
Abstract
This study investigates the effect of extended laminectomy (EL) on spinal cord injury (SCI) caused by spinal shortening, and further, the timing and the optimal length of removal. Dogs received spinal column shortening at T13 segment, following which the control group underwent regular laminectomy while other groups underwent laminectomy with an additional 1-lamina length removed 6h after shortening (“1-lamina EL 6 h”), an extra 1.5-lamina length resected at 6 h or 12 h after shortening (“1.5-lamina EL 6 h” and “1.5-lamina EL 12 h”), and an extra 2-lamina length removed at 6 or 12 h after shortening (“2-lamina EL 6 h” and 2-lamina EL 12 h”), respectively. Somatosensory evoked potential (SSEP) and neurological function were recorded periodically; spinal cord blood flow (SCBF) and nerve cell apoptosis were detected. The results showed that resection of an additional 1-lamina length appeared inadequate to relieve the sharp kinking of the spinal cord, whereas the kinking disappeared with an additional 2-lamina length resection. The “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups showed no significant differences from the control in latency of SSEP, SCBF, hindlimb function and apoptosis. By contrast, significant recovery of SSEP, SCBF and hindlimb function as well as reduction of apoptosis were presented in other three groups. The “2-lamina EL 6 h” group, in particular, showed the most prominent recovery. In conclusion, an additional resection of two laminae at 6 h after shortening showed the best effect in alleviating SCI. Timely and adequately extended laminectomy could be a potential therapeutic strategy for SCI attributable to spinal shortening.
Introduction
Spinal cord injury (SCI) attributable to excessive spinal shortening is a serious complication of spine-shortening vertebral osteotomy. 1 –6 Existing research concerning this problem has remained focused on the safe limit of spinal shortening to reduce SCI incidence, 7 –12 whereas little has been reported about the treatment to alleviate such post-operative injury once it happens. In clinical practice, increasing the length of the lamina to be removed is a common way to relieve spinal cord compression, as has been evidenced in a number of studies. 13,14 Kadir and associates 13 found that additional removal of lamina prevented excessive kinking and compression of the cord, and Yang and colleagues 14 reported that extended laminectomy (EL) under the constant length of vertebrectomy could increase the safe limit for spinal shortening.
Enlightened by these findings, we speculate that increasing the laminectomy length might alleviate SCI caused by spinal shortening. To validate this speculation, we conducted the present study in which laminectomy with different degrees of extension was performed in canine models of SCI induced by spinal shortening. The potential protective effect of such a treatment was evaluated by observing the morphometry, electrophysiology, motor function, spinal cord blood flow (SCBF), and histopathology of the spinal cord. In addition, we attempted to evaluate the best time for performing this operation and the optimal length to be removed from the additional lamina.
Methods
Animals
SCI induced by thoracolumbar spinal shortening was established in 36 adult dogs (24 males and 12 females, purchased from Northwestern Polytechnical University, Xi'an, China) with a body length of 70 ∼ 82 cm. Animals were randomly allocated to six groups. Group A was the control group (n = 6), in which no extra lamina was resected after spinal shortening. Animals in group B (n = 6, the “1-lamina EL 6 h” group) received a resection of an additional lamina 6 h after spinal shortening. Group C (n = 12, with two subgroups) underwent a laminectomy with 1.5 additional laminae resected at 6 h (n = 6, the “1.5-lamina EL 6 h” group) and 12 h (n = 6, the “1.5-lamina EL 12 h” group), respectively, after spinal shortening. Group D (n = 12, with two subgroups) underwent a laminectomy with two additional laminae resected at 6 h (n = 6, the “2-lamina EL 6 h” group) and 12 h (n = 6, the “2-lamina EL 12 h” group), respectively, after shortening (Table 1).
Length and Time of EL for Various Groups
Hours after spinal shortening.
EL, extended laminectomy.
Surgical preparation, anesthesia, and intraoperative management were similar to that we described previously. 9,11 Laboratory animal care and the experimental procedure followed the guidelines of the National Institutes of Health and were approved by the Medical and Laboratory Animal Ethics Committee of Northwestern Polytechnical University (Xi'an, China).
Surgical procedure
Spine-shortening vertebral osteotomy was performed as we described previously, 9,11 with some optimization. Animals were anesthetized with 3% sodium pentobarbital at an initial dose of 1 mL/kg by intraperitoneal (i.p.) injection, and a supplemental dose (one fifth of the initial dose), if necessary, would be given through a catheter inserted into the radial vein. Animals were intubated and ventilated mechanically with air. T13 was located by C-arm fluoroscopy, and the thoracolumbar spine from T12 to L1 was exposed by a posterior approach. Four pedicle screws were inserted in parallel at both sides of T12 and L1 and were temporarily fixed by two titanium rods. Total lamina of T13, the lower half of T12, upper half of L1, and zygapophysial joints of T12/13 were resected, and the anterior vertebral body was exposed. The length of the T13 vertebral body (rostral-caudal) was measured using a vernier caliper, and its proximal two-thirds part was marked.
Then, the disk of T12–T13 was resected with a curette, and the T13 body was transected at the marked level using piezosurgery, a device with a blunt blade oscillating with a microamplitude at an ultrasonic frequency that achieves selective and precise bone cutting without injuring the surrounding soft tissues, such as the dura and spinal cord. Transection was fulfilled through two semitransections, from the left and right sides, respectively, to improve its precision and operability. After that, the proximal two-thirds part of the T13 vertebral body was removed en bloc. The spine was shortened slowly and gently until making contact with the osteotomy surface, followed by final fixation of the titanium rods. As a result, the length of shortening was the sum of the T12–T13 disk width (2.9 ± 0.33 mm, n = 36) and two-thirds vertebral body length (15.7 ± 0.99 mm, n = 36). Given that the length of the vertebral body and disk differs very slightly between individuals, the intergroup difference in the length of spinal shortening was slight.
