
Abstract
Moderate traumatic brain injury (mTBI) is a heterogeneous entity that is poorly defined in the literature. Patients with mTBI have a high rate of neurological deterioration (ND), which is usually accompanied by poor prognosis and no definitive methods to predict. The purpose of this study is to develop and validate a prediction model that estimates the ND risk in patients with mTBI using data collected on admission. Data for 479 patients with mTBI collected retrospectively in our department were analyzed by logistic regression models. Bivariable logistic regression identified variables with a p < 0.05. Multi-variable logistic regression modeling with backward stepwise elimination was used to determine reduced parameters and establish a prediction model. The discrimination efficacy, calibration efficacy, and clinical utility of the prediction model were evaluated. The prediction model was validated using data for 176 patients collected from another hospital. Eight independent prognostic factors were identified: hypertension, Marshall scale (types III and IV), subdural hemorrhage (SDH), location of contusion (frontal and temporal contusions), Injury Severity Score >13, D-dimer level >11.4 mg/L, Glasgow Coma Scale score ≤10, and platelet count ≤152 × 109/L. A prediction model was established and was shown as a nomogram. Using bootstrapping, internal validation showed that the C-statistic of the prediction model was 0.881 (95% confidence interval [CI]: 0.849–0.909). The results of external validation showed that the nomogram could predict ND with an area under the curve of 0.827 (95% CI: 0.763–0.880). The present model, based on simple parameters collected on admission, can predict the risk of ND in patients with mTBI accurately. The high discriminative ability indicates the potential of this model for classifying patients with mTBI according to ND risk.
Introduction
Traumatic brain injury (TBI) is the leading cause of death and disability of young adults at their most productive age. 1 –3 Moderate TBI (mTBI), which is typically defined by a Glasgow Coma Scale (GCS) score of 9–13 at admission, 4 has received relatively little attention in the literature describing TBI because of the relatively mild condition. 5 To date, few studies have concentrated specifically on characteristics and prognosis of patients with mTBI. There are no clear guidelines for management of mTBI in these patients. 6
In fact, patients with mTBI are in a dangerous state and at high risk of neurological deterioration (ND). In a prospective multi-center clinical study, as high as 33.3% of patients with mTBI were observed to have ND in the subsequent course of disease. 7 The ND is typically followed by fatal results or severe disability and is a prognostic factor related to unfavorable outcomes. 5,8 Among patients with mTBI who have poor outcomes, more than half were reported to have ND. 9
Hence, patients with mTBI who are at high risk of ND need a higher level of medical care than those at low risk of ND. If a patient with mTBI who is at high risk of ND could be identified in advance, a high level of monitoring and treatments including neurological assessment, intensive care unit, and even increased intracranial pressure monitoring may be implemented. Thus, early identification of a patient with mTBI at high risk of ND is critical. Unfortunately, there is no study reporting a risk factor or prediction model for ND of patients with mTBI.
The objectives of this study were to evaluate the prognostic value of admission risk factors related to ND of patients with mTBI and to develop a prediction model by combining independent predictors. The prediction model was then validated in a separate cohort of patients.
Methods
Patient population
All patients with mTBI who were treated at Tangdu Hospital affiliated with the Air Force Medical University from January 1, 2015 to December 31, 2020 were reviewed. The patients' information, medical records, laboratory parameters, and radiological images were collected via a physician workstation.
We screened all patients who received a diagnosis of mTBI and collected their demographic and clinical characteristics on admission. The inclusion criteria were: (1) a GCS score of 9–12 on admission; (2) admission within 24 h post-injury; (3) performing a computed tomography (CT) scan on the day after admission; (4) patients older than 18 years. The exclusion criteria were: (1) presence of penetrating injuries and associated spinal cord trauma; (2) nursing and pregnant women; (3) patients who had other malignant tumors, severe mental disorders, or hematologic diseases; (4) patients who died in the emergency department (ED); (5) patients with evacuated mass lesions (defined according to the Marshall brain CT classification). 10
The data were collected separately for model validation at the department of neurosurgery of Yan'an People's Hospital (Yan'an, China) using the same inclusion and exclusion criteria from June 2015 to December 2020.
