
Abstract
Assessment of the degree of impaired autonomic nervous system (ANS) function is not part of routine clinical practice during inpatient rehabilitation following traumatic spinal cord injury (SCI). The goal of this investigation was to determine the utility of the International Standards for Neurologic Classification of SCI (ISNCSCI) and the recently revised International Standards to document remaining Autonomic Function after SCI (ISAFSCI) in documenting cardiovascular ANS impairment during inpatient rehabilitation following traumatic SCI. Beat-to-beat recording of supine heart rate (HR) and blood pressure (BP) were collected at the bedside for estimation of total cardiovascular ISAFSCI score, cardio-vagal modulation (i.e., high frequency HR variability [HFHRV]) and sympathetic vasomotor regulation (i.e., Mayer wave component of systolic BP [SBPmayer]). A total of 41 participants completed baseline testing, which was conducted 11 ± 5 days from the admission ISNCSCI examination. There were no differences in supine HR or BP based on the ISNCSCI or ISAFSCI assessments. The HFHRV was generally lower with more distal lesions (r2 = 0.15; p = 0.01), and SBPmayer was significantly lower in those with American Spinal Injury Association Impairment Scale (AIS) A compared with AIS B, C, D (Cohen's d = -1.4; p < 0.001). There were no significant differences in HFHRV or SBPmayer in patients with or without ISAFSCI evidence of cardiovascular ANS impairment. These preliminary data suggest that neither the ISNCSCI nor the ISAFSCI are sensitive to changes in ANS cardiovascular function following traumatic SCI. Bedside assessment of HR and BP variabilities may provide insight, but are not readily available in the clinical setting. Further research is required to evaluate methods that accurately assess the degree of ANS impairment following traumatic SCI.
Introduction
The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) is used during inpatient rehabilitation to document the neurologic level of injury (NLI) pertaining to the motor and sensory nervous systems following traumatic injury in patients with spinal cord injury (SCI). While inpatient rehabilitation following traumatic SCI is focused on regaining motor function, clinicians spend a significant amount of time managing disorders of the autonomic nervous system (ANS)—in particular, severe cardiovascular dysfunction. 1 The ISNCSCI examination, however, does not directly assess the degree of ANS impairment and it is unclear if the level or completeness of motor and sensory function reflect ANS injury after traumatic SCI. Yet, individuals with SCI rate recovery of ANS function as one of their highest priorities, due in part to the significant adverse impact on their quality of life. 2 As such, clinical assessment following SCI should include testing pertaining to ANS control of organ system function.
The ANS is involved in the regulation of heart rate (HR) and blood pressure (BP) during routine activities of daily living, and following SCI, damage to the ANS is associated with various cardiovascular disorders, including bradycardia, tachycardia, hypotension, orthostatic hypotension (OH) and autonomic dysreflexia (AD). 3 -5 It is commonly reported that these cardiovascular disorders are highly prevalent in individuals with more rostral NLI (i.e., at or above T6), and more complete injuries as assessed by the ISNCSCI examination, 4 although this evidence is inconclusive. 6,7 In fact, we and others have reported substantial BP instability in individuals with chronic low thoracic (below T6) lesions. 8,9 The completeness of motor and sensory loss as determined by the American Spinal Injury Association Injury Scale (AIS) classification from the ISNCSCI examination does not relate to the degree of ANS completeness of injury over the first year post-SCI 10 or in the chronic (>12 months after injury) stage of injury. 6,7
Yet, the degree of cardiovascular ANS impairment following SCI is significant because clinical reports suggest that unstable BP in individuals with SCI may contribute to the increased incidence of cardiovascular disease, 11 stroke risk, 12 and cognitive dysfunction, 13 and cardiovascular disorders are a leading cause of morbidity and mortality among individuals with SCI. 14 It has been reported that OH and AD, and their respective symptoms, impede function and lead to missed crucial rehabilitation therapy time in newly injured patients with SCI. 4 In fact, BP changes reflecting OH were documented during 73.6% of mobilization therapy sessions, and symptoms were noted in 58.9% of cases, which were perceived to substantially limit participation in the treatment. 4 Important new evidence indicates that the completeness of the ANS injury, assessed approximately 1 month after the SCI onset, was associated with symptoms of OH and fatigue at a 1-year (415 ± 17 days) follow-up visit. 10
Despite the significance of ANS impairment and the adverse clinical consequences, we are limited in our ability to assess the extent of impairment during inpatient rehabilitation in patients with SCI. Because cardiovascular ANS regulation occurs independently of volitional motor function or sensation, determining the level of ANS cardiovascular impairment following SCI is challenging. As such, an expert panel of clinicians and scientists developed the International Standards to document remaining Autonomic Function after SCI (ISAFSCI), 15 which was recently revised 16 and is recommended to be used in conjunction with the full ISNCSCI examination to document the degree of ANS impairment following SCI.