Laminectomy was performed rostral-caudal symmetrically after spinal shortening. Specifically, animals in group B had the remaining upper half of the lamina of T12 and lower half of the lamina of L1 resected, animals in group C had the upper half of the lamina of L2 resected sequentially, and those in group D had the lower half of the lamina of T11 further resected.
In the surgical procedures, arterial blood pressure (measured with pneumatic cuffs placed around the forelimb) and pulse oxygen saturation (oximeters placed at animals' tongue) were monitored by a veterinary monitor (Umec12 Vet, Mindray, China); bleeding was controlled to prevent hypotension. Electrocoagulation and bone wax were used for hemostasis. The application of piezosurgery effectively shortened the operation time, which reduced blood loss and also made the repetitive administration of additional anesthetic unnecessary. Volume expansion with crystalloid fluid or even dopamine was used, if necessary, to keep the systolic arterial pressure (SAP) between 100 ∼ 130 mm Hg. Rectal temperature was maintained above 37.5°C using a heating blanket. Pulse oxygen saturation was monitored and maintained above 98% by oxygen inhalation. To ensure the comparability of measurements over time, the fluctuation of SAP for an individual animal was controlled within 15 mm Hg and the fluctuation of body temperature was <1°C.
Somatosensory evoked potential measurement
Somatosensory evoked potential (SSEP) was recorded after anesthesia at the following time points: before surgery; after spinal shortening but before extended laminectomy; and then 1, 7 and 14 days after extended laminectomy. A neurophysiology workstation (Xltek; Natus Medical Incorporated Excel-Tech Ltd, Ontario, Canada) was used for the measurement. Briefly, the stimulating electrodes were positioned on the bilateral tibial nerves, and square-wave electrical stimuli with a duration of 0.2 ms and an intensity of 10–16 mA was applied. The recording electrode was inserted halfway between nasion and inion at the midline of the skull, and the reference electrode was placed at the left ear. An electroneurogram was drawn by averaging 50 consecutive signals, and peak latency and amplitude were analyzed. SSEP monitoring at each time point was performed under the same anesthesia and testing condition by an experienced technician blinded to the animal's treatment condition.
Spinal cord blood flow measurement
SCBF in experimental groups (groups B, C, and D) was recorded before spinal shortening (as the baseline), before extended laminectomy, and 6 h after laminectomy, respectively. In the control group, the detection was performed before spinal shortening and then 6, 12, and 18 h after spinal shortening. Animals recovered from anesthesia after the spinal shortening procedure or each SCBF detection and were reanesthetized by an i.p. injection of sodium pentobarbital for the subsequent detection.
Laser Doppler flowmetry (Periflux system 5000 with Pf403 probe; Perimed, Stockholm, Sweden) was used for this measurement, with the wavelength set as 650 nm. The probe was fixed to the adjoining spinous process to avoid motion caused by breathing. The Doppler probe head was placed directly on the surface of the dura, lightly pressing the dura down until it touched the cord. This would minimize the space between the cord and the probe so as to achieve an efficient measurement. Four points (two on each side of the posterior spinal vein) at the vertex of the spinal cord buckling were selected as the detecting points to place the probes. Values measured at these four points were averaged and are expressed as a percentage of the baseline to eliminate variations between individual animals.
Post-operative neurological examination
Neurological function was evaluated according to the Tarlov scoring system 15,16 by two trained observers blinded to the experimental procedures at the time points of after spinal shortening, but before EL, and then 1, 7, and 14 days after laminectomy. Grade 0 represents complete paraplegia with no hindlimb motion, grade 1 represents minor joint movements, grade 2 represents major joint movements, grade 3 means being able to stand, grade 4 means being able to walk, and grade 5 means being able to climb a 20-degree slope.
Quantification of apoptotic cells
At day 14 after EL, animals were deeply anesthetized and transcardially perfused with ∼3 L of heparinized isotonic saline and then 4% paraformaldehyde (PFA). A 1.5-cm cord segment centered on the shortening site was dissected, fixed in 4% PFA, embedded in paraffin, and cut into 6-μm cross-sections. After dewaxing and rehydration, sections were immersed in antigen retrieval solution for 40 min at 96°C. Next, endogenous peroxidase activity was eliminated using 3% H2O2, and non-specific binding of immunoglobulins was blocked by 15% normal goat serum at 37°C.
Subsequently, sections were incubated in diluent primary antibody (anti-caspase-3) at 4°C for 24 h and then washed three times with phosphate-buffered saline, followed by incubation of 20 min in biotinylated secondary antibody at 37°C and then incubation for another 20 min with the addition of the avidin-biotin-peroxidase complex. Finally, 3,3′-diaminobenzidine was used for color developing. Negative controls were processed through the same procedures, except that the primary antibody was omitted. Sections were then observed under a light microscope (Olympus BX51; Olympus Corporation, Tokyo, Japan), and images were captured in eight visual fields at 200 × magnification by the Olympus CCD system. The number of caspase-3–positive cells per square millimeter within injured tissues was analyzed by two observers blinded to the group allocation.
