
Abstract
Mild traumatic brain injury (mTBI) is an important but less recognized public health concern. Research shows that altered subcortical structures mediate cognitive impairment in patients with mTBI. This has been performed mostly using voxel-based morphometry methods and traditional volume measurement methods, which have certain limitations. In this study, we conducted a vertex-wise shape analysis to understand the aberrant patterns of caudate subregions and recovery from mTBI. The study involved 36 patients with mTBI and 34 matched healthy controls (HCs) observed at seven days (acute phase) and followed up for one month (subacute phase) post-injury. Different aberrant shapes of the caudate subregions were observed at the acute phase, which revealed atrophy in the bilateral dorsal medial caudate, and increase in the size of the right ventral anterior caudate in patients with mTBI related to HCs. Moreover, specific and significant shape restoration of right dorsal medial caudate in mTBI was observed at the subacute phase, which significantly associated with the cognitive function improvement of the patients. These findings suggest that the restoration of the aberrant shape atrophy of the right dorsal medial caudate plays a vital role in the improvement of cognitive function of patients with mTBI, providing an alternative clinical target for these patients.
Introduction
Mild traumatic brain injury (mTBI) is a critical yet not well understood public health problem that accounts for nearly 80% of traumatic brain injuries. 1,2 Individuals with mTBI have impaired cognitive function, which disrupts the normal performance of daily activities. 3 Magnetic resonance imaging (MRI) investigating neural and cognitive function impairment in mTBI has revealed that patients with mTBI have an abnormal white matter fiber tract. 4
Increasing evidence shows that patients with mTBI have a thinner left middle frontal gyrus, involved in regulating attention. 5 Also, patients with mTBI have a thinner left dorsal prefrontal cortex, which slows downs the speed of processing information. 6 In addition, individuals with mTBI have abnormal subcortical structures, which impairs cognitive functions.
The level of change in the hippocampus volume is related to the degree of trauma in mTBI. 7 Also, mTBI results in post-stress disorder, which is related to abnormal surface morphology of the amygdala. 8 Further, reduced caudate volume is associated with acute confusion in patients with mTBI, 9 whereas abnormal dorsal caudate disrupts processing of information in patients with mTBI. 10 In addition, abnormal ventral caudate in mTBI is linked to severe/frequent headaches and severe insomnia. 11 –13 Therefore, impaired cognitive function in patients with mTBI results from damage to the subcortical structures. 14,15
Most previous studies of abnormal subcortical structures in patients with mTBI have relied on voxel-based morphometry (VBM) and traditional volume measurement methods. These methods have certain limitations in analyzing the subcortical nucleus, 16 –18 because they largely depend on the smooth range and accurate classification of tissue types. For instance, it is difficult to detect the local differences in surface morphology of the subcortical nucleus using these methods. Further, given the variation in gene expression, receptor distribution and neural circuits, subcortical subfields regulate different human cognitive function. 14,15 Therefore, it is necessary to consider more subtle surface morphological differences in the subcortical nucleus when exploring the relationship between cognitive dysfunction and subcortical structure abnormalities in patients with mTBI.
Vertex-wise shape analysis has been applied in subcortical morphology studies 19 –21 and overcomes the limitations of the VBM and traditional volumetric approach. This method uses a joint shape and appearance model to determine robustly the subcortical boundary. It then provides a local and direct measure of geometric change that does not depend on the tissue-type classification or arbitrary smoothing extent. 22
Vertex-wise shape analysis of subcortical structures of patients with moderate to severe TBI revealed that these patients display surface atrophy of the hippocampus, thalamus, and basal ganglia. 23,24 A separate study involving American soldiers revealed that mild brain injury was accompanied by abnormal local surface morphology of the hypothalamus, nucleus accumbens, and amygdala. 8 These impairments, in addition to abnormalities of the caudate, impaired the speed of processing information. 25 Characterization of subcortical brain abnormalities in patients with mTBI using vertex-wise shape analysis, however, has not been applied extensively.
In this study, we investigated abnormalities in the shape patterns of subcortical structures in patients with mTBI at the acute phase using the vertex-wise shape analysis. The shape patterns of specific subcortical subregions at the subacute phase were also explored. Finally, we examined the relationships between the recovery of specific subcortical subregions and improvement of function cognitive in patients with mTBI. The overall aims of the study were to: (1) identify the different aberrant patterns in the subcortical subregions of patients with mTBI; (2) to assess the recovery of abnormalities in specific brain subregions of patients with mTBI; and (3) investigate the association between recovery of abnormalities in specific regions and cognitive function improvement in patients with mTBI.
Methods
Participants
Thirty-six patients with mTBI (17 females, 19 males, combined mean age of 37.6 ± 12.5 years) were recruited from the local emergency department of the Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University. The diagnosis of mTBI was performed by two experienced neurologists in accordance with the guidelines of the World Health Organization's Collaborating Centre for Neurotrauma Task Force. 26
To be included in this study, the study participant had to have fulfilled the following: (1) with Glasgow Coma Scale score of 13–15; (2) one or more of the following: loss of consciousness (if present) <30 min, post-traumatic amnesia (if present) <24 h, and/or other transient neurological abnormalities such as focal signs, seizure, and intracranial lesion not necessitating surgery.
