
Abstract
Degenerative cervical myelopathy (DCM) is hallmarked by spinal canal narrowing and related cord compression and myelopathy. Cerebrospinal fluid (CSF) pressure dynamics are likely disturbed due to spinal canal stenosis. The study aimed to investigate the diagnostic value of continuous intraoperative CSF pressure monitoring during surgical decompression. This prospective single center study (NCT02170155) enrolled DCM patients who underwent surgical decompression between December 2019 and May 2021. Data from n = 17 patients were analyzed and symptom severity graded with the modified Japanese Orthopedic Score (mJOA). CSF pulsations were continuously monitored with a lumbar intrathecal catheter during surgical decompression. Mean patient age was 62 ± 9 years (range 38-73; 8 female), symptoms were mild-moderate in most patients (mean mJOA 14 ± 2, range 10-18). Measurements were well tolerated without safety concerns. In 15/16 patients (94%), CSF pulsations increased at the time of surgical decompression. In one case, responsiveness could not be evaluated for technical reasons. Unexpected CSF pulsation decrease was related to adverse events (i.e., CSF leakage). Median CSF pulsation amplitudes increased from pre-decompression (0.52 mm Hg, interquartile range [IQR] 0.71) to post-decompression (0.72 mm Hg, IQR 0.96; p = 0.001). Mean baseline CSF pressure increased with lower magnitude than pulsations, from 9.5 ± 3.5 to 10.3 ± 3.8 mm Hg (p = 0.003). Systematic relations of CSF pulsations were confined to surgical decompression, independent of arterial blood pressure (p = 0.927) or heart rate (p = 0.102). Intraoperative CSF pulsation monitoring was related to surgical decompression while in addition adverse events could be discerned. Further investigation of the clinical value of intraoperative guidance for decompression in complex DCM surgery is promising.
Introduction
Degenerative cervical myelopathy (DCM) is a disabling and painful spine disorder. 1 Despite being a common cause for neurological impairment in adults, it is generally underrecognized. 2 –5 The pathophysiology is complex and incompletely understood, but spinal cord compression, mechanical stress, and secondary ischemia and axonal degeneration are considered fundamental for its development. 6,7 Diagnosis of cervical myelopathy is based upon clinical findings and cervical magnetic resonance imaging, 8 complemented by neurophysiological examination to confirm and exclude alternate diagnoses. 9 However, pathology suggested by imaging often does not adequately reflect disease severity. Historically, cerebrospinal fluid (CSF) pressure dynamics have been assessed through Queckenstedt's test to diagnose cervical cord compression. 10 Those bedside CSF pressure assessments were also responsive to surgical decompression when done sequentially before and after surgery. 11 More recently, intraoperative CSF pressure monitoring has been investigated in acute spinal cord injury (SCI), revealing increased baseline CSF pressure during surgery. 12 In DCM, however, injury mechanisms are different, and translation from SCI is not straightforward.
Therefore, this study aims to investigate intraoperative CSF pressure dynamics in DCM, with a focus on cardiac-induced CSF pulsations, which have not been investigated to date in spinal cord compression. We hypothesized that CSF pulsations increase during surgical decompression, related to specific surgical steps. The analysis of CSF pressure dynamics during surgical decompression may help to better understand the pathophysiology of DCM and potentially contribute to the field of intraoperative monitoring in DCM.
Methods
Trial profile and main outcome measures
Details on the methodology and the study protocol were published previously.
13,14
This prospective cohort study in patients with degenerative cervical myelopathy undergoing surgical deCOMPression of the spinal CORD (COMP-CORD), was registered in

Strengthening the Reporting of Observational Studies in Epidemiology flowchart of study recruitment.
Diagnostic assessments
DCM was diagnosed in patients with at least one clinical symptom and one sign of cervical myelopathy, 17 complemented by corresponding stenosis and/or hyperintense T2-weighted signal in cervical spine magnetic resonance imaging (MRI). Each patient underwent full neurological examination and scoring of mJOA, 18 Nurick score, 19 American Spinal Injury Association Impairment Scale, 20 Spinal Cord Independence Measure (SCIM), 21 and Numerical Rating Scale for pain assessment (NRS). All but two patients received Graded Redefined Assessment of Strength, Sensation and Prehension (GRASSP). 22 Details on neurophysiological examination, imaging, and recording of surgery are provided in the Supplementary Materials.
