
Abstract
Two multi-contact epineural electrodes were placed around radial and median nerves of two subjects with high tetraplegia C4, American Spinal Injury Association Impairment Scale (AIS) A, group 0 of the International Classification for Surgery of the Hand in Tetraplegia. The purpose was to study the safety and capability of these electrodes to generate synergistic motor activation and functional movements and to test control interfaces that allow subjects to trigger pre-programmed stimulation sequences. The device consists of a pair of neural cuff electrodes and percutaneous cables with two extracorporeal connection cables inserted during a surgical procedure and maintained for 28 days. Continuity tests of the electrodes, selectivity of movements induced, motor capacities for grasping and gripping, conformity of the control order, tolerance, and acceptability were assessed. Neither of the two participants showed general and local comorbidity. Acceptability was optimal. None of the stimulation configurations generated contradictory movements. The success rate in task execution by the electro-stimulated hand exceeded the target of 50% (54% and 51% for patients 1 and 2, respectively). The compliance rate of the control orders in both patients was >90% using motion inertial measurement unit (IMU)-based detection and 100% using electromyography (EMG)-based detection in patient 1. These results support the relevance of neural stimulation of the tetraplegic upper limb with a more selective approach, using multi-contact epineural electrodes with nine and six contact points for the median and radial nerve respectively.
Introduction
In people with tetraplegia, functional electrical stimulation (FES) is, today, the only technology that makes it possible to consider a functional restoration of grasping in cases in which the active muscle resources below the elbows are absent or insufficient to allow surgery for tendon 1 or nerve transfers. 2,3
Similarly to the first implanted electrical stimulation neuroprosthesis Freehand™ (Neurocontrol, Cleveland, USA), 4 the majority of devices using FES directly stimulate sublesional muscles that have retained their innervation and contractility (surface, 5 –7 intramuscular, 8 or epimysial 9 electrodes). They require a high number of internal components, and each muscle must be activated via a dedicated electrode (8 electrodes for the Freehand, 12 electrodes for the second generation Implantable Stimulator Telemeter (IST)-12, 4 and 36 electrodes in a more recent experiment 10 ). Retrospective studies demonstrated good patient compliance with the system and functional usefulness. 11 –14 Unlike epimysial stimulation, direct neural stimulation allows, with a single electrode, to stimulate several muscles that are difficult to reach because they are too close to each other and/or too deep. In addition, it requires less energy, considerably decreases the number of implanted parts, and reduces the risk of complications 15 (infection, failure, and surgical risk through less invasive surgery). Some publications defended the relevance of the neural approach early on. 16,17 This was suggested in a first preliminary study with eight patients. 18 The surgical procedure consisted of placing a multi-contact cuff electrode around the radial or median nerves and observing the effects of neural electrical stimulation. It was applied intraoperatively, in patients undergoing reconstruction of active elbow extension, allowing direct access to the radial or median nerve. The electrodes were left in place for 45 min. For all subjects, it was possible to selectively stimulate muscle groups to open and close the thumb and fingers, to flex and extend the wrist, and to put the forearm in pronation. A second part of the study examined the ability of 17 patients with tetraplegia to use voluntary contractions of supra-lesional muscles (electromyography [EMG] recordings in 8 subjects) or voluntary shoulder movements (inertial sensor recordings in 9 subjects) to control the movements of a robotic hand or to trigger electrical surface stimulation of forearm muscles. All patients were able to master the proposed interface after a short familiarization period. 19,20
Based on the results of these two studies, we aimed to test the functional effectiveness of two multi-contact epineural cuff electrodes, placed around nerves and connected to the stimulator through percutaneous cables. This type of electrode has already shown effectiveness in people with spinal cord injury in stimulating the femoral nerve 21,22 and the phrenic nerve, 23 or in stimulating several nerves of the upper limb 24,25 in people with upper limb amputations 26,27 and in subjects with hemiplegia, to control foot drop. 28,29 The uniqueness of these electrodes in this study lies in the distribution of electrical contacts around the nerve in two rings and a central row of six (radial) or nine (medial) contacts. The stimulator can control the current over the contacts to form virtual electrodes.
The objectives of the study were to study (1) the safety of the surgical and experimental procedures and (2) the ability of these electrodes and associated multi-current stimulation to generate synergistic motor activation and produce functional movements, and (3) to test the control interface (voluntary movements or muscle contractions) allowing subjects to trigger pre-programmed stimulation sequences.
Methods
Participants
Participants received written and oral information at least 30 days before inclusion based on criteria presented in Table 1. The electrodes were placed at Day 0 (D0) and the explantation was performed at D28 leading to the maximum time allowed for a short-term clinical trial (European Medical Device Regulation 2017/745). The study was approved by the ethics committee and health agency.
Demographic and Clinical Data of Both Participants
Inclusion criteria: age between 18 and 65, tetraplegia with a single neurological level ≥ C7, AIS A or B, neurological stability (no change in motor testing for the last 6 months), non-eligibility for tendon transfer surgery, group 0 or 1 (ICSHT classification).
