (73.121 pg/mL), allowing a differentiation between individuals with SCI and healthy controls within the first 4 days after SCI. Serum proteins NfL and GFAP qualify as diagnostic biomarkers for the presence and severity of SCI in the acute post-injury phase, where the reliability of clinical exams is limited.
Introduction
Efforts to validate the effect of therapies and interventions after acute traumatic spinal cord injury (SCI) rely on clinical assessments, which are imprecise and often impossible to assess in severely injured individuals. 1 –4 The American Spinal Injury Association (ASIA) International Standards for Neurological Classification of SCI (ISNCSCI) score is used to assess motor and sensory function in patients with SCI. Neurological examination in the acute phase is often confounded by pharmacological sedation, or concomitant injuries—especially traumatic brain injury (TBI). 5 However, interventions including sedation, or intubation are mostly inevitable and are hence complicating a reliable neurologic examination in the very first days after injury and sometimes beyond.
Therefore, diagnostic biomarkers that objectively characterize injury severity or the mere presence of SCI are urgently needed. Diagnostic markers would be of utmost interest, not only for research purposes, but also to assess the severity of SCI, and monitor the process of neurological recovery within the subacute phase in a clinical setting.
Previous studies have shown that markers of neural origin facilitate outcome prediction after TBI. 5,6 Also, several studies reported about promising diagnostic capacity of serum concentrations of neural markers in patients with spinal cord ischemia as a complication of thoraco-abdominal aortic aneurysm repair. 7 –10 Further, it has been previously reported that cerebrospinal fluid (CSF) microRNA, metabolites, and concentrations of several proteins and cytokines are related to the severity of neurological impairment after SCI and inform a prediction whether an individual will experience an improvement in the ASIA impairment scale (AIS). 1,3,11 –15 However, sample collection of CSF is invasive and often accompanied by complications. 16,17 Biomarkers derived from blood would constitute a less invasive alternative. 3 Yet, the diagnostic value of blood-borne biomarkers in the very acute phase after traumatic SCI is not entirely understood. 2,18 -20
Accordingly, the aims of this study were to evaluate: 1) if serum concentration of glial fibrillary acidic protein (GFAP), neuron-specific enolase (NSE), and neurofilament light protein (NfL) are able to differentiate between patients with SCI in the acute post-injury phase (1-4 days post-SCI) and healthy controls, and if those parameters are related to 2) injury severity, and 3) magnetic resonance imaging (MRI) parameters.
Methods
Patients and healthy control subjects
Eighty-one individuals with acute traumatic SCI were recruited at Trauma Center Murnau (Bavaria, Germany) as part of the prospective Autoantibodies in Spinal Cord Injury Study (
Blood samples
Peripheral blood was collected by venipuncture. In the SCI group, sample collection was performed between Days 1 and 4 post-SCI. The serum tubes were stored at room temperature for 45 min followed by 1 h at 4°C, allowing the blood to clot. After that, blood was centrifuged at 4°C at 1500 g for 20 min, and serum was aliquoted and stored at -80°C until shipped to the laboratory of the Institute of Molecular Regenerative Medicine at the Paracelsus Medical University (Salzburg, Austria) on dry ice for analysis.
Analytical procedures
GFAP, NSE, and NfL were measured by R-Plex singleplex assays (Meso Scale Discovery, Rockville, MD). Measurements were carried out following manufacturer's instructions, including dilution of samples and standards (instructions are available on the manufacturer's website). The same serum aliquot was used for all three biomarkers without any freezing and thawing cycles in between. For a detailed description please refer to the Supplementary Material.
Neurological assessment
Motor and sensory function of individuals who sustained SCI was evaluated according to ISNCSCI. 22 Complete ISNCSCI scores and its sub-scores (upper extremity motor score [UEMS], lower extremity motor score [LEMS], pin prick [PP] sensory score, and light touch [LT] sensory score) were available from all 38 patients 30 days post-injury. The Spinal Cord Independence Measure (SCIM) 23 was assessed within the first post-injury days and at discharge from the hospital.
Radiological assessment
In 22 of 38 patients, pre-operative MRI was available. Sagittal and axial T2-weighted and sagittal T1-weighted MRI scans were performed using a 1.5-Tesla MRI unit (Achieva, Philips Medical Systems, Eindhoven, Netherlands; Multi Coil NV16). MRIs were analyzed by one neuro-radiologist who had no access to study relevant data.
