
Abstract
High quality evidence shows decompressive craniectomy (DC) following traumatic brain injury (TBI) may improve survival but increase the number of severely disabled survivors. Contemporary international practice is unknown. We sought to describe international use of DC, and the alignment with evidence and clinical practice guidelines, by analyzing the harmonized Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) and Australia-Europe NeuroTrauma Effectiveness Research in Traumatic Brain Injury (OzENTER-TBI) core study datasets, which include patients admitted to intensive care units (ICUs) in Europe, the United Kingdom, and Australia between 2015 and 2017. Outcomes of interest were treatment with DC relative to clinical trial evidence and the Brain Trauma Foundation guidelines. Of 2336 people admitted to ICUs following TBI, DC was performed in 320 (13.7%): in 64/1422 (4.5%) patients with diffuse TBI and 195/640 (30.5%) patients with traumatic mass lesions. Secondary DC (for treatment of intracranial hypertension) was used infrequently in patients who met enrollment criteria of the two randomized clinical trials informing the guidelines—specifically, in 11/124 (8.9%) of those matching Decompressive Craniectomy in Diffuse Traumatic Brain Injury trial (DECRA) enrollment, and in 30/224 (13.4%) of those matching Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intracranial Pressure (RESCUEicp). Of patients who underwent DC, 258/320 (80.6%) were ineligible for either trial: 149/320 (46.6%) underwent primary DC, 62/320 (19.4%) were outside the trials’ age criteria, and 126/320 (39.4%) did not develop intracranial hypertension refractory to non-operative therapies prior to DC. Secondary DC was used infrequently in patients in whom it had been shown to increase survival with severe disability, indicating alignment between contemporaneous evidence and practice. However, most patients who underwent DC were ineligible for the key trials; whether they benefited from DC remains unknown.
Introduction
Traumatic brain injury (TBI) is a global health problem: the worldwide annual incidence is 69 million, of whom 5.48 million suffer severe TBI. 1,2 Outcomes following severe TBI remain poor: a minority of patients survive to live independently or return to work, while over 50% die or suffer long-term severe disability. 3
Three randomized trials have compared decompressive craniectomy (DC) to medical management in the treatment of intracranial hypertension following TBI; of these, two were in adults and of high methodological quality. 4 -6 The Decompressive Craniectomy in Diffuse Traumatic Brain Injury trial (DECRA) and Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intracranial Pressure (RESCUEicp) trials showed DC reduces intracranial pressure (ICP) but may increase the number of survivors with severe disabilities. 5,6 These trials provide the highest level of evidence available to guide surgical management of patients with TBI and underpin the Brain Trauma Foundation (BTF) guidelines. 7
Contemporary international use of DC in relation to evidence is unknown. In all disciplines, including neurotrauma and critical care, evidence frequently fails to translate into practice and worse outcomes may result. 8,9 Further, results of these trials may be over-generalized to inapplicable circumstances, and significant knowledge gaps may remain in the use of DC. 10,11
The Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI) and Australia-Europe NeuroTrauma Effectiveness Research in TBI (OzENTER-TBI) studies include granular data on management of patients with TBI in Europe, the United Kingdom (UK), and Australia, and offer a unique opportunity to examine use of DC. 12,13 We hypothesized that use of DC following TBI may vary between regions, and that evidence and practice may not be aligned.
Methods
Study design
This cohort study used prospectively collected data from hospitals providing neurosurgical services that participated in the harmonized, longitudinal CENTER-TBI and OzENTER-TBI studies (
The CENTER-TBI Core study was conducted in 54 hospitals in 19 countries in Europe (including the U.K.) and Israel between 2015 and 2017. OzENTER-TBI was conducted in the two designated adult major trauma centers in Victoria, Australia, between February 2015 to March 2017. More detail about the CENTER-TBI Core Study can be found in the study protocol and publication of the main results. 13,15 Patients of any age were included if they underwent a brain computed tomography (CT) for a clinical diagnosis of TBI and were admitted to intensive care (ICU) within 24 h of injury. Patients were excluded if they had a pre-existing neurological disorder potentially confounding outcome assessment.
Human research ethics approvals were granted by ethics committees of all individual participating hospitals, and additionally of Monash University for OzENTER. Informed consent by patients and/or their legal representative was obtained for all patients according to local legislative requirements.
