
Abstract
Patients with spinal cord injury (SCI) frequently develop infections that may affect quality of life, be life-threatening, and impair their neurological recovery in the acute and subacute injury phases. Therefore, identifying patients with SCI at risk for developing infections in this stage is of utmost importance. We determined the systemic levels of immune cell populations, cytokines, chemokines, and growth factors in 81 patients with traumatic SCI at 4 weeks after injury and compared them with those of 26 age-matched healthy control subjects. Patients who developed infections between 4 and 16 weeks after injury exhibited higher numbers of neutrophils and eosinophils, as well as lower numbers of lymphocytes and eotaxin-1 (CCL11) levels. Accordingly, lasso logistic regression showed that incomplete lesions (American Spinal Injury Association Impairment Scale [AIS] C and D grades), the levels of eotaxin-1, and the number of lymphocytes, basophils, and monocytes are predictive of lower odds for infections. On the other hand, the number of neutrophils and eosinophils as well as, in a lesser extent, the levels of IP-10 (CXCL10), MCP-1 (CCL2), BDNF [brain-derived neurotrophic factor], and vascular endothelial growth factor [VEGF]-A, are predictors of increased susceptibility for developing infections. Overall, our results point to systemic immune disbalance after SCI as predictors of infection in a period when infections may greatly interfere with neurological and functional recovery and suggest new pathways and players to further explore novel therapeutic strategies.
Introduction
Patients with spinal cord injury (SCI) face life-long recurrence of infections, mainly of urinary and respiratory tracts, that have a great impact on their quality of life. In addition to being the leading cause of morbidity and mortality after SCI, 1 –3 infections during the acute phase are a predictive factor of impaired neurological recovery and reduced functional independence. 4,5 The high rate of infections is directly linked to the impaired adaptive and innate immune responses that results from SCI. 6 –16 Among the reasons why this occurs, autonomic nervous system dysfunction (and subsequent increase of ß2-adrenergic signaling in immune cells) as well as activation of the hypothalamic–pituitary–adrenal axis (and subsequent increase of cortisol levels) are the major contributors. 17 –20 However, in contrast to the increasing knowledge about the mechanisms mediating SCI-induced immune depression, little is known about whether the individual immune profile could be used to predict infections.
Recently, Jogia and colleagues 21 reported that the neutrophil to lymphocyte ratio (NLR) is higher at 3 days after injury among patients who suffer from respiratory infections afterwards. Further, the NLR serves as a predictive marker of infection occurrence. 21 However, to our knowledge, there is a lack of a more detailed immune profile including other markers of immune status, such as cytokines and other inflammation-related molecules, that would predict infections.
Our aim was to specifically address whether the immune profile of patients with SCI during the subacute period could be used to predict infections. To achieve this, we studied the peripheral blood immune cell populations as well as the levels of cytokines, chemokines, and growth factors from a blood sample that was collected 4 weeks after injury. Further, we explored the association of these markers with occurrence of infections in the following 12 weeks.
Methods
Patients and healthy control subjects
Eighty-one patients with traumatic SCI were recruited at the Trauma Center Murnau (Bavaria, Germany) or at the Hospital Nacional de Paraplejicos (Toledo, Spain) under the development of the Autoantibodies in Spinal Cord Injury study.
22
The study protocol and the informed consent sheet of the Autoantibodies in Spinal Cord Injury study were evaluated and approved by the Ethics Committee of Toledo Health Care Area and by the Ethics Committee of the Bavarian Medical Board (registry number 15046). The study follows and adheres to the World Medical Association Declaration of Helsinki and is registered at the public database
All patients fulfilled the inclusion and exclusion criteria and gave their informed consent to participate.
Inclusion criteria were: males and females; at least 18 years old; any neurological level of injury, except cauda equina syndrome; complete and incomplete lesions; and if the patient was treated with glucocorticoids, the last dose should have been administered at least 7 days before study onset.
Exclusion criteria were: a diagnosed autoimmune disorder; a diagnosed tumor; and preexisting neurodegenerative disease.
In addition, patients with traumatic brain injury (Glascow Coma Scale score <14) were excluded from this study. Polytrauma patients were recruited as long as their injuries did not interfere with neurological examination.