Exclusion criteria: unstable seizure, pacemaker, dermatological problems contraindicating the application of surface electrodes and an electrical mapping identified as negative at the inclusion visit; that is, with muscles rated <4/5 Medical Research Council (MRC).
This mapping was performed using surface electrodes placed on the skin for each muscle or nerve. The CEFAR Physio 4® (Cefar-Compex Scandinavian AB, Sweden) was configured to deliver rectangular currents, at a 30 Hz frequency and a 300 μsec pulse width.
BMI, body mass index; SCI, Spinal Cord Injury; SNL, single neurological level; AIS, American Spinal Injury Association (ASIA) Impairment Scale; ICSHT, International Classification for Surgery of the Hand in Tetraplegia; ZPP, zone of partial preservation; Gr, Group.
Surgical procedure and startup scheme for a neurostimulation program
The two procedures for applying and removing the electrodes are described in detail in Figure 1. The first electrostimulation session was scheduled on the 5th day after implantation. During each session and for each contact, we checked the integrity of the electrodes: impedance was estimated by the ratio of voltage to current at the end of the cathodic phase of a balanced bipolar stimulation between each contact and the proximal ring. Stimulation parameters were set to 60 μA, 300 μs, 4 Hz, five pulses. The first pulse was discarded and the four remaining were averaged. This measurement was performed intraoperatively and then repeated 12 times. It was associated with the estimation of the muscle activation threshold of the medial and radial nerve electrodes using the standard bipolar configuration (i.e., the two outer rings are used, the distal ring as the cathode and the proximal ring as the anode). Both ensured that the electrodes and the stimulator remained within their nominal ranges of impedance (1–10KOhm).

Surgical procedures for the implantation of neural electrodes on the median and radial nerve at Day 0 and explantation at Day 28. The maximum time allowed for a short-term clinical trial is 30 days according to the European Medical Device Regulation 2017/745.
The full device (Fig. 2) combined a pair of multi-contact cuff electrodes, percutaneous cables with two extracorporeal connection cables, and an external stimulator that was connected to a computer. Sensors were fixed on the skin surface to wirelessly collect EMG data from muscle contractions or inertial sensor data related to movements in areas above the spinal cord lesion. For each participant, the two control modes were evaluated.
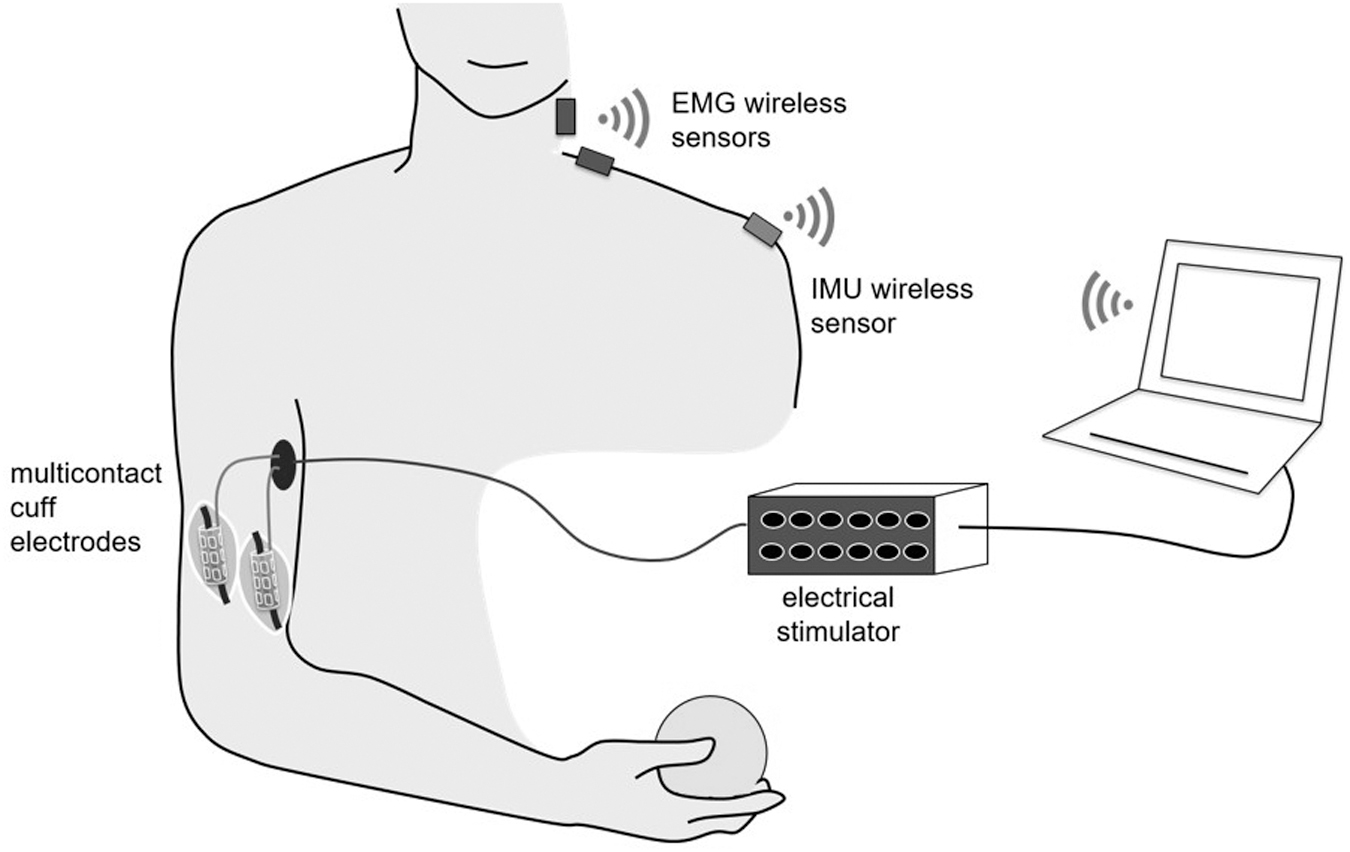