To quantify the extent of the lesion, the following parameters were assessed: maximal extent of intramedullary lesion width on axial images, longitudinal length of intramedullary lesion (IML), maximum spinal cord compression (MSCC), maximum canal compromise (MCC), Brain and Spinal Injury Center (BASIC) score, and Sagittal Grade. 24 –28
In one patient, the lesion could not be classified according to the above-mentioned scores due to an extensive spinal epidural hematoma. Hence, MRI data of 21 individuals were included in the analysis.
Statistical analysis
All statistical analyses and figures were compiled in R (R Core Team, 2018, version 4.0.4 running under: Windows 10 x64). Descriptive statistics for continuous variables and frequency counts for categorical variables were calculated. Pearson's chi-squared tests were applied to test the association between categorical variables. Independent t-tests were used to determine differences in continuous variables.
Conditional inference trees
Our primary statistical analysis employed Unbiased Recursive Partitioning regression with Conditional Inference Trees (URP-CTREE) using the R package “party.” 29,30 Biomarkers of similar cellular origin and/or temporal trajectories have strong inter-correlations and do not necessarily add significant information in the prediction models when combined. 6 Therefore, we employed URP-CTREE because it uses p values for variable selection and as a stopping criterion. 29 –32
MRI versus biomarkers
To assess the relation between neurological function and blood-borne markers with MRI findings, correlation analyses were performed, including MRI markers from 21 patients who underwent pre-operative MRI. For this, the AIS ISNCSCI and its sub-scores, SCIM at discharge, and the serum markers (NfL, GFAP, and NSE) were correlated with IML, MSCC, MCC (Pearson's r), BASIC score, and Sagittal Grade (Spearman's ρ). Pearson's r was compiled for continuous variables using the R package “corrplot.” 33 Spearman's ρ was calculated for the ordinal MRI scores using the R package “lares” (v4.8.4; Lares Bernardo, 2020).
Results
A total of 79 individuals were included in this study (Table 1).
Summary of Subject Characteristics
Independent t-test between SCI and Control; bPearson's chi-squared test.
SCI, spinal cord injury; SD, standard deviation.
Table 2 depicts the distribution of injury severity among different neurological levels of injury showing that individuals with thoracic lesions have more clinically complete injuries compared with patients with cervical lesions.
Summary of Subject Characteristics in Individuals with SCI
Pearson's chi-squared test; *significance.
SCI, spinal impairment scale; NLI, neurological level of injury; AIS, American Spinal Injury Association Impairment Scale.
Diagnostic biomarkers: SCI versus control
With the aim to evaluate if the serum concentrations of NfL, GFAP, and NSE can differentiate between individuals who sustained SCI and healthy controls, we employed URP-CTREE including all three neural markers from the sample collection between post-injury Days 1-4. The URP-CTREE based on a sample of 79 individuals produced three terminal nodes (3, 4, 5), for which the end-point distribution (SCI vs. healthy controls) is shown in the diagrams in Figure 1A. Two parameters differentiated between individuals with SCI and healthy controls: serum levels of 1) NfL and 2) GFAP. The first node represents the cut-off value for the serum concentration of NfL at 75.217 pg/mL (p = 0.005). In node 2, the subgroup with NfL levels below 75.217 pg/mL is further separated by the serum concentration of GFAP at 73.121 pg/mL (p = 0.003), resulting in three terminal nodes. All individuals with an NfL serum concentration above 75.217 pg/mL sustained SCI (node 5), while almost all individuals with NfL levels below 75.217 pg/mL and GFAP levels below 73.121 pg/mL were healthy controls (node 3).

Unbiased Recursive Partitioning regression with Conditional Inference Trees (URP-CTREE) first node: neurofilament light protein (NfL) concentration in pg/mL; second node: glial fibrillary acidic protein (GFAP) concentration in pg/mL; three terminal nodes (3, 4, 5) for the end-point distribution spinal cord injury (SCI) vs. healthy controls

Serum concentrations of neurofilament light protein (NfL) in the very acute phase (1-4 days post-injury) in pg/mL; Control vs. SCI. Color image is available online.
