
Abstract
In this study, we investigate the association of serum calcium with coagulopathy and hemorrhagic progression contusion (HPC) in patients with traumatic intraparenchymal hemorrhage (tIPH), and further explore the interaction and mediation effect between serum calcium and coagulopathy on HPC. We conducted retrospective analyses of patients with tIPH admitted to the First Affiliated Hospital of Wenzhou Medical University between January 2016 to December 2019. The clinical data, coagulation parameters, and serum calcium levels were collected for further analysis. Multi-variate logistic regression analysis was applied to identify the association of serum calcium level with coagulopathy and HPC. Causal mediation analysis (CMA) and additive interaction model were used to estimate the interaction and mediation effect between serum calcium as well as coagulopathy on HPC. Additionally, we repeated the analysis using corrected calcium. A total of 473 patients were included in this study. Of these, 54 (11.4%) patients had hypocalcemia at admission, 105 (22.2%) presented with coagulopathy, and 187 (39.5%) experienced HPC. Admission serum calcium level in patients presented with coagulopathy and HPC were 8.84 (interquartile range [IQR]: 8.44-9.40] and 8.92 (IQR: 8.48-9.40) mg/dL respectively, which were significantly lower than that of patients without coagulopathy (9.10 [IQR: 8.68-9.88] and 9.12 [IQR: 8.72-9.89] mg/dL; all p < 0.001). Multi-variate logistic regression analysis identified that hypocalcemia emerged as an independent risk factor for coagulopathy and HPC. However, no significant interaction was detected between hypocalcemia and coagulopathy. CMA showed that the mediator coagulopathy explained 24.4% (95% confidence interval: 4.7-65.0%; p = 0.006) of the association between hypocalcemia and HPC. Moreover, comparable results were held using corrected calcium, as well. Admission serum calcium level is associated with the HPC for patients with tIPH and this relationship is partially mediated by coagulopathy, but no significant interaction is detected. Further studies are needed to validate the findings and explore its mechanisms.
Introduction
Traumatic brain injury (TBI) has been recognized as a public health problem in the world, causing a huge burden to society and families. According to the most recent data from the Global Burden of Diseases, 1 more than 10 million people worldwide experience TBI resulting in hospitalization or death each year. Among variants of TBI associated pathologies, traumatic intraparenchymal hemorrhage (tIPH) is one of the most common injury types. 2,3 It is markedly associated with a high risk of coagulopathy and hemorrhagic progression of contusion (HPC), and leads to an increased risk of death and disability. 4 -6 In a systematic review of the literature on the contusion progression following TBI, Adatia and colleagues 7 found that 16-75% of patients with tIPH experience HPC in subsequent computed tomography (CT) imaging. Therefore, early identification of patients at high risk for HPC could lead to interventions that reduce the long-term disability and mortality of tIPH patients.
A large amount of evidence has suggested that serum calcium is an essential cofactor for the coagulation cascade and involved in platelet function. 8 -10 In the context of spontaneous (non-traumatic) IPH, low serum calcium level has been associated with impaired hemostasis and leads to an increased risk of hematoma expansion. 11 -13 In addition, hypocalcemia may contribute to hematoma progression through increased arterial vascular tone and greater blood pressures (BP). 14,15 However, to our knowledge, the association between serum calcium level with coagulopathy and HPC in patients with tIPH have not been investigated at all. Further, given the links between calcium level, hemostatic mechanisms, and hematoma progression found in previous studies, 8 –15 it seems reasonable to hypothesize that coagulopathy mediates the association between hypocalcemia and HPC in tIPH patients. On the other hand, a possible interaction effect between hypocalcemia and coagulopathy may occur when they act together in causing HPC.
Therefore, this study aimed to investigate the association between serum calcium level and HPC as well as coagulopathy as a mediator and its interaction with hypocalcemia on HPC, which can provide a new insight to TBI management and improve early identification for high-risk patients of HPC. To simplify assessment, patients with mainly tIPH were included in the analysis because it may have the higher likelihood with spontaneous IPH. 16,17
Methods
Ethics statement
The study was approved by the Ethics Committee in Clinical Research of First Affiliated Hospital of Wenzhou Medical University (No. 2020-zz-141). All procedures performed in our study were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this retrospective study, the need for written informed consent was waived. The study proposal was also registered with Chinese Clinical Trial Registry, and its registration number is ChiCTR2100046571.
Patient population
We retrospectively analyzed consecutive tIPH patients admitted to the First Affiliated Hospital of Wenzhou Medical University, Zhejiang province, China, between January 2016 and December 2019. Inclusion criteria were listed as follows: 1) adult patients (age >18 years) having isolated TBI without severe injury to other regions (an extracranial Abbreviated Injury Scale [AIS] score <3); 2) arrival at the emergency department within 8 h after trauma and the initial head CT completed immediately after admission; 3) patients with mainly a tIPH on CT who do not combine remarkable acute subdural or epidural hematomas (thickness >5 mm and/or volume >10 mL); and 4) one or more repeat head CT scans were conducted to determine the HPC within 24 h after admission. Exclusion criteria were listed as follows: 1) decompressive craniectomy affects HPC progression via a putatively distinct biology from an intact cranium 6 and we therefore a priori excluded those patients with early craniectomy before follow-up CT scan; 2) since we were interested in the progression of tIPH, patients who presented with enlargement of extradural hemorrhage (EDH), subdural hemorrhage (SDH), or subarachnoid hemorrhage (SAH) also were excluded; 3) the contusion was located in a deep structure (the diencephalon, brainstem, or cerebellum); 4) penetrating brain injuries (gunshot or stab wound); 5) known coagulation disorders, such as thrombocytopenia, liver failure, deep venous thrombosis, and myocardial infarction; 6) use of anticoagulant or antiplatelet agents (clopidogrel, aspirin, and coumarin, and others) ; and 7) the absence of the availability of results of coagulation testing or CT image data.
