
Abstract
The clinical evaluation of spinal afferents is an important diagnostic and prognostic marker for neurological and functional recovery after spinal cord injury (SCI). Particularly important regarding neuropathic pain following SCI is the function of the spinothalamic tract (STT) conveying nociceptive and temperature information. Here, we investigated the added value of neurophysiological methods revealing discomplete STT lesions; that is, residual axonal sparing in clinically complete STT lesions. Specifically, clinical pinprick testing and thermal thresholds were compared with objective contact heat-evoked potentials (CHEPs) and a novel measure of pain-autonomic interaction employing heat-induced sympathetic skin responses (SSR). The test stimuli (i.e., contact heat, pinprick) were applied below the lesion level in 32 subjects with thoracic SCI while corresponding heat-evoked responses (i.e., CHEPs and SSR) were recorded above the lesion (i.e., scalp and hand, respectively). Readouts of STT function were related to neuropathic pain characteristics. In subjects with abolished pinprick sensation, measures of thermosensation (10%), CHEPs (33%), and SSR (48%) revealed residual STT function. Importantly, SSRs can be used as an objective readout and when abolished, no other proxy indicated residual STT function. No relationship was found between STT function readouts and spontaneous neuropathic pain intensity and extent. However, subjects with clinically preserved STT function presented more often with allodynia (54%) than subjects with discomplete (13%) or complete STT lesions (18%). In individuals with absent pinprick sensation, discomplete STT lesions can be revealed employing pain-autonomic measures. The improved sensitivity to discerning STT lesion completeness might support the investigation of its association with neuropathic pain following SCI.
Introduction
Spinal cord injury (SCI) results in disrupted sensorimotor communication through the site of neuronal damage. The standard neurological classification of an SCI encompasses sensory and motor testing, and defines a clinically complete SCI by the absence of sensorimotor function in the most sacral segments of the spinal cord. 1 Early studies from the 1980s reported preserved supraspinal motor control in subjects with such clinically complete SCI, and shaped the terminology of “discomplete” lesions. 2 –4 The term “discomplete lesion” was defined as neurophysiological evidence of residual axonal sparing in clinically complete lesions. 3,5 Further studies revealed a notable number of subjects with discomplete SCI, and the terminology was extended to the sensory system assessed with magnetic resonance imaging or electrophysiology. 6 –9 The identification of residual subclinical neuronal function offered a possible explanation for the prevalence of excessive spasticity 10 and, potentially, also the prevalence of neuropathic pain (NP) after SCI. 11 For the development of NP, residual function of the spinothalamic tract (STT) might be of particular importance. Multiple studies indicated that lesions of spinothalamic projections are necessary, however not sufficient, for the development of NP. 12,13 Strikingly, STT damage did not predict NP after SCI, 14 but residual STT function contributed to severe NP. 11,15 Additionally, partial integrity of pain pathways measured by laser-evoked potentials increases the probability of developing stimulus-evoked pain; that is, allodynia and hyperalgesia. 16
The neurological assessment of an SCI contains pinprick testing as a proxy for STT function. 1 This clinical bedside testing can be complemented with thermal stimulation, in particular cold and warm detection thresholds, to test STT integrity. 17 –20 In addition to bedside examination tools used in the clinical work-up of spinal lesions, electrophysiological methods including pain-related evoked potentials provide objective evidence of preserved somatosensory function. 21,22 In particular, contact heat-evoked potentials (CHEPs) provided additional value revealing residual STT function compared with pinprick testing in subjects with spinal disorders. 23,24 In general, contact heat or laser stimuli activate thermo-nociceptive primary afferents projecting to the fast-conducting STT. 25 The synchronized afferent volleys are relayed through thalamic nuclei and further processed within the insular and anterior cingulate cortex, 26,27 ultimately being recordable as pain-related evoked potentials. Beyond this activation pattern, nociceptive stimuli activate the central autonomic network composed of multi-synaptic spinal pathways to brainstem regions including the reticular formation, nucleus tractus solitarii, parabrachial nucleus, and ventrolateral medulla. 28 Further, the activation of the medial thalamic nuclei is conveyed to several brain regions including the amygdala and hypothalamus. 28 The activation of the central autonomic network by painful stimuli results in sympathetic activity; for example, increased vascular and sudomotor function. 28,29 The fact that thermo-nociceptive stimuli are processed in manifold ways along the nociceptive neuraxis and thereby evoke different somatosensory and autonomic responses may be leveraged as part of the assessment of the functional integrity in spinal lesions. Therefore, the primary objective was to investigate measures of pain-autonomic interaction; that is, heat-induced sympathetic skin responses (SSRs), as a readout for residual STT function in subjects with SCI. Our hypothesis was that the measure of heat-induced SSR has an additional value by unmasking discomplete STT lesions compared with conventional clinical testing; that is, pinprick and thermal thresholds, and CHEPs. The secondary objective was to investigate how residual STT function relates to the presence and clinical phenotype of NP after SCI. We hypothesized that subjects with spared STT function after SCI are more likely to report spontaneous NP and allodynia.