CSF pressure monitoring
A lumbar catheter was introduced before surgery following induction of anesthesia and intubation at level L3/L4, L4/L5, or L5/1 and CSF pressure was continuously monitored. Correct placement of the catheter in the spinal canal was confirmed with CSF reflux, respiratory modulation of the signal, response to machine-assisted inspiration-hold maneuvers, and/or spontaneous CSF pulsation. To identify cardiac- induced CSF pulsations, arterial blood pressure (ABP) was obtained invasively from radial artery in all patients except two. The monitoring software, ICM+, 23 allowed online display of the raw signal and power values of cardiac-induced pulsations (i.e., those in the frequency range of ABP), which allowed to distinguish these high frequency pulsation amplitudes from low frequency respiration-associated modulations of the pressure signal (i.e., corresponding to the respiratory rate). Therefore, both peak-to-peak amplitudes and power values are reported. For technical details on the CSF pressure assessment, please refer to the study protocol (published previously). 14
Surgical procedures
Anterior cervical discectomy and fusion was performed in 11 patients. A dorsal decompression with laminectomy and in some cases additional laminotomy was performed in six cases. Further specific imaging details are provided in Table 1, including the level of maximum stenosis, number of segments affected, presence of myelopathy, site, and extent of maximum cord compression.
Clinical Characteristics of DCM Patients
Two patients are not listed: in one patient, the intraoperative data could not be analyzed at the beginning of surgery due to technical problems, in one patient catheter insertion was not possible. *in years
Sensory and grasping scores max. score 66 points.
in mm2 at max. stenosis.
Bid, bidirectional; BL, baseline; CHEPS, contact-heat evoked potentials; Compr., compression. CSF, cerebrospinal fluid; CSA, cross-sectional area; D, dorsal; FU, follow-up; L, left; mJOA, modified Japanese Orthopedic Score; N, no; NA, not available; R, right; Uni, unidirectional; V, ventral; Y, yes.
Anesthesia procedures
Total intravenous anesthesia was induced and maintained with propofol using a target-controlled infusion system. Details on anesthesia procedures are provided in the Supplementary Materials.
Statistical analysis
Data analysis was performed with MATLAB (The MathWorks, Inc., Natick, MA). For signal processing, the CSF pressure recordings were first high-pass filtered (cut-off frequency = 0.02 Hz) to discount artificial low frequency signal changes related to height adjustment of the operating table and physical impact on the pressure sensor. During this step, the mean CSF pressure was reconstructed using a moving average filter (window length = 1 min) on the unfiltered signal. Details on the CSF pressure data analysis and statistical analysis are provided in the Supplementary Materials.
Results
Demographics and clinical characteristics
Patients mean age was 62 ± 9 years (range, 38-73), and patients were mostly male (9 male; Table 1). Symptoms were mild to moderate in most patients, severe in one participant (mean mJOA 14 ± 2, range 10-18; mild: n = 8, moderate: n = 8; severe: n = 1). Mean duration of symptoms was 1 year, range between less than 6 months to 2.5 years. Most patients had sensory deficits of the upper extremities (16/17; 94%) and pathological GRASSP scores (14/15, 93%). Other symptoms were spastic ataxia (9/17; 53%), neuropathic pain (6/17; 35%), and neurogenic bladder disorder (2/17; 12%). Mean Nurick score was 1.5 ± 1 (range 0-4) and mean NRS pain in neck and/or arm area was 20 ± 20 (range, 0-40). SCIM was normal in most patients (mean 100; range 86-100). All patients were graded AIS D. Blood loss during surgery ranged between 50- 500 mL. Four patients (ID 3,7,13,18) underwent revision surgery for adjacent segment degeneration. Findings from imaging and neurophysiology are shown in Table 1 and in detail in the Supplementary Materials.
Safety
Overall, the measurements were well tolerated. None of the patients reported discomfort or pain from the catheter insertion site during or after the measurements. In one patient a toxic skin lesion developed related to residuals from disinfectants used during catheter insertion (1/17, 6%). Two patients developed post-puncture syndrome, which remitted spontaneously within days (2/17, 12%). There were no signs of local or systemic infection related to the catheter. The median depth of lumbar catheter placement from skin was 28 cm (range, 20-35 cm). Correct catheter placement was confirmed in all patients.