Sensorimotor function of patients was evaluated following the International Standards for Neurological Classification of Spinal Cord Injury scale (ISNCSCI) at an average time of 31 ± 1 days after injury (from now on described as 4 weeks after injury). All evaluations were performed by experienced personnel who attended the ISNCSCI training course at Heidelberg University Hospital. On the same dates of sensorimotor function evaluation, a blood sample was obtained from each patient. Age, gender, lesion level, and severity of patients are summarized in Table 1.
Demographic and Clinical Characteristics of Participants
t-test mean values SCI versus CTL p-value = 0.65.
Frequencies of age ranges, Fisher's exact test p-value = 0.18.
Frequencies of genders, Fisher's exact test p-value = 0.028.
AIS, American Spinal Injury Association Impairment Scale; CTL, control subjects; SCI, spinal cord injury; SEM, standard error of the mean.
Twenty-six healthy volunteers were recruited at the Hospital Nacional de Paraplejicos. A single blood sample was taken after the signing of the informed consent and fulfilling the inclusion and exclusion criteria detailed above was confirmed (with the obvious exception of not suffering an SCI). Age and gender of these individuals are summarized in Table 1.
Blood sera
Peripheral blood was collected by venipuncture. A blood clot was allowed to form by maintaining the tubes for 45 min at room temperature (RT) followed by 1 h at 4°C. Blood was centrifuged at 4°C, at 1,500g for 20 min and serum was aliquoted and stored at −80°C until used.
Whenever a blood sample was taken, a standard hematological analysis was performed in parallel by the clinical laboratories at Murnau Trauma Center (Bavaria, Germany) or at the Hospital Nacional de Paraplejicos (Toledo, Spain).
Documentation of infections
Pneumonias, upper respiratory tract infections (URIs), and urinary tract infections (UTIs) occurring between the day after the first examination date (4 weeks after injury) up to the second examination date (16 weeks after injury) were annotated in the medical records. The most frequent infections were UTIs (54 patients), followed by URIs (9 patients), and pneumonias (6 patients).
