
Abstract
This study compares remote neurodegenerative changes caudal to a cervical injury in degenerative cervical myelopathy (DCM; i.e., non-traumatic) and incomplete traumatic spinal cord injury (tSCI) patients, using magnetic resonance imaging (MRI)–based tissue area measurements and diffusion tensor imaging (DTI). Eighteen mild-to-moderate DCM patients with sensory impairments (modified Japanese Orthopedic score: 16.2 ± 1.9), 14 incomplete tetraplegic tSCI patients (American Spinal Injury Association Impairment Scale C and D), and 20 healthy controls were recruited. All participants received DTI and T2*-weighted scans in the lumbosacral enlargement (caudal to injury) and at C2/C3 (rostral to injury). MRI readouts included DTI metrics in the white matter (WM) columns and cross-sectional WM and gray matter area. One-way analysis of variance with Tukey's post hoc comparison (p < 0.05) was used to assess group differences. In the lumbosacral enlargement, compared with DCM, tSCI patients exhibited decreased fractional anisotropy in the lateral (tSCI vs. DCM, -11.9%, p = 0.007) and ventral WM column (-8.0%, p = 0.021), and showed a trend toward lower values in the dorsal column (-8.9%, p = 0.068). At C2/C3, compared with controls, fractional anisotropy was lower in both groups in the dorsal (DCM vs. controls, -7.9%, p = 0.024; tSCI vs. controls, -10.0%, p = 0.007) and in the lateral column (DCM: -6.2%, p = 0.039; tSCI: -13.3%, p < 0.001), while tSCI patients had lower fractional anisotropy than DCM patients in the lateral column (-7.6%, p = 0.029). WM areas were not different between patient groups but were lower compared with controls in the lumbosacral enlargement (DCM: -16.9%, p < 0.001; tSCI: -10.5%, p = 0.043) and at C2/C3 (DCM: -16.0%, p < 0.001; tSCI: -18.1%, p < 0.001). In conclusion, mild-to-moderate DCM and incomplete tSCI lead to similar degree of degeneration of the dorsal and lateral columns at C2/C3, but tSCI results in more widespread white matter damage in the lumbosacral enlargement. These remote changes are likely to contribute to the patients' impairment and recovery. DTI is a sensitive tool to assess remote pathological changes in DCM and tSCI patients.
Introduction
Degenerative cervical myelopathy (DCM), the most common form of non-traumatic spinal cord injury, involves a chronic mechanical compression of the cervical spinal cord. 1,2 Traumatic spinal cord injury (tSCI) results from an immediate mechanical insult to the spinal cord leading to sensorimotor deficits and autonomic dysfunction. 3 While DCM can stay asymptomatic for a long time (months to years), 4 the accumulation of degenerative changes often results in progressive motor and sensory impairments, although usually less severe than in tSCI. 5,6 Animal models demonstrated several common pathophysiological features at the injury site including necrosis, 7,8 apoptosis, 11 axonal degeneration, 10 -12 demyelination, 11,12 neuroinflammation, 9,13 and changes in microvasculature. 14 In both diseases, the pathological changes are not restricted to the injury site, but spread rostrally and caudally via anterograde, retrograde, and trans-synaptic degeneration. 2,6,15 -17 However, there are also fundamental differences in the onset, progression, and nature of secondary injury mechanisms between DCM and tSCI (abrupt onset in traumatic SCI vs. slowly developing symptoms in DCM). 6 Consequently, it is not clear whether DCM and tSCI patients with similar functional deficits present with similar magnitudes of remote microstructural and macrostructural degenerative changes.