Methods
Subjects
This study was performed in 34 subjects with chronic thoracic SCI. Subjects were recruited through the Swiss Spinal Cord Injury Cohort Study (SwiSCI) database and a local outpatient registry at Balgrist University Hospital in Zurich, Switzerland. Inclusion criteria were (1) having had an SCI for ≥1 year and (2) neurological level of injury between T1 and T12. Exclusion criteria were (1) having neurological disorders other than SCI and (2) psychiatric or cognitive status interfering with the study.
Study design
The study was designed as a one-visit, cross-sectional study. All subjects provided written informed consent, and all procedures were in accordance with the Declaration of Helsinki. The study was approved by the local ethics board Kantonale Ethikkommission Zürich, KEK (ref. number: EK-04/2006, PB_2016-02051,
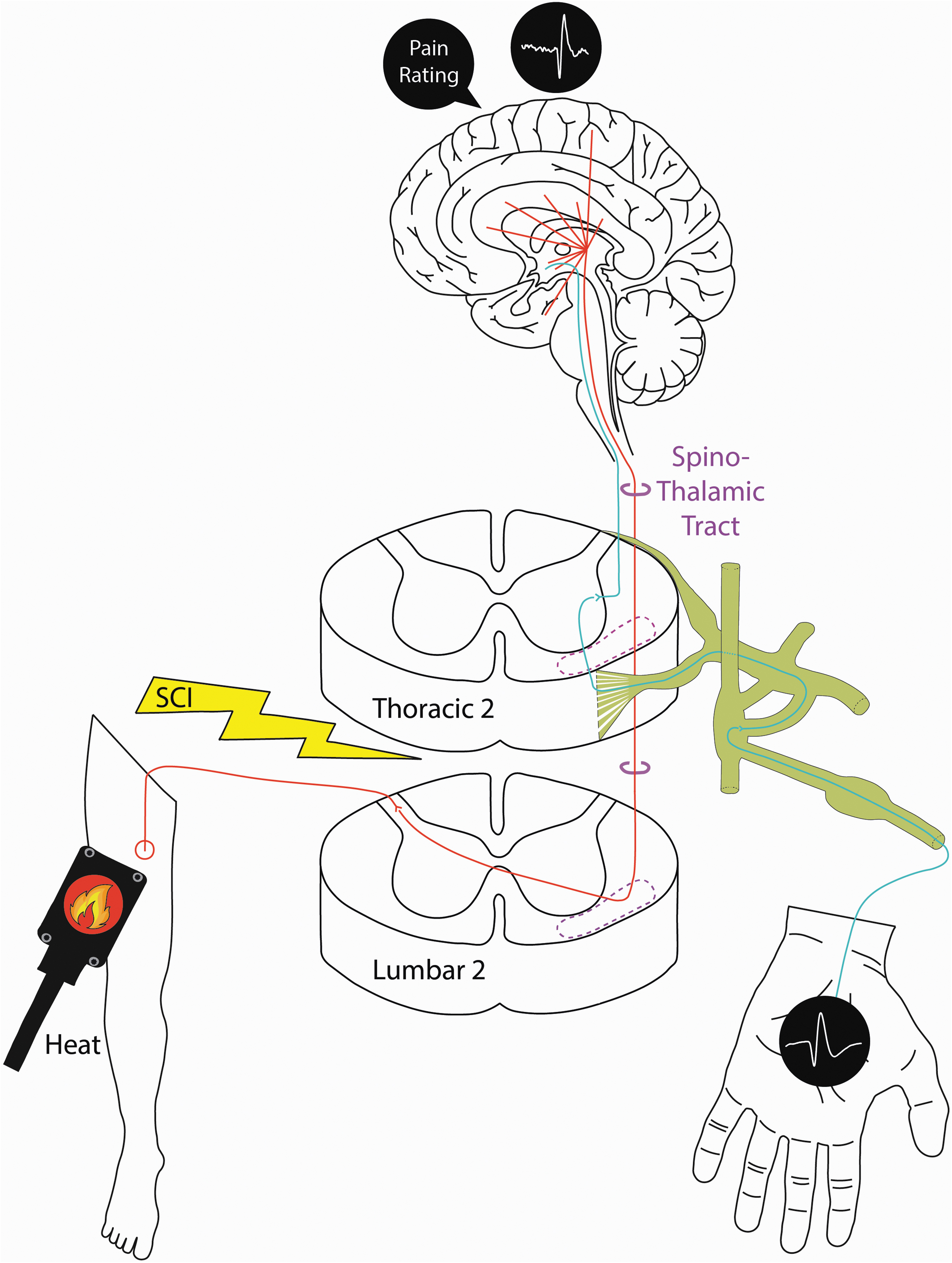
Schematic drawing of neuroanatomical pathways of electrophysiological readouts to noxious heat application below a spinal cord injury. Contact heat stimuli were applied to the right thigh. The peripheral nociceptive neurons synapse to the second-order neurons of the nociceptive neuraxis (red) at the corresponding L2 and adjacent spinal levels (Lissauer's tract, not shown). These neurons cross the midline of the spinal cord and comprise the STT (purple). Activation of thalamic nuclei is relayed to multiple brain regions of the pain matrix as well as autonomic centers; for example, the hypothalamus. Pain rating was noted as a subjective readout, whereas CHEPs and SSRs were recorded as objective readouts of the noxious heat stimuli. Autonomic efferent control (blue) includes spinal sympathetic pre-ganglionic neurons (high thoracic level), the paravertebral chain, and post-ganglionic neurons innervating the specific effector organ; that is, eccrine sweat glands of the hand. CHEPs, contact heat-evoked potentials; SSRs, sympathetic skin responses; STT, spinothalamic tract. Color image is available online.