Statistical analysis
Data were expressed as
Results
Spinal cord kinking
When the spine was shortened, the cord presented an obvious kinking, with the vertex of the kinking at almost the midpoint of the exposed cord at the rostral side of the T13 nerve root. The nerve root was tensed, and its outlet direction initially vertical to the cord, changed rostral (Fig. 1B,C). In addition, the spinal cord was compressed by the rostral and caudal edges of lamina after laminectomy. This compression would become less obvious with EL.

Morphological change of the spinal cord after spinal shortening and progressive extension of laminectomy. (
After laminectomy in which an additional 1-lamina length (the remaining upper half of the lamina of T12 and lower half of the lamina of L1) was removed, kinking of the spinal cord was slightly alleviated, but the sharp bend was still observable. With further resection of the caudal half lamina (1.5-lamina length), kinking became gentle, the sharp fold almost subsided, and the T13 nerve root was relaxed (Fig. 1D). There was still a certain compression to the cord at the upper edge of the laminectomy, but it disappeared after further resection of the rostral half of the lamina. At this point, an additional 2-lamina length was removed and the spinal cord appeared slightly curved dorsally, but not angulated.
Somatosensory evoked potential
Latency measured before surgery and after spinal shortening showed no significant difference among the control and experimental groups. In the control group, latency was prolonged immediately after spinal shortening (p<0.01, compared to before surgery). Although it showed a tendency to recover over the next 2 weeks, it was still obviously prolonged as compared with that before surgery (p<0.01; Table 2). In the experimental groups, latency was significantly shorter than that of the control group 1 day after EL, whereas it was still significantly prolonged as compared to the normal level (Table 2). Seven days after laminectomy, latency further shortened at different degrees in different groups, respectively. Latency in the “1-lamina EL 6 h,” “1.5-lamina EL 6 h,” and “2-lamina EL 6 h” groups was significantly shorter than the control, whereas the “1.5-lamina EL 12 h” and “2-lamina EL 12 h” groups showed no significant difference from the control group.
Latency and Amplitude of SSEP in Various Groups after Shortening and EL
Amplitude was expressed as percentage of the baseline recorded before surgery.
p<0.05, ** p<0.01 compared with control.
SSEP, somatosensory evoked potential; EL, extended laminectomy.
Over the next 7 days, latency continued decreasing significantly. At day 14, latency in the “1.5-lamina EL 6 h,” “2-lamina EL 6 h,” and “2-lamina EL 12 h” groups was significantly shorter than that in the control group; in particular, latency in the “2-lamina EL 6 h” group showed no statistical difference from the normal level measured before surgery (p = 0.125). For the “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups, latency did not show any significant difference from the control (Table 2), indicating the ineffectiveness of these treatments (Fig. 2).
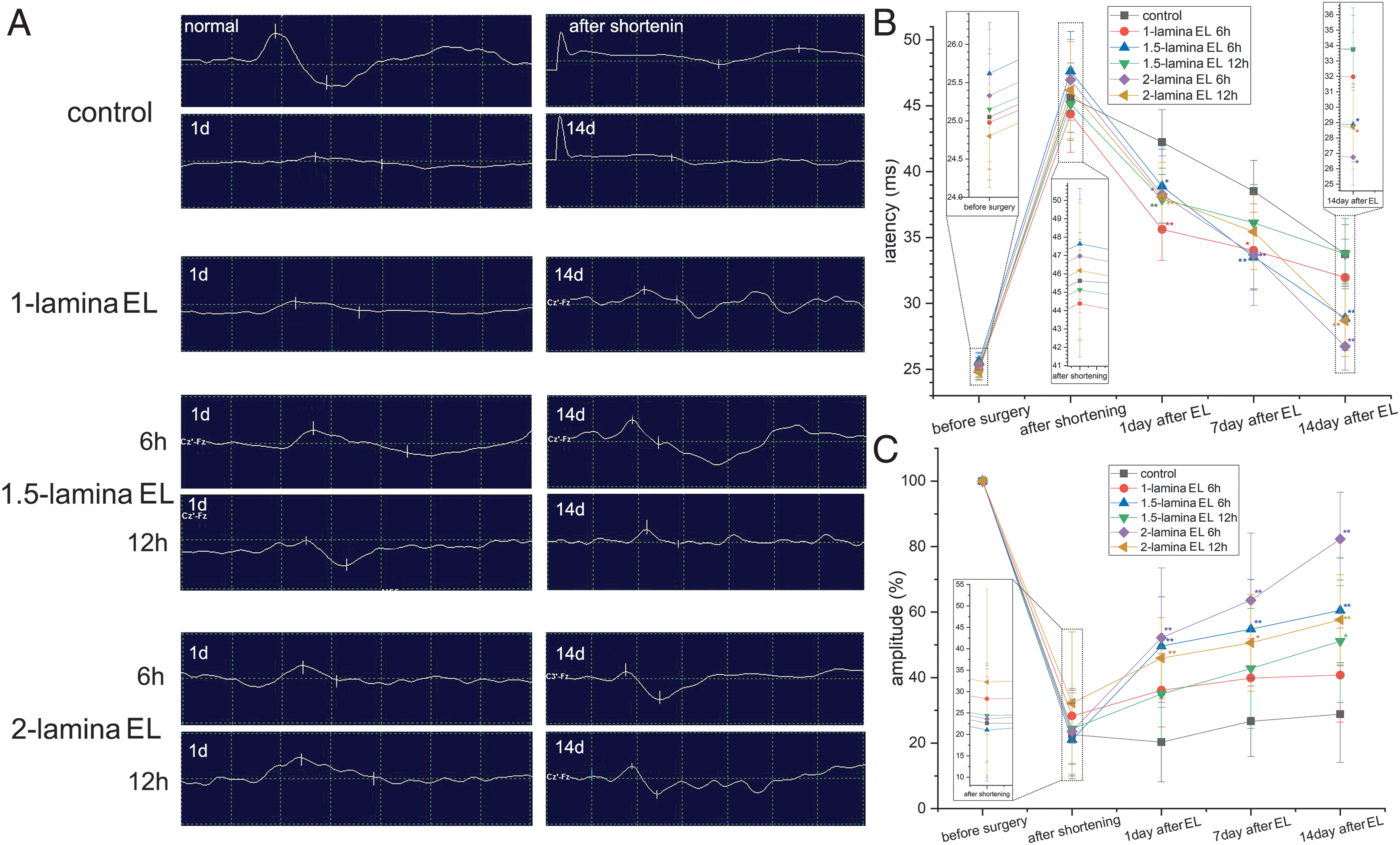