Diffusion tensor imaging (DTI) is a magnetic resonance imaging (MRI) technique to probe white matter integrity, which is especially useful to characterize the secondary degeneration remote to the injury site, where conventional MRI technologies often fail to detect abnormality. 18 -20 Metrics derived from DTI also have been shown to correlate with disease severity both in DCM 21 –25 and tSCI, 26 -28 providing means to assess the grade of microstructural damage to white matter. By applying DTI in vivo at C2/C3 (rostral to injury), Seif and colleagues recently showed that DCM patients feature less altered DTI indices compared with tSCI patients, but largely similar values when comparing only to incomplete tSCI patients. 29 Although DCM and tSCI have already been compared with healthy controls, a cross-comparison between these two etiologies has not been performed caudal to the cervical myelopathy such as the lumbosacral enlargement, a region crucial for lower motor control, 30 bladder 31 and sexual functions. 32
In this study, we explore similarities and differences in the radiological presentation of DCM and incomplete tSCI with cervical injury in the lumbosacral enlargement, both in terms of microstructural changes and tissue atrophy, and compare these findings with those reported in the upper cervical cord. To this end, we utilize spinal cord DTI to characterize the tissue integrity in the white matter columns and high-resolution T2*-weighted structural imaging to measure the cross-sectional area of gray and white matter.
Methods
Study participants
Eighteen non-traumatic (DCM) patients (seven females, age, mean ± standard deviation [SD]: 55.4 ± 9.7 years), 14 tSCI patients (no female, 48.0 ± 12.9 years), and 20 healthy controls (four females, 42.7 ± 15.3 years) participated in the study (Tables 1 and 2). Inclusion criteria were: 1) no pre-existing neurological or mental disorders; 2) no previous spine operations; 3) no history of head and brain lesions; 4) no MRI contraindications; 5) >18 years of age; 6) for DCM patients, observed spinal canal stenosis in MRI and clinical diagnosis of DCM 33 ; and 7) for tSCI patients, chronic stage of injury (>12 months), incomplete injury (American Spinal Injury Association Impairment Scale [AIS] C-E), and tetraplegic injury. The tSCI patients were scanned on average (± SD) 5.7 ± 4.9 years after injury. The study protocol was designed in accordance with the Declaration of Helsinki and was approved by the local ethics committee (Kantonale Ethikkommission Zürich, EK-2010-0271). All participants provided written informed consent prior to study enrolment. Previous studies included parts of the DCM, 34 tSCI, 28 and healthy cohort. 28,34
Demographic and Clinical Information of the DCM Patients
Multi-segmental cervical spine stenosis.
DCM, degenerative cervical myelopathy; mJOA, modified Japanese Orthopedic Association score (max. 18); AIS, American Spinal Injury Association Impairment Scale; UEMS, International Standards for Neurologic Classification of Spinal Cord Injury (ISNCSCI) upper extremity motor score (max. 50); LEMS, ISNCSCI lower extremity motor score (max. 50); LT, ISNCSCI light touch score (max: 112); PP, ISNCSCI pinprick score (max: 112); F, female; M, male.
Demographic and Clinical Information of the tSCI Patients
tSCI, traumatic spinal cord injury; AIS, American Spinal Injury Association Impairment Scale; UEMS, International Standards for Neurologic Classification of Spinal Cord Injury (ISNCSCI) upper extremity motor score (max. 50); LEMS, ISNCSCI lower extremity motor score (max. 50); LT, ISNCSCI light touch score (max. 112); PP, ISNCSCI pinprick score (max. 112); M, male.
MRI acquisition protocol
MRI scanning was performed on a 3T Siemens SkyraFit scanner, using a radiofrequency transmit coil for transmission and a 16-channel head and neck coil and a spine matrix coil for reception. An MRI-compatible cervical collar was used to reduce involuntary neck motion. 35 Foam wedges were placed under the knees to minimize the distance between the lower spine and the spine matrix coil. 36 The imaged regions included: 1) the lumbosacral spinal cord (SC) with the field of view (FOV) centered at the lumbosacral enlargement and 2) the upper cervical cord with the FOV centered at the C2/C3 disc. Slice prescription was done on a sagittal T2-weighted two-dimensional turbo spin echo image of the cervical and lumbosacral cord, respectively (Fig. 1), where the lumbosacral enlargement was identified as the widest point of the lumbosacral cord as appearing on the T2-weighted image. In both regions, axial T2*-weighted images were acquired using a three-dimensional (3D) multi-echo spoiled gradient-echo image sequence (Siemens MEDIC; Fig. 1) with the following parameters: 20 slices with slice thickness = 2.5 mm, in-plane resolution = 0.5 × 0.5 mm2, FOV = 192 × 162 mm2, echo time (TE) = 19 msec, repetition time (TR) = 44 msec, flip angle = 11°, readout bandwidth = 260 Hz/pixel, four repetitions, total acquisition time = 7:16 min. Diffusion-weighted images for DTI were acquired using a reduced FOV single-shot spin-echo echo planar imaging (EPI) sequence consisting of 60 diffusion-weighted (b = 500 sec/mm2) and seven T2-weighted (b = 0 sec/mm2) images. Slice prescription was identical to the MEDIC sequence and acquisition parameters were slice thickness = 5 mm (+10% gap), in-plane resolution = 0.76 × 0.76 mm2, FOV = 133 × 30 mm2, TE = 73 msec, TR = 350 msec, acquisition time around 8 min, depending on the heart rate. Cardiac gating was used to reduce pulsation artifacts and two saturation bands were placed anterior and posterior of the cord to avoid fold-over artifacts.