This report adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement and guidelines. 16
Data collection
De-identified clinical data were collected by hospital research personnel using web-based electronic case report forms (QuesGen Systems Incorporated, Burlingame, CA), then stored on a secure database hosted by the International Neuroinformatics Coordinating Facility in Stockholm, Sweden. Data were accessed using Neurobot data management software (RRID: SCR_01700).
Encoded rules were used to check data at time of entry; any subsequent queries were referred to centers. Where data were missing no assumptions have been made and results are presented as percentages of available data, expressed as n/N (%).
Data extracted included demographics, injury mechanisms, injury severity scores, pre-hospital secondary insults (hypoxia and hypotension), pre-hospital Glasgow Coma Scale (GCS) scores, emergency and ICU therapies, including details of any DC and reported indications. Initial CT appearances were characterized for Marshall classification by central investigator review. 17 Scans were unavailable if performed prior to transfer to participating neurosurgical center, or if upload quality prohibited central interpretation. Admission clinical and CT data were used to estimate risk of poor functional outcome (defined as Extended Glasgow Outcome Score [GOSE] <5) using the International Mission for Prognosis and Analysis of Clinical Trials in TBI (IMPACT) CT model. 18 Non-operative therapies for intracranial hypertension were noted including high dose sedation, osmotherapies (hypertonic saline and mannitol), muscle relaxants, therapeutic hypocapnia or hypothermia, or cerebrospinal fluid drainage. Lengths of stay and hospital outcomes were obtained from hospital records, and 6-month GOSE by interview or postal questionnaires with patients or carers. In Australia, these were collected by the Victorian State Trauma Registry, a population-based registry that follows up all major trauma patients.
The principal variable of interest was the proportion of patients who underwent DC during initial ICU stay. Authors DG, EW, and TvE categorized DC as primary when performed with traumatic lesion evacuation, or secondary when performed for intracranial hypertension with an ICP monitor already in situ (as was tested in DECRA and RESCUEicp). To examine alignment of practice with evidence, patients were grouped by conformity with the trials’ eligibility criteria (Supplementary Content Table S1 and Fig. S1A and S1B). Participants in DECRA were those with severe TBI (GCS 3-8), diffuse brain injury (defined by Marshall CT classification I-IV vs. evacuable traumatic mass lesion[s] defined by Marshall V-VI), and intracranial hypertension (ICP >20 mm Hg) refractory to non-operative therapies within 72 h of injury. RESCUEicp included patients with diffuse injuries or traumatic mass lesions with intracranial hypertension (ICP >25 mm Hg) refractory to non-operative therapies at any time during initial ICU stay. The proportion of patients matching trial eligibility who underwent secondary DC was calculated. To determine if practice changed following publication of RESCUEicp in September 2016, the proportions who underwent secondary DC were compared according to whether they were injured before or after January 1, 2017 (to allow for dissemination of results).
Statistical analysis
Categorical data are presented as numbers (%); continuous data are presented as mean ± standard deviation (SD) for normally distributed data, and as median interquartile range (IQR) for skewed data. Proportions between groups were compared using chi-squared and Fisher's exact tests. Multi-variable logistic regression analysis was performed to identify patient or site characteristics associated with secondary DC performed for intracranial hypertension. Variables considered for model inclusion were age, GCS, Marshall classification, and region; age was included as a continuous variable.
Statistical analyses were performed using Stata version 16.0 (StataCorp LLC, TX). A p value of <0.05 was considered statistically significant. No adjustments were made for multiple comparisons.
Results
In total, 2336 patients were admitted to ICUs following TBI: 1867 in Europe, 271 in the U.K., and 198 in Australia (Table 1). Of these, 1068 (45.7%) had severe TBI (Supplementary Content Table S2).
Characteristics of Patients Admitted to Intensive Care with Traumatic Brain Injury
Variables for the International Mission for Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (IMPACT) CT model were available for 1740 (74.5%) patients
Data are n/N (%) or median (interquartile range), unless otherwise indicated.
GCS, Glasgow Coma Scale; CT, computed tomography; GOSE, Extended Glasgow Outcome Score; SD, standard deviation.