Patient management and CT scans
According to the well-established guidelines for the management of TBI, tIPH patients were standardly evaluated and treated. 18,19 Briefly, all patients underwent a careful neurological evaluation, and head CT scans were routinely performed at admission, and they then received initial fluid resuscitation. Subsequently, the neurological status and CT image were evaluated to determine whether emergency surgery should be performed. Repeat brain imaging were routinely performed within 24 h after the initial scan or when the patients exhibited clinical deterioration. During conservative therapy, clinical deterioration was defined as a reduction in Glasgow Coma Scale (GCS) score of ≥2 points that was not attributable to sedation. 20,21
Data collection
Demographic and clinical characteristics
The files of tIPH patients were reviewed. Then, the following demographic and clinical data were collected: patient's age, sex, smoking, drinking, and comorbidities (hypertension, diabetes mellitus [DM], coronary artery disease [CAD] or others); mechanism of injury (traffic accident, fall or others), admission GCS score; baseline BP; and time from injury to first CT scan. Smoking in participants was defined as one cigarette or more per day for up to 1 year. Drinking was defined as consumption of at least 50 mL of white spirits at one time and having a drink at least once a week for >6 months. Histories of hypertension, DM, CAD, and other comorbidities were self-reported and confirmed by their family members.
Coagulation parameters and serum calcium level
Upon arrival to the emergency room, the following parameters of coagulation were collected and examined: platelet count (PLT), prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (APTT), and fibrinogen level (FIB). To obtain comparable hazard ratios for the relationships, we rescaled each variable as follows: PLT <100 × 109 to ≥100 × 109/L; INR ≤1.25 to >1.25; PT ≤14 to >14 sec; APTT ≤36 to >36 sec; and FIB <2.0 to ≥2.0 g/L. 22,23 Coagulopathy was defined as one or more of the following: PLT <100 × 109/L; INR >1.25; PT >14 sec; APTT >36 sec; and/or FIB <2.0 g/L. 22 -24 Further, white blood cell (WBC), blood glucose, and serum calcium levels were measured and recorded.
Hypocalcemia on admission was defined as a total serum calcium level of less than 8.4 mg/dL (to convert to millimoles per liter, multiply by 0.25). 12 The serum calcium measurements can underestimate the presence of hypocalcemia. 12,25 We therefore repeated the analysis using corrected calcium based on the serum albumin values, which was calculated as follows: corrected calcium (mg/dL) = serum calcium (mg/dL) +0.02 × (4.0 - albumin [g/dL]). 26 Previous studies showed that corrected calcium more accurately reflects the physiologically active component of serum calcium. 12,25,26
Radiological variables
All CT scans were evaluated by two independent neurosurgeons and a consultant radiologist for contusion and all associated intracranial injuries. The following radiological data were collected and analyzed, including the number of contusion lesions, the morphological pattern, hematoma volume, and the presence of other post-traumatic intracranial injuries (EDH, SDH, SAH, or others). 27,28 We defined tIPH as traumatic intraparenchymal hemorrhagic lesions whose morphology can vary from mixed hyperdense areas to those with a well-defined and solid appearance (hematoma). 4,29 Petechial lesions with the typical radiological pattern of diffuse axonal injury were not considered tIPHs. According to the morphological pattern of the presentation of tIPH, we distinguished two groups: solid or homogeneous pattern and mixed pattern. 28,30
Hematoma volume was assessed with 3D Slicer (Surgical Planning Laboratory, Harvard University, Boston, MA) software. 5,31 Briefly, the region of interest was manually selected and automatically separated from the environment via software based on a fixed threshold in Hounsfield units (HU). The isolated regions were visually inspected and manually adjusted to ensure that the hemorrhage was visible in all three projections. Adjacent voxels were automatically summarized, which provided the hematoma volume, by using a threshold value (a fixed window of 100 and 50 HU) for distinguishing hematomas from the surrounding. When multiple tIPHs were present in the contusion region, the total volume was calculated. In relation to their size, we recorded whether the initial volume was more than 5 mL, as previously described. 4,28,30,32 An HPC defined as the appearance of new lesions or a conspicuous increase in the size of hemorrhagic lesions (i.e., a relative growth of ≥25 % or absolute hematoma growth of ≥5 mL on the repeat imaging), according to previously published studies. 5,33
Statistical analysis
Statistical analysis was performed using SPSS 25.0 (IBM, Armonk, NY) and R software (MathSoft, Cambridge, Massachusetts). A two-sided p < 0.05 was considered statistically significant. Continuous variables were presented as means (standard deviations [SDs]) or median (interquartile range [IQR]) according to the distribution of the variables, and which were analyzed by independent t test or Mann-Whitney U test. Number (n) and percentage (%) were computed for the categorical variables, comparisons between groups were performed by the χ 2 test or Fisher exact test. The associations of serum calcium level with coagulation parameters, admission BP and hematoma volume were assessed with the Spearman test. Propensity score (PS) matching (1:3 match, caliper 0.2) was performed to adjust the imbalances of covariates among hypocalcemia and normocalcemia patients.
Analyses of coagulopathy and HPC were conducted in the PS-matched cohort, account for 50% of all cases. Multi-variate logistic regression analysis was performed to determine factors that could be considered as independent predictors of the coagulopathy and HPC, adjusted by confounding variables according to the results of the univariate analysis. Variables with two-sided p values of ≤0.10 in the univariate analysis were included in the model; odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Receiver operating characteristic (ROC) curves were used to determine the predictive value of serum calcium level for HPC. To assess whether the serum calcium would add discrimination ability to the established model, we analyzed the difference in the area under the ROC curve (AUC) of the three models according to the method suggested by Hanley and McNeil. 34
We hypothesized that hypocalcemia has an interactive effect with coagulopathy on HPC, an additive model was used by cross analysis to calculate the interaction. In addition, the following interactive indicators were calculated, including the relative excess risk due to interaction (RERI), the attributable proportion due to interaction (AP), and the synergy index (SI). At last, CMA was used to investigate whether the effect of hypocalcemia on the HPC event is proportionally mediated by the coagulopathy. CMA is a method to decompose the total effect of variable into direct and indirect effects. In this method, the hypocalcemia as the exposure (X), coagulopathy as the mediator (M), HPC as the outcome (Y), and the previously known predictors as the prespecified covariates. To perform mediation analysis, it is necessary to test three pathways: 1) X is associated with the Y (Fig. 1, pathway c); 2) X is associated with the M (Fig. 1, pathway a); 3) M is associated with the Y after adjusting for X (Fig. 1, pathway b). If all three associations are confirmed, mediation (indirect effect) can be established in a fourth step through estimation of the direct causal relationship (Fig. 1, pathway c′). The average causal mediation effect (ACME) and average direct effect (ADE) were estimated using nonparametric 1000 bootstrapping.