Examples of the acquired magnetic resonance imaging (MRI) scans and diffusion tensor imaging (DTI) maps, both in the upper cervical cord (C2-C3) and lumbosacral enlargement (usually between T11-L1). T2*-weighted MRI (Siemens MEDIC) and diffusion MRI were acquired with identical slice prescription, defined on sagittal T2-weighted images with the slice stack (yellow rectangle) centered at the C2-C3 disc in the upper cervical cord and at the widest point of the spinal cord (SC) in the lumbosacral enlargement. SC and gray matter (GM) were segmented manually on the T2*-weighted images to obtain cross-sectional areas. Notice the good contrast between GM and white matter (WM) and between WM and cerebrospinal fluid. WM area was obtained by subtracting GM from the SC area. DTI maps including fractional anisotropy (FA), mean (MD), axial (AD), and radial diffusivity (RD) were computed from the diffusion MRI dataset. Shown is a single slice of the group-averaged FA, MD, AD, and RD maps. Notice the lower FA, MD, AD, but higher RD in the GM compared with the WM. Color image is available online.
Processing of diffusion-weighted images
Images were cropped to an in-plane FOV of 30 × 30 mm2, followed by slice-wise eddy-current and motion correction using the ECMOCO algorithm in ACID. 37 Maps of DTI metrics including fractional anisotropy, mean, axial, and radial diffusivity were obtained by fitting the tensor model on the corrected images using a robust tensor fitting algorithm (Fig. 1). 37,38 The mean diffusion-weighted images were segmented for SC with Propseg 39 and were normalized to the PAM50 template using Spinal Cord Toolbox. 40 The obtained deformation field was then applied to all DTI maps. Mean values of DTI metrics were extracted within the dorsal, lateral, and ventral white matter (WM) columns using the maximum a posteriori method of Spinal Cord Toolbox.
Processing of T2*-weighted images
The four MEDIC images were averaged using serial longitudinal registration in SPM12 41 to account for between-volume motion. The average image was resliced to 5 mm thickness to increase signal-to-noise ratio. SC was segmented using the semi-automatic 3D active surface cord segmentation method as implemented in JIM 7.0, 42 while gray matter (GM) was segmented manually (Fig. 1). WM mask was created by subtracting the GM from the SC mask. Cross-sectional tissue areas including SC, GM, and WM areas were extracted from the segmentations and were averaged across slices. In the lumbosacral enlargement, only three slices around the slice with the largest SC area were considered to ensure comparable and reproducible anatomical location.
Clinical assessment
Neurological status and functional impairment were assessed according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) protocol. 43 Single motor scores summed up between C5-T1 and L2-S1 yield the upper and lower extremity motor scores, respectively. Single light touch and pinprick scores summed up over across all neurological levels are referred to as total light touch and pinprick scores. DCM patients were assessed on the modified Japanese Orthopedic score (mJOA, max. 18 points).
Statistical analysis
Differences in age and clinical scores between groups were assessed using pairwise Wilcoxon rank-sum tests, with the p values corrected by the Benjamini-Hochberg procedure. One-way analysis of variance (ANOVA) was used to assess between-group differences in cross-sectional tissue areas (SC, GM, WM areas) and DTI metrics in the dorsal, lateral, and ventral WM columns. Significant differences between pairs of groups were tested using Tukey's multiple comparison test for post hoc analysis (p < 0.05). Images were carefully inspected and excluded if they were affected by extensive susceptibility and/or motion artifacts. As a result, one tSCI patient was excluded fully and another only from the analysis of cross-sectional areas in the lumbosacral enlargement. One healthy control was excluded from the DTI analysis at C2/C3.