CSF pulsations: Responsiveness to decompression
In most patients (15/16, 94%), CSF pulsations were timely responsive to decompression (Fig. 2). In one case, pulsations were present at the beginning of surgery, but lost in the time-window of access preparation due to technical reasons (adjustments of surgery table; ID 16). In three cases (ID 4, 6, 14), CSF pulsations were lost in the time-window of decompression or post-decompression associated with adverse event with impact on CSF pulsations.

Overview of intraoperative changes in cerebrospinal fluid (CSF) pulsations in specific phases of surgery. CSF pulsations were responsive to decompression in most cases (15/16; 94%) and could be distinguished from decreased pulsations related to adverse events. Color image is available online.
From the remaining patients, who all had a persistent increase of pulsations following decompression and throughout surgery (13/17, 76.5%), median pulsation amplitudes were 0.51 mm Hg (interquartile range [IQR] 0.71 mm Hg) before, and 0.72 mm Hg (IQR 0.96 mm Hg) following decompression (p = 0.001). Individual CSF baseline pressures, pulsation amplitudes, and pulsation powers are shown in Table 2. The different relations between baseline pulsation magnitude and post-decompression values are shown for representative examples in (ID 7, 9, 12; Fig. 3).
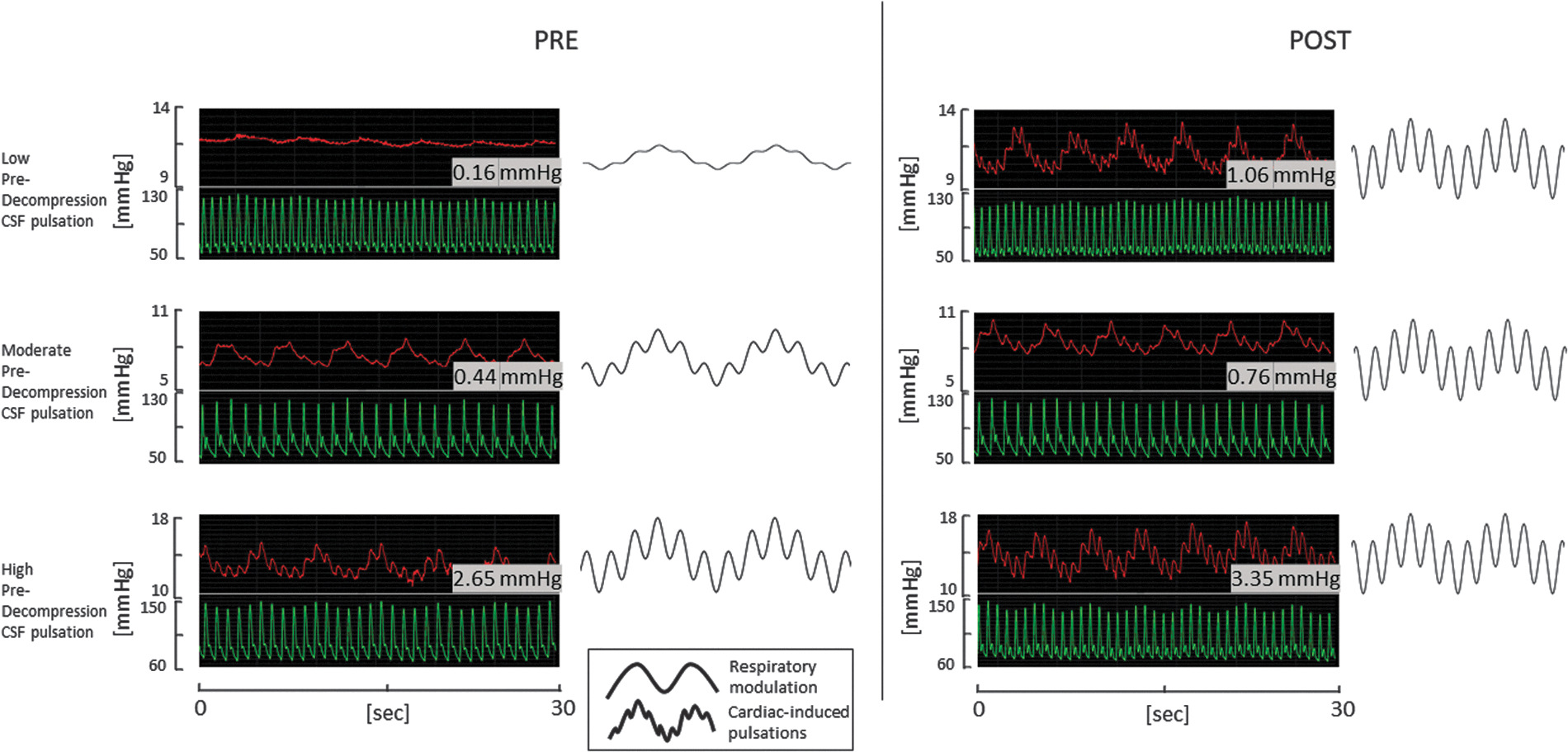
Representative cases of patients with initial almost lost (ID 9), moderate (ID 12), and high (ID 7) Cerebrospinal fluid pulsation amplitudes (red lines) at baseline, and consecutive increment post- decompression. The changes were independent of systemic blood pressure values (green lines) and effects of respiration. Color image is available online.