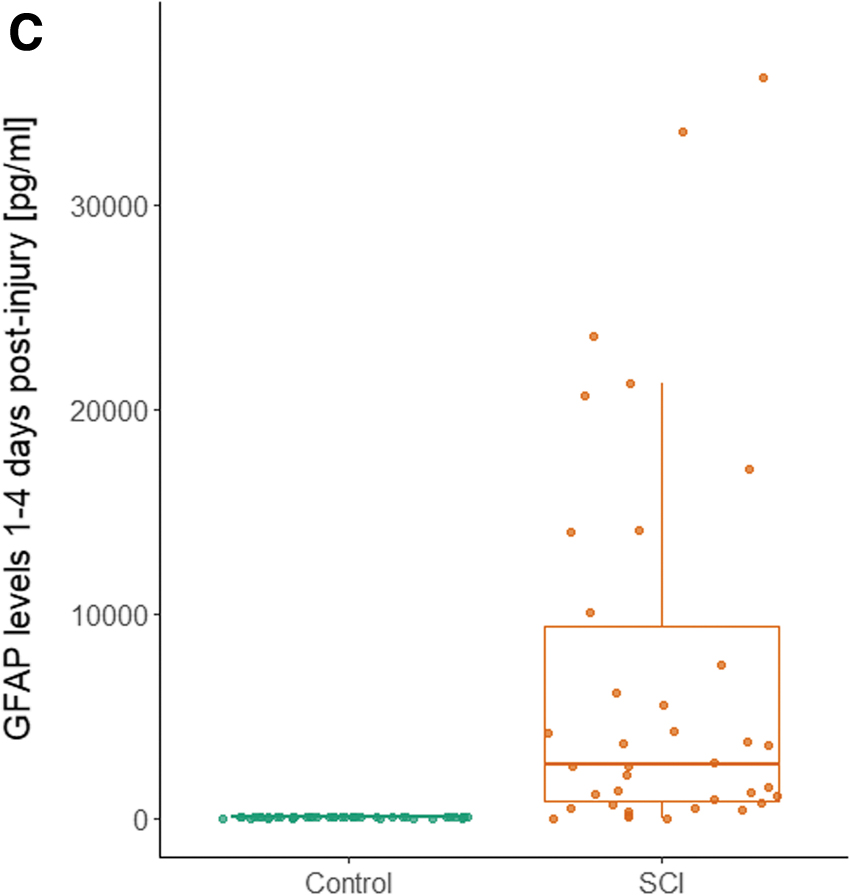
Serum concentrations of glial fibrillary acidic protein (GFAP) in the very acute phase (1-4 days post-injury) in pg/mL; Control vs. SCI. Color image is available online.
With NfL levels below 75.217 pg/mL and GFAP levels above 73.121 pg/mL chances to be in the SCI group were approximately 70% (node 4). Node 4 represents the smallest node (n = 7) in URP-CTREE and an area of greater uncertainty. Two individuals from the control group had GFAP levels slightly above the proposed cutoff (73.43 and 74.67 pg/mL). This might be due to an unknown central nervous system (CNS) disease or spinal canal stenosis. Also, five less severely injured SCI patients had NfL levels below 75.217 pg/mL. Serum concentrations of NSE were not significantly associated with the presence of SCI in this study cohort, although NSE might have been affected by hemolysis, since this enzyme is also present in erythrocytes. 34,35
Both parameters from URP-CTREE (Fig. 1A) were significantly different between the group of individuals with SCI in the acute post-injury phase and the healthy control group. The mean difference in serum concentration of NfL was 299.04 pg/mL (p = 0.003) between the SCI group and the control group (332.68 (577.3) and 33.64 (14) mean (standard deviation [SD]) pg/mL, respectively; Fig. 1B). The mean difference of GFAP levels was 9188.72 pg/mL (p = 0.003) between SCI and controls [9225.02 (17924.19) and 36.3 (18.96) mean (SD) pg/mL, respectively; Fig. 1C; Table 3].
Serum Concentrations in pg/mL of Neural Markers: SCI vs. Control
All values in mean (SD, range).
Independent t-test between SCI and Control; *significance.
SCI, spinal cord injury; NfL, neurofilament light protein; GFAP, glial fibrillary acidic protein; NSE, neuron-specific enolase.
Biomarker concentrations and injury severity
To evaluate if the included serum markers are related to injury severity by means of ISNCSCI scores and AIS, correlation analyses were conducted. Figure 2 depicts significant Pearson's correlation coefficients between levels of NfL and GFAP in the very acute phase and all ISNCSCI sub-scores (correlations coefficients ranging between 0.33 and 0.43, p < 0.05). NSE did not show any significant correlation with ISNCSCI sub-scores.