Results
Patients' characteristics and clinical outcomes
Demographic and clinical information is listed in Table 1 for DCM and Table 2 for tSCI patients. In the DCM cohort, the maximal cervical spinal stenosis was at C4/C5 in two patients, C5/C6 in 14 patients, and C6/C7 in two patients. Of the 18 patients, 10 had multi-segmental cervical spinal canal stenosis; 14 DCM patients had mild (mJOA ≥15) and four patients moderate (12 ≤ mJOA ≤14) DCM. In the tSCI cohort, one patient was AIS C, 12 AIS D, and 1 AIS E (Table 2). There was no significant age difference between tSCI patients and controls (p = 0.213) and between DCM and tSCI patients (p = 0.126), but DCM patients were older than controls (p = 0.034). Compared with DCM patients, tSCI patients had lower extremity motor score (tSCI vs. DCM, mean [± SD], 43.5 [± 11.1] vs. 50 [± 0], p = 0.002), but not upper extremity motor score (48.3 [± 2.6] vs. 49.6 [±1.2], p = 0.131), pinprick (91.1 [± 24.6] vs. 105.5 [± 9.1], p = 0.063), and light touch scores (98.6 [± 15.8] vs. 105.9 [± 9.8], p = 0.190).
Diffusion tensor imaging metrics (microstructure)
In the lumbosacral enlargement, DCM patients did not show significant differences in any DTI metric compared with controls (Table 3; Fig. 2). The tSCI patients, on the other hand, had lower fractional anisotropy in the lateral (tSCI vs. controls, -15.5%, p < 0.001) and ventral WM columns (-10.4%, p < 0.001) and showed a trend toward lower values in the dorsal column (-9.0%, p = 0.057). Radial diffusivity was higher in the lateral column (tSCI vs. controls, +13.2%, p = 0.018). Compared with DCM patients, tSCI patients had lower fractional anisotropy in the lateral (tSCI vs. DCM, -11.9%, p = 0.007) and ventral column (-8.0%, p = 0.021), and showed a trend toward lower values in the dorsal column (-8.9%, p = 0.068). In addition, tSCI patients had higher radial diffusivity than DCM patients in the lateral column (+11.3%, p = 0.049).

Boxplot of fractional anisotropy
List of Tissue-Specific Cross-Sectional Areas and Column-Specific Diffusion Tensor Imaging (DTI) Metrics
Values represent mean and standard deviation across participants, separately for each region (C2/C3 and LSE) and group (healthy controls, degenerative cervical myelopathy (DCM) patients, and traumatic spinal cord injury (tSCI) patients).
ROI, region of interest; SC, spinal cord; WM, white matter; GM, gray matter; FA, fractional anisotropy; MD, mean diffusivity; AD, axial diffusivity; RD, radial diffusivity; WM dor, dorsal white matter column; WM lat, lateral white matter column; WM ven, ventral white matter column; LSE, lumbosacral enlargement
At C2/C3, compared with controls, DCM patients showed decreased fractional anisotropy in the dorsal (DCM vs. controls, -7.9%, p = 0.024) and lateral column (-6.2%, p = 0.039) and increased radial diffusivity (+22.0%, p = 0.020) in the dorsal column (Table 3; Fig. 2). The tSCI patients had lower fractional anisotropy in all WM columns (tSCI vs. controls; dorsal: -10.0%, p = 0.007; lateral: -13.3%, p < 0.001; ventral: -8.2%, p = 0.023) and higher radial diffusivity in the lateral (+25.7%, p = 0.003) and ventral column (+17.4%, p = 0.050). Compared with DCM patients, tSCI had lower fractional anisotropy in the lateral column (−7.6%, p = 0.029).