Those with a history of neurological diseases, psychiatric condition, head injury, substance or alcohol abuse, intubation, and/or presence of a skull fracture and were administered sedatives on arrival in the emergency department, spinal cord injury, mTBI from other injuries (e.g., systemic injuries, facial injuries, or intubation), or other problems (e.g., psychological trauma, language barrier, or coexisting medical conditions), or from craniocerebral injury, were all excluded from the study.
The healthy controls (HCs) comprised 34 age and sex-matched individuals (20 females, 14 males, with a combined mean age of 34.9 ± 10.9 years) with no history of psychiatric or neurological illness, alcohol or substance misuse.
The MRI scanning for patients with mTBI was performed within seven days after injury (acute phase) and one month post-injury (subacute phase). Neuropsychological tests were performed within 48 h of MRI scanning. The HCs underwent the same assessments. All participants consented to participate in this study in writing. The protocol for the study was approved by the ethics committee of the Second Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University and conducted in accordance with the Declaration of Helsinki.
Neuropsychological assessment
Previous research has found cognitive impairments such as impaired memory, processing speed problems, and executive dysfunction are common in individuals after TBI. 27 –29 In addition, diverse symptoms, including headache and insomnia, have been reported in TBI. 30,31 In this study, neuropsychological performance tests were performed, including (1) Trail-Making Test Part-A (TMT-A) for rote memory assessment 32 ; (2) Forward Digit Span (FDS) and Backward Digit Span (BDS) test of Wechsler Adult Intelligence Scale-III for working memory assessment 33 ; (3) Digit Symbol Coding (DSC) task for cognitive function assessment and speed of information processing. 34
Self-reported symptomatology assessments included: (1) insomnia evaluated using the Insomnia Severity Index (ISI) for sleep quality 35 and (2) the short-form Headache Impact Test (HIT) for the severity of headache. 36 All the neuropsychological tests were performed by an experienced clinical psychologist blinded to the study.
MRI data acquisition
The MRI scanning was performed using the 3.0T MRI scanner (GE 750 Medical Systems). The heads of the participants were held in position using a custom-built head holder. High-resolution structural images were acquired using three-dimensional magnetization-prepared rapid gradient echo sequence with the following parameters: echo time = 3.17 msec, repetition time = 8.15 msec, flip angle = 9°, slice thickness = 1 mm, field of view = 256 mm × 256 mm, matrix size = 256 × 256, acquisition time = 4 min, 30 sec. The resting-state functional MRI data and diffusion-weighted imaging data were also captured, but are not discussed in this study. All participants were asked to relax with their eyes closed and not to engage in cognitive or motor related activity. Alertness of the participants during the scan was confirmed immediately afterward.
Multiple neuroimaging data (including T1-flair, T2-flair, T2, susceptibility weighted imaging) for all patients with mTBI at the acute phase were also captured. These data were used to identify the presence of focal lesions and cerebral microbleeds. Visible contusion lesions were not detected in any of the patients.
Vertex-wise shape analyses
High-resolution structural MRI data were analyzed using FSL tools (FMRIB Software Library v6.0). 37 First, brain tissue volume, normalized for participant head size, was estimated using Structural Image Evaluation, using Normalisation, of Atrophy (SIENAX). 38 First, the volumes of neocortical gray matter (GM), total GM, white matter (WM), cerebrospinal fluid (CSF), total intracranial volume (TIV), and a volumetric scaling factor were measured using SINEAX.
Second, alterations in neurotransmission in the subcortical structures was assessed using FSL-integrated registration and segmentation toolbox, 22 an automated registration/segmentation tool. Briefly, all subcortical structures were segmented based on the high-resolution structural images. The Gaussian assumptions and Bayesian probabilistic approach were used. 22 The features of the volumetric labels were obtained automatically based on the deformable surfaces of each subcortical structure. The normalized intensities along the surface of meshes were then sampled and modeled. The shapes were modeled based on the multi-variate Gaussian assumptions. The shape was expressed as a mean with modes of variation. Quality of segmentation and registration of all subcortical structures of each subject were checked manually and confirmed.
For the normalized volume of brain tissue (GM, total GM, WM, CSF, and TIV) from SIENAX, univariate mixed analysis of variance (ANOVA) with normalized volume as a dependent variable, “group” (mTBI patients and HCs) as a between-subjects factor, and “time point” (acute phase and subacute phase) as a within-subjects factor for each brain tissue was performed. Data were analyzed using SPSS software, V. 25.0 (Statistical Package for Social Sciences, Release 25.0, IBM, Chicago, IL).
Vertex-wise shape analyses of subcortical structures were first performed by group level two-sample unpaired t test. The statistical maps were defined using a general linear model (GLM) with permutation-based nonparametric testing to examine group differences at the acute phase. Maps showing significant group differences between patients with mTBI and HCs were generated by thresholding the images of t statistics with cluster-based family-wise error (FWE) correction at p < 0.05.