Correlation matrix: significant Pearson's correlation coefficients; significance level p < 0.05. UEMS_day30, upper extremity motor score 30 days post-injury; LEMS_day30, lower extremity motor score 30 days post-injury; LT_day30, light touch sensory score 30 days post-injury; PP_day30, pin prick sensory score 30 days post-injury; SCIM_at_discharge, Spinal Cord Independence Measure at hospital discharge; very_acute_NSE, Neuron-Specific Enolase at day 1-4 post-injury; very_acute_NfL, Neurofilament light protein at day 1-4 post-injury; very_acute_GFAP, Glial Fibrillary Acidic Protein at day 1-4 post-injury. Color image is available online.
As mentioned above, biomarkers of similar cellular origin may have strong inter-correlations, 6 which is also seen in our data with significant correlations between the levels of GFAP and NfL (Fig. 2). Additionally, AIS grade correlated significantly with NfL (Spearman's ρ r = -0.47, p = 0.0028) and GFAP (r = -0.47, p = 0.003).
Therefore, both markers that produced nodes in the URP-CTREE are also significantly related to injury severity by means of motor and sensory scores. Patients with lower ISNCSCI scores had higher serum concentrations of NfL and GFAP 1-4 days after SCI.
MRI markers versus neurological function and neural markers
To evaluate if the morphological extent of SCI is associated with neurological function and serum levels of the included neural markers, we performed correlation analysis including MRI markers from 21 patients who underwent pre-operative MRI. The mean (SD) time from injury to MRI was 4.91 (4.31) h (ranging from 1.72 to 17.33 h). A correlation matrix including Pearson's correlations coefficients for continuous variables (ISNCSCI motor and sensory scores, SCIM at discharge, levels of NfL, GFAP, and NSE, the axial lesion width on MRI, IML, MSCC, MCC) is depicted in Figure 3A.
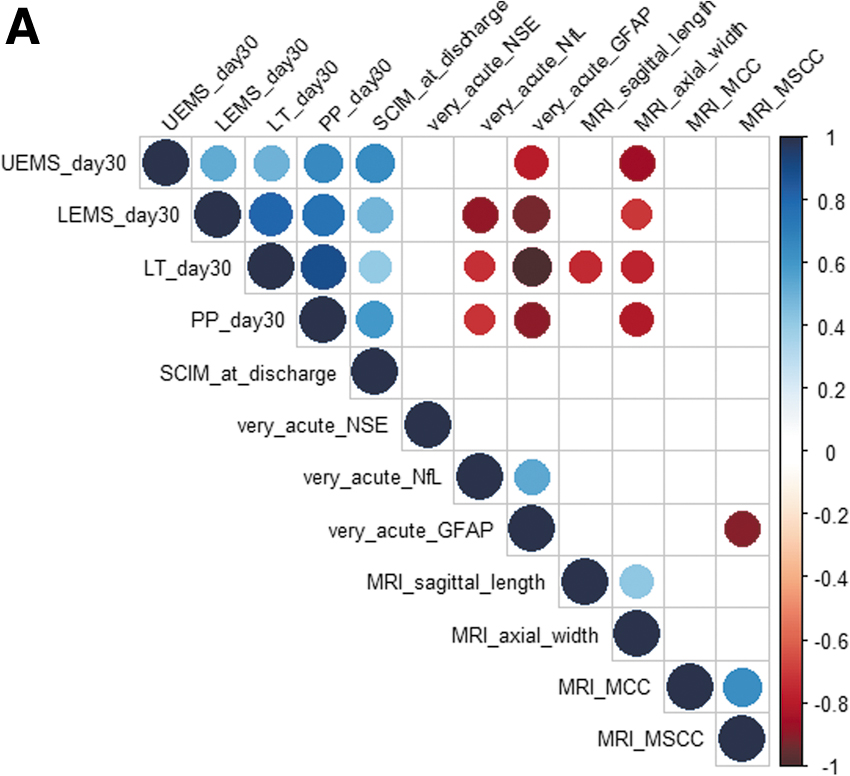
Correlation matrix: significant Pearson's correlation coefficients; significance level p < 0.05. The axial lesion width according to magnetic resonance imaging (MRI) correlates significantly with upper extremity motor score (UEMS), lower extremity motor score (LEMS), pin prick (PP) sensory score, light touch (LT) sensory score 30 days post-injury; the longitudinal length of intramedullary lesion (IML) correlates only with the light touch (LT) sensory score; and maximum spinal cord compression (MSCC) correlates significantly inversely with the serum concentration of glial fibrillary acidic protein (GFAP) in the very acute post-injury phase (Days 1-4 post-injury). Color image is available online.