Potential predictors of early ND
Two researchers reviewed all eligible patients. Demographic variables, mechanism of injury, clinical characteristics, head CT scan findings, and laboratory parameters on admission were recorded for subsequent analysis.
Clinical characteristics
The data related to basic diseases (hypertension, coronary heart disease, chronic obstructive pulmonary disease, and diabetes) and history of medication (aspirin, clopidogrel, anticoagulants) were recorded. The GCS score was recorded by each component of eye opening, verbal response, and motor response. Mechanism of injury included motor vehicle accident, pedestrian accident, fall from height, assault, etc. Extracranial trauma injury was quantified by the Injury Severity Score (ISS) and the Abbreviated Injury Scale. 11
Head CT scan findings
Of the CT scan findings, type of intracranial hemorrhage was first recorded as epidural hemorrhage (EDH), traumatic subarachnoid hemorrhage (tSAH), subdural hemorrhage (SDH), intraventricular hemorrhage (IVH), and brain contusion. The brain is divided into functional lobes, including frontal lobe, temporal lobe, parietal lobe, occipital lobe, cerebellum, and brainstem. The maximum thickness of SDH and volume of EDH were measured on the CT scan. 12,13 The severity of tSAH was evaluated with the modified Fisher (mFisher) scale. 14 The Marshall brain CT classification was implemented according to Marshall LF M's criteria. 10
Laboratory examinations
Laboratory examinations were performed within 12 h after injury. The hematological parameters were hemoglobin, red blood cell count, white blood cell count, and platelet (PLT) count. For coagulation parameters, prothrombin time, fibrinogen, fibrinogen degradation products (FDPs), D-dimer, and activated partial thromboplastin time were detected.
The blood creatinine, glomerular filtration rate, and blood urea nitrogen were identified as the indicators of renal function. The levels of alanine aminotransferase, albumin, and aspartate aminotransferase (AST) were assessed as the indicators of hepatic function.
Definition and detection of ND
The ND was defined as the occurrence of one or more of the following criteria within seven days after injury: (a) a decrease in GCS score of 2 points or more from the initial GCS score with no pharmacological sedation; (b) a deterioration in neurological status being sufficient for neurosurgical intervention. 7,15 –17 Accordingly, patients were divided into an ND group (with ND) and a non-ND group (without ND).
Derivation and validation of the prediction model
Univariate and multi-variate logistic regression analysis with stepwise backward were applied to screen the risk factors for ND. To obtain comparable odds ratios (ORs) for the linear relationships and attain clear threshold values for those continuous variables, we rescaled each variable by using the receiver operating characteristic (ROC) curve.
The logistic regression model was established by including the risk factors, with ND as the prediction. The optimal model selection was performed by applying a backward stepwise selection procedure through a likelihood-ratio test with Akaike information criterion (AIC). A nomogram was constructed based on the risk factors selected by the multi-variate logistic regression test. The nomogram's prediction accuracy was evaluated by C-statistic, calibration curve, decision curve (DCA), and clinical impact curve (CIC) analysis. Finally, the model was validated externally in a separate cohort from Yan'an People's Hospital.
The study was approved by the Institutional Review Board, Tang Du Hospital, Fourth Military University (approval number: 202011-14) in December 2020. All procedures performed in the present study were in accordance with the 1964 Declaration of Helsinki.
Statistical analysis
Descriptive statistics were used to characterize categorical and numerical variables. Categorical data were tabulated and presented as number(s) and percentage(s). Continuous variables were summarized using mean (standard deviation) or median (interquartile range). Univariate (chi-square test, t test, or Mann-Whitney U test, as appropriate) and multi-variate logistic regression analyses were used. The ORs, together with their 95% confidence intervals (CIs), were derived as well.