Patients were in the hospital during the duration of the study; all infections were acquired during the inpatient period. Distribution of dates of first infection after 4 weeks from injury are shown in Figure 1.
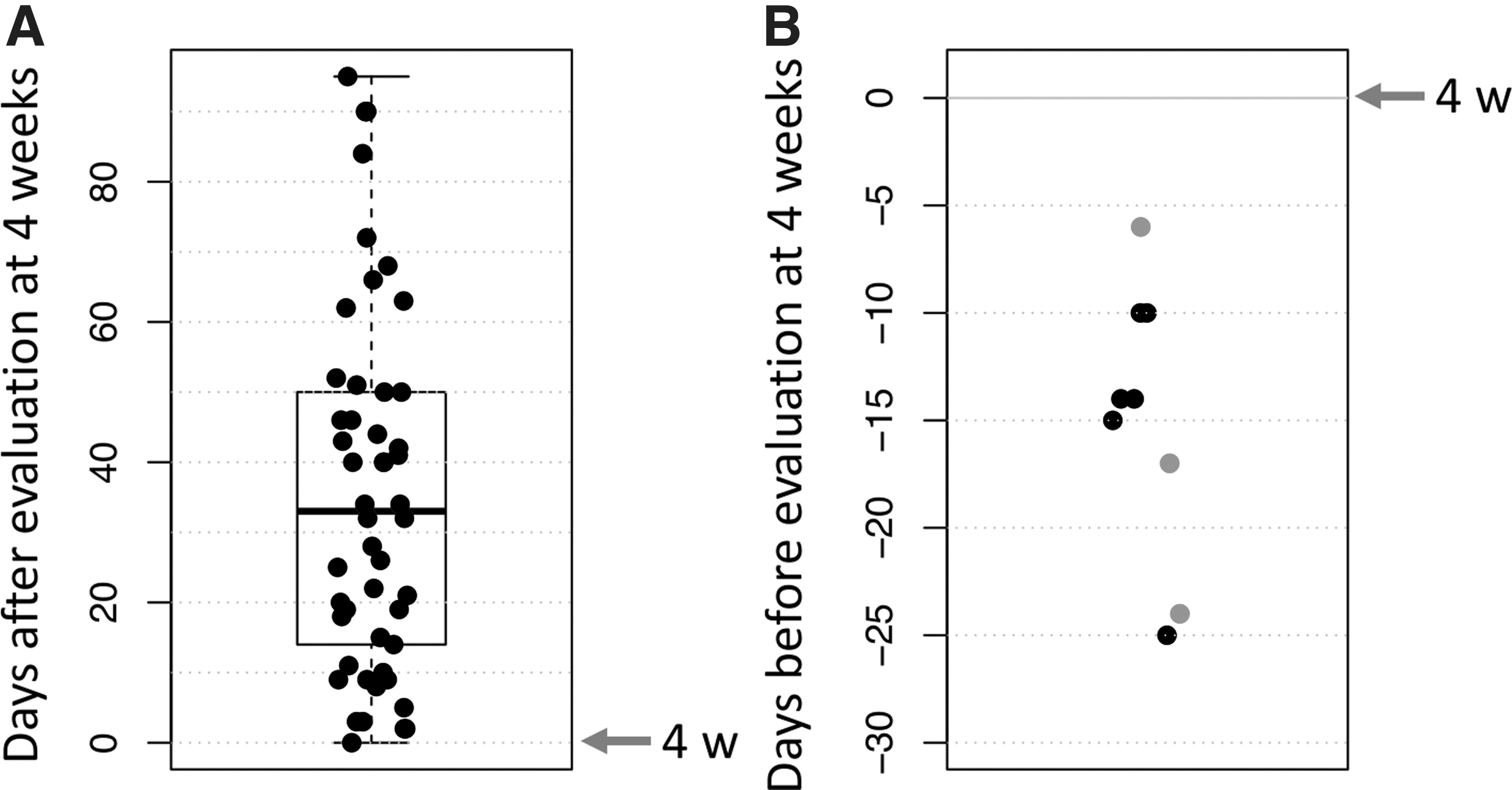
Dates of infections after SCI.
Pneumonias were diagnosed by clinical examination and confirmed by chest X-ray. UTIs were diagnosed by clinical examination and confirmed by laboratory findings in urine (bacteriuria and/or high number of leukocytes). URIs were diagnosed by clinical examination.
The 55 patients from Murnau Trauma Center (Germany) were admitted to the hospital in the acute phase after injury, whereas the 21 patients from the National Hospital for Paraplegics (Spain) received acute medical management at other medical centers. Thus, infections before inclusion in the study (4 weeks) were available only for patients from the Murnau Trauma Center. Pneumonias, URIs, and UTIs before inclusion were defined as stated above and extracted from medical records.
Determination of serum inflammation-related factor levels
Serum cytokines, chemokines, and growth factors related with distinct types of immune responses were measured with a custom human 16-plex panel (ProcartaPlex Immunoassay, Thermo Fisher Scientific; interleukin [IL]-1β, IL-6, IL-10, IL-17A, IL23, IL-37, tumor necrosis factor [TNF]-α, IL-8 [CXCL8], IP-10 [CXCL10], eotaxin-1 [CCL11], MCP-1 [CCL2], GRO-α [CXCL1], PD-L1, vascular endothelial growth factor [VEGF]-A, brain-derived neurotrophic factor [BDNF], tPA) and a transforming growth factor (TGF)-β1 single-plex panel (ProcartaPlex Immunoassay, Thermo Fisher Scientific), according to the manufacturer's protocol on a Luminex MAGPIX instrument. The 7-point standard curves were created using the Procarta Plex Analyst software. The lower limit of quantitation (LLOQ) was 2.0 pg/mL for IL-1β, 9.2 pg/mL for IL-6, 2.2 pg/mL for IL-10, 2.0 pg/mL for IL-17A, 16.7 pg/mL for IL-23, 4.2 pg/mL for IL-37, 7.2 pg/mL for TNF-α, 2.4 pg/mL for IL-8, 1.8 pg/mL for IP-10, 2.1 pg/mL for eotaxin-1, 3.6 pg/mL for MCP-1, 2.0 pg/mL for GRO-α, 4.0 pg/mL for PD-L1, 5.7 pg/mL for VEGF-A, 2.1 pg/mL for BDNF, 38.3 pg/mL for tPA, and 1.4 pg/mL for TGF- β1.