Clinical assessment and pain phenotyping
Subjects underwent a standard neurological assessment (International Standards for Neurological Classification of Spinal Cord Injury [ISNCSCI]) in which sensorimotor complete SCI (American Spinal Injury Association impairment Scale; [AIS A]) is defined as absent sacral sparing (S4-5 dermatomes), and incomplete SCI is defined as preserved sensory and/or motor function (AIS B–D). 1 Pinprick testing on the right mid-thigh (L2 dermatome), an area below the lesion, was used as a proxy for STT integrity. Next to pinprick, thermosensation was tested using cold and warm detection thresholds (CDT, WDT) in accordance with the German Research Network on Neuropathic Pain (DFNS) protocol. 33 A contact heat stimulator (PATHWAY Pain & Sensory Evaluation System, Medoc Ltd., Ramat Yishai, Israel) using a thermode with a 3 x 3 cm contact surface and a heating and cooling rate of 1°C/sec was applied with safety cutoffs at 0 and 50°C. 18
The pain phenotyping included a central NP assessment according to the International Association for the Study of Pain (IASP) Neuropathic Pain Special Interest Group (NeuPSIG) guidelines. 34,35 The NP subtype was classified as at- or below-level according to the International Spinal Cord Injury Pain criteria. 36 Presence of allodynia was tested with 25°C and 40°C thermorollers (Somedic, Hörby, Sweden), a brush, and the International Spinal Cord Injury Pain Data Set (ISCPDS) questionnaire. 35 Based on previous literature, pain extent was reported as the number of 13 body regions affected by NP 18,35 and with pain drawings using two DIN-A4 papers with standardized body charts (frontal/dorsal view). 37 Shaded body areas of perceived NP at the moment were assessed by (1) verbal descriptors, (2) pain intensity (numeric rating scale [NRS]; 0 = no pain, 10 = worst pain imaginable), and (3) type of NP (evoked or spontaneous). Only NP intensities of ≥3 NRS were taken into account for further analyses. The shaded pixels were analyzed as percentage of total body area.
CHEPs
Recording of CHEPs was performed based on a previously published setup. 23,24,38 –41 Briefly, 20 heat stimuli to the right mid-thigh; that is, below the lesion level (see Fig. 1), were applied after a familiarization on the left forearm. The heat stimuli had a baseline and destination temperature of 42°C and 52°C, respectively. 23,24,38,41 Within the inter-stimulus interval of 15–19 sec, the thermode positioning was slightly changed to avoid peripheral adaptation. 42 Subjects were instructed to rate the pain intensity of the applied heat stimulus on the NRS after an auditory signal. CHEPs were recorded at the vertex (Cz, referenced to the earlobes) using a customized LabVIEW program (V2.04 CHEP, ALEA Solutions, Zurich, Switzerland) with a recording time of 10 sec including a 1-sec pre-trigger window. The signals were acquired at 2000 Hz using a preamplifier (20000x, ALEA Solutions, Zurich, Switzerland) and band-pass filtered in the range of 0.5–30 Hz. During offline analysis, individual trials were inspected by two examiners for artefacts (e.g., coughing, blinking, and spasticity). The resulting 15 artifact-free trials were averaged to determine N2 latencies and N2P2 amplitudes.
Pain-autonomic interaction: Sympathetic skin responses
While CHEPs were recorded as cortical responses to noxious heat stimuli, sympathetic sudomotor activity elicited by the same noxious stimulus; that is, heat-induced SSRs, were simultaneously measured as a readout for pain-autonomic interaction (see Fig. 1). SSRs were recorded with self-adhesive recording electrodes (AMBU BlueSensor NF-50-K/W, Ambu, Denmark) on the left hand. The signals were acquired with the same setup as described previously for CHEPs albeit using a moving average filter of 50 samples for the recorded signal. Quantitative analysis of the SSR trials included the latency and peak-to-peak amplitude. In order to ensure intact sympathetic innervation of the recorded hand, heat stimuli were also applied above the lesion level; that is, at the volar forearm.