T2-weighted sagittal MRI indicating extensive intramedullary edema.
Focusing on MRI parameters, MSCC correlates significantly inversely with the GFAP levels in the very acute post-injury phase (Fig. 3A). Negative MSCC values are indicative of swelling of the spinal cord which is predominantly seen in more severe SCI. 25,28 The significant negative correlation between MSCC and GFAP (Pearson's r = -0.61, p = 0.0034) outlines that more severely injured individuals—by means of swelling—have higher serum concentrations of GFAP in the very acute phase after SCI. An example of a very extensive swelling on MRI is shown in Figure 3B.
Spearman's rank correlation was calculated to evaluate if BASIC score and Sagittal Grade are related to neurological function (ISNCSCI, SCIM) and the serum concentration of neural markers (Fig. 4A). BASIC score as well as Sagittal Grade correlate significantly with neurological function as described in previous literature. 24,26,36 However, GFAP levels in the very acute post-injury phase (Days 1-4) also correlate significantly with Sagittal Grade (Spearman's ρ = 0.53, p = 0.014) with higher levels in more severe lesions (Fig. 4A, 4B). Neither NfL, nor NSE correlated significantly with BASIC score or Sagittal Grade (p > 0.05).
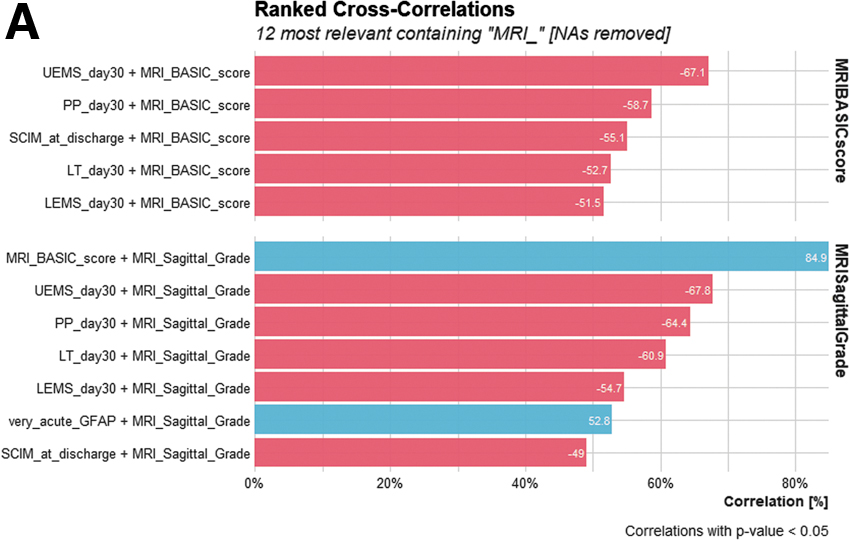
Spearman's rank correlation for magnetic resonance imaging (MRI) Brain and Spinal Injury Center (BASIC) score and MRI Sagittal Grade; MRI BASIC score correlates significantly with upper extremity motor score (UEMS; lower extremity motor score (LEMS; pin prick (PP) sensory score; light touch (LT) sensory score 30 days post-injury; and Spinal Cord Independence Measure (SCIM) at discharge; MRI Sagittal Grade correlates significantly with MRI BASIC score, UEMS, LEMS, PP sensory score, LT sensory score 30 days post-injury, SCIM at discharge, and the serum concentration of glial fibrillary acidic protein (GFAP) in the very acute post-injury phase (Days 1-4 post-injury). Color image is available online.