Among the studied cytokines, IL-1ß, IL-6, IL-8, IL-10, IL-17A, IL-23, IL-37, TNF-α, and PDL-1 were excluded from the analysis due to their absence or low proportion of detection. IL-1ß, IL-10, IL-23, IL17A, and TNF-α levels were below the LLOQ in all samples, including patients and control subjects. IL-37 was over the LLOQ in only 1 patient (1.2%) and IL-6 in 3 patients (3.7%), whereas both cytokines were below the LLOQ in all control subjects. IL-8 was above the LLOQ in 9 patients (11.1%) and in 4 healthy control subjects (15%). PD-L1 was above the LLOQ in 15 patients (18.5%) and in 3 control subjects (11%). Additionally, this protein was above the upper level of quantification (ULOQ) of 233.0 pg/mL in 1 patient.
Statistical analysis
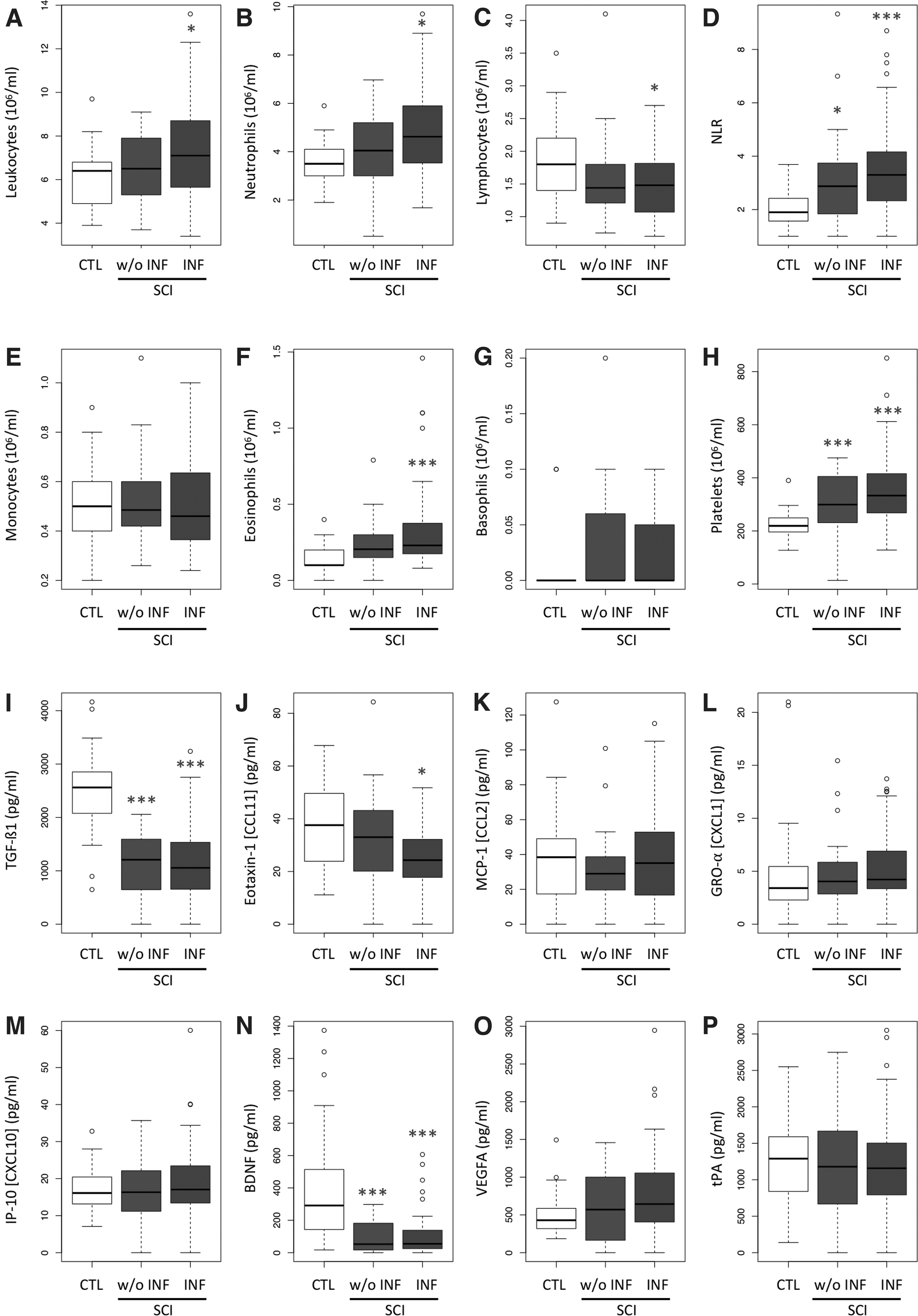
All statistical analyses were performed in R statistical programming language 23 using RStudio. 24 For comparisons of three groups by one-way analysis of variance (ANOVA; results shown in Fig. 2), we first checked normality of residuals by Shapiro's test and homoscedasticity by Levene's test. When both conditions were fulfilled, ANOVA and Tukey honest significant difference post hoc test were performed. Otherwise, we performed a Kruskal-Wallis rank sum test followed by Dunn's test. The precise statistical procedure used in each case is detailed in the legend of Figure 2. Levene's test was applied using the car package 25 and Dunn's test using the FSA package. 26
SCI-induced changes in the number of systemic immune cell populations and inflammatory mediators at 4 weeks after injury were more prominent in patients who suffered from infections afterwards. The number of peripheral blood total leukocytes was higher at 4 weeks after injury in patients who suffered from infections in the following 12 weeks compared with control subjects
Lasso logistic regression was performed using the glmnet package. 27 Shrinkage parameter, lambda, was estimated by 10-fold cross-validation. The model was trained with the number of cells and levels of inflammatory mediators shown in Figure 2, as well as with age, sex, lesion level (paraplegic or tetraplegic), and severity (American Spinal Injury Association Impairment Scale [AIS] grade) of each participant.
To build a receiver operating characteristic (ROC) curve and to calculate the area under the ROC curve (AUC) we employed the library pROC. 28 The decision threshold of the lasso regression outcome for classifying patients as with or without infections was determined from the ROC curve according to the maximum Youden's J statistic, useful for imbalanced classification. 29 Then, accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of the lasso regression model were estimated. A precision-recall (PR) curve was built employing the library PRROC. 30