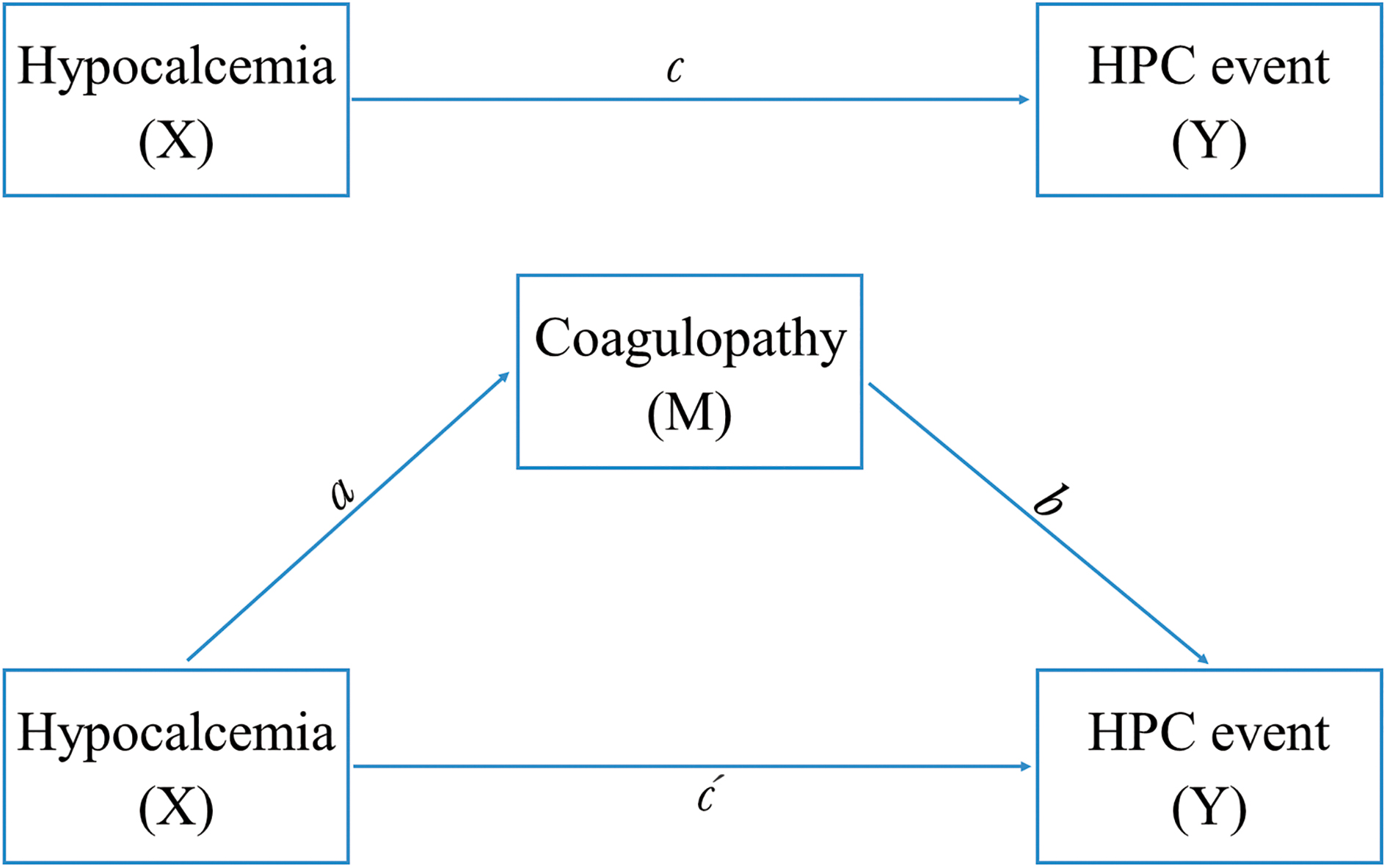
Framework of mediation analysis. HPC, hemorrhagic progression of contusion.
Results
Patients' characteristics
A total of 975 tICH patients met the inclusion criteria. Among them, 502 cases were excluded due to a variety of reasons. Ultimately, 473 valid tIPH patients were included in our study (Fig. 2). There were 278 (58.8%) male and 195 (41.2%) female patients. The median age of patients was 52 years (IQR: 44-60 years), and the median baseline volume of the tIPH on the initial CT scan was 7.09 mL (IQR: 3.83-12.06 mL). The characteristics of the patients were presented in Table 1.