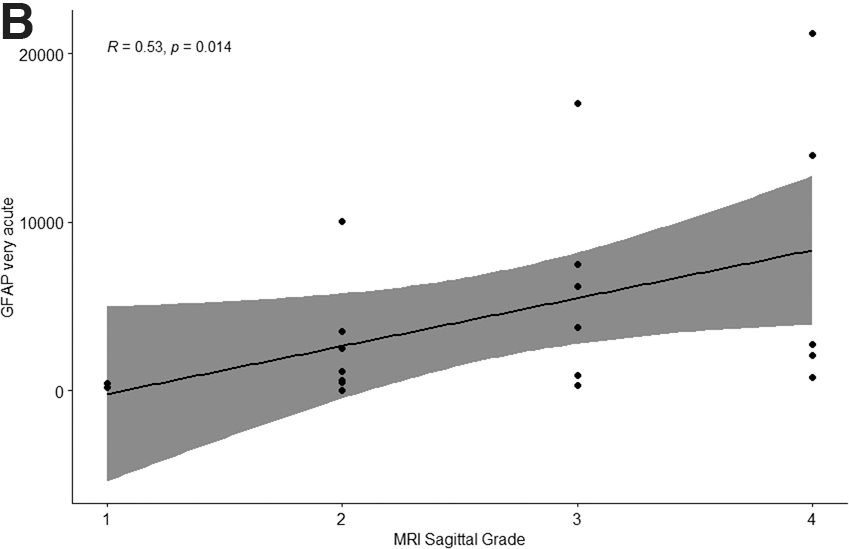
Spearman's rank correlation between Sagittal Grade in pre-operative magnetic resonance imaging and glial fibrillary acidic protein (GFAP) in the very acute post-injury phase (Days 1-4 post-SCI). More severe injuries are related to higher serum concentrations of GFAP.
Discussion
Surrogate markers are of uttermost importance in the diagnosis and prognosis for patients with SCI concerning the clinical management and for research purposes. In our study, serum levels of NfL and GFAP have shown promising diagnostic capacity in the very early stage of injury (1-4 days post-SCI). URP defined cut-off values for both markers to differentiate between individuals with SCI and healthy controls thereby providing an avenue for the diagnosis of presence of SCI in early post-injury phase where clinical examination is sometimes complicated by several confounders. Also, GFAP correlated significantly with ISNCSCI sub-scores and therefore also qualifies as a marker for injury severity.
GFAP is an astrocyte-specific intermediate filament protein that is elevated as a result of cellular damage after SCI with higher concentrations in more severely injured patients. 2,11 -13,19 NfL is a neuronal cytoplasmic protein which is released from damaged neurons and therefore constitutes a non-specific marker of neuronal injury/degeneration. 37,38
Although, GFAP and NfL have shown to facilitate diagnosis and outcome prediction after TBI, 5,6 literature on the diagnostic value in serum after traumatic SCI is tenuous. Kuhle and colleagues found up to 14-fold increased levels of NfL in individuals with acute SCI compared with healthy controls. In the group of individuals with SCI, serum levels of NfL continued to increase within the first week post-injury and correlated significantly with motor scores. The study reported higher serum concentrations of NfL in patients with a poor outcome. 20
Further, several studies found increased levels of NfL in CSF in patients with spinal cord ischemia as a complication of aortic aneurysm repair within the first days post-operative. 7 -9 CSF levels of NfL increased by up to 37 times within 24-48 h after endovascular aortic repair in patients with post-operative neurological dysfunction. 7 Also, two other studies including patients with spinal cord ischemia during thoraco-abdominal aortic repair found significantly increased CSF, as well as serum concentrations of GFAP, NfL, NSE, and S100B in the first 3-4 days post-operatively in patients with SCI compared to asymptomatic patients. 9,10 These findings are in accordance with a systematic review on spinal cord ischemia due to aortic aneurysm repair surgery summarizing that CSF levels of S100, NfL, and GFAP are elevated within 4 days post-operative. 8 Our findings coincide with previous findings showing that GFAP as well as NfL correlate with injury severity by means of ISNCSCI scores (Fig. 2).