Results
Changes in immune cell populations and inflammatory mediators at 4 weeks after injury are more prominent in patients who develop infections afterwards
The 81 patients with SCI included in the study were divided into two groups according to whether they suffered from infections in the following 12 weeks (57 patients) or they were infection free within the observation period (24 patients; Table 2). Except for the occurrence of infections, both groups of patients exhibited similar clinical and demographic characteristics at the baseline (Table 2). A first infection episode occurred across the whole period of the study, although skewness toward earlier times was observed: median time of infection was 33 days after baseline (Fig. 1A). Infections before 4 weeks occurred in 6 of 40 patients (13%) who developed them later on and in 3 of 15 patients (20%) who remained free of them (Fig. 1B). Thus, frequency of infections before 4 weeks does not seem to affect frequency afterwards (Fisher's exact test p-value = 0.69).
Relationship between Infections from 4 to 16 Weeks and Demographic and Clinical Variables of Patients with Spinal Cord Injury
Fisher's exact test p-value.
AIS, American Spinal Injury Association Impairment Scale.
We compared the immune cell populations and inflammatory mediators of both groups of patients in the subacute phase (4 weeks after injury) with those of healthy subjects as the reference. As shown in Figure 2, changes in immune cell populations and inflammatory mediators were more prominent among patients who suffered from infections in the follow-up period, whereas patients without infections had intermediate levels between those of controls and patients with infections. Indeed, the numbers of total leukocytes, neutrophils, and eosinophils were significantly higher, whereas those of lymphocytes were significantly lower only in patients suffering from infections compared with control subjects (Fig. 2). Neutrophil to lymphocyte ratio and platelet numbers were also higher in patients with infections than in those without infections, and the values of both groups of patients were significantly higher than those of control subjects (Fig. 2). Among the inflammatory mediators, the levels of the chemokine eotaxin-1 (CCL11) were significantly lower only among patients who afterwards suffered from infections (Fig. 2J), whereas the levels of TGF-ß1 and BDNF were significantly lower in both groups of patients compared with control subjects (Fig. 2D,H). No statistically significant differences were reached between patients with infections and patients without them.