Data classification and statistics
The four proxies of STT function; that is, pinprick, thermosensation, CHEPs, and SSR, were grouped into “abolished” and “preserved” function. Preserved function was assumed if (1) the pinprick score was a 1 (impaired) or 2 (normal); 1 (2) any thermal thresholds could be measured; (3) any CHEP was recordable, even with delayed latency or small amplitude; and (4) two or more out of five heat stimuli resulted in SSRs. 43 –45
Further, we introduced three classifications of STT lesion completeness: (1) “Incomplete”, (2) “complete”, and (3) “discomplete” STT lesions. The first two classifications were based on subjective clinical pinprick- and thermosensation being preserved or abolished, respectively. “Discomplete” STT lesions were classified by preserved objective CHEPs and/or SSRs readouts in “complete” STT lesions (abolished clinical measures). 3,5 –8
Statistical analysis
Statistical analyses were performed using R Studio (version 4.0.4). Normal distribution was tested using the Shapiro–Wilk tests and histograms. As most parameters were non-normally distributed, the data is reported as median and inter-quartile range (25th–75th percentile). Chi-square and Kruskal–Wallis tests were performed to compare pain parameters among three STT lesion classifications, with p < 0.05 considered as statistically significant.
Results
Subject characteristics
Thirty-two out of the 34 SCI subjects were included in the study. Reasons for dropout were a small fiber neuropathy detected during the study measures (n = 1) and an inability to follow experimental instructions (n = 1). Demographics and clinical subject characteristics are listed in Table 1. The subjects (5 females, 27 males) had a median age of 57.5 years (53.7–62.3 years) and a time since injury of 14.5 years (8.3–24.2 years). Half of the subjects were classified as having an injury that was sensorimotor complete (AIS A). NP below the level of injury was reported in 18 subjects (intensity: 5.8 NRS [3.5–7.0], extent: 5.5 regions [4.0–7.0 regions] or 11.5% [5.3–35.8%] of total body area, see Table 2 for NP characteristics). The median PCS score of 10.0 points (3.0–15.75 points) and BDI-II score of 7.0 points [3.0–10.5 points] reflected clinically relevant catastrophizing 30 in only one subject (32 points) and no moderate or severe depression in the total study cohort. Further, the PCS and BDI-II scores were related neither to the presence of spontaneous NP (p = 0.931, p = 0.193, respectively) nor to the presence of evoked NP (p = 0.394, p = 0.089, respectively). The current pain medication included anti-epileptic drugs (n = 8), non-steroidal anti-inflammatory drugs (n = 5), antidepressants (n = 4) and cannabinoids (n = 1).
Demographics and Clinical Characteristics of Subjects with Spinal Cord Injury (SCI)
AIS, American Spinal Cord Injury Association Impairment Scale; NLI, neurological level of injury; NT, non-traumatic; T, traumatic; Th, thoracic.
Pain Characteristics of Spinal Cord Injured (SCI) Subjects with Neuropathic Pain (NP)
The pain phenotype was segregated into spontaneous at- and below-level NP with intensity and extent. Additionally, the presence of thermal/mechanical allodynia and the intake of pain medication are reported. NRS, numeric rating scale.
STT function: From clinical to electrophysiological assessments
Based on the pinprick score (ISNCSCI examination) of the thigh, 21 subjects (66%) presented with abolished and 11 (34%) presented with preserved STT function. Thermosensation (CDT and WDT) was abolished in 20 (62%) and preserved in 12 subjects (38%). The latter group showed a CDT of 28.4°C (20.5–30.2°C) and a WDT of 37.3°C (35.6–42.6°C). Electrophysiological testing revealed 16 subjects with recordable CHEPs (50%) and abolished ones in the other half. Compared with normative data, the SCI subjects presented with increased CHEP latencies (N2 latency: 356 [350–442] ms) and lower pain ratings (3.5 [1.8–6.6] NRS), while CHEP amplitudes (N2P2 amplitude: 21.6 [17.1–27.9] μV) were within normal range. 41 Interestingly, SSRs were recorded in more than half of the subjects (66%, 21/32) after contact heat stimulation of the thigh. All analyzed SSRs (amplitude: 1212 [904–1836] μV; latency: 1.92 [1.85–2.04 sec]) were time locked to the stimulus.
Intact nociceptive processing above the level of injury was guaranteed in all subjects as they showed preserved CHEPs and palmar SSRs after stimulation of the volar forearm. This also confirmed the integrity of efferent sympathetic pathways to the hands (recording site).
A summary of pinprick sensation and electrophysiological outcomes is shown in Figure 2. All subjects with normal pinprick sensation presented with recordable CHEPs and SSRs, in line with preserved STT function. Out of the six subjects with impaired pinprick sensation, CHEPs were recorded in four (67%) and SSR was recorded in all subjects (100%). Most importantly, in the 21 subjects with absent pinprick sensation, thermosensation was preserved in 2 (10%), whereas CHEPs were recorded in 7 (33%) and SSR was recorded in 10 (48%). Additionally, heat-induced SSRs as a readout for pain-autonomic interaction was more sensitive for preserved STT function compared with CHEPs (abolished CHEPs, but preserved SSR, n = 5). Ultimately, when SSRs were abolished, none of the other proxies indicated preserved STT function. Representative examples of CHEPs and SSR recordings are shown in Figure 3.