Median Values of CSF Pressure Parameters in the Time-Window before (Pre) and following Decompression (Post) from Lowest to Highest Pulsations before Decompression
Patients with persistently increased pulsation are listed (n = 13/17), i.e., not those without surgical adverse events and technical limitations (n = 4/17). The respective median, interquartile range for CSF baseline pressure (*BL in mm Hg), CSF pulsation amplitude (*Pulsation amplitude in mm Hg) and power (**CSF pulsation power in mm Hg 2 ) are shown for the individuals, as well as the change from pre- to post- (*delta pulsation amplitudes in mm Hg, **delta power in mm Hg 2 ).
CSF, cerebrospinal fluid; BL, baseline.
Temporal evolution of CSF pulsation during surgical decompression: Video analyses
In most patients who were responsive to decompression (n = 15), decompression-related increase of pulsations occurred gradually over several minutes (13/15; 87%), whereas in some, instantaneous changes were found (2/15;13%). Pulsation increase occurred in distinct temporal relation with the initial opening of the posterior ligament removal (ID 9, 10, 16), ongoing laminectomy and laminotomy (ID 5, 11), completion of decompression (ID 6, 8, 12, 15). Representative examples for cases with an instantaneous and gradual increases of pulsations are illustrated with ID 9 and ID 5 (Fig. 4). The surgical video was synchronized to the CSF pulsation recording in ID 9 following the initial punch of the posterior ligament of the most caudal stenotic level (Supplementary Video S1). The corresponding pre- and 6-month post-surgical MRI for this patient does not show residual stenosis (Fig. 5). Typical data showing a gradual increase during progressive removal of the posterior ligament is shown for ID 8 (Supplementary Video S2).

Intraoperative recordings of cerebrospinal fluid (CSF) pulsations in blue and arterial pressure (MAP) in red. Yellow box shows time-window of decompression and indication of CSF pressure responses. Patients could show either:
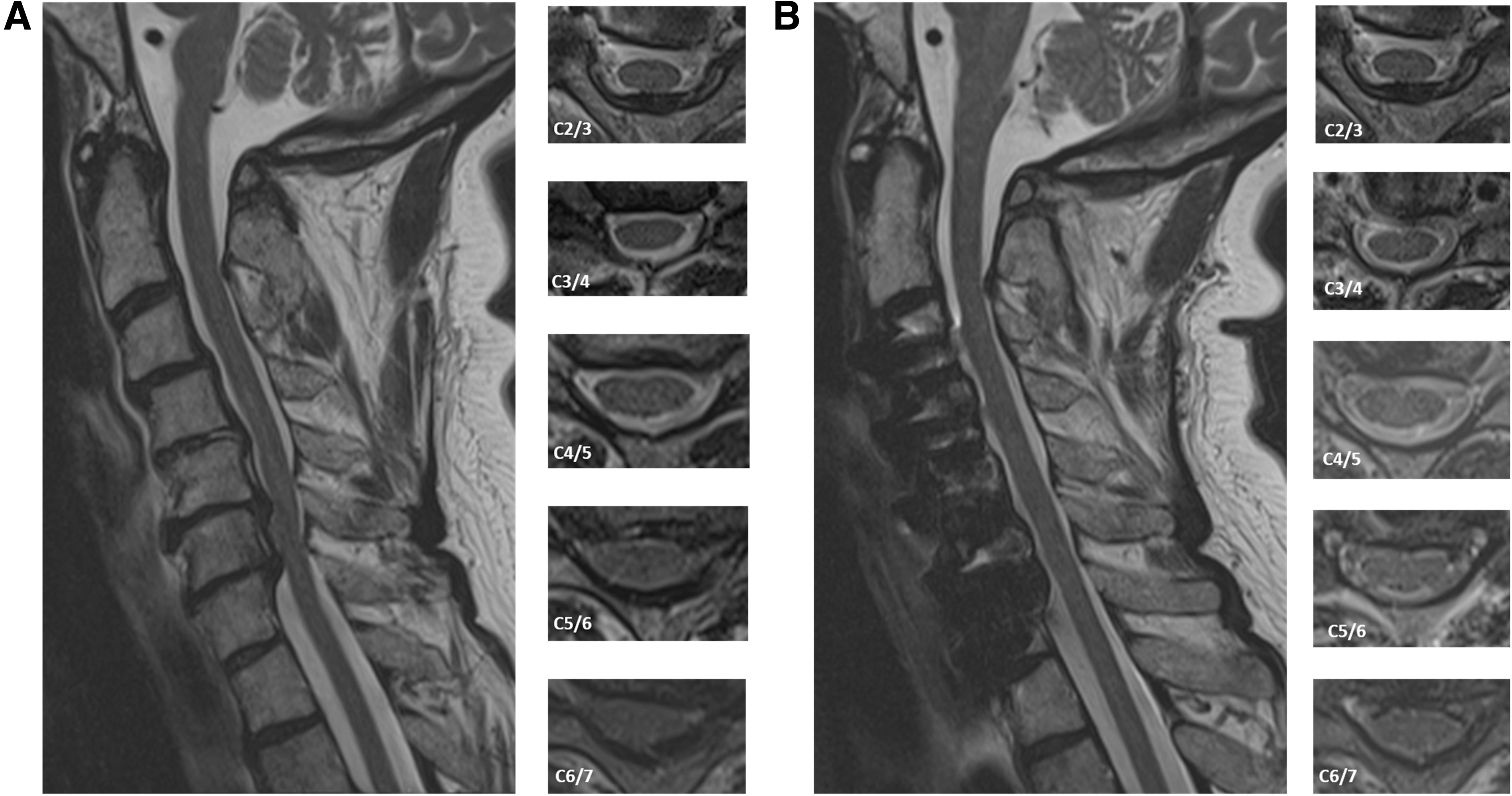
T2-weighted magnetic resonance imaging of the cervical spine of a representative degenerative cervical myelopathy patient (ID 9).
Intraoperative events and adverse events with impact on CSF pulsation
In 3/17 (18%) patients a secondary, sudden alteration of CSF pulsations occurred with almost loss of pulsation. Mean peak-to-peak amplitude severely decreased from 0.68 ± 0.36 mm Hg (range, 0.30-1.16 mm Hg) to 0.12 ± 0.10 mm Hg (range, 0.0007-0.24 mm Hg). In the time-window after decompression, this was related to CSF- leakage (ID 16), that was detected by the surgeon during surgery. In one case (ID 6), a decrease was observed in the time-window post-decompression, related to cage insertion. In ID 4, there was no video recording available, but upon surgeon judgement, a CSF leakage was the most likely cause for the loss of pulsation. Note that none of the patients had clinical sequelae associated with these events.
Potential confounders of CSF pulsations: Cardiocirculatory parameters and baseline CSF pressure
In patients with increased CSF pulsations, there were no differences in mean arterial pressure (MAP) before decompression (mean 79 ± 6 mm Hg; range 72-91 mm Hg) and post-decompression (79 ± 8 mm Hg; range 65-95 mm Hg; p = 0.927). Similarly, there were no changes in heart rate (HR) from pre- (mean 67 ± 12/min; range 43-90/min) to post-decompression (mean 70 ± 12/min; range 53-90/min; p = 0.102).
From patients with a persistent increase of pulsations throughout surgery, the mean CSF baseline pressure was 9.5 ± 3.5 mm Hg before (range 4.8- 15.7 mm Hg), and 10.3 ± 3.8 mm Hg (range 5.2- 17.4 mm Hg) following decompression (p = 0.003). Pulsation amplitudes increased unrelated to changes in baseline CSF pressure and MAP as shown in representative patient ID 11 and 15 (Fig. 6).