The full device. A pair of multi-contact cuff electrodes and percutaneous cables with two extracorporeal connection cables (CorTec GmbH Freiburg Germany) connected to the external stimulator (STIMEP, Inria, Montpellier, France) which was itself connected to a computer via an optically isolated link. Another system for measuring the electrical behavior of the electrodes associated with the STIMEP has been designed to measure the voltages at the terminals of the electrode contacts and the current delivered. Finally, DELSYS Trigno® sensors (Delsys Incorporated, Natick, USA) were fixed on the skin of the shoulder or neck via an adhesive surface to wirelessly collect and transmit electromyographic (EMG) information from muscle contractions or inertial sensor information related to movements in areas above the spinal cord lesion.
For the EMG modality, the participant produced supralesional voluntary contractions that were captured by surface EMG sensors (Trigno™ Delsys, Natick, MA). The EMG signal was rectified and low pass filtered (6 Hz low-pass Butterworth, 4th order) to extract the envelope. A threshold was set for each EMG sensor envelop on each muscle. For inertial measurement unit (IMU) modality, the participant performed pre-defined movements with his or her contralateral shoulder that were captured with inertial sensors (Trigno). A classifier algorithm was implemented to detect pre-defined shoulder movements (upward, backward, forward movement).
A finite state machine (FSM) was defined to associate user commands (EMG threshold detection or recognition of a pre-defined movement) with actions depending on the current FSM state. The detection of a contraction threshold or a stereotyped movement triggered the corresponding stimulation pattern.
Eight out of nine inner contacts on the median nerve electrode (the ninth not being in contact with the nerve because the nerve diameter was smaller than the nominal diameter of the electrode), and six inner contacts on the radial nerve were explored for each patient (Fig. 3). The stimulator (STIMEP, INRIA, Montpellier) provided a rectangular symmetric biphasic balanced current profile (100 μs interpulse, 25 Hz stimulation frequency and a 250 μs pulse-width for all sessions). The specific feature of the stimulator is that it can provide a distributed current with programmable ratios between several contacts. Preliminary theoretical and pre-clinical studies 33,34 were used to select three optimal configurations. The configurations used a single cathodic inner contact and the anodic currents ratios were defined as follows: tripolar longitudinal ring (TLR) 50% on the two outer rings, steering ring (STR) 25% on the two outer rings, 50% on the inner contact opposite to the cathodic one, and transverse tripolar ring (TTR), 25% on the two outer rings and on the two inner contacts adjacent to the cathodic one. The targeted area (therefore the targeted muscles) were modulated both by the inner contact selected as the cathode and the “configurations” of the current distributions (from TLR the least selective to TTR the most selective).