Flow chart of pinprick sensation (subjective) and electrophysiological (objective) readouts of spinothalamic tract (STT) function (n = 32). Summary of pinprick testing (pinprick score: normal = 2, impaired = 1, absent = 0) and recordable CHEPs as well as concomitant pain-autonomic interaction; that is, SSR. Cases with residual STT function assessed by CHEPs and SSR recordings are highlighted in bold font and thick boxes. CHEPs, contact heat-evoked potentials; SSR, sympathetic skin response.
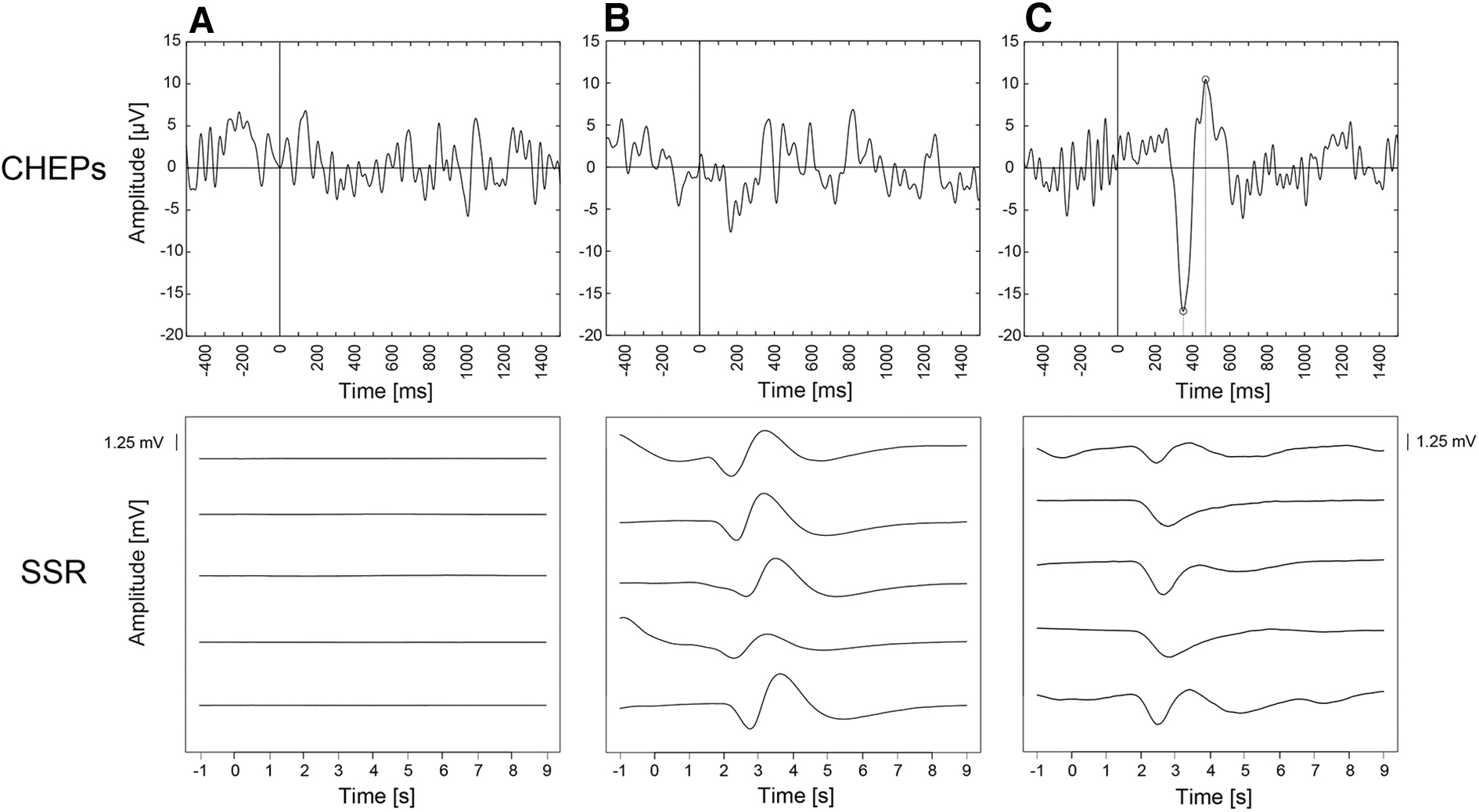
Representative examples of contact heat-evoked potentials (CHEPs) and simultaneous palmar sympathetic skin response (SSR) recordings in paraplegic subjects.
Completeness of STT lesion and NP
Sensorimotor complete (AIS A) subjects presented with more severe STT damage (9 complete, 6 discomplete, 1 incomplete STT lesion) than sensorimotor incomplete subjects (AIS C: 2 complete, 3 discomplete, 0 incomplete; AIS D: 0 complete, 4 discomplete, 7 incomplete).