In addition to the ISAFSCI, noninvasive techniques to quantify beat-to-beat changes in HR and BP have been used to estimate the degree of cardiovascular ANS impairment following SCI. 17 –20 Use of these techniques has been used to capture significantly altered HR variability (HRV) and BP variability (BPV) at rest and during provocative maneuvers in patients with chronic tetraplegia and paraplegia compared with uninjured controls, which is indicative of altered cardiovascular ANS function. 21,22 Lucci and colleagues recently examined the low frequency (LF) components of HRV and BPV in newly injured individuals with SCI and suggest that patients with injury at or above T6 with low LF-BPV (i.e., <2 mm Hg2) 1 month post-injury should be considered autonomically complete. 10 Impaired cardiovascular ANS function may predispose these patients to poor outcomes and diminished health-related well-being following traumatic SCI. In fact, low peak HR, reflecting cardiovascular ANS impairment, at discharge from inpatient rehabilitation was recently reported to be associated with poor participation and reduced physical activity levels 1 and 5 years later. 23
The present study was designed to examine the utility of the ISNCSCI and the recently revised ISAFSCI in documenting cardiovascular ANS impairment at a baseline assessment in patients with SCI during inpatient rehabilitation following injury. Cardiovascular ANS impairment was defined by the total score on the cardiovascular section of the ISAFSCI examination and by parameters of supine HRV and BPV.
Methods
Participants
Patients with traumatic SCI within 6 months of injury who were 18-80 years old, non–ventilator-dependent, and were able to understand the English language were recruited to participate from July 2017 to March 2020. Individuals were excluded if they had insufficient mental capacity, English speaking competency, or reading ability to provide informed consent. We certify that informed, witnessed, written or verbal consent was obtained from each participant prior to initiation of the study procedures. This project is supported by the National Institutes for Disability and Independent Living Rehabilitation Research model systems grant (#SI-0158) and is registered on
ISNCSCI examination
The ISNCSCI examination is recognized worldwide as the standard for the examination and classification of neurological sensorimotor impairment after SCI for use in clinical trials and routine clinical practice. 24 The ISNCSCI examination is performed with the individual in the supine position to evaluate segmental somatosensory perception, motor function, and provide the NLI and AIS classification of injury.