The systemic immune profile at 4 weeks after injury may predict the occurrence of infections
Lasso logistic regression was applied to automatically select the cell populations, inflammatory mediators, and clinical and demographic variables that best predict occurrence of infections. As shown in Table 3, the final model includes motor incomplete lesions (AIS C or D grades) as factors associated with lower odds of developing infections. Among the inflammatory mediators, eotaxin-1 levels are associated with lower odds of infections, whereas IP-10 and, to a lesser extent, MCP1, BDNF, and VEGF-A levels are associated with higher odds. Regarding the cell populations, the numbers of neutrophils and eosinophils are associated with higher odds of developing infections, whereas the opposite is observed for the numbers of lymphocytes, basophils, and monocytes. The decision threshold to discriminate whether the output of the model for a patient corresponds to occurrence of infections was estimated by the Youden's J statistic from the ROC curve. As shown in Figure 3A, the AUC-ROC was 0.83. Applying the optimum threshold value results in a model accuracy of 0.80 (p-value = 0.046), with a sensitivity (recall) of 0.68, a positive predictive value (precision) of 0.65, a specificity of 0.85, and a negative predictive value of 0.87. To further assess confidence on prediction of infections, we calculated the F1-score, 0.67, and the area under the PR curve, 0.93 (Fig. 3B).
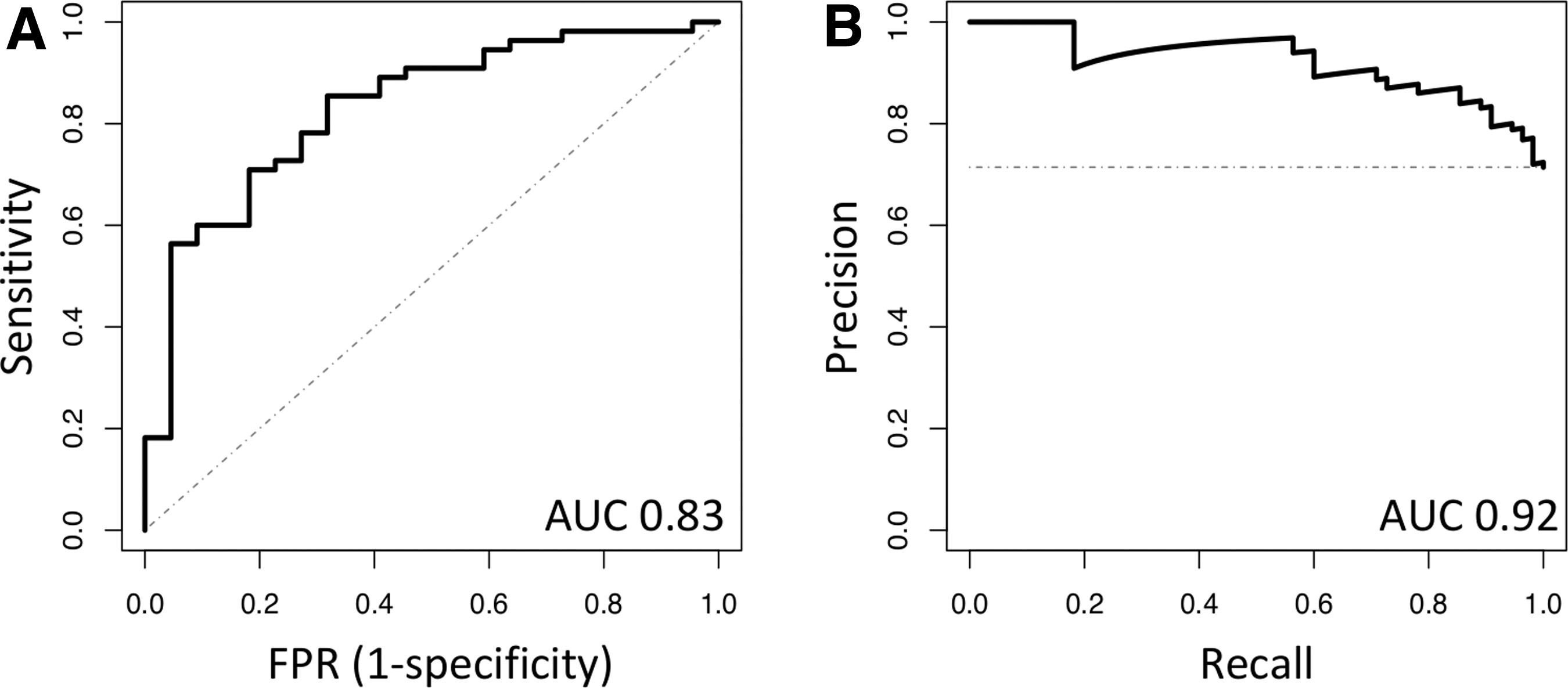
ROC and precision-recall curves for the lasso regression model. AUC, area under the curve; FPR, False positive rate; ROC, receiver operating characteristic.