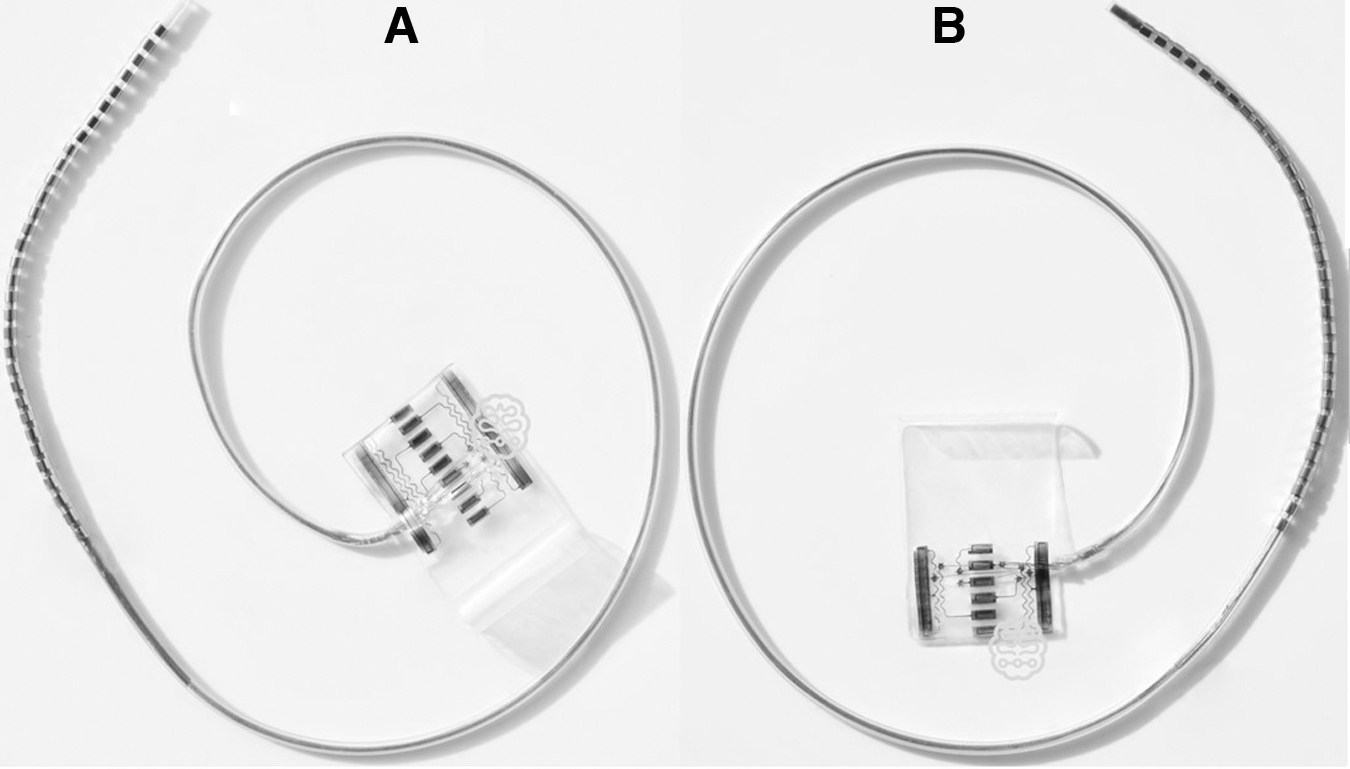
Nerve electrodes (CorTec GmbH Freiburg Germany): 2 cm long, inner contacts (2.4 × 0.8 mm2, 2.4 mm orthoradial spacing) and external rings are made of 90/10 Pt/Ir alloy embedded with silicone.
At the beginning of each week, each of these configurations was scanned in 20 μA steps –TLR, STR, TTR with six and eight cathode positions for the radial and median nerve respectively – which led to 42 scans for each patient. However, to limit full scan of current amplitudes, and therefore fatigue and scan time, we observed the movements produced with TLR only and selected cathode positions that showed sufficient fingers opening to grasp all presented objects during radial nerve stimulation and cathode positions that induced a balanced and strong fingers closure, rated 4/5 on the medical research council (MRC) scale during median nerve stimulation. For each, the current intensity was specified. Finally, the STR configuration on the selected cathode was explored to further improve the functional outcome. The TTR configuration was never selected because of too-high thresholds.
Post-implantation monitoring and evaluation methods
Local signs and pain around the electrode implantation site (allergy, local infection, electrode disinsertion) were investigated daily.
The maximum strength of each muscle, produced by the stimulation of each nerve, was evaluated by extrapolation with reference to the MRC scale. The selectivity of the stimulation configurations was based on the quality of the induced movements (finger opening, palmar grip, and key grip without antagonistic movement of the wrist) and on the intensity thresholds; that is, the minimum current intensity necessary to produce them.
The weekly functional assessment – Supplementary Text S1 The Motor Capacities Scale (MCS), which is an arm/hand function test specifically designed and validated for patients with tetraplegia who underwent a tendon transfer surgical procedure.
30,31
The grid includes three sub-categories: A, B, C (right hand) and/or D (left hand). Only MCS-C or D items were assessed using a four-point scale. The expected score was a minimum of 36/72. The evaluation was performed in a controlled environment, set up with a table height of 75–80 cm. The patient is facing the table. The reference objects used in this scale were for the analysis of two basic prehension gestures most often performed by the tetraplegic patient: the key-grip and the grasp. The objects were chosen from objects that the patients use in their daily lives. Each type of prehension involved three steps: grab, hold, and release. A score was available for each of these three steps. The ergonomic adaptation (non-slip support, lightweight foam handled cutlery) of the objects was allowed and considered in the score. The target of 50% for the MCS-C or D score was chosen on the basis of the progression of motor skills observed in patients with tendon transfers with ∼15% functionally significant variations.