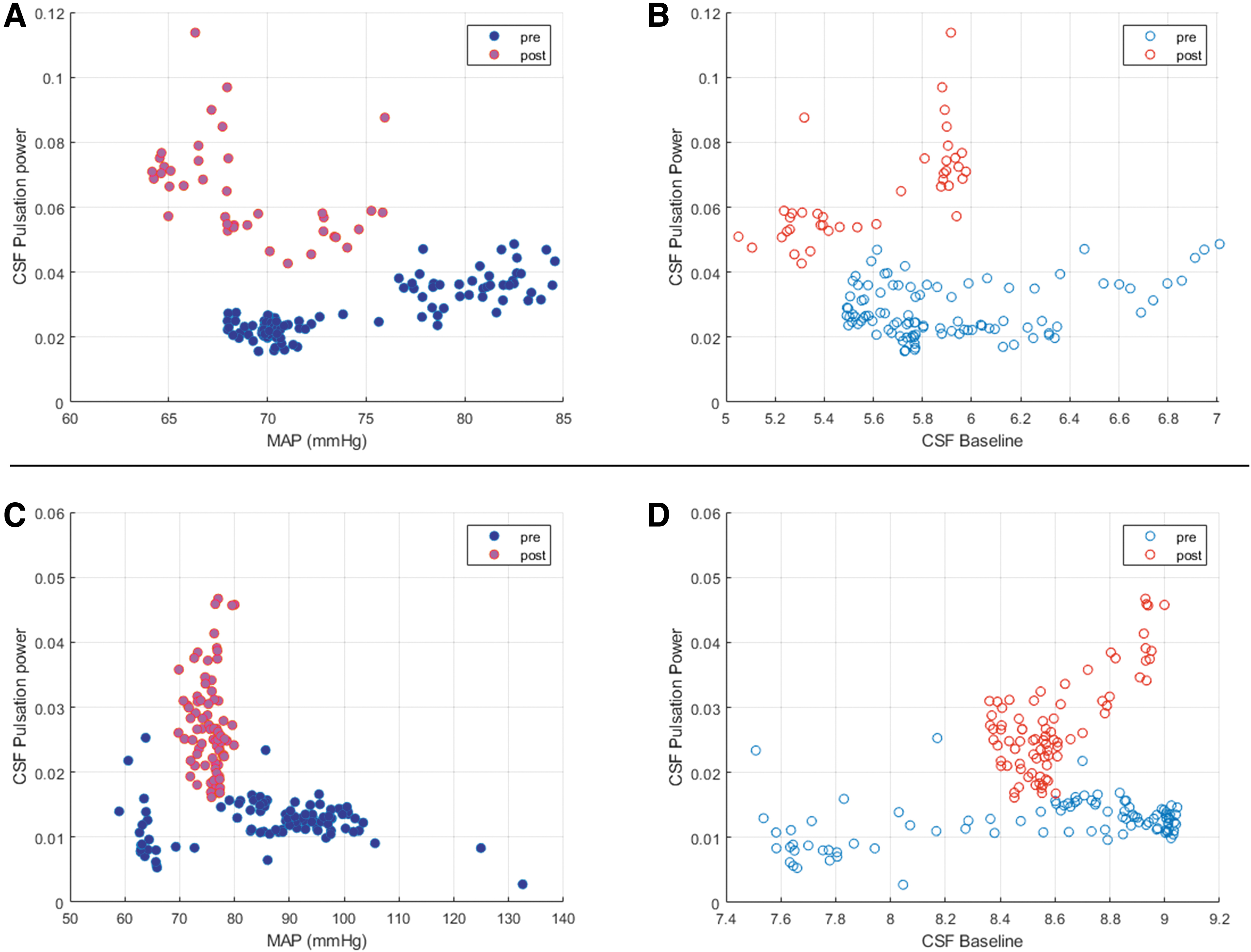
Intraoperative monitoring of cardiac-related cerebrospinal fluid (CSF) pulsations. Data from two representative patients (top ID 11, bottom ID 15) illustrating increases of pulsation power pre- to post- surgical decompression (y-axis; in mm Hg
2
), as they relate to changes to mean arterial pressure (MAP; x-axis;
The correlation between MAP and CSF pulsation was 0.38 before (p < 0.001), and 0.16 following decompression (p < 0.001). The correlation of HR to CSF pulsations was -0.08 before (p < 0.001), and -0.07 following decompression (p < 0.001).