Variables Automatically Selected by Lasso Logistic Regression as Significant Predictors of Infections
AIS, American Spinal Injury Association Impairment Scale; BDNF, brain-derived neurotrophic factor; IP-10, Interferon-γ-Inducible Protein 10; MCP1, Monocyte chemoattractant protein-1; VEGF, vascular endothelial growth factor.
Discussion
Our results suggest that the alterations in the systemic immune profile are more pronounced in patients who will suffer from infections and may be useful to predict the occurrence of infections in the subacute phase (4 weeks after injury and onwards), when most patients are hospitalized to undergo their physical rehabilitation program.
Previous studies have shown that patients experience transient neutrophilia and lymphopenia during the first week after injury. 11,21 Our results expand the period at which these alterations are still observable in the subgroup of patients who will suffer from infections. Indeed, although only a proportion of patients reached at 4 weeks after injury the clinical thresholds established for lymphopenia (≤106 cells/mL) or neutrophilia (≥8 × 106 cells/mL), the number of lymphocytes was significantly lower among the group of patients who suffered from infections compared with control subjects, whereas the numbers of neutrophils was significantly higher (Fig. 2). This disbalance toward neutrophils is reflected by the increase in the NLR (Fig. 2), which has been previously reported to be higher at earlier time-points (in the first week after injury) among patients who develop infections afterwards. 21 From a mechanistical perspective, NLR is considered an indicator of physical stress because it is increased by the rise in cortisol and catecholamines levels. 31 Thus, the association between more neutrophils and less lymphocytes with higher susceptibility to infections might reflect larger autonomic nervous system disbalance and/or more potent activation of the hypothalamic–pituitary–adrenal axis, the proposed two main causes of immunodepression after SCI. 17 –20
In this regard, the potential effect of pharmacological treatments with glucocorticoids should be also explored. In our cohort there were only two patients treated with glucocorticoids: one from days 24 to 13 before inclusion in the study and the other one from days 79 to 90 after the inclusion. Nevertheless, these patients did not exhibit a higher number of infections or present abnormal numbers of peripheral blood cell populations or levels of inflammatory mediators. Further studies are required to answer whether exogenous glucocorticoids may interfere with susceptibility to infections.
Noticeably, the number of eosinophils was also higher among patients who developed infections, whereas (as occurred with neutrophils and lymphocytes) patients free of infections showed intermediate levels between those of patients suffering infections and those of healthy controls (Fig. 2). Focusing on inflammatory mediators, the same tendency was also detected for eotaxin-1 (Fig. 2). Levels of this chemokine were significantly lower in patients who suffered from infections, whereas those without infections showed intermediate levels between the former and control subjects.
Eotaxin-1 is involved in the release of eosinophils from the bone marrow to blood and their homing into tissues. 32 Indeed, intravenous injection of eotaxin-1 rapidly produces eosinophilia. 33 However, our results show that although eotaxin-1 levels are significantly lower in patients with infections, the number of eosinophils goes in the opposite direction, suggesting that the increase in eosinophils is independent from eotaxin-1-induced release of these cells from the bone marrow. A potential explanation might be found in the upregulation of cytokines associated classically to be produced under allergic eosinophilic responses, such as eosinophilic esophagitis, in which IL-5 and IL-13 produced by pathogenic effector Th2 cells, innate lymphoid cells, or invariant natural killer T cells act as potent chemoattractants for eosinophils. 34 –36
We did determine the levels of Th2-related cytokines (except IL-10, whose levels were below the limit of detection in all samples), but catecholamines and glucocorticoids, elevated after injury and, as previously discussed, main effectors of immunodepression after SCI, 17 –20 are also well-known inducers of skewness toward Th2 activity. 37 To note, Th2 responses have been classically considered as downregulators of Th1-mediated cellular immune responses, essential to fighting against intracellular pathogens and other pathogens. Further work is warranted to study whether an imbalance on immune activity toward a Th2-like profile underlies eotaxin-1-independent increase of eosinophil numbers and whether this activity may enhance the susceptibility to infections in patients with SCI.