Figure 4 depicts a flow chart including the two clinical and the two electrophysiological proxies for the classification of STT lesion completeness. Based on clinical measures of pinprick and thermosensation, 13 subjects had an incomplete and 19 subjects had a complete STT lesion. Strikingly, eight of the subjects with a clinically complete STT lesion presented with recordable CHEPs and/or SSRs, and were therefore defined as having a discomplete lesion. The electrophysiological parameters for the three STT lesion classifications are displayed in Table 3.
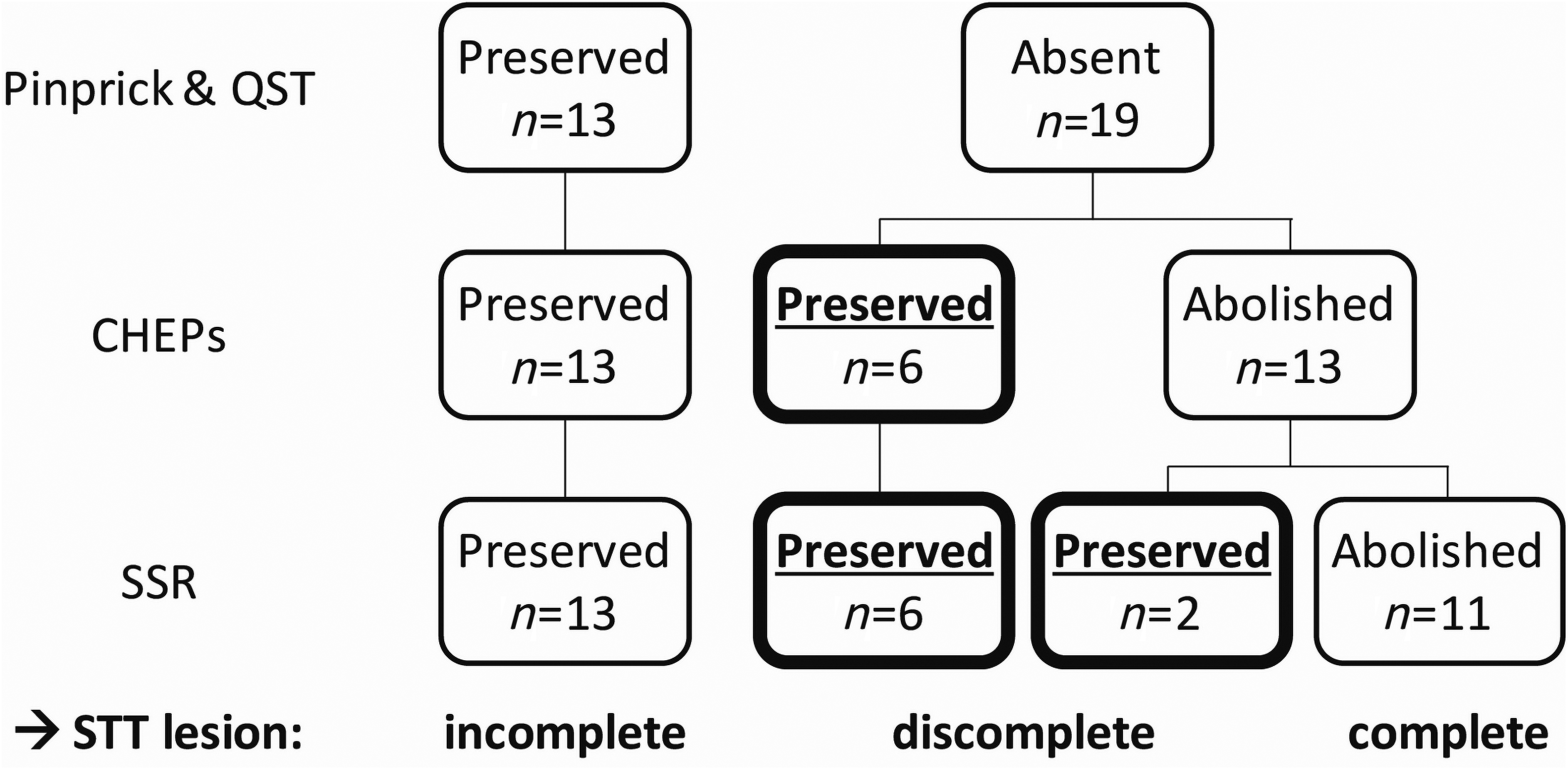
Flow chart for the classification of spinothalamic tract (STT) lesions into incomplete, discomplete, and complete subgroups via clinical assessments of STT function (pinprick and thermosensation). Discordant findings between clinical and electrophysiological measures are highlighted in bold. A total of eight spinal cord injured (SCI) subjects presented with a discomplete STT lesion. CHEPs, contact heat-evoked potentials; QST, quantitative sensory testing; SSR, sympathetic skin response.
Parameters of Contact Heat-Evoked Potentials (CHEPs) and Sympathetic Skin Response (SSR) after Contact Heat Stimulation at the Thigh Shown for the Three STT Lesion Classifications
Parameters are reported as median ± IQR. Mann–Whitney U tests were performed to compare incomplete and discomplete STT lesions. Statistical significance at p < 0.05 is shown in bold. IQR, interquartile range; NRS, numeric rating scale; STT, spinothalamic tract.