The recovery of different aberrant patterns in caudate subregions of patients with mTBI at the subacute phase was evaluated using a univariate mixed ANOVA analysis with vertex index of caudate shape as a dependent variable, group (mTBI patients, HCs) as a between-subjects factor, and time point (acute phase, subacute phase) as a within-subjects factor. The analyses were restricted to the caudate subregions. Post hoc analysis of simple effect was also performed after Bonferroni corrections. A p < 0.05 was considered statistically significant.
Volumetric analyses
The absolute volumes of subcortical structures were calculated using the fslstats package. Then, normalized volumes of subcortical structures were obtained by multiplying the absolute volumes by a volumetric scaling factor of each subject based on SINEAX data.
Two-way mixed ANOVA with a between-subjects factor group (mTBI patients and HCs) and a within-subjects factor time point (acute phase and subacute phase) was performed on normalized volumes for each subcortical structures (accumbens, amygdala, caudate, hippocampus, pallidum, putamen, and thalamus) to investigate volumetric alterations of subcortical structures in patients with mTBI. Post hoc analysis of simple-simple effect was performed after Bonferroni corrections using SPSS 25.0 software. A p < 0.05 was considered statistically significant.
Analysis of demographical and neuropsychological variables
Demographic and clinical characteristics of all participants were analyzed using SPSS software, version 25.0. Group differences in age and education level were evaluated using independent samples t tests, whereas the chi-square test was used to assess difference in sex between groups. For each neuropsychological measure, two-way mixed ANOVA with a between-subjects factor group (mTBI patients, HCs) and a within-subjects factor time point (acute phase, subacute phase) was performed on the test score. Post hoc analysis of simple effect was after Bonferroni corrections using SPSS software version 25.0. A p < 0.05 was considered statistically significant.
Correlation analysis
To examine whether the restoration of different aberrant shape patterns of caudate subregions would be associated with improved cognitive function, correlation analyses were performed between vertex percent change, which showed recovery change, and cognitive function improvement, which showed increased DSC score, in patients with mTBI at the subacute phase. The significance threshold was Bonferroni corrected for multiple comparisons.
Before the correlation analysis, the percentage change in vertex in the right dorsal medial caudate was calculated as described below:

Where dCaudateVertex-Change is the vertex percent change of the right dorsal medial caudate between the subacute and acute phase in mTBI.
The degree of cognitive function improvement (indexed by DSC score change) in the patients with mTBI was calculated using the following formula:

Where CogImpDSCscore-Change is the percent change in cognitive function between the subacute and acute phase in mTBI.
Results
Participants
There were no significant differences in age (t (68) = 0.991, p = 0.325), sex (χ2 (1) = 0.944, p = 0.331), and education level (t (68) = -0.825, p = 0.413) between the mTBI group and HCs. Demographic and clinical data of the study participants are shown in Table 1.
Demographic and Neuropsychological Characteristics of Patients with Mild Traumatic Brain Injury and Healthy Controls
mTBI, mild traumatic brain injury; HCs, healthy controls; TMT-A, Trail-Making Test Part-A; DSC, Digit Symbol Coding; FDS, Forward Digit Span; BDS, Backward Digit Span; ISI, the Insomnia Severity Index; HIT, the short-form Headache Impact Test.
Values presented as mean ± standard deviation unless otherwise stated.
Neuropsychological performance
At the acute phase, compared with HCs, patients with mTBI showed significant impairment in cognitive function (t(68) = -3.536, p < 0.001; assessed by DSC), severe insomnia (t(68) = 4.227, p < 0.001; measured by ISI), and high rates of headache (t(68) = 5.723, p < 0.001; assessed by HIT).
Two-way mixed ANOVA of self-reported symptomatology and cognitive function as a function of recovery revealed that there was a significant difference in self-reported headache between group × time point interaction on the HIT score between patients with mTBI and HCs (F (1, 68) = 12.909, p < 0.001), suggesting that headache was more frequent in patients with mTBI at the acute phase than HCs (p < 0.001), but there was no significant difference in headache cases between patients with mTBI at the subacute phase and HCs (p > 0.05).
Similarly, DSC revealed a strong interaction between group and time point for cognitive function (F (1, 68) = 4.356, p < 0.05). This suggests that compared with HCs, patients with mTBI at the acute phase displayed significantly poor cognitive function (p < 0.05). There was no significant difference in cognitive function, however, between patients with mTBI at the subacute phase and HCs (p > 0.05). Also, we found no significant difference in other neuropsychological measures between the two groups.
Measures of brain tissue volume
Two-way ANOVA revealed that there was no significant group × time point interaction on each brain tissue volume (all p > 0.05), implying that there were no significant group differences in brain tissue (GM, total GM, WM, CSF, and TIV) volume between the two groups (Supplementary Fig. S1).
Subcortical structural volume
Two-way ANOVA analysis investigating the volumetric alterations of subcortical structures in mTBI revealed that there was no significant difference in the volume of subcortical structures between patients with mTBI and HCs (all p > 0.05; Supplementary Fig. S2).