We employed lasso logistic regression to automatically select the variables that best predict the occurrence of infections. The final model (Table 3) shows that the numbers of neutrophils and eosinophils are related with higher odds of occurrence of infections, whereas the number of lymphocytes has the inverse relationship (more lymphocytes, lower odds of infections; Table 3). Noticeably, among these cell populations, the one that most affects the odds of infections is the number of eosinophils: odds of infections increase by 3.3 per each increment in 106 eosinophils/mL. Neutrophils present a weaker increment in the odds of infections (1.08 per 106 cells/mL), but it should be taken into consideration that the number of neutrophils among the patients in our study ranged from 5 × 105 to 9.7 × 106 cells/mL, so the final contribution of neutrophil number to the odds of infection may be much more substantial. Indeed, between the two patients with the extreme neutrophil number values, keeping all the other variables constant, the odds of infection would be doubled in the patient with higher neutrophil numbers (1.089.7-0.5 = 2.03).
Something similar occurs with odds associated to lymphocytes (0.78), whose numbers in our cohort of patients varied from 7 × 105 to 4.1 × 106 cells/mL, so the effect of lymphocyte numbers in odds of infections would be reduced almost 60% between the two patients discussed above (keeping all the other variables constant). Monocyte number is also a variable included in the model, but its contribution was more modest (odds = 0.94) and close to its maximum potential effect because in our cohort the highest monocyte number was 1.1 × 106 cells/mL. On the other hand, odds of infection decreased dramatically (0.004) for each increment on 106 basophils/mL, but it should be noted that this concentration of basophils was not achieved in our cohort (basophils mean value, 2 × 104 cells/mL; maximum value, 2 × 105 cells/mL).
Among inflammation-related molecules, eotaxin-1 has the greatest impact on odds of infections (0.95), followed closely by IP-10 (1.03). But in our cohort, the range of values for eotaxin-1 was wider, from 0 to 84.3 pg/mL, whereas for IP-10 the range was from 0 to 60 pg/mL. MCP-1, BDNF, and VEGF-alpha were also included in the model, but their contribution was much weaker (Table 3).
The association between the immunological profile of patients with SCI and their susceptibility to infections could be further supported by observing that a particular immunological profile is related to the number of infections or their duration. Unfortunately, our cohort was not suitable for exploring these issues because the number of patients with 0, 1, 2, 3, or 4 infections were (respectively) 24, 26, 19, 7, and 5; too few patients had 3 or 4 infections in order to conduct a reliable statistical analysis. Regarding the duration of infections, our cohort was quite homogenous and long-term infections did not occur. Indeed, the 95% confidence interval of infection duration was 8.1 ± 0.56 days, with an interquartile range from 6 to 10 days, and a maximum length of infection of 16 days.
The lasso logistic regression model also incorporates AIS C or AIS D lesions as factors that decrease the odds of infections. A potential explanation, in line with the discussion above, may be that less severe spinal cord lesions have a less severe effect on the immune system. In this regard, the association of infection occurrence with neurological and functional recovery is statistical, not causal: it still remains uncertain as to whether it is infection (or the immunodepression that underlies higher infection susceptibility) that impairs neurological recovery, or rather that lesion severity determines recovery, immunodepression, and susceptibility to infections.
A limitation of our study is the absence of a validation cohort to test the applicability of the model to predict infection occurrence in other data sets. But overall, our results show that the alteration of the systemic immune profile at 4 weeks after SCI is more pronounced in those patients who afterwards suffer from infections and it may serve to predict the occurrence of infections. Further work is needed to precisely identify the mechanisms underlying these differences and explore whether therapeutic strategies could be developed to harness the immune system in order to prevent infections.
Funding Information
This work was funded by the Ministry of Science and Innovation of Spain (MCIN)/Agencia Estatal de Investigacion (AEI)/DOI 10.13039/501100011033, grant ID PID2020-120652RB-I00 (to DGO and AAM).
Footnotes
Author Disclosure Statement
No competing financial interests exist.