The NP phenotype for the three different STT lesion classifications can be seen in Table 4. The presence of spontaneous NP was equally distributed over the three groups; 62% of subjects with incomplete, 50% of subjects with discomplete, and 55% of subjects with complete STT lesions (p = 0.866). Further, no group differences were seen for NP intensity (p = 0.784), extent (p = 0.401), or psychological readouts (PCS, p = 0.644; BDI, p = 0.876). Allodynia was most prevalent in subjects with incomplete STT lesions (54%), compared with subjects with discomplete or complete STT lesions (13% and 18%, respectively, p = 0.072).
Spinothalamic Tract (STT) Lesion Severity and Pain Characteristics
According to clinical and electrophysiological measures, the STT lesion completeness could be classified into three groups: incomplete, discomplete, and complete. Parameters are reported as percentage or median ± IQR. IQR, interquartile range; NRS, numeric rating scale.
Discussion
This study highlights the additional value of pain-autonomic interaction measures in the assessment of residual STT function in SCI subjects. The objective neurophysiological recordings of CHEPs and heat-induced SSRs revealed discomplete STT lesions in subjects with abolished sensation measured by conventional clinical sensory testing. The concurrent recording of SSR, in addition to cortical responses to heat stimuli, further improved the detection of residual STT function. Additionally, our results revealed an association of STT function with the presence of allodynia, whereas spontaneous NP was not related to the degree of STT lesion completeness.
The value of pain-autonomic interaction measures detecting discomplete spinal lesions
Awad and colleagues revealed discomplete lesions in ∼50% of sensorimotor complete subjects using both innocuous tactile and sharp nociceptive stimuli. 7 In comparison, our study revealed 42% discomplete lesions in subjects without clinically preserved pinprick sensation. Whereas pinprick testing assesses mechano-nociceptive processing along the neuraxis including peripheral Aδ fibers and the STT, 46 our other proxies rely on thermo-nociceptive processing. We particularly focused on the thermo-nociceptive system with the spinothalamic and spinoreticular tract as main ascending systems within the anterolateral system of the spinal cord. 47 In accordance with several studies, 17,23,24 subjects with absent pinprick sensation or thermal thresholds showed subclinical preservation of STT function assessed by CHEPs (7/21 and 8/21, respectively). On average, the preserved CHEPs had prolonged latencies compared with normative data, indicating damage to the nociceptive neuraxis. 41,48 Further, we showed that the preserved STT integrity in discomplete STT lesions was associated with longer CHEPs N2 latencies and lower SSR peak-to-peak amplitudes compared with incomplete STT lesions. This finding highlights altered electrophysiological recordings in subjects with partial damage of the STT; that is, discomplete lesion.
Next to CHEPs, measures of heat-induced SSR even increased the number of detectable discomplete lesions (8/19). The recording of palmar SSRs in all subjects when stimuli were applied above the lesion level assured the integrity of the pain-autonomic interaction including intact efferent sympathetic innervation of the palmar eccrine sweat glands. This is of particular importance when interpreting the SSR recording and using it as a proxy for afferent nociceptive processing. However, in comparison with previous literature, the preserved SSRs in our study sample had prolonged latencies, possibly attributable to impaired afferent conduction in line with damage to the nociceptive neuraxis. 48
Preservation of CHEPs and SSR despite loss of the respective perceptual correlates suggests a dissociation of spared nociceptive signaling from subjective pain perception. Indeed, there is evidence that sympathetic responses are more related to stimulus intensity than subjective pain perception. 49 Our results support this dissociation of spared nociception from pain perception with subjects showing no pinprick and thermal sensation, but recordable SSRs. 6 For example, a potential confounding effect of stimulation awareness on SSR recordings can especially be neglected in subjects without perceived heat pain (n = 8).
The comparison of the objective proxies for STT function revealed that roughly one third of the subjects with abolished CHEPs had preserved SSRs (5/16). This difference might be explained by the fact that thermo-nociceptive stimuli are processed in different pathways along the nociceptive neuraxis. Whereas the generation of cortical evoked potentials after radiant heat stimulation relies in particular on thermo-nociceptive Aδ fibers and fast-conducting fibers of the lateral STT; that is, the neospinothalamic tract, SSR can be elicited by a variety of afferent signaling; for example, electrical, heat, and cold. 16,50 Specifically, the spino-reticular-thalamic system is assumed to be involved in alertness and arousal in response to nociceptive stimuli. Slower conducting multi-synaptic pathways; that is, the paleospinothalamic tract, might be responsible for SSRs when fast-conducting fibers in the lateral STT are damaged (abolished CHEPs). 25,47 Another possible explanation for improved sensitivity, might be that CHEPs are reported to be dependent on highly synchronized afferent volleys, 23,24 whereas SSR might be elicited via less intact fibers, because already, minor arousing stimuli are captured with autonomic recordings. 51
In conclusion, measures of pain-autonomic interaction can complement CHEPs for the assessment of spinal lesions possibly by taking advantage of assessing the phylogenetically older spino-reticulo-thalamic pathway.