Different aberrant shape patterns of caudate subregions
Vertex-wise shape analyses revealed that patients with mTBI at the acute phase exhibited significant shape atrophy in the left dorsal caudate, compared with HCs (p < 0.05, FWE corrected; Fig. 1 and Table 2). A similar trend was observed for the right dorsal caudate (p < 0.05, FWE corrected; Fig. 2 and Table 2).

Vertex-wise shape analysis of the left dorsal caudate. The red-yellow colors indicate shape atrophy in the medial left dorsal caudate in patients with mTBI at the acute phase compared with healthy controls (p < 0.05, FWE corrected). The blue models represent the original left caudate structure. The colored bar represents p values. Color image is available online.
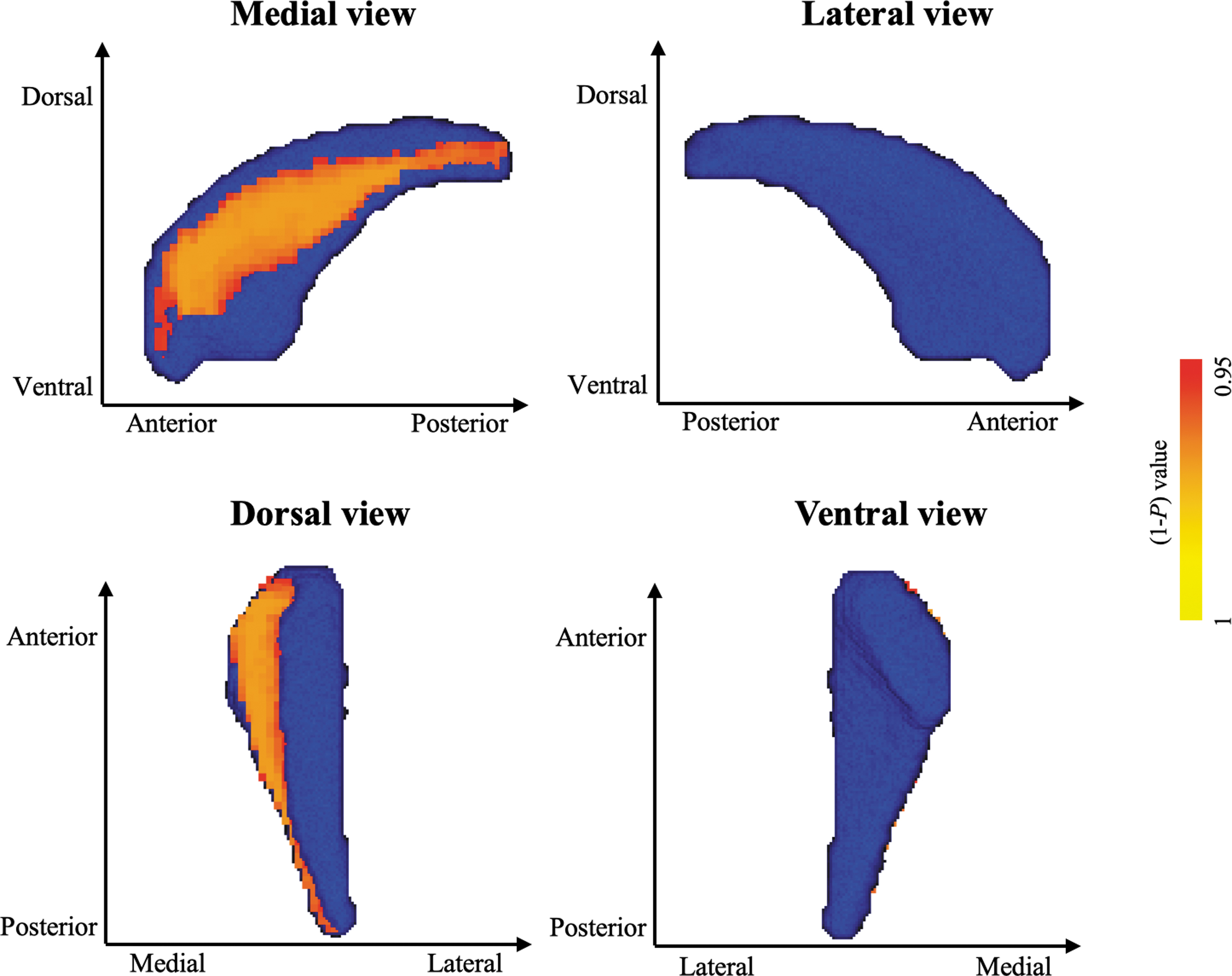
The vertex-wise shape analysis of the right dorsal caudate. The red-yellow colors indicate shape atrophy in the medial right dorsal caudate in patients with mTBI at the acute phase compared with healthy controls (p < 0.05, FWE corrected). The blue models represent the original right caudate structure. The colored bar represents p values. Color image is available online.
Different Aberrant Shapes of Caudate Subregions in Patients with Mild Traumatic Brain Injury at the Acute Phase in Relation to Healthy Controls
MNI, Montreal Neurological Institute; mTBI, mild traumatic brain injury.
In the healthy controls group, the average number of vertices of the left caudate was 2910, and the average number of vertices of the right caudate was 2908.
family-wise error corrected.