ISAFSCI examination
While the ISAFSCI is designed to document the degree of ANS impairment to multiple organ systems (i.e., broncho-pulmonary, thermoregulatory, sudomotor, bowel, bladder, sexual and reproductive), we focused this study on the cardiovascular section of the examination. We collected beat-to-beat supine HR and BP data at the bedside and used the definitions from the general autonomic function section of the ISAFSCI to assess the clinical presentation of cardiovascular ANS impairments post-SCI. 15,16 Beat-to-beat HR and BP were averaged over a 5-min supine observation, and ISAFSCI criteria for cardiovascular dysfunction were as follows: 1) bradycardia = HR ≤60 bpm; 2) tachycardia = HR ≥100 bpm; 3) systolic hypotension = supine systolic BP (SBP) ≤90 mm Hg; or 4) diastolic hypotension = supine diastolic BP (DBP) ≤60 mm Hg. In addition, we classified individuals with 5) neurogenic shock if they were within 30 days of injury (n = 14) and met criteria for both bradycardia and systolic hypotension. To document orthostatic hypotension (OH), we passively re-positioned patients into the seated position by moving the head of their bed into an up-right position between 45° and 90° while the legs remained horizontal to the hips, and we monitored beat-to-beat changes in HR and BP continuously. We did not perform the sit-up test, which is a provocative maneuver used in the SCI population to test for OH, 25 to avoid eliciting symptoms of orthostatic intolerance and because there were mechanical limitations with the hospital beds. We defined OH 6) as a fall in SBP ≥20 mm Hg and/or 7) a fall in DBP ≥10 mm Hg when moved from the supine to the seated position. 15,26 Autonomic dysreflexia (AD), was defined as 8) a rise in SBP >20 mm Hg from average supine SBP any time during testing in individuals with lesions at or above T6. 16
Data collection
Testing was conducted at the bedside after hospital admission to an acute SCI rehabilitation unit. Instrumentation was applied during quiet rest with the patient in the supine position and included: a three-lead ECG (UFI RESP1 Impedance Pneumograph, Morro Bay, CA), a finger photoplethysmography cuff (Finometer MIDI, Finapres Medical Systems B. V., Enschede, the Netherlands), and a digital sphygmomanometer (Welch Allyn 300 Series Vital Signs Monitor, Skaneateles, NY). Beat-to-beat BP was monitored and recorded at the middle finger of the dominant hand and brachial BP was recorded at 1-min intervals on the opposite arm, which was used to calibrate the finger BP signals. The depth and rate of breathing was monitored by the RESP1 Impedance Pneumograph, and the 5-min assessment of supine beat-to-beat HR and BP, used to determine ISAFSCI score and parameters of cardiovascular ANS function (i.e., HRV and BP), was recorded during normal tidal, unpaced breathing.
Data analysis
The continuous HR and BP signals were viewed and monitored in real time and were stored on a laptop hard drive for offline analysis. The customized analytical program, written with LabView graphical software (National Instruments, Austin TX), performs automated peak detection with visual inspection for artifacts and anomalies and allows for cursor-based manual editing of individual beats where appropriate (e.g., because of errors in the automated peak detection process). Discrete Fourier transform algorithms were employed to quantify the power spectra within the high-frequency range of HR (HFHRV: 0.15-0.40 Hz) and at the Mayer wave frequency range for SBP (SBPmayer: 0.07-0.14 Hz) as markers of cardio-vagal and sympathetic vasomotor tone, respectively. The natural log (ln) was applied to the raw signals for statistical comparisons and a constant of 1.0 was added to each score to remove negative ln values.
Statistical analysis
Group differences in demographic characteristics, supine cardiovascular ANS assessments, HFHRV and SBPmayer were compared with a simple analysis of variance model for NLI (cervical: C2-T1, high thoracic: T2-T5, and low thoracic: T6-T12) or independent t tests for AIS (AIS A versus AIS B/C/D) and ISAFSCI score (0, ≥ 1). The relationships between parameters of cardiovascular ANS control (HFHRV, SBPmayer), with demographic characteristics (age, sex, medications), injury characteristics determined on the ISNCSCI examination (NLI, AIS, motor score, sensory score, time since injury [TSI]) and the ISAFSCI examination (total cardiovascular score), were assessed using bivariate regression. Significant univariate associations were further explored with multiple regression analyses to examine the collective impact of the independent variables on HFHRV and SBPmayer. Of note, in the multiple regression models, NLI was treated as an integer (e.g., C1 = 30, C2 = 29…), AIS A = 1 and AIS B/C/D = 0. All analyses were conducted using R software, with the exception that JASP was used to calculate Bayes factors. Data are reported as means ± standard deviation and significance was set at an alpha of 0.05.