Cross-sectional tissue areas (macrostructure)
In the lumbosacral enlargement, compared with controls, DCM patients had smaller SC (DCM vs. controls, -14.4%, p < 0.001), WM (-16.9%, p < 0.001), and GM area (-8.7%, p = 0.045) than controls (Table 3; Fig. 3). Similarly, tSCI patients had smaller SC area (tSCI vs. controls, -9.9%, p = 0.017) and WM area (-10.5%, p = 0.043). No statistical differences between tSCI and DCM were detectable.
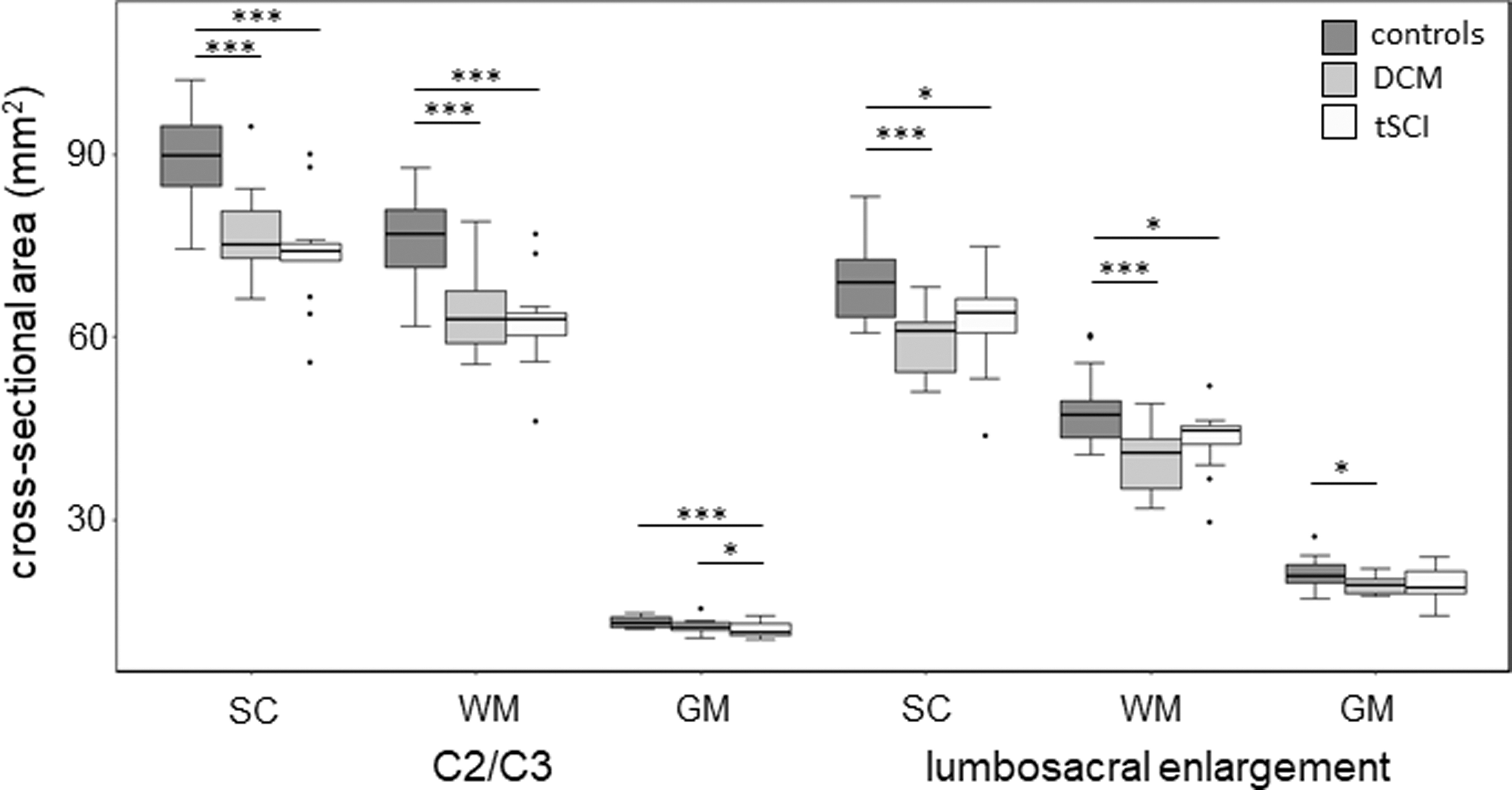
Boxplot of cross-sectional area of spinal cord (SC), white matter (WM), and gray matter (GM) in healthy controls, degenerative cervical myelopathy (DCM) patients, and traumatic spinal cord injury (tSCI) patients. Values are plotted separately for C2/C3 and the lumbosacral enlargement; p values less than 0.05, 0.01, and 0.001 are designated with *, **, and ***, respectively.