In contrast, the anterior aspect right ventral caudate head was significantly bigger for patients with mTBI at the acute phase, relative to HCs (p < 0.05, FWE corrected; Fig. 3 and Table 2). There were no significant differences in the shape of other subcortical structures between patients with mTBI and HCs.
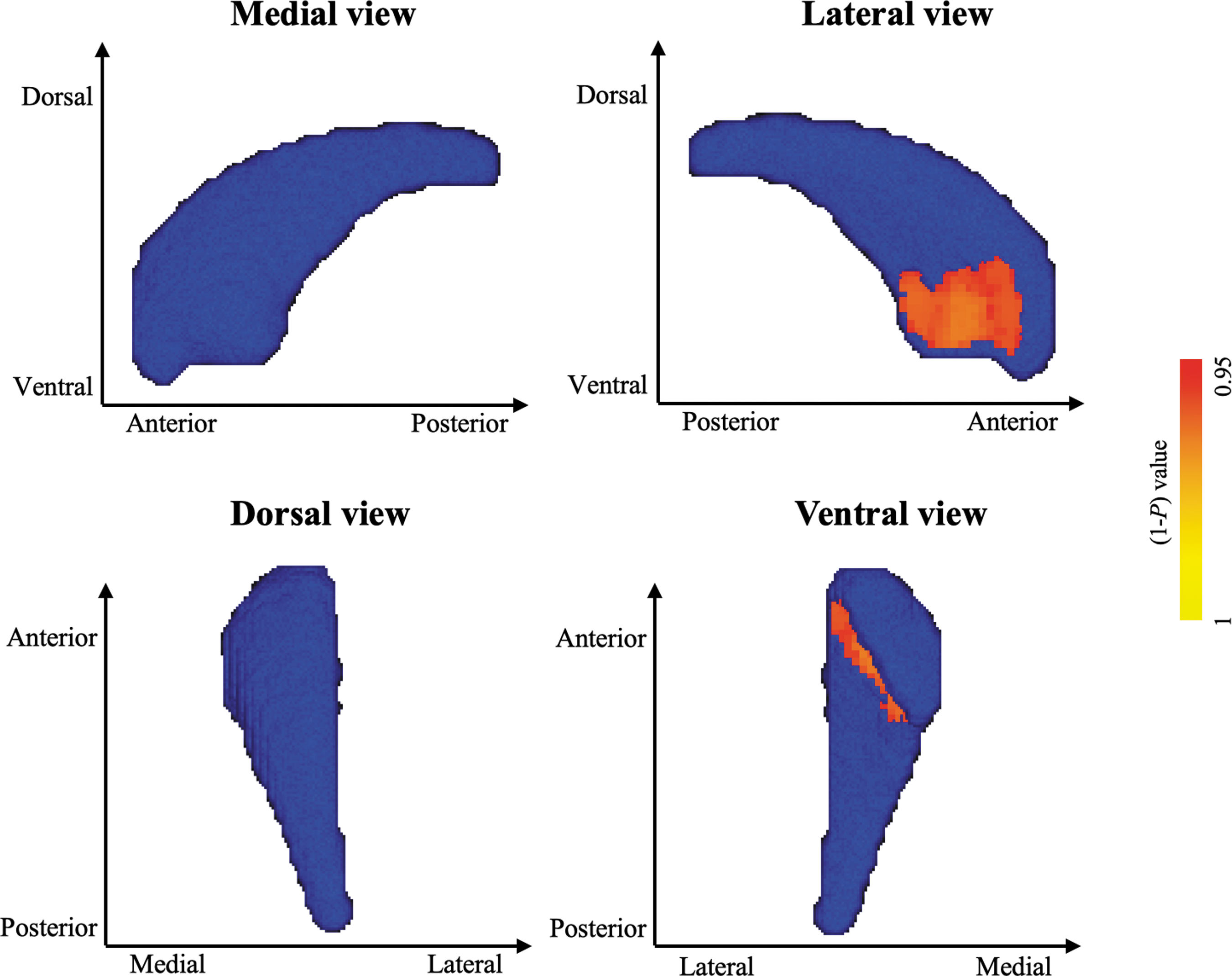
The vertex-wise shape analysis of the right ventral caudate. The red-yellow colors indicate increase in size of the anterior right ventral caudate head in patients with mTBI at the acute phase compared with healthy controls (p < 0.05, FWE corrected). The blue models represent the original right caudate structure. The colored bar represents the p values. Color image is available online.
Restoration of the aberrant shape of caudate subregions
Two-way ANOVA revealed a significant interaction between group and time point regarding changes in the shape of the right dorsal medial caudate (F (1, 68) = 7.065, p < 0.05, Fig. 4). This suggests that compared with HCs, patients with mTBI at the acute phase exhibited significant shape atrophy of the right dorsal medial caudate (p < 0.005), but there was no significant difference for this phenomenon between patients with mTBI at the subacute phase and HCs (p > 0.05). This finding supports the evidence that the shape of the right dorsal medial caudate of patients with mTBI changes to restoration at the subacute phase.