Results
Demographic and injury characteristics are presented for the 41 participants with baseline data (Table 1). The study sample was mostly male (80%) with cervical (56%) AIS A (71%) lesions and were on average 43.8 ± 16.7 years old (range 18-80 years). The most common injury etiology was falls (36.5%), followed by motor vehicle accidents (28.9%) and violence (21.2%). Baseline testing was conducted, an average 49.6 ± 38.4 days from injury (range 9-193 days) and an average of 11.9 ± 5.8 days from administration of the ISNCSCI examination (range 5-26 days). The baseline testing was not conducted with the admission ISNCSCI because this was a research study and the consent process required time between the initial clinical evaluation of eligible patients and voluntary signature for active participation. Patients with cervical injuries tended to be older (47.6 ± 16.8 years) than those with high thoracic (35.8 ± 13.7 years) and low thoracic (37.7 ± 16.2 years) injuries; however, this was not significant (η2 = 0.10; p = 0.06, Bayes Factor [BF10] = 1.5). Participants with AIS A lesions were significantly younger than those with AIS B/C/D lesions (Cohen's d = 0.58; p = 0.047, BF10 = 1.5, 95% confidence interval [CI] for mean difference = -18.7 to -0.16 years).
Participant Characteristics
ID, participant identification; NLI, neurologic level of injury; AIS, American Spinal Injury Association Injury Classification Scale; TSI, time since injury; NLI, neurologic level of injury; ISAFSCI, International Standards to document remaining Autonomic Function after SCI; Brady, bradycardia; Tachy, tachycardia; Hypo, hypotension; NS, neurogenic shock; OH, orthostatic hypotension; AD, autonomic dysreflexia; M, male; F, female; na, not assessed
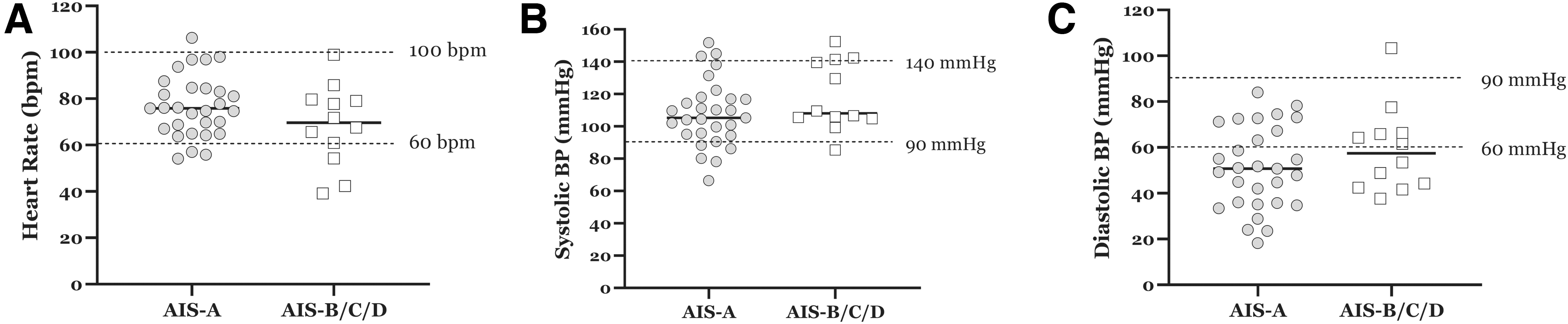
Although average supine HR (74.3 ± 14.9 bpm), and SBP (111.0 ± 21.1 mm Hg) were within normal limits based on ISAFSCI thresholds, average DBP (53.3 ± 18.4 mm Hg) was in the hypotensive range. 16 Overall, 18 (44%) participants had evidence of cardiovascular ANS impairment based on the criteria from the ISAFSCI. Six participants (15%) were bradycardic and six were hypotensive; however, only two met both criteria and were within 30 days of injury to be classified with neurogenic shock: one (C2, AIS A) was 9 days from injury, the other (C4, AIS C) was 13 days from injury. Due to methodological data collection errors and patient intolerance, only 37 participants had available data during the orthostatic challenge, and 9 (24%) had evidence of OH. While 12 patients (29%) had an increase in SBP that met criteria for AD (i.e., rise in SBP >20 mm Hg; two had low thoracic lesions: (1) T7, AIS B; (2) T11, AIS A, which would not be considered AD, and none reported any symptoms.