Change of somatosensory evoked potential (SSEP) after spinal shortening as well as extended laminectomy (EL) at different lengths and times. (
Amplitude is expressed as a percentage of the baseline recorded after anesthesia but before surgery. After spinal shortening, amplitude declined to 21.1 ∼ 32.2%, and there were no statistical differences among the control group and experimental groups at this point (p>0.05). In the following 14 days, the control group remained at this low level without any notable change. In contrast, a significant increase, as compared to that at the time point of after shortening, was observed 1 day after EL in all the experimental groups except the “1-lamina EL 6 h” group (p = 0.053; Table 2). The “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups showed no difference from the control group at this time, and this trend persisted until 7 days after laminectomy. At 14 days after laminectomy, the amplitude of the experimental groups, except the “1-lamina EL 6 h” group, significantly increased as compared with that of the control group. Even though the amplitude did not yet recover to the normal level (p<0.01 vs. baseline), four groups achieved >50% of the baseline amplitude (Table 2; Fig. 2).
Spinal cord blood flow
SCBF dropped to 77.3 ∼ 83.7% after spinal shortening. In the control group undergoing laminectomy with no extension, SCBF continued decreasing to 56.6% at 18 h after spinal shortening. In the “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups, SCBF decreased significantly at 6 h after laminectomy (Table 3), and it was not significantly different from that in the control group at the corresponding time point (Table 3). This suggested that these two forms of EL had no effect on reducing SCBF. In the “1.5-lamina EL 6 h” and “2-lamina EL 12 h” groups, SCBF measured 6 h after laminectomy showed no noticeable change as compared with that before laminectomy, but it was remarkably higher than that of the control group at the corresponding time point.
SCBF in Various Groups before and after EL
“6 h after spinal shortening” corresponds to the time point of “before EL” for the “1-lamina EL 6 h,” “1.5-lamina EL 6 h,” and “2-lamina EL 6 h” groups.
“12 h after spinal shortening” corresponds to the time point of “after EL” for the “1-lamina EL 6h,” “1.5-lamina EL 6 h,” and “2-lamina EL 6 h” groups, but “before EL” for the “1.5-lamina EL 12 h” and “2-lamina EL 12 h” groups.
“18 h after spinal shortening” corresponds to the time point of “after EL” for the “1.5-lamina EL 12 h” and “2-lamina EL 12 h” groups.
p<0.05, ** p<0.01 compared with control; # p<0.05, ## p<0.01 compared with their SCBF after spinal shortening but before EL.
SCBF, spinal cord blood flow; EL, extended laminectomy.
These two forms of management, although they did not improve SCBF, prevented a further decline. The “2-lamina EL 6 h” group presented even more exciting results. SCBF rose from 77.3% to 92.3% after laminectomy (p = 0.000), which was significantly higher than that of the control group (p = 0.001), and showed no difference from its normal level (baseline; p = 0.121; Table 3). This suggested that EL for an additional 2-lamina length at 6 h after spinal shortening could effectively reverse the continuous decline of SCBF (Fig. 3).