At C2/C3, compared with controls, DCM patients had smaller SC (DCM vs. controls, -14.4%, p < 0.001) and WM (-16.0%, p < 0.001) area, while tSCI patients had smaller SC (tSCI vs. controls, -17.6%, p < 0.001), WM (-18.1%, p < 0.001) and GM area (-14.2%, p < 0.001) (Table 3, Fig. 3). Compared with DCM patients, tSCI patients had smaller GM area (tSCI vs. DCM, -9.7%, p = 0.035).
Discussion
This study highlights disease-specific differences across the spinal cord axis, caudal and rostral to the primary injury. Compared with DCM patients, tSCI patients exhibited more severe microstructural changes in the WM of the lumbosacral enlargement. At C2/C3 (rostral to stenosis/injury), such differences were observed only in the lateral WM column. Interestingly, both patient groups seemed to exhibit similar degree of tissue atrophy in the lumbosacral enlargement despite tSCI patients having more severe microstructural damage.
Diffusion tensor imaging metrics (microstructure)
Beside the primary injury, an insult to the spinal cord leads to widespread and distant changes along the whole neuroaxis through secondary axonal degenerative processes, resulting in irreversible damage to the myelin sheath and the axonal cytoarchitecture. 6,15,44 Remote degenerations, both rostral and caudal to the stenosis/injury level, of the WM and GM were previously demonstrated in vivo in DCM 45 -47 and tetraplegic tSCI. 26 -28,48 When comparing mild-to-moderate DCM to incomplete tSCI patients, we add to this by showing that tSCI patients exhibit more severe microstructural degenerative changes in the WM of the lumbosacral enlargement. In fact, DTI metrics in DCM patients were not significantly different to those in healthy controls, while tSCI patients had 9-16% lower fractional anisotropy and 5-13% higher radial diffusivity values (also shown in David and colleagues). 28
Radial diffusivity has been linked to myelin content and integrity in various dysmyelination and demyelination models, 49 –53 while a decrease in fractional anisotropy can indicate both demyelination and axonal injury. 50,54 -56 This suggests that demyelination is likely to be the dominant degeneration process in the lumbosacral enlargement of incomplete tSCI patients. In contrast to previous studies that showed decreased axial diffusivity at 57 -59 but also caudal to the injury, 28 the axial diffusivity decrease in the lumbosacral enlargement was not significant in our study. This could be explained by the less severe injury in our cohort (no complete tSCI patients were involved) and the application of more conservative statistical tests (ANOVA with Tukey's post hoc test). Also, a previous study found increased mean, axial, and radial diffusivity in the lumbosacral cord of DCM, 34 which might be due to the different cohorts and type of analysis (template-based column-specific analysis vs. whole WM analysis).
The reason behind tSCI patients having more altered DTI metrics in the lumbosacral enlargement is unknown; a potential explanation is that compensatory mechanisms may limit the overall amount of microstructural damage in DCM owing to the slowly progressing nature of the condition (see Fig. 4 for potential mechanisms). tSCI, on the other hand, represents a blunt insult interrupting the axons, followed by rapid degeneration along the neuroaxis, 54 which leaves less opportunity for compensatory mechanisms. By 2 months post-injury, significant WM damage has already been shown in the lateral column of the lumbosacral enlargement with fractional anisotropy being 10% lower than in healthy controls. 60 Another explanation can be that the microstructural changes associated with DCM are more local with degenerative changes lagging at larger distances. This notion is supported by the findings at C2/C3 located only a few segments rostral to the injury site, in contrast to the lumbosacral enlargement which is at least 12 segments caudal to it.