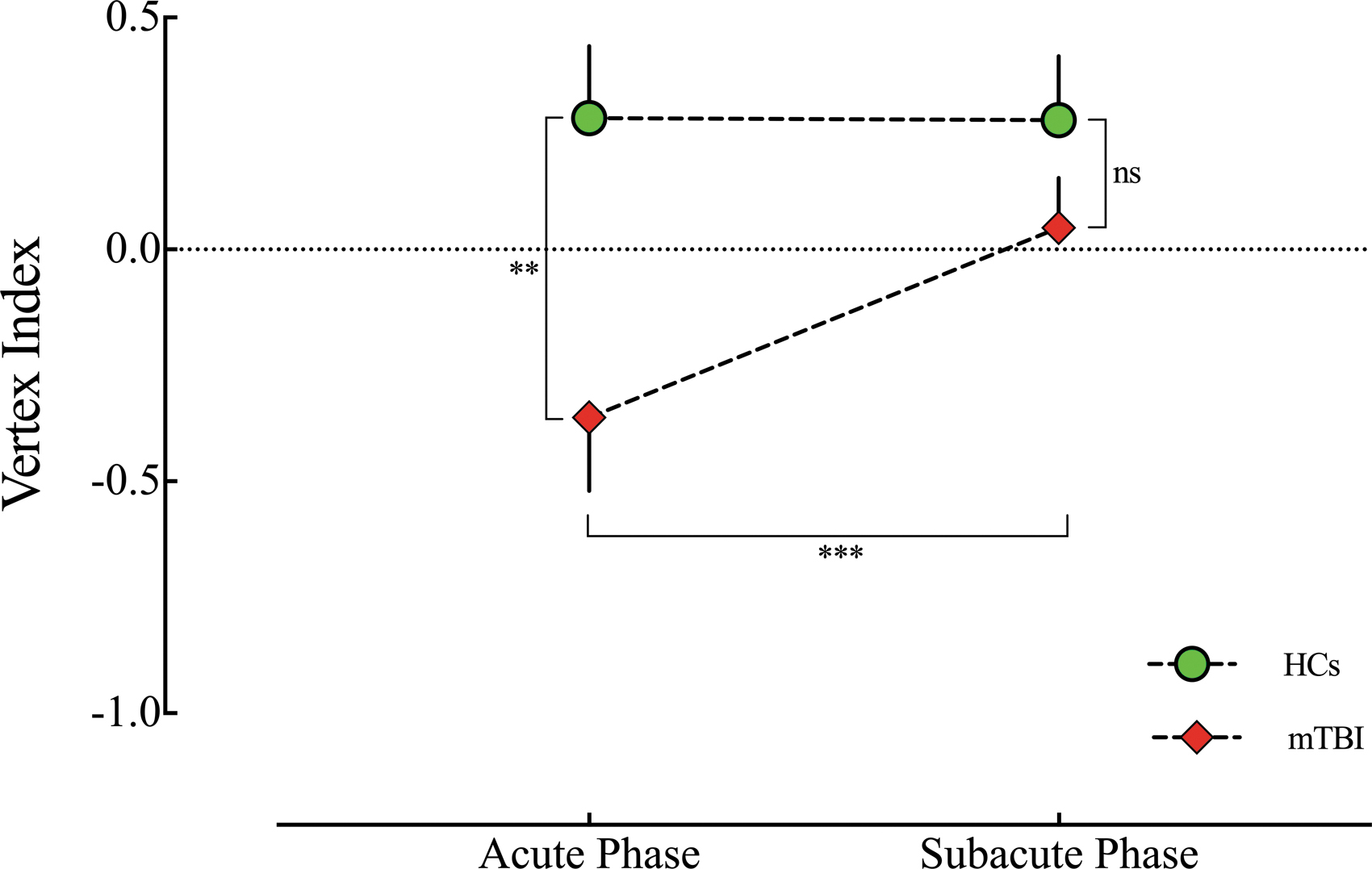
The change in atrophy of the right dorsal medial caudate of patients with mild traumatic brain injury (mTBI) at the subacute phase. There was a strong interaction between “group”
In contrast, there were no significant changes in the shape of the left dorsal medial caudate and right ventral anterior caudate between patients with mTBI and HCs.
Shape restoration of dorsal medial caudate associated with cognitive function improvement
The shape restoration of the right dorsal medial caudate of patients with mTBI (indexed by vertex percent change) positively correlated with improvement in cognitive function (R = 0.667, p < 0.001, Bonferroni corrected); however, no significant correlation was found in HCs (R = 0.166, p = =0.347, Bonferroni corrected, Fig. 5). We found for further no significant correlation between change in the shape of the right dorsal medial caudate in patients with mTBI and other factors such as headache (p > 0.05).