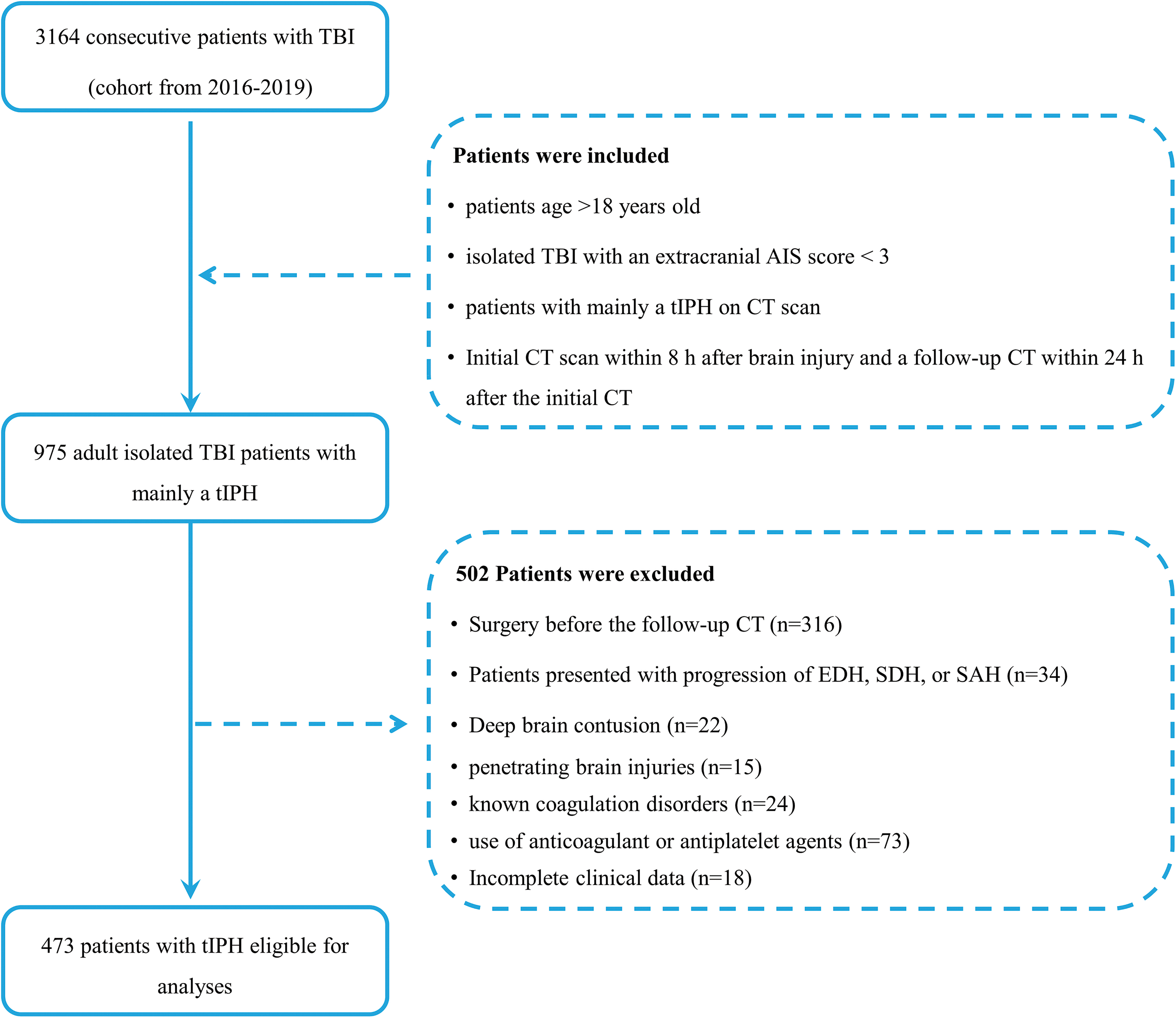
Flow diagram of the patients in this study. TBI, traumatic brain injury; AIS, Abbreviated Injury Scale; tIPH, traumatic intraparenchymal hemorrhage; CT, computed tomography; EDH, extradural hemorrhage; SDH, subdural hemorrhage; SAH, subarachnoid hemorrhage.
Characteristics of the Study Population (n = 473)
Data are expressed as n (%), mean ± standard deviation, or median (interquartile range), as appropriate.
It contains hyperlipidemia, chronic kidney disease and pulmonary disease.
It contains stumble, assault, and hit by falling objects.
It contains intraventricular hemorrhage, skull fracture, and pneumocephalus.
Percentage of hypocalcemia stratified according to serum calcium level.
Percentage of hypocalcemia stratified according to serum corrected calcium level.
SBP, systolic arterial pressure; DBP, diastolic arterial pressure; MAP, mean arterial pressure; CT, computed tomography; tIPH, traumatic intraparenchymal hematomas; EDH, extradural hematoma; SDH, subdural hematoma; SAH, subarachnoid hemorrhage; WBC, white blood cell; PLT, platelet count; PT, prothrombin time; INR, international normalized ratio; APTT, activated partial thromboplastin time; FIB, fibrinogen; HPC, hemorrhagic progression of contusion.
Association of serum calcium level with coagulation parameters, BP and hematoma volume on admission
Spearman's correlation indicated that a weak, albeit significant, association existed between serum calcium level and coagulation markers (PLT: r = 0.470, p < 0.001; INR: r = -0.286, p < 0.001; PT: r = -0.440, p < 0.001; APTT: r = -0.262, p < 0.001; FIB: r = 0.453, p < 0.001). In contrast, there was no significant correlations of serum calcium level with BP and hematoma volume on admission (SBP: r = -0.035, p = 0.450; DBP: r = -0.021, p = 0.648; mean arterial pressure: r = -0.033, p = 0.479; hematoma volume: r = -0.018, p = 0.690).
Subsequently, patients were dichotomized into normocalcemia and hypocalcemia groups. Further investigation showed patients with hypocalcemia on admission had significantly higher INR, PT, and APTT, and lower FIB and PLT counts compared with normocalcemia patients. Regarding the end-points, patients with hypocalcemia experienced the coagulopathy and HPC more frequently (p < 0.05). Additionally, patients with hypocalcemia had worse clinical status on admission and a greater level of SBP, hematoma volume, and blood glucose in the unadjusted analysis. To account for confounding bias between patients with hypocalcemia versus normocalcemia, PS matching was performed, after which two evenly balanced cohorts were available for analyses of coagulopathy and HPC (Supplementary Figs. S1 and S2). Interestingly, the proportion of patients with coagulopathy and HPC were significantly higher among hypocalcemic patients as well (Supplementary Table S1 in Supplementary File S1).