Visual summary of the findings from the analysis of cross-sectional tissue areas and DTI maps in degenerative cervical myelopathy (DCM) and traumatic spinal cord injury (tSCI) patients with incomplete cervical injuries. Significantly lower fractional anisotropy (FA) within a white mater (WM) column, compared with controls, is indicated by red shading. FA was selected for visualization because this DTI metric showed the most changes relative to controls. In addition, the size of the schematic slices in the upper cervical cord and lumbosacral enlargement is scaled proportionally to the measured spinal cord area, compared with the corresponding slice in controls. While the primary injury mechanisms in DCM and tSCI are fundamentally different, with tSCI being a sudden traumatic event and DCM resulting from progressive degeneration of the cervical spine, they share similar secondary injury mechanisms involving axonal degeneration and accompanying demyelination. 2,6 This neurodegeneration propagates rostral and caudal to the primary injury site (dotted lines) in both DCM and tSCI, via anterograde, retrograde, and trans-synaptic degenerations. As a result, tSCI patients showed FA decrease in the dorsal, lateral, and ventral WM columns both rostral (upper cervical cord) and caudal (lumbosacral enlargement) to the incomplete cervical injury. In contrast, DCM patients were found to have decreased FA only rostral to the lesion, in the dorsal and lateral WM columns. Interestingly, the observed WM and gray matter decreases, relative to controls, were comparable in DCM and tSCI at both levels. Color image is available online.
At C2/C3, DCM patients exhibited altered fractional anisotropy and radial diffusivity compared with healthy controls, the magnitude of which was similar to those in tSCI patients as demonstrated previously. 29 However, the spatial distribution of these changes was not uniform; while our and previous results 25,45 indicate strong secondary WM damage in the dorsal and lateral column rostral to stenosis, the differences were found to be negligible in the ventral horn. In contrast, and confirming previous findings, 27,48,61 incomplete tSCI resulted in severe and widespread WM damage across all WM columns at C2/C3. Previous histopathological analyses of DCM showed evidence of both anterograde and retrograde degeneration of sensory tracts in the dorsal column 62,63 and motor tracts in the lateral column, 63 -65 with the former being linked to poor or disturbed sensation and the latter to spastic gait, but less axonal damage in the ventral column. 66
Cross-sectional tissue areas (macrostructure)
Remote atrophy of neural tissue occurs as a result of accumulation of degenerative changes, usually leading to irreversible tissue loss. At C2/C3, we confirmed a previous observation 29 and found no difference in SC and WM area between DCM and incomplete tSCI patients. In the lumbosacral enlargement, DCM and tSCI patients had similar SC and WM area of approximately 10-17% smaller than in healthy controls, shown previously for DCM 34 and tSCI patients. 28 In both patient groups, GM area was between 7% and 9% smaller than in healthy controls, demonstrating similar degree of remote GM atrophy in the lumbosacral enlargement. While it did not reach significance in our cohort, GM atrophy caudal to the injury is well known after tSCI, affecting, for example, the lower motor neurons. 67,68 Histopathology of chronic compression in DCM has also revealed degeneration of central GM, occurring typically in patients with poor sensation, proprioception defects or sphincter disturbance, 62 which represented 61% of our DCM patients. Rostral to the injury, tSCI patients showed more GM atrophy than DCM patients, which might be explained by the differential pathophysiology above and below the lesion. While GM atrophy below the lesion occurs primarily via trans-synaptic degeneration, 69,70 above the lesion it is thought to occur via several processes including transsynaptic/transneuronal degeneration of the propriospinal network, 71 vascular changes, 72,73 and apoptotic cell shrinkage of the motor neurons. 74 Since the exact pathophysiological mechanisms of remote degeneration are not fully understood, we can only speculate that the observed changes are due to more severe primary injury at the injury epicenter in the tSCI group.
Atrophy in the lumbosacral cord of DCM patients without concomitant DTI alterations is interesting. It may indicate a mere compression of the tissue, consequence of a chronic compression leading to elevated neuron density, 75 along with some degree of demyelination. These two pathophysiological processes have opposite effects on DTI parameters such as FA, resulting in little to no net changes. Overall, both DTI and cross-sectional area measurements are unspecific, meaning that different neurodegenerative processes or their combination can lead to similar changes, which limits their interpretability. Further histological research and validation studies are warranted to understand the contribution of pathophysiological mechanisms to tissue atrophy and changes in DTI.