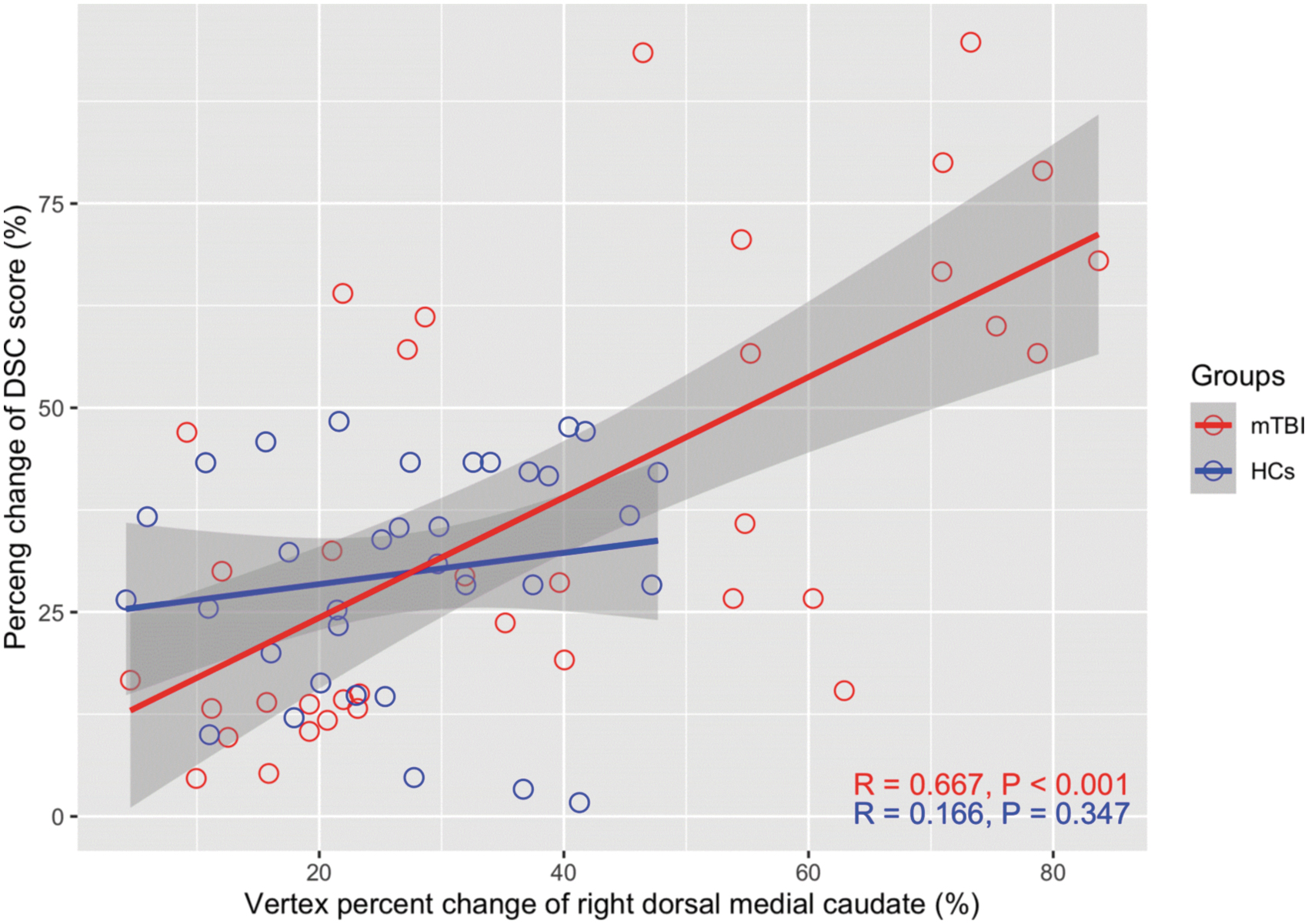
The relationship between recovery of dorsal medial caudate shape and cognitive function improvement. Recovery of the right dorsal medial caudate shape (indexed by vertex percent change) was significantly associated with cognitive function improvement (measured by percent change of DSC score) in patients with mild traumatic brain injury (mTBI) patients at the subacute phase (R = 0.667, p < 0.001); however, no significant correlation was found in healthy controls (HCs) (R = 0.166, P = 0.347, Bonferroni corrected). Color image is available online.
Discussion
To the best of our knowledge, this is the first study on the effect of aberrant shape of caudate subregions in patients with mTBI and cognitive functions using vertex-wise shape analysis. Different aberrant shape patterns of the caudate subregions were observed. Shape atrophy was observed in the bilateral dorsal medial caudate, but increase in the size of the right ventral anterior caudate in patients with mTBI at the acute phase. There were no significant abnormalities in the shape of other subcortical structures in patients with mTBI.
In addition, there was a specific significant change in the shape of the right dorsal medial caudate in mTBI at the subacute phase. The shape restoration of the right dorsal medial caudate positively correlated with improvement in cognitive function. These results suggest that restoration of the aberrant shape atrophy of the right dorsal medial caudate plays a vital role in the improvement of cognitive function of patients with mTBI, providing an alternative clinical target for these patients.