Association of serum calcium level with coagulopathy
Overall, 22.2% (n = 105) of the study population presented with coagulopathy after acute tIPH. With respect to different markers of coagulopathy, we observed a PLT <100 × 109/L in 8.2% (n = 39) of patients, INR >1.25 in 6.1% (n = 29), PT >14 sec in 8.5% (n = 40), APTT >36 sec in 4.7% (n = 22), and FIB level <2.0 g/L in 12.7% (n = 60) of patients. Patients with coagulopathy had significantly lower serum calcium level compared with those without coagulopathy (8.84 [IQR: 8.44-9.40] vs. 9.10 [IQR: 8.68-9.88] mg/dL; p < 0.001; Fig. 3A). Then, multi-variate logistic regression analyses were performed to identify the association of serum calcium level with coagulopathy. After adjustment for the confounders including GCS scores, number of hematomas, and blood glucose, hypocalcemia was significantly and independently associated with coagulopathy (OR = 2.033; 95% CI: 1.090-3.789; p = 0.026). When included as a continuous variable, serum calcium level also was associated with a reduced risk of coagulopathy (adjusted OR per 1-unit increase in the calcium level = 0.675; 95% CI: 0.522-0.873; p = 0.003; Supplementary Table S2 in Supplementary File S1; Table 2).

Serum calcium levels between the coagulopathy (+/-) group
Multi-Variable Logistic Regression Models Evaluating the Association of Serum Calcium Level with Coagulopathy and HPC
Bolded numbers indicated statistical significance.
Adjusted for the confounders (Glasgow Coma Scale [GCS] scores, number of hematomas, and blood glucose) which were statistically significant in univariate analysis (p ≤ 0.10).
Adjusted for the confounders (age, GCS scores, number of hematomas, hematoma pattern, subdural hematoma, blood glucose and coagulopathy) which were statistically significant in univariate analysis (p ≤ 0.10).
Per unit change in regressor.
Percentage of hypocalcemia stratified according to serum calcium level.
In a sensitivity analysis, we excluded those with severe trauma (GCS scores <9).
HPC, hemorrhagic progression of contusion; OR odds ratio.