Statistical analyses were performed using the SPSS 24.0 software (IBM Corp., Armonk, NY), and nomogram establishment was undertaken by R 3.6.1 programming language. A p value <0.05 was considered statistically significant.
Results
Patient demographic and clinical characteristics in the derivation cohort
A total of 676 patients with mTBI were screened. Overall, 479 patients who met the inclusion criteria were included in the study and classified into the ND group and non-ND group (Supplementary Table S1). Of the 479 patients, ND developed in 135 (28.2%) within seven days after injury. The median time of ND in patients was 39 h, 107 (79.3%) patients deteriorated within 72 h, and 28 (20.7%) patients deteriorated between 72 h and seven days after injury (Supplementary Table S2).
The distribution of patient characteristics differed between the two groups. The proportion of hypertension, coronary heart disease, and diabetes was higher in the ND group than in the non-ND group. Patients in the ND group also had a longer history of taking aspirin and anticoagulants, high Marshall scale, tSAH, SDH, skull fracture, and brain contusion than those in the non-ND group. The results of further analysis of EDH, SDH, and brain contusion are shown in Supplementary Tables S3–S5.
Continuous variables were dichotomized by using the ROC curve (Supplementary Fig. S1 and Supplementary Table S6). Age >55, GCS score ≤10, PLT count ≤152 × 109/L, ISS >13, D-dimer >11.4 mg/L, FDP >22.3 mg/L, and AST >39 U/L were defined as the cutoff values, with a significantly higher incidence of ND observed in patients within these ranges than others. Patients with ND had worse outcomes (death rate, 34.8%) than patients who did not (death rate, 4.1%) (Supplementary Table S7).
Multi-variate logistic regression analysis
Severe risk factors associated with a higher risk of ND were investigated (Supplementary Table S1). The independent predictor variables were then identified by stepwise backward logistic regression analysis. After excluding variables exhibiting poor predictive performance or multi-collinearity, eight variables maintaining prognostic significance were derived as follows (Table 1 and Supplementary Fig. S2): hypertension, Marshall scale, SDH, location of contusion (LOC), ISS >13, D-dimer level (>11.4 mg/L), GCS score ≤10, and PLT ≤152 ( × 109/L).
Results of the Multi-Variate Logistic Regression Analysis
OR, odds ratio; CI, confidence interval; DI, diffuse injury; NEML, non-evacuated mass lesion; ISS, Injury Severity Score; GCS, Glasgow Coma Scale; PLT, platelet.
control group
Development, validation, and assessment of the nomogram
Each of the eight prognostic variables was assigned a point proportional to its regression coefficient (Supplementary Table S8). A score for a patient was calculated by summation of the points corresponding to each risk factor (Supplementary Table S9). A prediction model was established and is shown as a nomogram in Figure 1.

Nomogram for the prediction of ND and its discrimination performance. Data of the development cohort were employed to establish the purposed nomogram, which incorporated hypertension, Marshall scale, SDH, LOC, Injury ISS >13, D-dimer level (>11.4 mg/L), GCS score ≤10, and PLT ≤152 ( × 109/L). A total point for a patient was calculated by summation of all the points assigned to each factor. The patient's risk was determined by drawing a perpendicular line from the axis of total points to the probability axis.
With bootstrapping, internal validation showed that the C-statistic of the risk score was 88.10% (95% CI: 84.90–90.90) (the mean absolute error was 0.02) (Fig. 2A and Supplementary Table S10). The calibration curve analysis of this purposed predictive model presented a good agreement in our research (slope of 0.8432 and intercept of -0.1108; Fig. 2B). The DCA curve showed that because threshold probability was within the range from 0.1 to 1.0, this nomogram could obtain a greater net benefit than either “treat none” or “treat all” scheme. The nomogram also received a higher net benefit than each factor alone across the reasonable threshold probabilities (Fig. 3A).