There were no differences in demographic or injury characteristics comparing participants with (n = 18) to those without (n = 23) ISAFSCI evidence of cardiovascular ANS impairment (all p > 0.11, all Cohen's d < 0.51). Further, although 72.2% (n = 13) of participants with ISAFSCI evidence of cardiovascular ANS impairment had cervical injuries, two patients with low thoracic injuries (T7 and T11) had OH, due to supine hypertension (DBP = 103 mm Hg; SBP = 143 mm Hg; respectively). In addition, there was an equal number of participants with cervical AIS A lesions with (n = 7) and without (n = 7) ISAFSCI evidence of cardiovascular ANS impairment.
Use of prescription medications that may impact cardiovascular ANS function is presented (Table 2); four participants were prescribed an anti-hypertensive medication, 33 (80%) were prescribed an anti-hypotensive medication and 39 (95%) were prescribed a medication for pain or neuropathic pain. It should be noted that we were unable to determine the impact of prescription medication use on cardiovascular ANS impairment because of the large number of medications prescribed among relatively few patients.
Medications and Co-Incident Conditions
OH, orthostatic hypotension; AD, autonomic dysreflexia.
There were no significant differences in average supine HR or BP by NLI (Fig. 1) or AIS classification (Fig. 2). The influence of the NLI and AIS classification of injury on the parameters of cardiovascular ANS control is presented (Fig. 3). Patients with low thoracic injuries had, on average, significantly lower HFHRV (3.88 ± 1.25 ln) as compared with those with cervical (5.81 ± 1.42 ln; p < 0.01) and high thoracic (5.87 ± 1.19 ln; p < 0.05) injuries (Fig. 3A). There was a significant linear relationship between NLI (C1 = 30; C2 = 29…) and HFHRV (r2 = 0.15, slope = -0.11 ln HF area per spinal segment, BF10 = 4.1, 95% CI = -0.19 to -0.02). The relationship between NLI and SBPmayer was not significant (data not shown). Patients with AIS A lesions had significantly lower SBPmayer compared with those with AIS B/C/D lesions (0.66 ± 0.6 vs. 1.65 ± 0.9 ln, respectively; Cohen's d = 1.44, p < 0.001, BF10 = 146.9; Fig. 3B). Based on the recent Lucci and colleagues' findings, 10 we determined that 30 (73.2%) participants had complete autonomic injuries i.e., SBPmayer < 2.0 mm Hg2—14 (46.7%) with cervical AIS A lesions and the median TSI was 48 days (range: 9-193 days). Parameters of cardiovascular ANS control did not differ significantly in patients with and without ISAFSCI evidence of cardiovascular ANS dysfunction (data not shown). Further, chronologic age and the number of prescription medications did not relate significantly to HFHRV or SBPmayer.

Supine heart rate
Supine heart rate

Supine HFHRV
Regression models were constructed to identify variables with significant contribution to HFHRV and SBPmayer. The predictor variables included: age, sex, TSI, motor scores, sensory scores, NLI (as an integer), AIS classification (AIS A [1]; AIS B/C/D [0]) and ISAFSCI (with [1]; without [0]); variables with significant bivariate correlations were entered into multi-variate models to predict HFHRV and SBPmayer. It should be noted that age, sex, and motor scores from the ISNCSCI examination lacked discriminatory capacity in the prediction of cardiovascular ANS function and were not entered into any of the models. Only NLI was a significant predictor of HFHRV (R2 = 0.15; p = 0.01, BF10 = 4.1), therefore multi-variate models were not constructed.
Bivariate analyses for SBPmayer indicated significant associations with TSI (R2 = 0.11; p = 0.04, BF10 = 1.8), AIS classification (R2 = 0.31; p = 0.001, BF10 = 147), and sensory score (R2 = 0.24; p = 0.01, BF10 = 28.5). Results of the multi-variate model to predict SBPmayer with TSI, AIS classification and sensory score is presented (Table 3). With AIS classification in the model at step 1 (R2 = 0.31, p < 0.001), TSI added significantly to the model when entered in at step 2 (increment in R2 = 0.08, p = 0.03); however, when sensory score was introduced into the model at step 2, the effect did not reach significance (increment in R2 = 0.06, p = 0.07). When all three variables are forced into the model, the increment in R2 of 0.04 (p = 0.12) was not a significant improvement compared with the model with AIS and TSI alone. Due to the relatively small sample size, caution should be employed when interpreting this result, which should be confirmed in a subsequent trial.