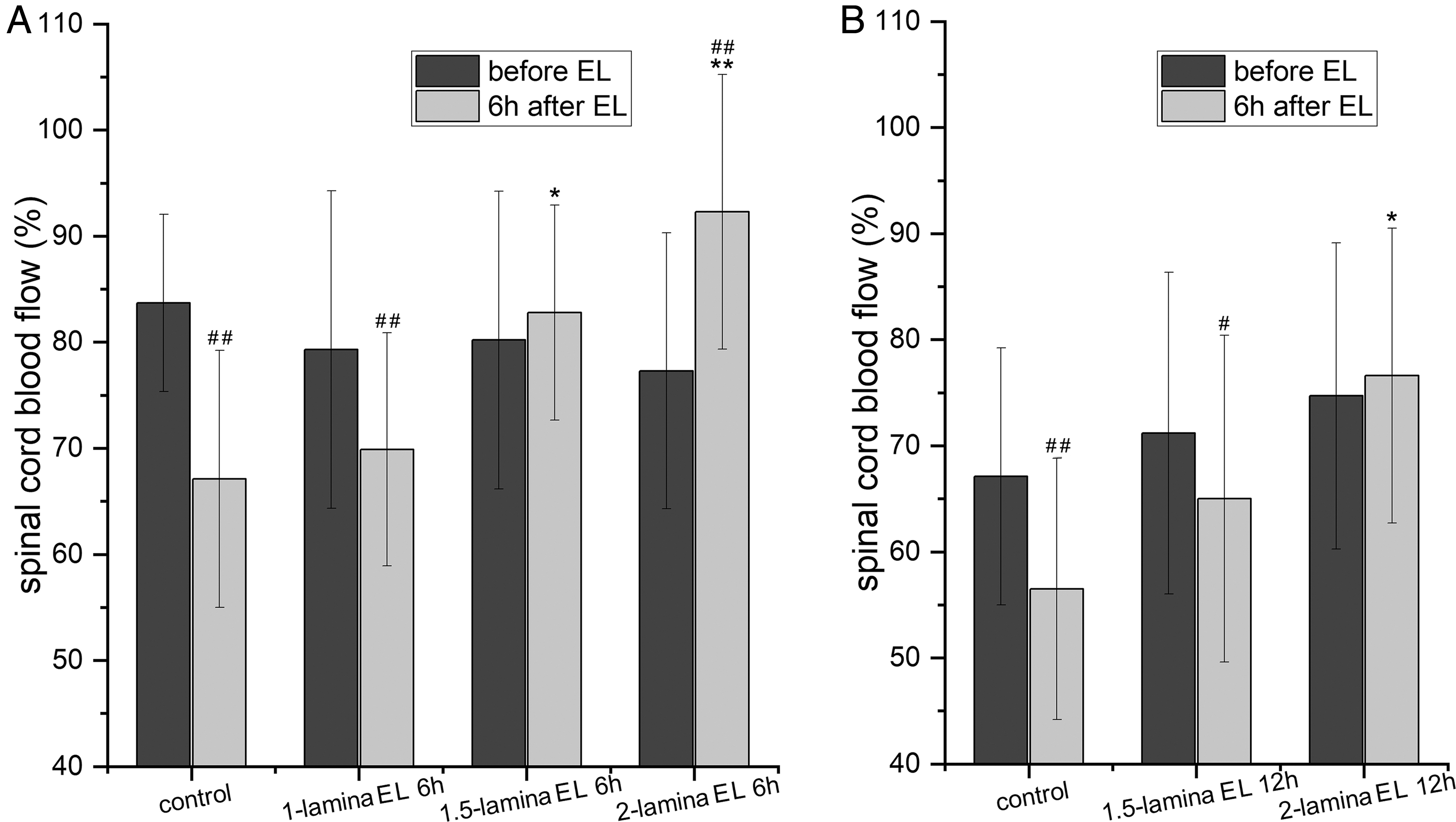
Changes in spinal cord blood flow (SCBF) at 6 h after extended laminectomy (EL). (
Neurological function
The Tarlov grade decreased dramatically after spinal shortening. Most animals (91.7%) were scored under grade 3, and no improvement was observed up to 1 day after laminectomy. There were no differences among groups at this point (Hc = 2.345, p = 0.800). Until day 14 post-operation, the Tarlov grade in the control group had barely improved, with a median score of 2 and only 1 animal able to stand (grade 3) by then. Within the 14 days after EL, the Tarlov score of the “1-lamina EL 6 h” group showed no difference from that of the control group (Hc = −0.392, p = 0.695), whereas the “1.5-lamina EL 12 h” (median score, 2), “2-lamina EL 6 h” (median score, 3), and “2-lamina EL 12 h” groups (median score, 2) presented a clearly increased neurological function at day 7 post-laminectomy (“1.5-lamina EL 12 h” vs. control: Hc = −2.448, p = 0.014; “2-lamina EL 12 h” vs. control: Hc = −2.448, p = 0.014; “2-lamina EL 6 h” vs. control: Hc = −3.542, p = 0.000). One animal in the “2-lamina EL 6 h” group was scored grade 4, which was the highest of these three groups.
At day 14, the Tarlov score was significantly higher in the “1.5-lamina EL 6 h” (median score, 3), “2-lamina EL 12 h” (median score, 3), and “2-lamina EL 6 h” (median score, 3.5) groups (“1.5-lamina EL 6 h” vs. control: Hc = −2.007, p = 0.038; “2-lamina EL 12 h” vs. control: Hc = −2.007, p = 0.038, “2-lamina EL 6 h” vs. control: Hc = −3.050, p = 0.002). The “2-lamina EL 6 h” group had the highest median Tarlov score, in which all animals were able to stand and 3 could walk. In the “2-lamina EL 12 h” group, 1 animal got the highest Tarlov score (grade 5), but 2 animals remained unable to stand (grade 2; Fig. 4).