The results of calibration and ROC curve analysis of the purposed nomogram. (
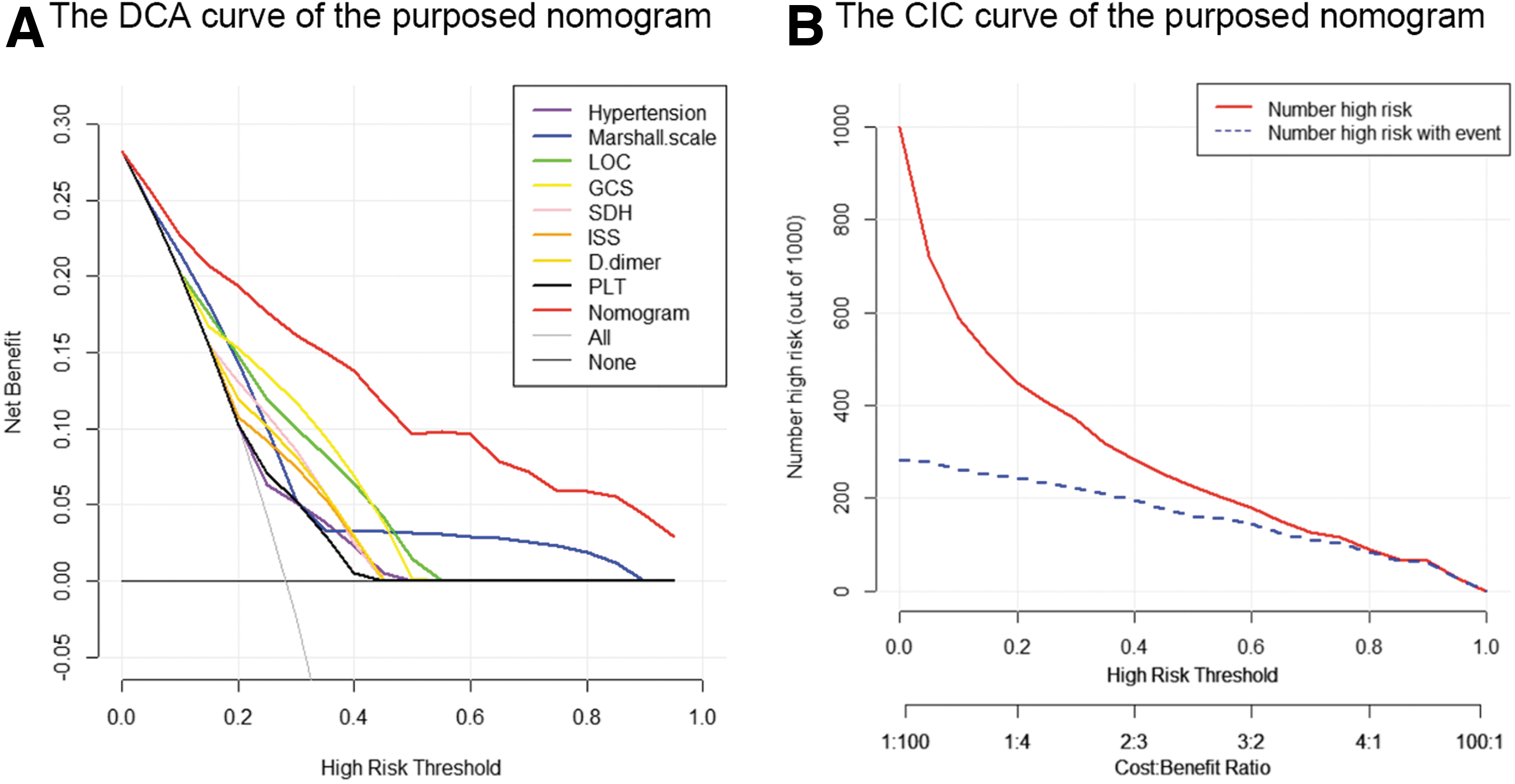
The results of the DCA and the CIC of the purposed nomogram for predicting early neurological deterioration (ND) in the training cohort. (
The clinical effectiveness of the nomogram was demonstrated by the CIC. The number of subjects who were at high risk (the number of positive cases predicted by the nomogram) was highly matched with the number of subjects who were at high risk with outcomes (the number of true-positive cases) when the threshold probability was above 65% (Fig. 3B).