We found no abnormalities in the volume of the subcortical nucleus in patients with mTBI. In contrast, previous studies revealed that the volume of subcortical structures such as the hippocampus, 7,24,39 thalamus, 40 and caudate nucleus 8,41 was significantly reduced after TBI compared with that in HCs. This discrepancy may have resulted from a difference in time of trauma assessment. In the present study, neuroimaging scanning was performed within one week and one month of TBI, whereas in other studies, TBI assessment was performed after an average of one year. 8,39,40
In addition, the severity of TBI is directly proportional to the nature of neurobiological changes. 42 Patients included in this study sustained mild brain trauma, which to a certain extent, has not yet reached the cumulative effect and still could not result in abnormalities in the volume of the subcortical nucleus. In contrast, the severity level of brain trauma in patients in other studies ranged from moderate to severe. 8,24,40 Therefore, the time from brain trauma and the severity of the injury substantially affects neuroimaging findings. We believe the mild brain trauma of the patients included in our study resulted in no significant effect on the volume of the subcortical structures.
In this study, we observed different aberrant shapes of caudate subregions in patients with mTBI at the acute phase. In particular, atrophy was observed in the bilateral dorsal medial caudate, whereas the right ventral anterior caudate displayed an increase in size. These changes impaired the speed of information processing as well as caused severe headaches and insomnia. Previous research has found that abnormal caudate volumes in patients with TBI significantly disrupt the speed of information processing, 43 task switching ability, 23 and the level of coma. 9 These studies mostly used the VBM method, which does not effectively detect local abnormal surface morphology of the subcortical nucleus.
These studies, however, revealed that TBI can damage the caudate, and clinical symptoms observed in patients are related to the abnormal changes in caudate volume. One previous study revealed an increase in the volume of the anterior left ventromedial caudate in American soldiers with mTBI and suggested that this resulted from repetitive brain trauma, which might cause post-traumatic stress disorder and an increase in the ventral caudate volume that regulates emotional responses. 8
Herein, we observed reverse directions of local shape abnormalities in the dorsal and ventral caudate nucleus, implying that the neural mechanisms in caudate subregions are different in patients with mTBI, 42 which showed different aberrant shape patterns. This may be related to their different functional networks, which play different roles in various cognitive functions. 44 Further, regional atrophy has been found in a number of studies about TBI, 39,45 –47 and it is postulated that the shape atrophy that occurs may be because of direct injury to neuronal cell bodies, 48 ultimately resulting in cytotoxic or apoptotic cell death, 43,47 which may finally result in shape atrophy in caudate subregions in our study.
In addition, we found that the shape of the right dorsal medial caudate of patients with mTBI recovered in a specific fashion at the subacute phase, and this was strongly linked to improvement in cognitive function, consistent with previous findings. 25 Numerous studies have shown that the caudate nucleus regulates the speed of information processing in patients with varied clinical diseases. 49 –51,52 Atrophy of the caudate in various neurological diseases is related to impaired motor function. 53 Several studies have shown that the caudate-frontal functional network regulates critical functions, particularly those requiring fast information processing. 54,55 This explains the correlation between restoration of the right dorsal medial caudate shape and the speed of information processing in patients with mTBI at the subacute phase.
We found no significant shape recovery, however, in the left dorsal medial caudate and right ventral anterior caudate in patients with mTBI at the subacute phase. This may be because during TBI, the right dorsal medial caudate acts as a compensation mechanism and undergoes self-recovery in a short period, promoting the normal performance of individual cognitive functions in the patients. Several neuroimaging studies have shown that the right dorsal caudate nucleus plays an important role in cognitive control 56 and is involved in processing information and memory. 57
Despite our findings, this study has several limitations. First, we only investigated changes in the shape of subcortical structures in the acute phase (seven days post-injury) to the subacute phase (one month post-injury) of mTBI. As such, it is unclear whether the observed recovery changes could last beyond the one-month period. Future studies should explore this phenomenon. Second, the vertex-wise shape analyses were confined to the subcortical structures. The effect of mTBI on functional networks changes in the subcortical structures, however, was not assessed. Finally, the neuropsychological assessments performed in this study have certain limitations. More objective methods such as psychological experimental paradigm may therefore be more appropriate for assessing cognitive impairment in patients.
Conclusions
Patients with mTBI have aberrant shape patterns in the caudate subregions. Shape atrophy occurs in the bilateral dorsal medial caudate, whereas the size of the right ventral anterior caudate increases in patients with mTBI at the acute phase. Moreover, the right dorsal medial caudate undergoes specific and significant shape recovery, which is positively associated with improved cognitive function in patients with mTBI at the subacute phase. Taken together, the restoration of the aberrant atrophy of the right dorsal medial caudate may regulate the improved cognitive function in mTBI, and it may be a potential target for treatment of cognitive dysfunction in patients with mTBI.
Footnotes
Authors' Contributions
H.X. and B.Y. conceived the study, designed the trial, and obtained research funding. H.X., P.Z., and D.L. supervised the conduct of the trial and data collection. H.X., M.Z., and G.B. provided statistical advice on study design and analyzed the data; H.X., Y.T., and B.Y. drafted the manuscript, and all authors contributed substantially to its revision. H.X. and B.Y. took responsibility for the article as a whole.
Funding Information
This study was funded by the Natural Science Foundation of Zhejiang Province (No. LY19H180003, LY15H090016), Wenzhou Science and Technology Bureau in China (No. Y20180112, Y20140577), and Beijing New Health Industry Development Foundation (No. XM2020-02-002).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.