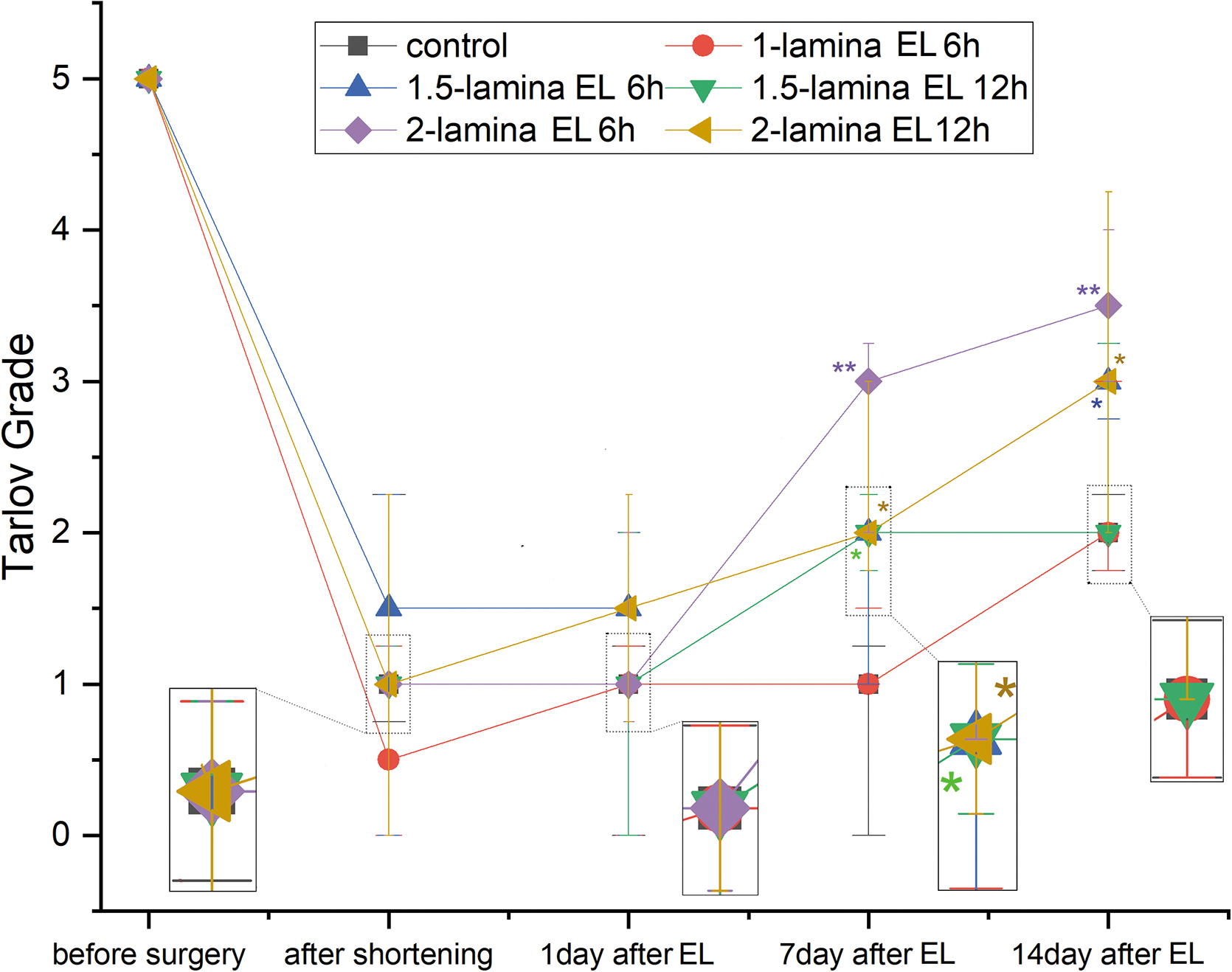
Neurological function recovery evaluated according to the Tarlov scoring system after spinal shortening and then 1, 7, and 14 days after extended laminectomy (EL). Data represent the median and 25th–75th percentiles. *p < 0.05, **p < 0.01 compared with control.
Apoptosis
Casepase-3–positive cells increased remarkably after spinal shortening (145.1 ± 28.3/mm2) as compared with the normal cord (16.7 ± 3.9/mm2). The number of apoptotic cells decreased in animals receiving laminectomy with an extra 1-lamina length removed at 6 h post-shortening or laminectomy with an extra 1.5-lamina length removed at 12 h post-shortening, but the decrease was not statistically significant (“1-lamina EL 6 h” vs. control: p = 1.000; “1.5-lamina EL 12 h” vs. control: p = 0.975). The remaining three forms of EL evidently alleviated the apoptosis of nerve cells as compared with the control (“1.5-lamina EL 6 h”: 85.8 ± 25.8/mm2, p = 0.003; “2-lamina EL 6 h”: 66.7 ± 24.5/mm2, p = 0.000; “2-lamina EL 12 h”: 74.7 ± 22.2/mm2, p = 0.000). However, the number of casepase-3–positive cells in these groups was still significantly higher than the normal level (“1.5-lamina EL 6 h”: p = 0.000; “2-lamina EL 6 h”: p = 0.022; “2-lamina EL 12 h”: p = 0.004). The laminectomy with an extension of 2-lamina length at 6 h post-shortening did not show any evident advantage over the other treatments (“1.5-lamina EL 6 h” vs. “2-lamina EL 6 h”: p = 0.994; “2-lamina EL 12 h” vs. “2-lamina EL 6 h”: p = 1.000; Fig. 5).

Apoptosis in the spinal cord at 14 days after extended laminectomy (EL). Immunohistochemical detection of casepase-3 in the spinal cord sections from uninjured animal (
Discussion
In this study, we explored the effect of EL on SCI caused by spinal shortening by observing the morphometry, electrophysiology, motor function, SCBF, and histopathology of the spinal cord. We found that kinking of the injured spinal cord disappeared when the laminectomy extended to have an additional 2-lamina length removed. Resection of an additional 2-lamina length at 6 h post-shortening, compared with other forms of management in our experiment, resulted in the most prominent recovery in SSEP, SCBF, and neurological function. These results indicate that a timely and adequately extended laminectomy could be a potential therapeutic strategy for SCI caused by spinal shortening.