31
The Constraint Acceptability Questionnaire was designed for this study to invite the participants to share their experience and the possibility of using such a device if it was permanently implanted. The total score was defined as the sum of the answers to the 13 questions asked (with a minimum score being 13 and a maximum score being 65). The objective was a score of at least 49/65 (acceptability rate of 75%) In the evaluation of finger opening and closing control using EMG and IMU, both sensing modalities were explored in each participant. For EMG modality, two sensors were placed on two residual active muscles, whose contraction triggered either opening or closing of the fingers. For IMU modality, one inertial sensor was placed on the shoulder to detect two pre-defined movements triggering either opening or closing of the fingers. For each modality, 10 pre-determined and random instructions (opening or closing the fingers) were given by the examiner. The test aimed to estimate how many of the 10 muscle contractions detected by EMG and 10 movements detected by IMU led to the expected outcome (opening or closing of the fingers). A percentage of success was calculated. The compliance target was at least 90% for each modality, corresponding to the ability of the patient, in at least 9 cases out of 10, to follow the right command to open or close the fingers in accordance with the instruction given by the examiner. We conceded a 10% margin of error for each modality of control. An error could correspond to different cases: (1) the patient selected the wrong shoulder motion/muscle contraction or (2) the patient selected the right shoulder motion/muscle contraction but the detection algorithm failed. In both cases the induced movement did not correspond to the expected one. The safety of the technique was validated at the end of the experiment at D45 by the absence of any general and local complications.
Results
The demographic and clinical data of the participants included in the study are presented in Table 1.
Surgical procedures
Electrode implantation
In patient 1, surgical exposure of the median nerve during electrode placement revealed an anatomical variation characterized by a supra-epitrochleo-olecranial exostosis associated with fibrous covering and enclosing the median nerve. Resection of the exostosis and fibrous tract was performed to expose the median nerve over a length of 5 cm. The electrodes were gently placed around the nerve and self-adapted to the actual diameter. No further suture or fixation was needed.
Electrode explantation
In both cases, the electrodes were removed without any difficulty. In patient 1, an impression of the electrode on the radial nerve was observed with no apparent effect on perineural vascularization. Similarly, the impression on the medial nerve gave the image of a “reddish tattoo” of the stimulation plates on the nerve. A small shrinkage along the length of the electrode was noticed. The same observation was made for the median and radial nerves of patient 2 without alteration of the nerves' trophicity. An anatomo-pathological sampling of the perineural neocapsule around the electrode of the two nerves revealed a simple inflammatory fibro-conjunctive tissue without malignant transformation.
Total procedure duration
The procedure duration (from approach to final suture) was 114 and 100 minutes for implantation for patients 1 and 2 respectively, and 60 and 57 minutes for explantation, respectively.
Electrical continuity of the electrode contacts
The continuity tests – Supplementary Text S2 – highlighted the consistency and quality of each of the electrodes' contacts. Two contacts were detected during the implantation as having too high an electrical impedance (suspicion of a breakage even though the current could still flow through the contact), later confirmed with a post-implant analysis. This analysis revealed a very small break of the conductive metal in the electrode for these two contacts, but the break was small enough for current to flow. However, to maintain reliable results, data from these two contacts are not reported and were discarded from the analysis. While the electrodes were in place, no other failures occurred and the impedances remained stable. Finally, the contact nine of the two electrodes placed on the median nerve showed a slightly higher impedance, but one that was within the accepted range, confirming that it was not in contact with the nerve but in contact with the silicone located underneath (more than one turn of the electrode around the nerve).
General and local postoperative tolerance
Neither of the two participants showed general comorbidity. Patient 2 revealed a suppuration point around the cable exit port of the radial nerve at D23. General antibiotics were initiated before the removal of the electrodes and cables at D28. Three bacteriological samples taken when the electrodes were removed were negative. It was the same patient who presented, after the electrode explantation, a hematoma of the anterior compartment of the arm, which was non-compressive and resolved spontaneously in a few weeks. Platelet aggregation inhibitors, maintained intraoperatively because the patient had a history of traumatic vertebral artery dissection, contributed to this hematoma. No patient reported pain related to the presence of the device.
Acceptability of the constraints related to the different stages of the experiment
The total acceptability score is evaluated on 65 points (Fig. 4). As the last question of the questionnaire was not applicable for patient 1, his score was evaluated on 60 points and remained at a higher level throughout the experiment. Out of a total of 65, a point drop in the score was observed at D15 for patient 2.