Studies investigating both, CSF and serum concentrations, reported that CSF levels did not consistently correlate with concentrations in peripheral blood in patients with ischemic SCI. 8,10 In contrast, studies investigating biomarkers in acute TBI reported about the predictive value of several proteins measured in blood serum. Serum concentration of S100B and GFAP from a sample collection within 4 h after injury, together with baseline patient characteristics predict outcome after moderate-to-severe TBI. 5 Additionally, among several biomarkers (S100B, ubiquitin carboxy-terminal hydrolase-L1 (UCH-L1), GFAP, and tau), the serum levels of GFAP and NfL within the first 2 weeks after TBI contributed the most significant information to predict outcome and mortality. 6
The debate whether biomarker concentrations in CSF and serum correlate has not yet been resolved completely and is dependent on the ability of a marker to cross the blood–brain barrier (BBB), BBB integrity, and the post-injury time interval. 4,11,39,40 For some proteins, like S100B, the extravasation from the injured CNS into the bloodstream may be more indicative of BBB integrity than injury severity. 11,39 Serum levels of NfL are not influenced by BBB permeability, with a strong correlation between the concentration in serum and in CSF in individuals with different degrees of BBB impairment. 41
Kwon and colleagues found that CSF levels of GFAP were orders of magnitude greater than in serum 24 h post-SCI, and the time course of expression showed that GFAP was upregulated very early after SCI in the CSF depending on injury severity. 2
Studies including patients with spinal cord ischemia as a consequence of aortic repair surgery have shown that biochemical markers in CSF did not increase until after the appearance of clinical signs of neurological dysfunction. Therefore, an upregulation occurs too late for an intra-operative monitoring, 7,9 although CSF levels of GFAP increased before or in parallel to symptom onset. 9,10 This early upregulation, together with the findings in acute TBI suggest that GFAP might be a promising diagnostic biomarker in the very acute phase post-SCI. Our findings add to this emerging body of research by proposing GFAP as a marker for the presence and severity of acute traumatic SCI.
MRI findings versus neural markers
Previous studies reported, that MRI findings within the first 24-48 h after SCI are related to injury severity. 24,28 Swelling of the spinal cord is associated with more severe injuries and worse neurological outcome. 28,42,43 The expansion rate of spinal cord edema is measured by MSCC and is particularly high within the first 24 h after injury. 28,44 The time from injury to MRI was 4.91 (4.31) mean (SD) h in our cohort ranging from 1.72 to 17.33 h. Serum levels of GFAP 1-4 days after SCI correlated significantly with Sagittal Grade and MSCC (p < 0.05). This is in accordance with previous findings reporting strong correlations of CSF levels of GFAP with lesion, and hematoma length on pre-operative MRI. 12
Limitations
Due to missing data in terms of neurological assessment according to ISNCSCI in our study cohort in the very acute phase, we had to fall back to AIS ISNCSCI scores from the sub-acute examination 30 days post-injury in our analysis.
Generally, SCI is often accompanied by concomitant TBI and/or peripheral nervous injuries. Therefore, a differentiation by means of blood parameter would not be reliable in those cases, as GFAP and NfL are not specific to lesions of the spinal cord. Also, the time window of sample collection (Days 1-4) might confound the serum concentrations of neural markers and future studies should strive to collect blood samples in a narrower post-injury time frame or if possible, several times during the acute stage of injury. For quantification of neural markers, we used a research-use only R-Plex assay that is not approved for clinical use. Therefore, the proposed cut-offs should be considered preliminary.
Conclusion
Serum concentrations of NfL and GFAP within the first 4 days post-injury distinguish individuals with SCI from healthy controls, and correlate with the extent of the lesion according to MRI. Serum levels of NSE were not significantly associated with clinical scores, or MRI parameters in our cohort. Accordingly, NfL and GFAP qualify as potential diagnostic biomarkers for the presence and severity of SCI in the very early stages of SCI.
Footnotes
Acknowledgments
Ethics approval: All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the ethics committee of the Ethics Committee of the Bavarian Medical Board. The study was registered on the
Consent to participate: All participants provided written, informed consent.
Consent for publication: All authors have read and approved the manuscript.
Authors' Contributions
LG, AAM, DGO, LA, DM, and IL conceived and designed the study. LG, BA, AG, AAM, DGO, LA, and IL were responsible for drafting of the manuscript. IL was responsible for statistical analysis and interpretation of results. OM was responsible for curation of data. BA was responsible for serum analysis. AG performed radiological classification. CW was responsible for blood sample collection. BA, DM, AAM, DGO, LA, LG, and IL performed critical revision of the manuscript regarding important intellectual content. All authors read and approved the final manuscript.
Funding Information
The main study on which this post hoc analysis is based on was funded by the Fundacion Mutua Madrileña in 2014. The assays for serum analysis in this study were funded by the Spinal Cord Injury and Tissue Regeneration Center Salzburg (SCI-TReCS).
Author Disclosure Statement
No competing financial interests exist
Supplementary Material
Supplementary Material: Analytical Procedures