Patient characteristics
Median age of all patients was 49 (29-66), and 1711/2336 (73.2%) were men. One-third were at least 60 years old. Causes of head injuries and severity varied between regions: initial GCS scores were lower in the U.K. (6; 3-11) than in Australia (8; 3-12) or Europe (10; 4-14). Marshall CT classifications were available for 2062/2336 (88.3%) patients. Overall, two-thirds of patients had diffuse radiological injury (1422/2062 [69.0%]) but a disproportionate number had traumatic intracranial lesions in the U.K. (81/210 [38.6%]), compared with Europe (506/1674 [30.2%]) and Australia (53/178 [29.8%]). Characteristics of patients who underwent DC are available in Supplementary Content Table S3.
Care processes including ICP therapies and hospital outcomes are shown in Supplementary Content Table S4. Fewer patients received ICP monitors in Europe (748/1842 [40.6%]) than in the U.K. (173/271 [63.8%] or Australia (117/198 [59.1%]). Intracranial hypertension was treated with metabolic suppression with barbiturates or therapeutic hypothermia in 591/2336 (25.3%) patients. At 6 months, 900/2022 (44.5%) had died or had severe disability (GOSE 1-4); 1122/2022 (55.5%) had favorable recovery (GOSE 5-8; Supplementary Content Fig. S2). Most patients with outcome data missing were from European sites and were equivalent in baseline characteristics.
Use of decompressive craniectomy
Use of DC is shown in Figure 1 by region, radiological appearance, and use of primary or secondary DC. Patients with traumatic mass lesions underwent DC more frequently than with diffuse injury (195/640 [30.5%] compared with 64/1422 [4.5%]). Frequency of DC was highest in the U.K. both for patients with diffuse TBI (9/129 [7.0%]) and with mass lesions (40/81 [49.4%]); this aligned with greater severity of injury in U.K. patients compared with other regions (Tables 1 and 2). A unilateral fronto-temporal approach was most common (241/320 [75.3%]), performed in 156/195 (80.0%) patients with mass lesions and 44/64 (68.8%) with diffuse injury. Fewer patients underwent bifrontal DC (35/320 [10.9%]): 11/195 (5.6%) of those with intracranial mass lesions and 13/64 (20.3%) of those with diffuse TBI. Few patients underwent posterior fossa craniectomy.
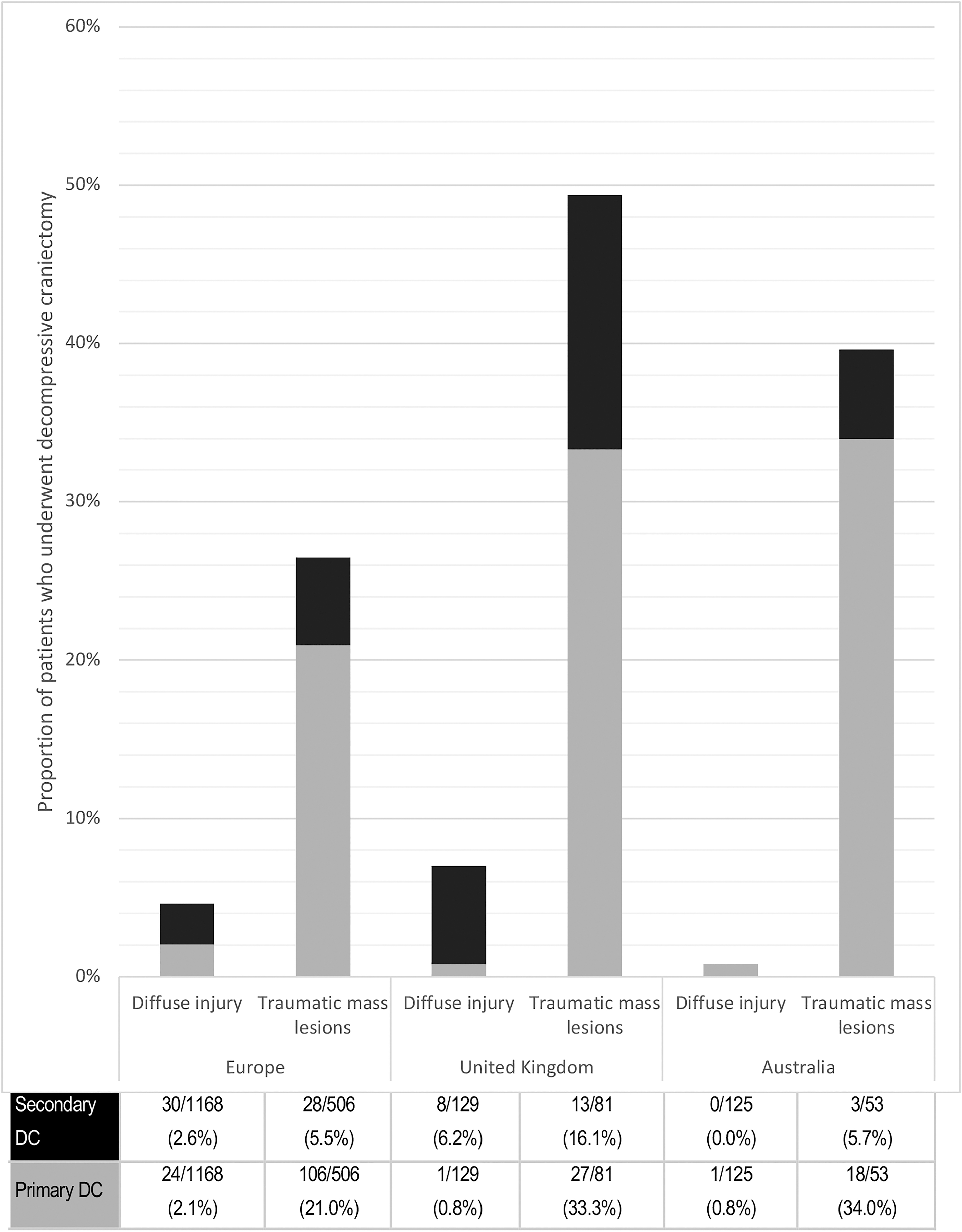