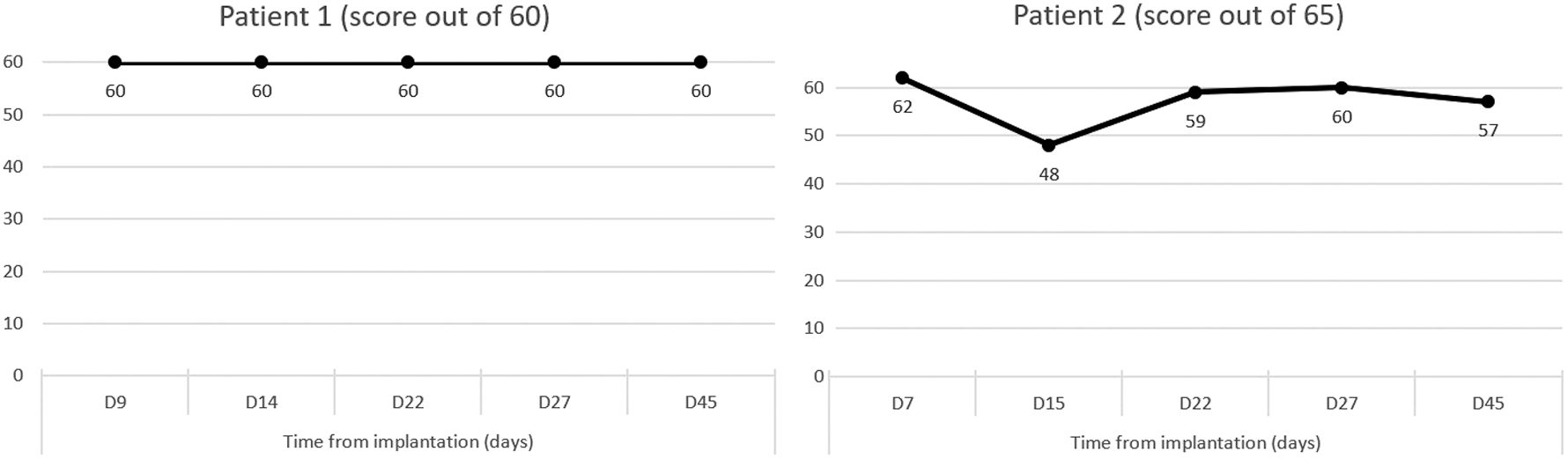
Acceptability total score.
MRC muscle strength produced by electrostimulation
Analytical testing of the maximum muscle strength generated by non-selective electrostimulation revealed the absence or inconsistency of individualization of AbP contraction in patients 1 and 2 respectively (Fig. 5). In both patients, all other muscles – except the pronator teres – were rated at least 4/5 MRC at D27.
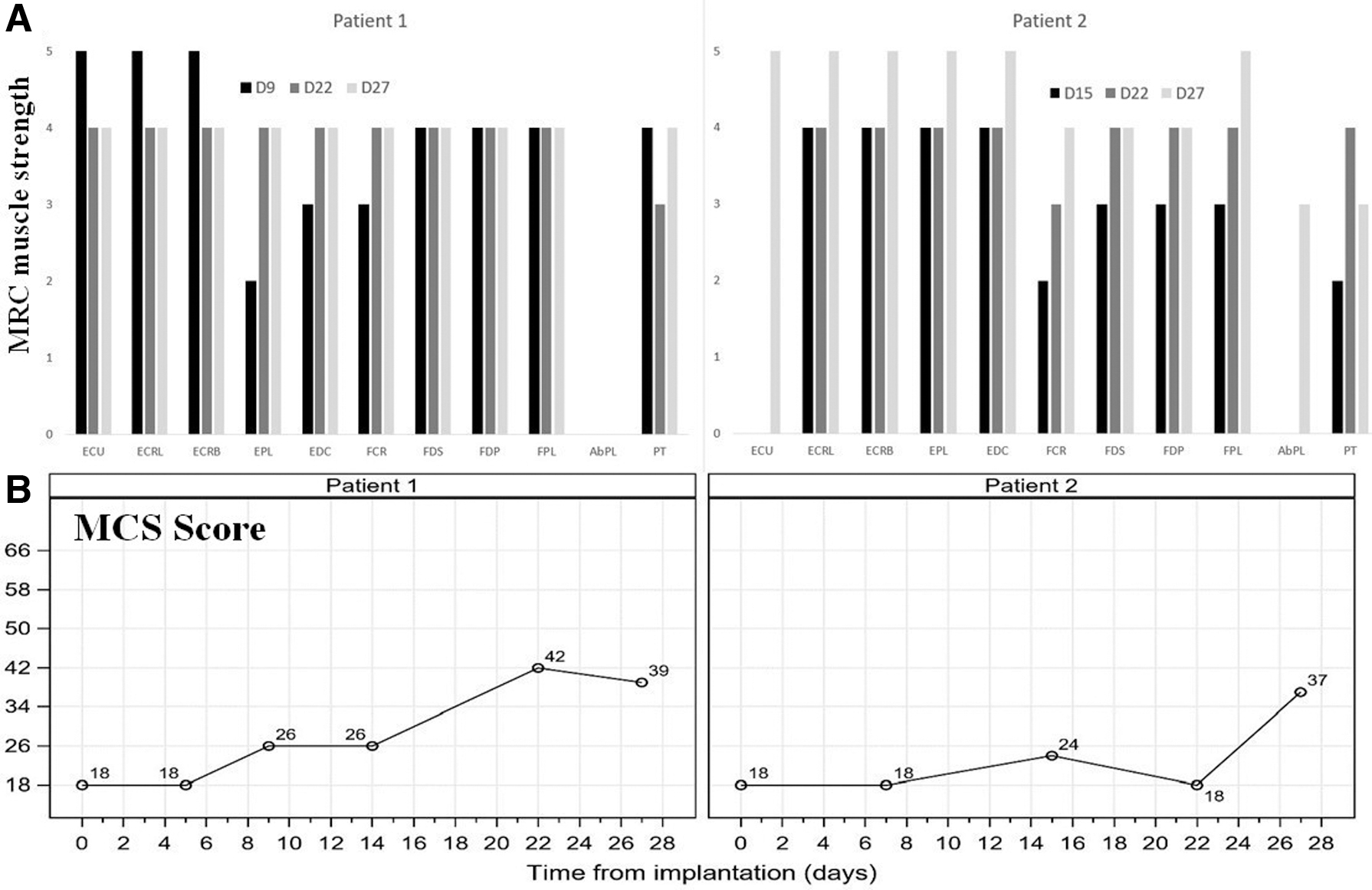
Maximum muscle strength (MRC) produced by electrical stimulation of the median and radial nerve (
Selectivity of movements induced by electrostimulation
Tests confirmed the ability of the electrodes to produce multiple movements (Table 2). In patient 1, the configuration TRL 7 offered a reproducible active key-grip in terms of kinematics and strength with intensity from 450 to 580μA. TRL 1 showed a reproducible digito-palmar grasp with an intensity varying from 350 to 500μA. In patient 2, TRL 6 induced a digito-palmar grasp with the same intensity as 380μA. Few other configurations/cathode positions generated the same movement, highlighting the possibility of obtaining the same result through different contacts (e.g., for opening the fingers, TRL3 and TRL4 in patient 1, TRL2 and STR2 in patient 2). The same was true for the key-grip and the palmar grasp with thumb for patient 2. The expected finding was that none of the stimulation configurations generated contradictory movements.
Movements Induced by Nerve Electrostimulation: Selectivity Tests
D, day; TLR, tripolar longitudinal ring; STR, steering ring; I, intensity; PW, pulse width; F, frequency.
Motor capacities for grasping and gripping
Without stimulation, no hand opening and closing function was possible and both participants were completely dependent on a third person for any grasping task. With the stimulation, the MCS-C score rose progressively from D9 for patient 1 and abruptly at D27 for patient 2, with two scores of almost equal level at D27 (39/72 for patient 1 and 37/72 for patient 2) (Fig. 5). Table 3 details the grasping and gripping modalities at D27 and emphasizes the importance of the associated wrist orthosis (Supplementary Video). During this experiment, the adaptation of the objects to be grasped (thickening of a cutlery or application of an anti-slip surface, for example) or the use of technical aids on the market or 3D printed were produced.
Total Motor Capacities Score for Grasping and Gripping on Day 27
Control commands (EMG detection and motion capture using IMU)
In Patient 1, EMG muscle contraction detection and IMU motion detection compliance were optimal, at 100% and 97.5% respectively (Table 4). For patient 2, EMG detection of neck muscles was not possible. Therefore, only motion detection compliance with the examiner's instructions was studied, revealing a success rate of 90%. As the participant felt muscle fatigue, we also tested a head control (a push button) that offered good reactivity in the transmission of commands, but required a retropulsion effort on the head that prevented visual control of the object to be reached. The participant is waiting for a voice control solution.
Control Commands (EMG Detection and Motion Capture Using IMU): Fingers Opening and Closing in Response to 10 Control Orders Delivered by the Examiner