Association of residual STT function with NP
The association of STT function with NP is heavily discussed in the field of central NP. Previous studies reported that STT damage is a necessary condition for NP development; however, NP development cannot be sufficiently explained by STT damage only. 12,13 It has been shown that SCI subjects with and without NP had similar loss of STT function at and below the level of injury, 15 and impairment or loss of STT function is not a significant NP predictor. 12,14 Our findings on the lack of a difference in spontaneous NP; that is, presence, intensity, and extent, among the three different STT lesion classifications (incomplete, discomplete, complete) are in accordance with these studies. Next to the impact of STT functional integrity, the presence and severity of ongoing central NP have previously been discussed with mechanisms such as hyperexcitability and disinhibition within the central nervous system. 14,15,52,53 These mechanisms, as potentially reflected in increased windup and lack of conditioned pain modulation, might further improve the mechanistic exploration of the effects caused by the structural STT damage, eventually resulting in spontaneous NP. Although no additional readouts on mechanistic changes were performed in the current study, a recent study found a significant mediation effect of conditioned pain modulation in the link between STT damage and central NP. 54 This study by Defrin and colleagues further highlighted the value of assessing anti-nociceptive indices (such as conditioned pain modulation) in predicting NP. 54 Further, the highly debated imbalance theory claims that STT dysfunction in conjunction with preservation of the dorsal columns is responsible for NP development. 15
With regard to evoked pain, we found that only 38% (8/21) of our subjects with residual STT function; that is, incomplete or discomplete, reported allodynia, indicating that STT preservation is not sufficient for the development of allodynia. However, preserved STT integrity may be a requirement for the development of evoked pain, whereas patients with a profound deafferentation had spontaneous pain exclusively. 11,16,55 It has been hypothesized that subjects with large lesions – affecting the whole STT system – are less prone to imbalanced spino-thalamic subsystems; that is, the medial/lateral system, which potentially would increase the likelihood of observing hyperalgesia/allodynia. 16 Interestingly, 80% of our SCI subjects with allodynia (8/10) showed preserved STT function based on neurophysiological testing. However, only one of these subjects belonged to the discomplete STT group, whereas the other subjects had an incomplete STT lesion apparent from the clinical testing.
Further, whereas pain catastrophizing and depression scores were previously reported to be associated with more severe chronic pain, 56 –58 our psychological measures were not related to NP intensity and extent. This is possibly attributed to the floor effect seen in the two psychological scales. Therefore, the relationship between STT integrity and NP characteristics can be interpreted without any potential confounding of pain catastrophizing and depressive states.
Limitations
There are several limitations of this study. The small sample size hinders more sophisticated statistical analyses of the findings on STT function and its relation to NP characteristics. Also, no further questionnaires; for example, the Neuropathic Pain Symptoms Inventory (NPSI), 59,60 were performed to cover pain qualities and refine associations of STT integrity with distinct NP characteristics. Further, the electrophysiological recordings were based on a thermal stimulation only, but additional stimulation modalities (cold and mechano-nociceptive stimuli) would exhaustively assess all aspects of the STT. Further, only one body region was examined, although covering multiple sites; for example, at-level regions, might be interesting regarding zones of partial preservation or overlap with pain symptoms. Moreover, the link of STT damage to the presence and characteristics of NP was not further investigated on a more mechanistic level. For example, to assess neuronal hyperexcitability and deficient pain modulatory capacity, more elaborated test batteries, including windup and conditioned pain modulation paradigms, could further elucidate the link between STT integrity and NP.
Conclusion and Clinical Relevance
In conclusion, we provide evidence that neurophysiological readouts such as CHEPs and heat-induced SSRs provide information regarding STT integrity beyond the clinical examination of pinprick and thermal thresholds. Our findings might be of particular interest with respect to the interpretation of pinprick scores during standard neurological examination of an SCI. In SCI subjects with absent pinprick sensation, 30–50% can still be assumed to present with discomplete spinal lesion; that is, neurophysiological evidence of subclinical afferent sparing, having implications for clinical research study designs. Further, in SCI subjects with impaired/diminished pinprick sensation, residual STT function can be assumed by means of recordable SSRs in all subjects.
With regard to NP, the findings on STT integrity might have implications for the understanding of evoked NP; however, the direct relation to spontaneous NP warrants further investigations including studies targeting the mechanisms underlying chronic NP.
Footnotes
Authors' Contributions
J.R. and M.H. conceived the original idea. R.L. conducted the experiment. R.L. and M.H. performed the analysis. J.R. and A.C. supervised the findings of the work. All authors discussed the results and contributed to the final manuscript.
Funding Information
The study was supported by the Clinical Research Priority Program of the University of Zurich (CRPP Pain), the Swiss National Science Foundation (320030_169250), and the Swiss Spinal Cord Injury Cohort Study (2016-N-005, to J.R.).
Author Disclosure Statement
No competing financial interests exist.