Proportions of patients who underwent decompressive craniectomy by region and radiological appearance. Radiological Marshall CT (computed tomography) appearances were available for 259/320 (80.9%).
Features of Decompressive Craniectomies According to Radiological Appearance *
Marshall CT classifications were available for 2062 (88.3%) patients.
Data are n/N (%) or median (interquartile range), unless otherwise indicated.
CT, computed tomography; ICP, intracranial pressure, DC, decompressive craniectomy.
Details of secondary DC use are shown in Supplementary Content Table S5. Proportions of patients who underwent secondary DC varied between regions and by radiological appearance; no patients with diffuse TBI in Australian sites underwent secondary DC. Most patients received at least some medical therapies prior to surgery, and their use did not differ between regions.
Following adjustment for pre-specified variables, the odds of undergoing secondary DC were lower in older patients (odds ratio (OR) 0.97, 95% confidence interval [CI] 0.96-0.98, p < 0.001), in those with less severe TBI based on higher initial GCS (OR 0.90, 95% CI 0.85-0.95, p < 0.001), and in those with diffuse injury (OR 0.31, 95% CI 0.19-0.51, p < 0.001; Table 3). Odds of undergoing secondary DC were higher in patients treated in the U.K. (OR 2.14, 95% CI 1.21-3.78, p = 0.009).
Multi-Variable Model Investigating Variables Associated with Secondary Decompressive Craniectomy (Compared with Other Indications or No Craniectomy)
OR, odds ratio; GCS, Glasgow Coma Scale.
Alignment with key randomized trial evidence
The proportions of patients who matched enrollment criteria was low for both DECRA (124/2336 [5.3%]) and RESCUEicp (224/2336 [9.6%]; Table 4). Eleven of 124 (8.9%) DECRA-eligible patients underwent secondary DC: 9/95 (9.5%) in Europe, 2/23 (8.7%) in the U.K., and none in Australia (0/6). Thirty of 224 (13.4%) RESCUEicp-eligible patients underwent secondary DC: 21/154 (13.6%) in Europe, 9/66 (13.6%) in the U.K., and none in Australia (0/4).
Use of Secondary Decompressive Craniectomy among Patients Matching Trial Eligibility Criteria
DECRA eligibility: aged 15-59, GCS 3-8, diffuse traumatic brain injury (TBI), admitted to intensive care unit, intracranial pressure (ICP) monitor in situ, ICP >20 within first 72 h following injury refractory to medical therapies (excluding barbiturates).