Preliminary clinical follow-up evaluation
Six-month follow-up (completed in 14 out of 17 subjects) showed significant improvement for mJOA, from pre-operative mean of 15 ± 2 to 16 ± 1 post-operative score (p = 0.048). Changes in Nurick score were slightly below the threshold for statistical significance (p = 0.055), remaining on average 1 ± 1 before and after surgery (p = 0.055). In patients without intraoperative events that negatively affected CSF pulsations, we did not find a significant correlation between the magnitude of pulsation changes and post-operative mJOA changes (p = 0.538). Patients with immediate CSF pulsation increase (ID 5 and 9) did not fare better than those with gradual responses. Both patients that revealed immediate changes had in common that bidirectional, multi-segmental stenosis was present.
Discussion
Summary of main findings
To our knowledge, this was the first study that evaluated the dynamics of intraoperative CSF pulsations in decompressive surgery of DCM. The intraoperative evolution of CSF pulsations suggests that CSF dynamics were severely affected in cases with spinal cord compression and increased at the point of surgical decompression. All changes were observed during decompression, highlighting the potential of infra-stenotic CSF pressure monitoring. A potential interference of MAP, HR, and baseline CSF pressure with recovery of CSF pulsations from pre- to post-decompression could be ruled out.
Bedside investigations of CSF pressure dynamics in spinal cord compression
Under normal conditions, the intracranial and spinal CSF compartments are considered a communicating fluid space. In the presence of spinal canal stenosis, the communication is compromised. 24,25 Thirty years ago, a study investigated Queckenstedt's test (QT) in 85 patients with DCM before and after decompressive surgery and found that responses recovered following surgical decompression. 26 QT is performed by firm manual pressure on both jugular veins during lumbar puncture and parallel measurement of CSF pressure at lumbar level. Our findings extend these observations to the intraoperative setting with detailed intraoperative analysis of CSF pressure dynamics and real time feedback illustrating the potential of the method to allow for timely surgical adjustments as needed (e.g., in complex or multi-level stenosis).
Intraoperative CSF and intraspinal pressure monitoring in spinal cord compression: Comparison of monitoring data and safety
More recently, one study investigated CSF pressure in 22 patients with acute SCI during decompression and focused on opening CSF pressure as primary outcome. 12 The authors described an increase of baseline pressure following decompression, with initially higher baseline CSF pressure than in this DCM cohort (13.8 ± 1.3 mm Hg vs. 9.5 ± 3.5 mm Hg). The increase of baseline pressure reported for SCI—it nearly doubled—was much larger than in our cohort, pointing to the differences of the pathophysiology between DCM and SCI. In acute SCI, sudden swelling and edema of the spinal cord, as well as hematoma may contribute to per-acute conditions with completely blocked CSF space at the injury site within the spinal canal, 27 while in DCM cord compression develops over months or years, with ligamentous, discal, and osseous alterations as the predominant mechanism of cord compression with remaining CSF space in most patients. 28 We suppose that in DCM monitoring of pulsations is particularly useful, because baseline CSF pressure changes were not as striking as in acute SCI. There is one other study that monitored CSF pulsations in 13 patients with acute SCI in the time-window after surgical decompression. 29 At that stage, CSF was non-pulsatile in 21% of the time. Again, compared with our cohort, from which all patients had pulsatile CSF, except for those with specific intraoperative (adverse) events, the pulsation abnormalities in acute SCI were more pronounced than in DCM.
CSF pressure monitoring and intraoperative ultrasound
Intraoperative ultrasound (IOUS) has been proposed as a tool to detect cord compression in DCM patients undergoing dorsal surgery. 30,31 Our findings are in line with the observation that cord pulsation was impeded in the presence of stenosis and returned following decompression. CSF pressure monitoring has the potential advantage that it would be feasible in both anterior and posterior decompression, while being more invasive than IOUS. To determine the common ground of IOUS and CSF pressure readouts, parallel assessment can be helpful.
CSF pressure–clinical outcome interrelation
Most patients who underwent 6-month follow-up showed significant improvement of mJOA. Therefore, we assume to have achieved successful decompression in the majority of patients. The absence of a correlation between preliminary outcomes and intraoperative pressure changes indicates that decompression is only one out of multiple factors contributing to recovery trajectories. However, in those who remained clinically stable, recovery may still be evident at later stages (e.g., within 12 months of follow-up), as recently shown in a sizable cohort of DCM patients. 17 Further, it is common observation that patients with mild symptoms experience smaller increments than patients with severe impairment, 32 which demands for more specific outcome measures than mJOA. 33 With regards to imaging, despite successful decompression, those patients with established myelopathy (i.e., multiple level of hyperintensity in T2- weighted MRI), may have worse outcomes than those without. 34 In conclusion, more follow-up data and possibly larger sample size is required to perform a meaningful subgroup analysis.