Limitations
While the sample size was rather small, potentially limiting the generalizability of the results, it was offset by the homogeneity of our study cohorts due to strict inclusion criteria in terms of severity and level of injury (Tables 1 and 2). Between DCM and tSCI cohorts, there existed clinical, radiological, and demographic differences. The tSCI patients had lower ISNCSCI lower extremity motor scores and had more frequently hyperintense signal at the epicenter (10/14 in tSCI vs. 6/18 in DCM). Such differences in the injury severity might contribute to the more altered DTI values in the lateral and ventral columns of the lumbosacral enlargement. However, the fact that group differences were observed in the dorsal column despite similar light touch scores implies that the observed findings represent, at least partially, intrinsic pathophysiological factors related to the injury mechanisms. To confirm this hypothesis, future studies with clinically more closely matched patients and large sample size are needed.
Also, DCM patients were on average 7.4 years older than tSCI patients. While the cord atrophy rate due to normal aging is estimated to be 0.06% per year, 76 this would account for a group difference of only 0.5%, in contrast to the observed group differences of 10-15%. Since the onset of symptoms in DCM patients is not known, there might be a considerable variability in the stage of progression in which participants entered the study. Patients with a later stage of progression were exposed longer to chronic compression but also had more time for compensatory mechanisms.
Although the segmentation of the cross-sectional area of the lumbar cord was semi-automatic (only the midpoint of the cord had to be set manually), the gray matter was segmented manually as automatic segmentation algorithms have been validated only for the cervical gray matter so far. 77 To minimize bias, all segmentations were done blinded by the same experienced rater.
Conclusion
This study suggests that mild-to-moderate DCM leads to anterograde degeneration of the dorsal columns and retrograde degeneration in the lateral column at C2/C3 (rostral to stenosis), but only to minimal changes in the lumbosacral enlargement (caudal to stenosis). Incomplete tSCI leads to more widespread WM damage, affecting the whole WM both in the lumbosacral enlargement and at C2/C3. These remote degenerative changes are important because they are likely to contribute to the patients' impairment and recovery potential. Therefore, clinical trials should target remote degeneration before irreversible damage (atrophy) occurs (e.g., by means of neuroprotective agents). Advanced MRI techniques, such as diffusion MRI are sensitive tools to assess remote pathological changes in both DCM and tSCI patients.
Footnotes
Acknowledgments
We would like to thank all the patients and healthy volunteers who participated in this study, as well as the staff of the Department of Radiology and Neurology at the University Hospital Balgrist.
Authors' Contributions
GD: study design, data analysis, interpretation of data, writing the manuscript. KV: recruiting participants, acquiring clinical data, critical revision of manuscript for intellectual content. MH: recruiting participants, acquiring clinical data, critical revision of manuscript for intellectual content. AC: study concept and design, critical revision of manuscript for intellectual content. PF: interpretation of data; writing the manuscript; critical revision of manuscript for intellectual content. MS: study design, data analysis, interpretation of data, writing the manuscript, critical revision of manuscript for intellectual content; study supervision.
Funding Information
This study is funded by Wings for Life (WFL-CH-007/14), the International Foundation for Research in Paraplegia (IRP-P158 and IRP-P184), the European Union's Horizon 2020 (grant agreement no. 681094, “NISCI”), the framework of ERA-NET NEURON (hMRIofSCI no: 32NE30_173678), and the Swiss State Secretariat for Education, Research and Innovation (SERI) (contract number: 15.0137). PF is funded by an SNF Eccellenza Professorial Fellowship grant (PCEFP3_181362/1). MS is funded by Wings for Life (WFL-CH-19/20) and Balgrist-Stiftung 2021. Open access of this publication is supported by the Wellcome Trust (091593/Z/10/Z).
Author Disclosure Statement
No competing financial interests exist for the individual authors.
The Wellcome Trust Centre for Neuroimaging and Max Planck Institute for Human Cognitive and Brain Sciences have an institutional research agreement with and receives support from Siemens Healthcare. JENNIFER