Rescue ICP methods eligibility: aged 10-65, TBI with abnormal CTB, ICP >25 despite medical therapies (excluding barbiturates)
Data are n/N (%)
DECRA; Decompressive Craniectomy in Diffuse Traumatic Brain Injury trial; DC, decompressive craniectomy; RESCUEicp, Randomised Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intracranial Pressure.
Of patients who underwent DC only 15/320 (4.7%) would have been eligible for DECRA and 60/320 (18.8%) would have been eligible for RESCUEicp (Fig. 2). The majority (258/320 [80.6%]) were ineligible for either trial for at least one reason: 149/320 (46.6%) had undergone primary DC, 62/320 (19.4%) were outside the trials’ age criteria, and 126/320 (39.4%) did not develop intracranial hypertension refractory to medical therapies.

Eligibility of patients among those who underwent decompressive craniectomy. *258/320 (80.6%) patients differed from the trials’ populations, for the following reasons: 149/320 (46.5%) underwent primary decompressive craniectomy; 62/320 (19.4%) were outside the trials’ age criteria; 126/320 (39.4%) did not have intracranial hypertension refractory to medical therapies.
Following RESCUEicp publication the proportion of patients matching eligibility for this trial who underwent DC was not significantly different: 47/176 (26.7%) before versus 13/48 (27.1%) after publication (p = 0.506; Supplementary Content Table S6).
Discussion
Key findings
In these harmonized, multi-center cohort studies conducted in Europe, the U.K., and Australia, one in seven patients admitted to ICU following TBI underwent decompressive craniectomy. Severity of injury of admitted patients and surgical management varied between regions. Patients with diffuse TBI were less likely to undergo DC than those with traumatic mass lesions, consistent with implementation of contemporaneous evidence and clinical practice guidelines. However, most patients who underwent DC differed from key trial populations. Decompressive craniectomy in such circumstances may be clinically appropriate but is not yet informed by high quality evidence.
Relationship to previous studies
Patient characteristics and practice variation
Availability of neurosurgical services and treatment of TBI varies globally, particularly in low- and middle-income countries. 19 We previously found that even within high income countries there were differences in characteristics of patients admitted to ICU following TBI, 20,21 and now show variation in selection of patients for DC and time to surgery. Patients admitted to ICUs in the U.K. were younger and more severely injured, which may reflect lesser availability of ICU beds, 22 and may explain why U.K. patients were more likely to undergo secondary DC (noting this can shorten ICU stay). 5
Patient characteristics and alignment with underlying evidence
Our participants represent a broad spectrum of patients with serious TBI; demographics, mechanisms of injury, and injury characteristics were similar to those of other international cohorts. 23 -25 Among those patients matching DECRA eligibility (in whom DC may increase survival with severe disability), we observed infrequent use of secondary DC, in keeping with contemporary evidence and guidelines.
However, most patients in our study had injury characteristics that would have excluded them from both DECRA and RESCUEicp. This finding is consistent with the trials’ recruitment experience wherein few screened patients with TBI were eligible for enrollment, and with a smaller registry study in Canada in which few patients who underwent DC satisfied DECRA or RESCUEicp criteria. 26
Extrapolated use of decompressive craniectomy
Median ages and TBI severities of our patients were comparable to those of DECRA and RESCUEicp; however, our data suggest DC is mostly undertaken in circumstances where this evidence is not applicable. Among our patients, a large proportion underwent primary DC or underwent secondary DC prior to exhausting non-operative therapies; others were outside trial age cut-offs. It is possible there was sound clinical rationale for surgery in these patients, and recent pragmatic consensus guidelines allow for clinician discretion. 11 But such applications are outside the scope of available evidence or the evidence-based BTF guidelines, which refer to use of DC only for refractory intracranial hypertension. 7,27 Robust comparative research is needed to examine DC as it is currently being used; for example, primary DC in the context of evacuation of subdural hemorrhage (as in the forthcoming RESCUE-ASDH trial), 28 and by including older patients.
Change in practice in response to evidence
Based on DECRA findings, the 2016 BTF guidelines recommended against secondary DC in patients with diffuse TBI. 27 Our finding that few DECRA-eligible patients (and only 2.7% of all with diffuse injury) underwent secondary DC suggests the findings were implemented and international practice was consistent with this iteration of the guidelines, particularly in Australia.