Safety considerations
With regard to safety, in our study, the measurements were well tolerated overall, none of the patients complained of pain at the insertion site, post-puncture headache was in the expected range 35 and vanished timely. As we observed a skin lesion due to disinfectant agents, we recommend careful search for remnants in patients positioned on their back for surgery to prevent this preventable adverse event in patients undergoing CSF pressure monitoring.
Pathophysiological underpinnings of CSF pulsations and cardiocirculatory interplay
The mechanisms behind cardiac-induced CSF pulsations are complex and incompletely understood. Our results support the notion of an intracranial origin of pulse generation, 36,37 since pulsation was weak to absent in the presence of cord compression and sensitive to decompression, which could not be explained unless pulsations were mainly translated through the spinal canal and across the level of stenosis. Due to this interplay between the arterial and CSF compartment, 38 changes in MAP or HR could potentially confound CSF pulsations. However, within the blood pressure ranges recorded here (i.e., within the limits of autoregulation, typically controlled and maintained during spine surgery), any relevant systematic confounding of the CSF pulsation transduced by cardiocirculatory dynamics could be minimized. Further potential confounders need to be systematically investigated, for instance carbon dioxide levels. 39
Clinical implications
This study represents the proof of concept that intraoperative monitoring of CSF pulsation may detect immediate decompression-related changes in DCM. To date, neuromonitoring with motor evoked potential and somatosensory evoked potential is an established tool to detect intraoperative neurological injury during spine surgery and improves surgical outcomes. 40 Beyond the concept of prevention of damage, monitoring of CSF pulsations can potentially provide guidance in revealing and quantifying effects of surgical spinal cord decompression. Of note, this study aligns with two of the top 10 research priorities for DCM, identified by AO Spine RECODE DCM (REsearch Objectives and Common Data Elements for Degenerative Cervical Myelopathy): assessment and monitoring, and pathophysiology. 41
Limitations
This study primarily aims at proving safety, feasibility, and proof-of-concept of CSF pressure monitoring in DCM. As known from larger DCM cohort studies, this condition is usually highly heterogenous in terms of disease mechanisms and severity. 17 Our cohort was representative for mild- moderate DCM and most commonly multilevel stenosis was present. For patients with more severe symptoms and single level stenosis these findings should be viewed with caution. Also, patients with tandem stenosis, which represent a sizeable proportion of patients with DCM, 42 were not included in this sample. With respect to the radiological findings, subgroup analyses would be needed to predict specific CSF pressure signatures of soft tissue versus calcified stenosis.
Conclusion
Intraoperative monitoring of CSF pressure dynamics is safe and feasible in DCM, and temporally related changes of CSF pulsations indicate responsiveness to surgical decompression. While sensitivity and specificity are high, there is further need to elaborate on targeted levels of CSF pulsations and concepts in complex surgical procedures. These results represent the first proof-of-principle that cord decompression is accompanied by quantifiable changes in CSF pressure values, suggesting value of this method for intraoperative monitoring. Further studies are needed to investigate the diagnostic utility.
Footnotes
Acknowledgments
The authors would like to thank all patients for participation in this study. Also, we would like to thank the support of Mrs. Regula Schüpbach, Mrs. Romana Pfiffner, Mrs. Fabienne Grob, Mr. Martin Egloff, Mr. Christian Streng, Mr. Matthias Noll, the team of OR/ICU nurses and the attendants for surgical positioning.
Authors' Contributions
CZ, AC, MS: conception and design of the study, acquisition and analysis of data, drafting a significant proportion of the manuscript or figures. NP, NK, AB, JA, NU: acquisition and analysis of data, drafting a significant proportion of manuscript or figures. JS, AA, MB, FW, MH, VK, MF: acquisition and analysis of data.
Funding Information
No conflicts of interest resulted from the funding sources.
Author Disclosure Statement
CZ, AC, MS report a grant from the Swiss Paraplegia Foundation (Foko_2019_01); CZ, MS, MF, MH report a grant from the Balgrist Foundation. VK reports a grant from the Swiss National Science Foundation (Project Nr. 182683).
Supplementary Material
Supplementary Materials
Supplementary Video S1
Supplementary Video S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.