Laminectomy is a commonly applied, easily achievable approach to alleviating spinal cord compression. Two previous studies have reported the association between an increase in the length of laminae to remove in a laminectomy and the change of the spinal cord during spinal column shortening. 13,14 Yang and colleagues 14 performed EL with the removal of an extra 1-lamina length before spinal shortening and concluded that an appropriate extension in a laminectomy could increase the safe range of spinal shortening. This finding is inspiring, but the study did not explore whether EL would reduce SCI caused by spinal shortening. Kadir and associates, 13 by a classic morphological experiment in animal cadavers, confirmed that extension of a 1.5- or 2-lamina length in a laminectomy could obviously decrease the excessive kinking of the cord attributable to spinal shortening; whereas, as pointed out by the investigators, this was not sufficient to guarantee the protective effect of EL on neurological function, the observation of improved neurological outcome in living animals was necessary.
We believe that two factors merit particular attention in an actual operation. The first is the timing of EL. SCI is a continuous and gradual process, consisting of primary and secondary injuries. 17,18 EL is aimed at relieving the kinking and compression of the spinal cord, which are primary injuries that dominate in the early phase. Without effective decompression management, secondary injuries, such as microcirculatory disturbance, inflammation response, lipid peroxidation, and so on, would be ignited to aggravate SCI. Therefore, timing of the operation is crucial in discussing the application and effect of EL. The second factor to consider is the additional length of lamina to remove. An inadequate laminectomy may not achieve effective decompression, whereas excessive resection may aggravate surgical trauma and increase the risk of iatrogenic spinal instability. Hence, a reasonable length in EL is critical in achieving effective decompression with a minimal amount of lamina removed.
Based on these considerations, we designed the present study in which a laminectomy with the additional resection of different lengths of lamina was performed at different time points after SCI induced by spinal shortening in animal models. The effects of these various treatments were observed and measured. The one with the best result would represent the optimal combination of time for the operation and length of an additional laminectomy.
After spinal shortening, as observed in this study, morphological characteristics of the spinal cord were mainly the change of nerve root outlet direction, spinal cord kinking, and spinal compression at the vertebral edges after laminectomy. These manifestations were clearly relieved after EL. Kadir and colleagues 13 described the change of outlet direction of nerve roots in the coronal plane after spinal shortening, whereas, in this study, we observed a change in the sagittal plane, which would be more closely associated with the morphological changes of the spinal cord. In the process of spinal shortening, the cord would move dorsally and kink when it could no longer slide in the spinal canal. The nerve root stretched gradually until it was tensed, which would, in turn, strain the spinal cord and restrict its dorsal movement. This partly contributed to the formation of the sharp bend of the spinal cord between the T12 and T13 nerve roots (Fig. 1B).
With EL, kinking of the cord was alleviated and the nerve root became slacked. However, the change of the nerve root direction may be influenced by other factors, such as the spinal segment in the operation and the direction in which the shortening proceeds (shortening from rostral vertebra to caudal, or vice versa). More details concerning the relationship between nerve roots and spinal shortening need to be uncovered by further research.
After laminectomy, the edge of the remaining lamina not only stands as an obstacle that prevents dorsal movement of the cord, but also leads to a local compression on the cord. This is the anatomical basis for the validity of EL in dealing with shortening-induced SCI. When two additional laminae were resected, the caudal and rostral parts of the spinal cord moved backward, which alleviated the sharp kinking of the cord and achieved decompression at the edge of the lamina.
SSEP is a reliable way for evaluating the function of the spinal cord after shortening. 9,11,19 In this study, latency was prolonged noticeably after spinal shortening and showed some recovery in the subsequent 14 days, even without any treatment. However, this recovery was minor, given that latency was still much longer than the normal level at day 14 post-shortening (prolonged by 34.7% compared with the baseline). EL definitely prevented the electrophysiological deterioration of the spinal cord. Latency recorded 1 day after EL was significantly shorter than that of the control group, which received a non-extended laminectomy. However, such an effect was hard to sustain if EL was performed too late or inadequately. For example, latency in the “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups presented no difference from that in the control group 14 days after laminectomy, which might be attributable to inadequate resection and/or lack of timeliness.
By contrast, the “2-lamina EL 6 h” group that had undergone an adequate laminectomy in a timely manner had the best electrophysiological records. Generally, an >10% (against the baseline) increase in latency is considered meaningful. The “2-lamina EL 6 h” group presented a slight increase (<10%), but a greater increase was observed in the “1.5-lamina EL 6 h” group (delayed 12.8%) and the “2-lamina EL 12 h” group (delayed 15.7%). These observations suggested the importance of the length of the lamina to remove and the timing of the operation in the performance of EL.
In our experiment, amplitude dropped dramatically after spinal shortening; it almost disappeared in 4 cases. Different form latency, amplitude would not show any tendency of recovery unless an effective treatment was performed. An appropriate EL could promote its recovery, but compared with latency, amplitude was harder to return to the normal level. As evidenced by the “2-lamina EL 6 h” group, latency of the group returned to normal at day 14 after laminectomy, whereas amplitude was still significantly lower than the normal level. Despite certain discrepancies in the range and phase of their changes, amplitude and latency were consistent in their overall changes, and this consistency was especially presented in the “1-lamina EL 6 h” and “1.5-lamina EL 12 h” groups.