Historical data suggest use of DC was increasing prior to DECRA publication in 2011, and has since decreased. Between 1995-2005, several non-randomized studies supported its use. 29,30 Between 1999 to 2004 in the U.S. and Italy, DC for refractory intracranial hypertension was performed in 4.1-4.4% of patients, 31,32 and between 2004-2008 in 8.2% of patients in Australia. 33 Following DECRA, secondary DC was used in just 2.3% of patients with severe TBI in Australian centers. 17
The RESCUEicp findings (published in 2016, within our study period) have been interpreted to support use of “late” secondary DC in a 2020 update of BTF guidelines. 7 Delays between trials and guidelines make examination of their individual impact on clinical practice difficult. We observed secondary DC was used sparingly even among patients meeting RESCUEicp inclusion criteria and there was no immediately discernible change in practice following trial publication. In contrast, a recent survey of European neurotrauma centers found 47% of neurocritical care staff considered craniectomy “general policy” for treatment of refractory intracranial hypertension. 34 Ongoing detailed data collection may enable analyses of implementation that consider effects of emergent trial findings and guidelines. 35
Strengths and limitations
Strengths of this study are that it uses harmonized datasets from the largest collaborative TBI cohort studies conducted to date. It includes all patients with TBI admitted to ICUs at participating centers and had available granular clinical, radiological, and management data, which were essential to identify subgroups of patients to whom evidence was applicable.
The study also has some weaknesses. Some relevant data are missing, particularly CT appearances and reported indications for surgery. Some potential confounders were not recorded, including frailty scores, advanced care directives, and timing of withdrawal of life-sustaining treatments. These can impact decisions regarding procedures that may generate disabled survivors. Our definition of secondary DC may have captured cases where DC was performed for indications other than intracranial hypertension. Due to a lack of granular data for earlier time periods, reliable conclusions cannot be drawn regarding changes in practice; the effects of evidence and guidelines would be more distinguishable by interrupted time series analyses. Finally, participating hospitals were self-selecting neurotrauma referral centers; implementation may differ in non-specialized hospitals, and observed regional differences may be due to health system, population, and hospital factors, as well as clinician decision making.
Conclusions
In Europe, the U.K., and Australia, DC following TBI remains in use, predominantly in patients with traumatic mass lesions. Use of secondary DC in patients with diffuse injury is in keeping with available evidence. However, practice is predominantly outside the scope of the available evidence base, in that most patients who undergo DC would not satisfy enrollment criteria for the key trials, leaving clinicians without high quality evidence to guide surgical decisions. Additional clinical trials and pragmatic comparative effectiveness studies are needed to evaluate decompressive craniectomy following TBI in the circumstances in which it is currently used.
Footnotes
Acknowledgments
The authors would like to thank all patients for their participation in the CENTER-TBI and OzENTER-TBI studies, along with all investigators and researchers for ICU data collection and for sharing their valuable expertise. Finally, we would like to thank the International Initiative for Traumatic Brain Injury Research funders and investigators for the collaboration and support.
Authors' Contributions
All authors certify that they participated in the concept, study design, analyses, interpretation, writing, and revision of the manuscript. DG, PB, AIRM, SF, and DJC prepared the draft manuscript and coordinated production of the final version. EW and DG did the data extraction with supervision by TvE, and AIRM. DG, and EW performed statistical analyses and drafting of tables and figures. All authors reviewed the manuscript for important intellectual content and approved the submission of the final manuscript.
Funding Information
This research was funded by the European Commission 7th Framework program (602150), the Australian National Health and Medical Research Council (NHMRC 1074181) and the Victorian Transport Accident Commission (ISCRR N-14- 129). Additional support for CENTER-TBI was provided by the Hannelore Kohl Stuftung (Germany), OneMind (USA), Integra LifeSciences Corporation (USA) and NeuroTrauma Sciences (USA). The funders had no role in the collection, analysis, and interpretation of data, nor in the writing of the report or in publication decisions. The authors had full access to study data and the senior authors had final responsibility for the decision to publish.
Author Disclosure Statement
AIRM declares consulting fees from PresSura Neuro, Integra Life Sciences, and NeuroTrauma Sciences. DJC is an Australian NHMRC Practitioner Fellow and reports grants from the NHMRC and consulting fees to Monash University from PresSura Neuro; additionally, he is the Chief Investigator for the DECRA trial.
For the other authors, no competing financial interests exist.
Supplementary Material
CENTER-TBI Investigators and Participants
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.