D, day; EMG, electromyography; IMU, inertial measurement unit; ESS, external surface stimulation (dorsal and ventral face of the left forearm); INS, implanted neural stimulation; NT, not testable; C, compliant; NC, not compliant.
Discussion
As the Freehand device is no longer marketed, no solution has emerged to meet the expectations of patients with high tetraplegia. The experience gained by our team on the Stand Up And Walk (SUAW) project 32 has allowed us to validate the relevance of neural electrodes, >10 years after the implantation of a lower limb stimulation neuroprosthesis. In this previous work, a classical bipolar stimulation was used – selectivity was obtained by activating the fascicle to be stimulated during surgery – the “stability” of the neural electrodes compared with the epimysial electrodes proved to be much better in terms of both stimulation threshold and impedance variation. These findings encouraged us to favor neural stimulation on the upper limb with a more selective approach, using multi-contact cuff electrodes. Preliminary studies made it possible to optimize the design of the electrodes so that their diameter could be adapted to that of the nerve. 18,33,34
This experience has shown that the risks, especially infectious ones, can be controlled by daily monitoring. Comorbidity was found to be only local and had no effect on the functioning of the electrodes, the state of the nerves, and the patient's health. After explantation of the electrodes, a check of the muscular contractility in the territory of each of the two nerves confirmed the absence of deterioration of nerve conduction. It has also answered the expected promises of functional and useful electrostimulation. The success rate in tasks execution by the electro-stimulated hand was estimated using MCS-C score at 54% for patient 1 and at 51% for patient 2, exceeding the target of 50% planned for this project. Because patients in group 0 have significant deficits in active shoulder mobility and, to a lesser extent, in elbow flexion, the question arises as to whether to include patients unable to carry the arm at shoulder level and the hand at face level. This choice would unfortunately deprive group 0 patients who could use their electro-stimulated hand while using an electrical assistance device to control the arm and elbow. Patient 2's acceptability and adherence to this experiment was marked by a moment of discouragement at D15 linked to difficulty in positioning the forearm correctly. Difficulties in proximal control of the arm were also associated with the problem of control related either to muscular contractions or to movements in the areas above the lesional level. The reactivity of the induced movements led patient 1 to prefer EMG detection of small contralateral contractions of the platysma and upper trapezius muscles. Patient 2, however, was not able to offer the expected contractions. The muscles above the lesion were obviously not paralyzed. However, the muscle contraction proved to be insufficient to produce an EMG signal with a sufficient signal to noise ratio to be reliably detected. The learning and training time may have been too short to achieve this, as the patient had lost the habit of contracting the neck muscles, leading to early fatigue. Despite a satisfactory success rate in controlling the electrostimulated hand by contralateral shoulder movements, the repetition of shoulder movements was tiring.