Multi-Variate Models to Predict SBPmayer
Model 1 = AIS; Model 2 = AIS+TSI;
Model 3 = AIS+sensory score; Model 4 = AIS+TSI+sensory score.
versus Model 1; **versus Model 2.
SBPmayer, Mayer wave component of systolic blood pressure; AIS, American Spinal Injury Association Impairment Scale; TSI, time since injury.
Discussion
Clinical assessment of sensorimotor function using the ISNCSCI examination does not directly assess ANS function, and the utility of the ISAFSCI to document the integrity of cardiovascular ANS control has not been reported in newly injured patients with traumatic SCI. The findings of this study suggest that the ISAFSCI examination has limited sensitivity in discerning the degree of cardiovascular ANS impairment during inpatient rehabilitation following traumatic SCI. A novel yet somewhat counter-intuitive finding of the present study was the significant and linear association between NLI and HFHRV—that is, the higher the NLI the higher the degree of cardio-vagal tone. A second novel finding was that compared with patients with complete motor and sensory injury, as documented on the ISNCSCI examination as AIS A, patients with some sparing of motor and/or sensory function (AIS B/C/D) had significantly increased SBPmayer.
Based on the ISAFSCI examination, criteria for resting supine HR and BP did not relate to the parameters of cardiovascular ANS function, regardless of the NLI or AIS classification. Further, seven participants with AIS A tetraplegia did not present with evidence of altered supine hemodynamics based on the ISAFSCI criteria. It is unclear if this is because the NLI and AIS from the ISNCSCI examination do not accurately reflect—or if the ISAFSCI is not a valid surrogate of—cardiovascular ANS impairment. Because we took care not to elicit symptomatic OH by conducting the study at the bedside and limiting the orthostatic gradient imposed, we likely underestimated the incidence of impaired ANS orthostatic cardiovascular regulation. Use of the ISAFSCI to document cardiovascular ANS responses during mobilization to active rehabilitation should be reported to determine the utility of the examination for documenting response to routine in clinical practices during inpatient rehabilitation following traumatic SCI.
Although NLI and AIS classification as assessed on the ISNCSCI examination did not distinguish between patients with and without evidence of abnormal supine HR and BP defined by the ISAFSCI criteria as previously reported, 27 -29 parameters of HRV and BPV varied significantly by NLI and AIS classification, respectively. The noninvasive assessment of cardiovascular ANS function using parameters of HRV may be useful in more completely characterizing or stratifying changes in physiology associated with injury, which may have diagnostic, prognostic, or therapeutic significance. 17
In the general population, it is commonly accepted that a lower HRV is associated with increased cardiovascular risk and mortality 30 ; however, this association has not been reported in the SCI population. Interestingly, we found significantly reduced HFHRV, a marker of cardio-vagal modulation, 31 in patients with lesions between T6-T12 as compared with individuals with lesions between C3 and T4, which was an unexpected finding given prior reports of lower HFHRV in those with high cord injuries. 32,33 There were no significant differences in age or TSI between participants with lesions C3-T4 and those with lesions T6-T12 that might explain this finding. We speculate that reduced HFHRV in those with low thoracic lesions may reflect a heightened inflammatory response to recovery from acute injury. 34 Heightened inflammation in people with chronic SCI has been associated with pathological alterations of sympathetic outflow to intact regions, and individuals with low thoracic lesions would be expected to have more intact regions of cardiovascular sympathetic ANS control, which may result in the relatively diminished cardio-vagal modulation. This finding requires further study to confirm and to identify the contributing factors to low cardio-vagal tone during inpatient rehabilitation following traumatic SCI in patients with low thoracic injuries.