Regarding amplitude and latency, it is hard to decide which is more sensitive in evaluating neurological function. Amplitude has a smaller fluctuation interval, and a decline of >50% is generally considered the boundary of SCI. This theoretically weakens the sensitivity of amplitude, especially when it is close to this critical value, 50%. As in the “1.5-lamina EL 12 h” group, the amplitude was restored to 51.11% of the baseline 14 days after EL, but animals still presented poor neurological function. Because of this, it is more reasonable to combine amplitude and latency in evaluating neurological function. Based on our previous report and experience, shortening of two-thirds vertebral body length would cause an incomplete SCI commonly encountered in clinical practice, in which the waveform would not be likely to disappear completely so that the amplitude and latency are identifiable. In this study, we recorded only 4 cases with very low amplitude after shortening; this small number of cases would barely influence the statistical results.
Microcirculatory disturbance is generally considered the “trigger” of secondary injuries in SCI. 18,20,21 The change of SCBF after spinal shortening has its own characteristics. 8,9,11 Under normal conditions, the spinal cord is slightly stretched in the spinal canal because of the longitudinal traction of never roots. For this reason, the cord is retracted in the early phase of shortening, and the kinking is negligible given that the shortening is tolerated mostly by the sliding of the cord. 13 Therefore, the tension of spinal arteries decreases and the diameter of the anterior spinal artery increases 8 in this phase, resulting in a temporary increase of SCBF. As the shortening continues, the spinal cord and its arteries meander, the anterior spinal artery is obstructed at the site of spinal cord kinking, 8 and SCBF declines continuously. 8,9 This suggests that morphological change of the spinal cord is an important cause for decreased SCBF during spinal shortening. In addition, compression of the spinal cord at the edges of laminectomy, as mentioned previously, may also contribute to the fall of SCBF.
In our experiment, laminectomy with an extended removal of 2-lamina length eliminated spinal cord kinking and compression, and a clear recovery of SCBF was observed after surgery. What is worth noting is that the degree of recovery differed between groups receiving the same EL, but at different time points (6 vs. 12 h after spinal shortening). This indicated that the duration of shortening of the spinal cord was another inducer of SCBF decrease. Prolonged tortuosity of blood vessels would cause disruption of the blood–spinal cord barrier. 11 Presumably, the vascular wall might be deteriorated and a thrombus would subsequently form. Under this condition, SCBF would not be fully restored even when the tortuosity of blood vessels would be relieved by EL. In short, a timely and adequate laminectomy could prevent the decline of SCBF and promote its recovery, which, in turn, might relieve the subsequent secondary injuries.
Neurological function was evaluated using the Tarlov scoring system. As an ordinal variable with non-normal distribution, the Tarlov score of each group is expressed as the median and was analyzed by a non-parametric test. Neurological function of animals receiving a laminectomy with the extension of 2-lamina length at 6 h after spinal shortening was clearly improved. Although the Tarlov grade of this group showed no statistical advantage over that of the “1.5-lamina EL 12 h” group (p = 0.079), animals presented a more evident recovery in neurological function of the hindlimbs: All the animals in this group were able to stand whereas only 2 in the “1.5-lamina EL 12 h” group could stand. This deviation may be ascribed to the distinction between statistical and clinical significance.
Our pathological observation revealed that cell apoptosis occurred at not only the center of the kinking site, but also the rostral and caudal to the center, which indicated the occurrence of secondary injuries and the expansion in the scope of injury. Ischemia is one of the triggers of apoptosis. 22,23 Degree of apoptosis in the “1-lamina EL 6 h” group suffering persistent low SCBF was greater than that in the “2-lamina EL 6 h” group, which had a dramatic SCBF recovery. Nevertheless, the “2-lamina EL 6 h” group still had excessive apoptosis, even though spinal cord kinking was relieved and SCBF was almost restored. It remains unclear whether apoptosis was related to the process of ischemia/reperfusion after the EL that relieved the spinal cord kinking.
Degree of apoptosis and the electrophysiological parameters were not necessarily consistent with the neurological function. Taking the “2-lamina EL 6 h” group as an example, SSEP latency was recovered to the normal level at day 14 after laminectomy, but significant apoptosis was still observed in the spinal cord. As indicated, the degree of apoptosis can partially reflect the degree of SCI, but it is not the only reference for evaluating the neurological function. Many other factors, such as the volume of spared tissue as well as its compensatory ability, also contribute to the recovery of neurological function. 24,25
In this study, the spinal cord in the animal model suffered a very sharp kinking for the purpose of providing a strong visual illustration. This actually rarely happens in reality; instead, bending of the spinal cord or compression at the lamina edge is more likely to appear in clinical practice. In establishing the model of spinal cord contusion, impact velocity can influence the severity of injury. 26,27 In our experiment, the velocity was not precisely controlled, which might have caused variation in the degree of injury. To ensure the consistency, spinal shortening was required to be completed in more than 5 min and the process was carried out gently, especially when kinking the spinal cord.
Conclusion
Appropriate EL can effectively relieve the spinal cord kinking induced by spinal shortening and compression at the lamina edge after laminectomy. In the case of shortening of two-thirds vertebral body length with two laminae resected, an additional resection of two laminae at 6 h after shortening, compared with other forms of EL, yields the best results in terms of recovery of electrophysiology, SCBF, and neurological function. It also obviously reduces the apoptosis of spinal cord neurons. In short, timely and adequate EL can be a potential therapeutic strategy for SCI induced by spinal shortening.
Footnotes
Acknowledgments
We thank Professor Chen Qi for her contribution.
Funding Information
This work was funded by the Shaanxi Provincial Science and Technology Department (nos. 2020SF-092 and 2018ZDXM-SF-057) and National Natural Science Foundation of China (no. 81371347).
Author Disclosure Statement
No competing financial interests exist.