Epimysial electrostimulation has the advantage of producing a muscle-by-muscle adjustment but, compared with direct neural stimulation, it requires higher stimulation intensities and faces greater difficulty in distributing and balancing the stimulation over several agonist muscles. Fascicular neural stimulation is, in theory, easier to adjust. The experience of this study contradicts the rule. The main issue was the difficulty in maintaining the wrist in extension – and not in flexion – while the finger flexors were tightened around an object (without an object, the wrist managed to maintain itself in extension). It was this observation that led us to believe that it was only a problem of synergy adjustment. This was also the reason why the wrist was stabilized in an orthosis. In other words, how to adjust the balance between wrist extension on the one hand and strong finger flexion on the other? It is necessary to rely on a finer adjustment of the different movements, which was not possible with the version of the software that was used.
Although the benefit–risk balance promises to be favorable, neural electrostimulation may not be enough. Following the example of the “Freehand,” additional surgical procedures appear to be unavoidable: (1) stabilization procedures of the thumb and the metacarpo-phalangeal joints, (2) deformity correction surgery (forearm pronation or supination osteotomy), and (3) reconstruction of active elbow extension. The objective would be to propose minimal reconstructive surgery in order to prepare the global positioning of the upper limb in its approach to the object. Moreover, during this experiment, the adaptation of the objects to be grasped proved to be essential. When the challenge is to allow a reliable and useful grasp and grip, technical complements become indispensable.
Study limitations and perspectives
Although this case study is encouraging, it does not allow for any generalizations and, above all, it allows for no hasty conclusions. On the basis of the present results and those of the previous studies cited, it suggests that multi-contact neural cuff electrodes could offer individualized and reproducible fascicular stimulation. The experimental duration of 1 month, judged too short not only by the patients but also by our teams, to better accompany the learning, has been imposed by the regulations. However, this study was a critical step to demonstrate feasibility.
Our future working hypothesis aims to consolidate the proof of concept that multipolar neural electrical stimulation of the median nerve (flexion), radial nerve (extension), and ulnar nerve (proximal flexion and distal extension of the fingers) allows for useful grasps of standardized and participant-selected objects. The inclusion of the ulnar nerve in the future stimulation strategy seems interesting, because electrostimulation of this nerve would offer better stability of the metacarpophalangeal joints during finger opening, and a reinforcement of the distal flexion of the fingers as well as of the commissural component of the key grip. In this context, all the conditions would be met to extend the inclusion criteria to patients in groups 1 and 2 of the International Classification for Surgery of the Hand in Tetraplegia (ICSHT) classification, who would have the advantage of better control of their ipsilateral shoulder and elbow.
With respect to the new european Medical Device Regulation (MDR) 2017/745, European regulation, it is more relevant to go through a short-term use (30 days) to avoid a too-complex regulation pathway while providing a higher proof of clinical relevance. The final stage is already being prepared for a complete, long-term implanted system that requires at least 2 years of development and certification and should be ready in 2024.
Footnotes
Acknowledgments
The authors acknowledge the two patients and therapists, Marie-Anne Caralp and Marianne Porra (occupational therapist [OT]), and Isabelle Panel and Audrey Ferrer (physical therapist [PT]) as well as the healthcare teams in charge of day-to-day care. They also acknowledge Arthur Hiairrassary (engineer) for his contribution to the design and the development of the software. Finally, they acknowledge the sponsor Assistance Publique Hôpitaux de Paris (Délégation à la Recherche Clinique et à l'Innovation).
Funding Information
This study was supported by a grant from Innovation Programme of the European Institute for Innovation and Technologie (EIT Health) (grant number 20682 Agilis, 2020), Region Occitanie, Marie Curie grant.
Author Disclosure Statement
David Guiraud and David Andreu are shareholders of NEURINNOV company. No competing financial interests exist.
Supplementary Material
Supplementary Text S1
Supplementary Text S2
Supplementary Video
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.