Association of serum calcium level with HPC
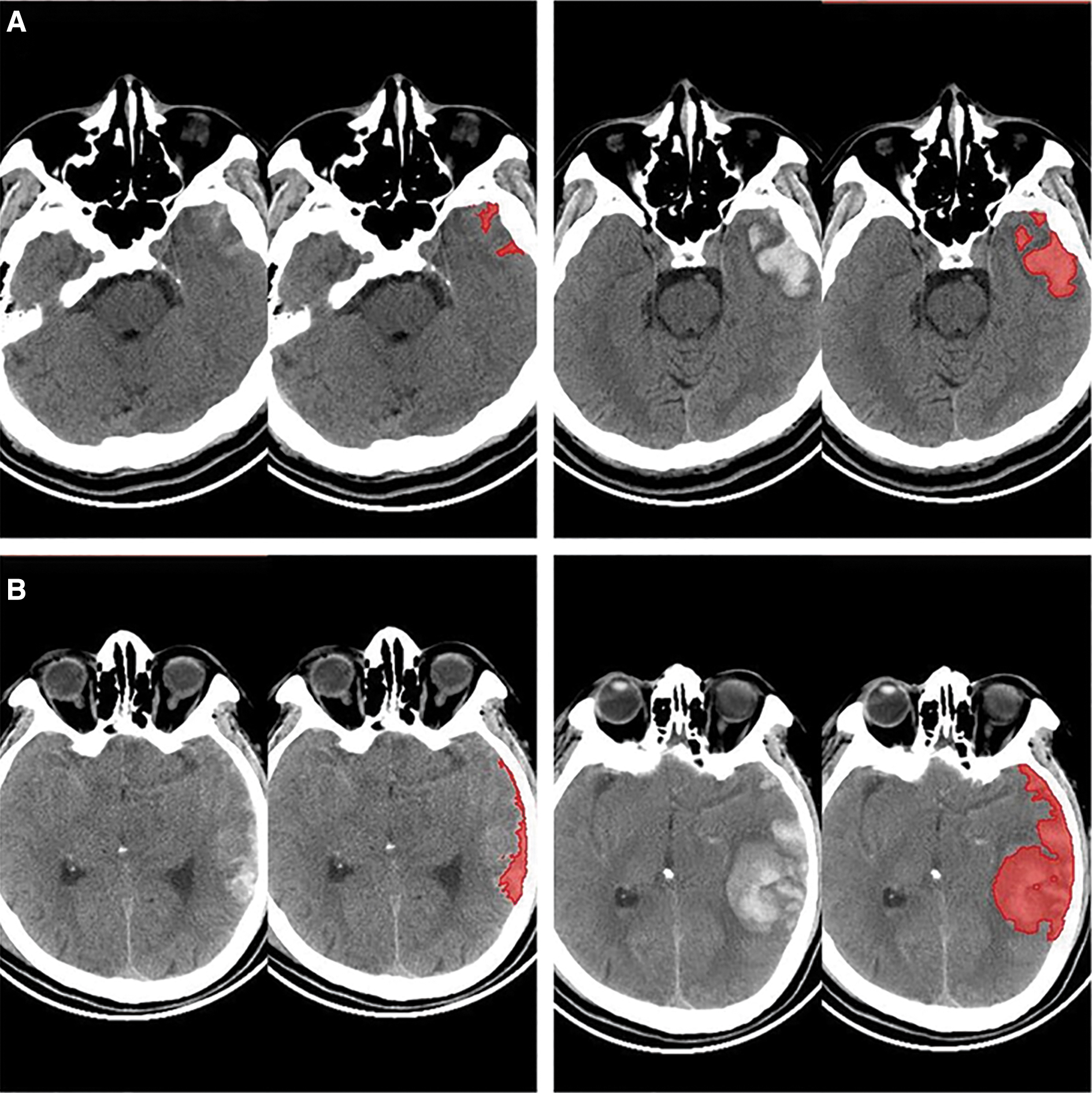
In the present cohort, HPC occurred in 187 (39.53%) patients. Examples of HPC in two patients are shown in Figure 4. The serum calcium level in patients presented with HPC was significantly lower than patients without HPC (8.92 [IQR: 8.48-9.40] vs. 9.12 [IQR: 8.72-9.89] mg/dL; p < 0.001; Fig. 3B). Moreover, patients that experienced HPC also had coagulopathy more frequently than those without (38.0 vs. 11. 9%, p < 0.001). Multi-variate logistic regression analysis identified hypocalcemia (OR = 2.708; 95% CI: 1.270-5.773; p = 0.010) and coagulopathy (OR = 3.728; 95% CI: 2.193-6.337; p < 0.001) as predisposing risk factors independently associated with the presence of HPC. Other established predictors included admission GCS scores <9, multiple hematomas, mixed hematoma pattern, SDH, and blood glucose ≥10 mmol/L (all p < 0.05). This association remained statistically significant in the multi-variable logistic regression, as a continuous variable (adjusted OR per 1-unit increase in the calcium level = 0.671; 95% CI: 0.511-0.881; p = 0.004; Supplementary Table S2 in Supplementary File S1; Table 2). We also performed sensitivity analyses excluding patients with severe trauma (n = 65, 13.7%) in view of its possible influence. Notably, low calcium levels remained significantly associated with coagulopathy and HPC, consistent with the results of the primary analysis (Table 2). ROC analysis showed that the model combining the calcium and other known predictors (AUC = 0.811; 95% CI: 0.772-0.850; p < 0.001) showed more favorable discriminative ability than the model without the calcium (AUC = 0.798; 95% CI: 0.757-0.839; p < 0.001) and the model using the calcium only (AUC = 0.628; 95% CI: 0.577-0.679; p < 0.001; Z test, AUC 0.811 vs. 0.798, p = 0.047; Fig. 5).
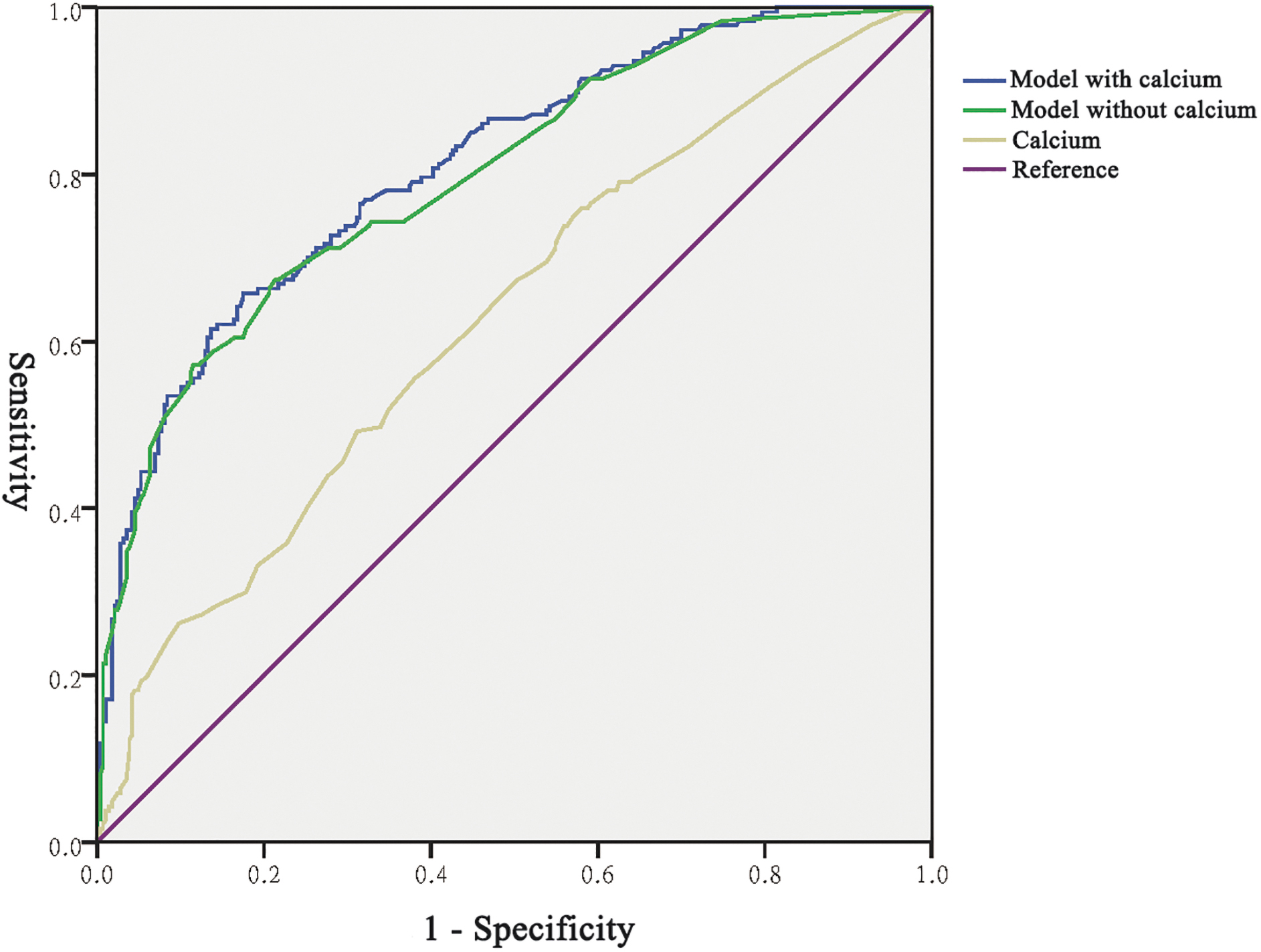
Receiver operating characteristic curve of the predictive value of serum calcium levels for HPC in tIPH patients. HPC, hemorrhagic progression of contusion; tIPH, traumatic intraparenchymal hemorrhage.