External validation was conducted in a validation cohort of 176 patients from another hospital. According to the results, the prediction model showed an accuracy of 80.68% (142/176) in the validation cohort, with 142 (112 + 30) patients consistent with the truth, 14 cases misdiagnosed, and 20 cases missed diagnosis (Supplementary Table S11). In the validation cohort, ROC curve analyses showed that the area under the curve (AUC) of the prediction model was 0.827 (95% CI: 0.763–0.880) (Fig. 4A and Supplementary Table S12). Besides, the calibration curve analysis of the purposed prediction model revealed a good agreement in the validation cohort (slope of 0.8358 and intercept of -0.1107; Fig. 4B).

The results of calibration and ROC curve analysis of the purposed nomogram for predicting neurological deterioration (ND) occurrence in the external validation cohort. (
Discussion
Neurological deterioration was reported in quite a large proportion of patients with mTBI, and it is associated mainly with unfavorable outcomes. 7 Early identification of patients with mTBI who are at high risk of ND is essential to determine treatment efficacy. Previous ND-based studies concentrated on mild TBI or included mild and moderate TBI as a single entity. The mild TBI, however, is quite different from mTBI in terms of clinical features, treatments, and outcomes. This study, for the first time, developed and validated a prediction model for ND of patients with mTBI.
The GCS score indicates the severity of injury in patients with TBI. Initial GCS score has been identified as a predictor of ND in patients with mild TBI. In the present study, patients with mTBI with GCS scores ≤10 were considered to have a higher risk of ND than those with GCS scores ≥10. Accordingly, mTBI has already been dichotomized by a GCS score equal to 10. Further, patients with mTBI with GCS scores ≤10 and abnormal CT findings were suggested to be treated according to a severe TBI protocol, because of high risk of deterioration. 6 Besides, a lower GCS score was found to be associated with a higher risk of contusion progression, 18 which is a major cause of ND.
The mTBI is typically complicated by multiple injuries, aggravating brain injury, as well as being associated with poor outcomes. 5,6 The severity of multiple injuries could be quantized by ISS. The results of the present study showed that ISS ≥13 predicted ND, indicating that patients with mTBI who had moderate-to-severe multiple injuries may be at high risk of ND. A negative association, however, between ISS and ND was reported by Scheetz and associates. 19 The divergence may be attributed to different research subjects; for instance, Scheetz and associates 19 concentrated on older patients, representing only the minority of patients with mTBI. 5
High D-dimer level and low PLT count were also demonstrated to predict ND. These two parameters have also been proven to be risk factors of progressive hemorrhagic injury, 20 which may lead to ND.
The findings of the current study revealed the role of hypertension in ND. Hypertension has been reported to be detrimental for patients with TBI. 21,22 The mechanism of the increased blood pressure in ND may be because of cerebral edema, which can be aggravated by the increased regional blood flow and transudation of fluid across disrupted blood–brain barrier in case of hypertension. 23 Besides, catecholamine can be secreted in patients with TBI who have hypertension. 24 Catecholamine has been reported to aggravate brain edema by increasing cerebral capillary pressure and permeability. 21,23 –25
In the present study, it was also found that the Marshall class of patients with mTBI ranged from II to III, and the sample size of such patients with grade I and above III was small, which was similar to the results of Compagnone and colleagues. 7 The Marshall classification system plays an important role in predicting the prognosis of patients with TBI, aiming to evaluate the diffuse axonal injury. The higher degree of diffuse TBI is, the more severe the secondary brain damage will be, 26,27 which may justify aggravating the early ND in patients with mTBI.