Quantification of BPV may be of prognostic and pathophysiological importance, and an association between BPV and cardiovascular complications such as hypertension has been reported. 35 Changes in the Mayer wave frequency of BP (∼0.1 Hz) during a head-up tilt provocation mirrored increases in post-ganglionic neural sympathetic activity in healthy volunteers, 36 and diminished Mayer wave amplitudes has been reported during tilt in patients with SCI at or above T3, compared with those with lower lesions and to uninjured controls. 37 Taken together, these findings suggest that the Mayer wave amplitudes of BP may represent a surrogate marker of sympathetic vasomotor activity, which appears to be absent in those with cervical SCI. 38,39 Our data suggest that, although NLI did not contribute to SBPmayer, patients with complete AIS A lesions had significantly lower amplitudes of SBP oscillations between 0.07 and 0.14 Hz as compared with patients with AIS B/C/D. The difference between our findings and previous reports may be that we did not provide a great enough sympathetic challenge (i.e., tilt maneuver), that the participants were more acutely injured (≤ 6 months from injury) and that the cervical group was comprised of more incomplete lesions (38%) than the thoracic (18%) groups. The association between the clinical evaluation of the neurologic (ISNCSCI) and autonomic (ISAFSCI) injury with sympathetic vasomotor tone (SBPmayer) should be further explored throughout inpatient rehabilitation in persons with SCI.
Clinical perspective
Routine clinical assessment of the degree and extent of ANS impairment following SCI is complicated and limited by the lack of validated assessment tools. The ISAFSCI was developed to fill this gap in clinical assessment capabilities; however, it is relatively new and has not been adequately tested for validity during inpatient rehabilitation following injury. That said, the ISAFSCI does provide clinically relevant information regarding thresholds for ANS impairment that were established by consensus from an international consortium of experts, 16 and while this article focuses only on cardiovascular impairments, the ISAFSCI provides guidance for assessing the presence and degree of ANS impairments to multiple organ systems. Given recent evidence indicating that the degree of ANS impairment (low frequency SBP: 0.5-0.15 Hz), approximately 1 month following injury was related significantly to symptoms of OH and fatigue 12-18 months later, 10 routine clinical assessment should include measurement of global ANS function. Gaining a better understanding regarding the ability of the ISAFSCI to identify patients at risk of ANS impairment will alert clinicians to individual patient needs so that appropriate interventions, such as compression garments, blood pressure medications, or care-giver education, can be initiated to improve long-term outcomes following traumatic SCI.
Study limitations
These data were collected at the bedside in patients with SCI, and while we attempted to control the environment during testing, background noise, room lighting, and temperature were not rigorously controlled. Although only two patients met criteria for neurogenic shock, we recognize that this period of hemodynamic instability is poorly understood and may confound interpretation of the study findings. We did not control for medication use, and acknowledge that the number, timing, and dose of prescription medications use may have influenced the study results in an unpredictable manner. However, these data remain relevant because it is important to understand the impact of the injury, as well as the impact of the clinical management of injury, on cardiovascular ANS function. Finally, there is no “gold-standard” to document cardiovascular ANS control and the utility of the ISAFSCI examination is not currently known, but the expensive equipment and customized software programs that are required to evaluate HRV and BPV limit the utility of these assessments in the clinical setting.
Conclusions
Cardiovascular dysfunction due to impaired ANS control has been reported in patients with SCI during inpatient rehabilitation following injury. The conditions of ANS dysfunction, such as OH and AD, can derail acute inpatient rehabilitation through their sudden and unpredictable onset, which may adversely impact long-term outcomes. While the ISAFSCI did not appear to be sensitive in discerning differences in cardiovascular ANS impairments, determining the relationship between NLI and AIS as assessed on the ISNCSCI, and the degree of ANS impairment during inpatient rehabilitation following SCI will help identify patients at risk of long-term adverse outcomes. Improvements in the clinical assessment of global ANS function, should be prioritized in clinical practice given the importance of regaining ANS control of multiple organ systems to promote health, vitality, and longevity in individuals living with SCI.
Footnotes
Acknowledgments
We would like to thank all the study participants for their involvement in this study.
Funding Information
This project is funded by the National Institute on Disability, Independent Living and Rehabilitation Research Model Systems grant # SI-0158.
Author Disclosure Statement
No competing financial interests exist.