Interaction and mediation analysis between serum calcium and coagulopathy on HPC
Since the interaction analysis required the variables to be dichotomous, patients were then stratified into four subgroups according to the hypocalcemia and coagulopathy definition. Individuals with the hypocalcemia and coagulopathy possessed the highest risk of experienced HPC as compared with those with the normocalcemia and non-coagulopathy (OR = 6.519; 95% CI: 1.738-24.453; p = 0.005). However, no significant interaction was detected between the hypocalcemia and coagulopathy on HPC in all indicators: RERI = -0.300 (95% CI: -8.792-9.392), AP = -0.046 (95% CI: -1.294-1.386), and SI = 1.057 (95% CI: 0.201-5.566; Table 3). In the mediation analysis indicated partial mediation of coagulopathy on the association between hypocalcemia and HPC in patients with tIPH. For the unadjusted model, the mediator coagulopathy explained 28.0% (95% CI: 14.0-52.0%; p < 0.001) of the association of hypocalcemia with HPC. This proportion was 24.4% (95% CI: 4.7-65.0%; p = 0.006) in the adjusted model (Fig. 6).
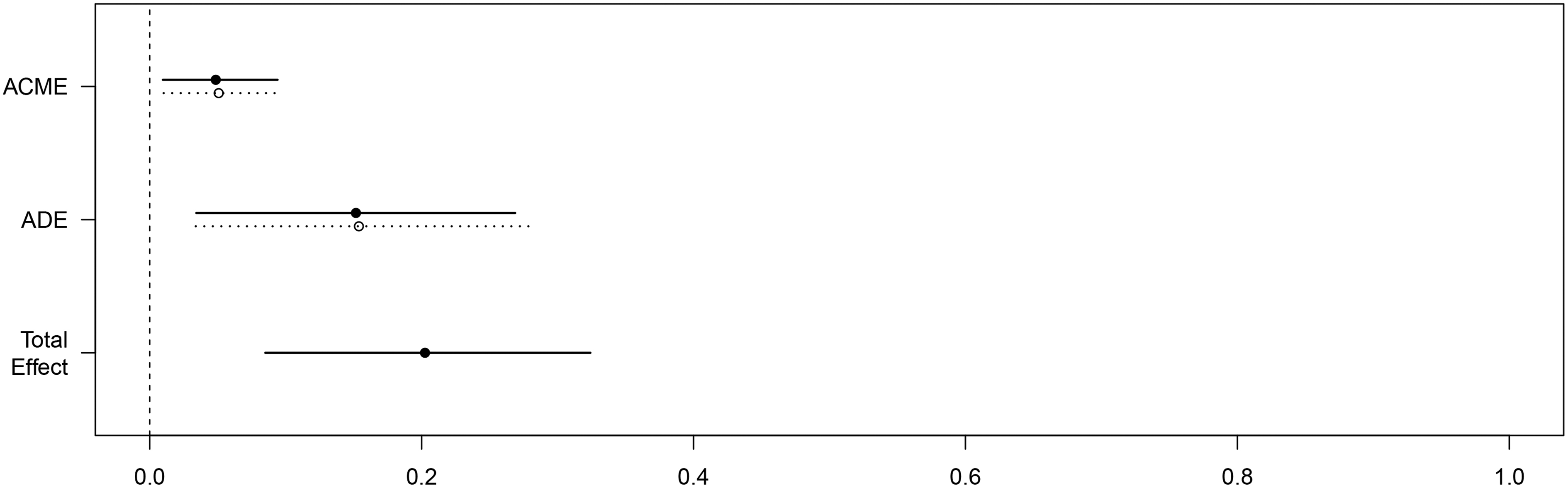
Mediation analysis of association between hypocalcemia* and HPC with mediator coagulopathy.*Percentage of hypocalcemia stratified according to serum calcium level. HPC, hemorrhagic progression of contusion.
The Interactive Effects of Hypocalcemia with Coagulopathy on Risk of HPC
Percentage of hypocalcemia stratified according to serum calcium level.
HPC, hemorrhagic progression of contusion; OR, odds ratio; RERI, relative excess risk due to interaction; AP, attributable proportion; SI, synergy index.
Repeat analysis using corrected calcium
As expected, comparable results were held using corrected calcium as well (Supplementary File S2).
Discussion
Currently, HPC is a dynamic and complex phenomenon in the clinical setting, and its pathophysiology is still obscure. Prior studies have identified that active inflammation response, higher admission BP, and impaired blood coagulation may be one of the crucial driving forces for the occurrence of HPC. 7,24,35 Further, emerging studies provide convincing evidence of the pivotal role of serum calcium levels in patients with primary (non-traumatic) IPH. 8 –15 Although low serum calcium levels at admission are capable of revealing larger hematoma volume, higher risk of hematoma expansion, and predicting patient worse outcomes, few studies have examined the role of serum calcium in patients with TBI. Given that tIPHs seem to evolve similarly to a greater likelihood of primary IPH, only patients with contusional hematomas were included in the analysis. Our study indicates that hypocalcemia is associated with increased HPC among tIPH patients and this relationship is partially mediated by coagulopathy. Additionally, even though fold increase of cumulative risk of HPC in patients with the hypocalcemia and coagulopathy is noted, no significant interaction is detected.