The current study showed a positive association between SDH and ND in patients with mTBI. The SDH has also been reported to be a risk factor for ND in patients with mTBI. The SDH typically occurs from tearing of cerebral cortical vessels or bridging veins. 28 It is not stable and has a tendency for rebleeding because the crevasses of blood vessels are only occluded by blood clot. It has been reported that approximately 10% of acute SDH without surgical intervention in the early stage may be associated with hematoma enlargement during follow-up. 29
The initial thickness of SDH could also be a predictor of ND, indicating that the size of SDH could be associated with ND. This was consistent with a previous study by Mathew and coworkers 30 who showed that all SDHs greater than 10 mm in thickness required surgical evacuation. A large SDH with a high initial thickness may occur because there is a lower possibility of deterioration compared with a small hematoma.
A combination of frontal and temporal lobes was also found to be a predictor of ND in patients with mTBI. Coup or contrecoup traumatic intraparenchymal contusions commonly occur along the inferior frontal and anterior temporal lobes, where the brain has the greatest chance of impact against the rigid bone. 26,27 The location of contusion has been suggested to be associated with subsequent growth, with frontal and temporal contusions being more likely to progress compared with other locations.
According to the results of the present research, the simultaneous presentation of frontal and temporal contusion could be a predictor of ND in patients with mTBI, while solitary presentation of frontal or temporal contusion was not. This may be plausible because patients with multiple contusions are more likely to experience contusion progression than those with a single contusion. 28 Moreover, the volume of frontal or temporal lobes was <10 mL, and patients are at a low risk of hemorrhagic progression. 29,31
In patients with mTBI with both frontal and temporal contusions, the volume was above 15 mL, and patients were at high risk of hemorrhagic progression. 31 Both the frontal and temporal contusions may coalesce as they progress. The association between contusion and ND may also represent that a more severe initial injury is inherently combined with a greater risk of progression.
In the present study, we established a prediction model for ND of patients with mTBI and demonstrated that the risk of ND can be predicted by variables on admission. The performance of the prediction model was highly reliable when it was validated in a separate external cohort. Patients with mTBI who are at high risk of ND may be identified in advance by using this prediction model and receive aggressive therapies. The outcome of patients with mTBI who have a high risk of ND may possibly be improved, although whether they could benefit from aggressive therapies remains to be studied.
The strengths of our study included that all risk factors could be easily assessed on admission, the prediction model may support neurosurgeons in early detection of ND in patients with mTBI, and the generalizability of the prediction model was supported by external validation. Consider that mTBI is a heterogeneous entity poorly defined in the literature. The high discriminative ability indicates the potential of this model for classifying patients with mTBI according to ND risk.
The current study contains several limitations. First, because of the retrospective nature of the study, some data might be missed or misinterpreted. The time of ND was not recorded. Second, continuous variables were rescaled into categorical variables. This strategy simplifies the creation of a prediction model. The use of categorical variables, however, provides less information and worse predictive performance than continuous variables. Last, a few patients who were deteriorated after seven days were not included in this study, although the population of patients with a late deterioration was limited.
Conclusions
We developed and evaluated a novel model to predict the risk of ND among patients with mTBI and validated it in an external cohort. The purposed model provided significant information for the early identification of ND in patients with mTBI. It can be used as a supplementary resource for clinical data and CT images, and it may improve the reliability of clinical decisions. Further prospective studies are required, however, to confirm our results.
Footnotes
Authors' Contributions
QY and LZH conceived and designed the experiments; CMS, LZH, and YZF performed, analyzed, and interpreted the results of the experiments.
Funding Information
This work was supported by the found of clinical research major project of Tang Du Hospital (Grant No. 2021LCYNJ007).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11
Supplementary Table S12
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.