As for the present findings, there are two main explanations that can explain the causal and mechanistic links between low calcium level, coagulopathy and HPC. First, serum calcium is associated with vascular reactivity. Regulation of the calcium homeostasis plays a crucial role in BP, and a dietary pattern rich in calcium has been shown to reduce BP. 36 Several studies have demonstrated that hypocalcemia can contribute to the increased vascular tone and higher BP through hormonal factors, CaSRs-dependent, and CaSRs-independent mechanisms. 8,37 However, there was no significant association between serum calcium level and BP on admission in the current study. A plausible alternative hypothesis might be that acute stress after TBI is likely to fade-out the effect of hypocalcemia on BP in patients with tIPH. 38 Additionally, we did not compare BP levels before injury and further analyze the alteration of BP during the course of admission owing to the retrospective design. Research has shown that BP during the course of admission is more important than a single measurement since it tends to reflect longitudinal BP trajectory patterns in acute phase. 39 As highlighted in Chen and colleagues, 40 hence, BP level in the association between serum calcium level and the size and expansion in patients with IPH should deserve further consideration.
Second, serum calcium is a critical cofactor and plays an essential role in the coagulation cascade. As in previously published reports, hypocalcemia may lead to blood coagulation dysfunction and promote the development and progression of IPH. 8,12,25 Fukuda and colleagues 41 found that low serum calcium level was significantly associated with prolonged blood clotting time and bleeding tendency in rodent models. In the present study, a weak, albeit significant, correlation was found between serum calcium level with PLT, PT, INR, APTT, and FIB in patients with tIPH. These markers represent different pathways in coagulation. Several studies already suggested that coagulopathy commonly begins with a hypercoagulable state, marked by thrombin activation. The hypercoagulable state is followed by an excessive consumption of coagulation factors, reflected by a depletion of fibrinogen, and then prolonged prothrombin and partial thromboplastin times. 23,24 Of all presenting clinical variables, coagulopathy at admission is regarded as the main factor for HPC, with approximately half of all patients with TBI and coagulopathy subsequently displaying the hemorrhagic progression of initial brain contusions and ongoing IPH within 48 h. 24 In addition, the present investigation is one of the pioneer studies for exploring the association between serum calcium level and HPC as well as coagulopathy as a mediator and its interaction with hypocalcemia on HPC. Our findings demonstrates that hypocalcemia is associated with increased HPC risk among tIPH patients and this relationship is partially mediated by coagulopathy. On the other hand, even though fold increase of cumulative risk of HPC in patients with the hypocalcemia and coagulopathy is noted, no significant interaction is detected. These findings corroborate and extend the role of low serum calcium level in impaired hemostasis.
Notably, coagulopathy at admission only explained 24.4% of the total effect of hypocalcemia and HPC in patients with tIPH. One reason is that conventional coagulation assays such as INR, APTT, and PLT might appear normal even when the overall state of blood hemostasis is abnormal. 24 A recent meta-analysis by Yuan and colleagues 42 showed that laboratory tests have been somewhat inconsistent in detecting hemostatic alterations. Additionally, there may have been a more complex underlying pathophysiology for serum calcium. First, calcium plays an important role as extracellular signaling molecule, and activation of the calcium-sensing receptor by subtle increases in extracellular calcium leads to activation of intracellular second messengers and initiation of antiapoptotic pathways. It is reported that moderate increases in calcium of 50-200 nM may activate cell survival programs and promote resistance to hypoxia or ischemia by activated protein kinase B and mitogen-activated protein kinase–extracellular regulated protein pathways. 43 Second, calcium may alter blood–brain barrier (BBB) junction integrity by a number of different signal transduction cascades, as well as via direct interaction of calcium ions with junction proteins. If calcium levels, either extracellular or intracellular, become too high or too low, disruption of the BBB will occur. 11,44,45 Third, low serum calcium level could be a biomarker in acute IPH that represents a dysregulated homeostasis. Excessive cytosolic calcium leads to premature activation of intracellular enzymes, activation of ROS-generating enzymes, formation of free radicals, mitochondrial dysfunction, impaired autophagy, vacuolization, and necrosis. 19 Taken together, serum calcium may markedly influence HPC by complex interactions between multiple pathways.
Several limitations of the present study should be noted. First, our results were based on a single-center retrospective experience and as such may have sources of bias and variation. Second, serum total calcium consists of three fractions and ionized calcium is the active physiologic component, our study only had the data of total calcium and could not perform an analysis about ionized calcium. This was another major limitation of our study, but we do not think it significantly affects our conclusion because ionized calcium level was correlated well with total serum calcium level in the previous studies. 12,25,46 In addition, we have albumin values to account for the effects of albumin on serum calcium. 26 Indeed, research focusing on the significance of ionized calcium should be conducted in the future. Third, this study lacks a prospective design, we did not assess the previous serum calcium level and corresponding BP level, and further analyze the alteration of BP after TBI. Fourth, our primary interest in this research was in evaluating tIPH patients who did not require surgical management. As discussed above, we excluded all patients requiring immediate surgery. However, a low proportion of patients with severe trauma were not performed operations owing to other reasons (i.e., financial condition, fear of operation, or religious beliefs) and were included, which also might have the possible influence on our results. Although multiple regression analysis and sensitivity analysis were used to minimize the confounding effects, future studies with larger sample sizes would more thoroughly evaluate subgroup analyses to identify these issues. Fifth, although we evaluated different markers of coagulopathy available routine coagulation tests, we used a threshold level for each maker to dichotomize the patients. Finally, global hemostatic assays, such as viscoelastic (ROTEM and TEG) and thrombin generation tests, are often considered to provide a better assessment of coagulation. Therefore, our findings are preliminary, exploratory and requiring a large-scale replication. Further studies of these issues are warranted to confirm our findings and investigate the potential mechanisms in addition to coagulopathy.
Conclusion
In conclusion, our study demonstrates admission serum calcium levels may be associated with the HPC for patients with tIPH and this relationship is partially mediated by coagulopathy. Additionally, even though fold increase of cumulative risk of HPC in patients with the hypocalcemia and coagulopathy is noted, no significant interaction is detected. Further studies are necessary to confirm these findings and investigate potential pathophysiologic mechanisms in addition to coagulopathy.
Funding Information
This work was supported by the Zhejiang Provincial Science and Technology Innovation Program (New Young Talent Program) for College Students (Grant No. 2021R413072).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary File S1
Supplementary File S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.