
Abstract
The purpose of the present investigation was to assess the effects of whole-body exercise on the anaerobic threshold in individuals with spinal cord injury (SCI). Maximal oxygen uptake (VO2max) and oxygen uptake at anaerobic threshold (AT) were measured before and after six months of hybrid functional electrical stimulation row training in 47 participants with SCI aged 19–63, neurological levels of injury C4–L1, American Spinal Injury Association Impairment Scale grades A–D, and time since injury at enrollment from three months to 40 years. Changes in VO2max differed with time since injury, with greater increases earlier post-injury. The early chronic group (<3 years since injury; n = 31) increased VO2max from 1.65 ± 0.54 L/min at baseline to 1.83 ± 0.66 L/min at six months (p < 0.05), while the late chronic group (>3 years since injury; n = 16) did not change (1.42 ± 0.44 at baseline to 1.47 ± 0.41 L/min at six months, p = 0.36). Consistent with VO2max changes, AT increased in the early chronic group (1.03 ± 0.31 to 1.20 ± 0.40 L/min, p < 0.05) and did not change in the late chronic group (0.99 ± 0.31 to 0.99 ± 0.26 L/min, p = 0.92). Cumulative duration of exercise training was positively correlated to change in VO2max (r = 0.475, p < 0.05) but not to change in AT. Hybrid functional electrical stimulation row training is effective for increasing aerobic capacity and anaerobic threshold in individuals with SCI; however, these fitness benefits are only significant in individuals initiating the exercise intervention within three years of injury.
Introduction
Anaerobic threshold (AT) is the exercise intensity at which the requirement for adenosine triphosphate (ATP) eclipses the capacity of oxidative metabolic pathways. At work rates above the AT, muscles must employ anaerobic processes to maintain cellular ATP, leading to production of lactate and other metabolites that results in muscle fatigue and curtailment of exercise. 1 Hence, the AT must be sufficiently high to permit vigorous exercise for durations that result in significant physiological adaptations.
Indeed, improvements in AT may be more accountable for increased exercise performance than higher aerobic capacity (maximal oxygen uptake, VO2max) after training. 2,3 Although higher aerobic capacity allows for higher intensity exercise, it is AT that defines the upper limit of intensity that can be maintained for exercise training. This is important because sustained training at vigorous intensities with oxygen uptake at or above 21 mL/min/kg more effectively reduces cardiovascular risk than low intensity exercise, even with equivalent total energy expenditure. 4,5 Therefore, individuals with an AT above this level will be able to exercise at higher intensities for longer, garnering greater cardioprotective and other health benefits from exercise training.
Spinal cord injury (SCI) reduces the capacity to engage in high intensity aerobic exercise because of skeletal muscle paralysis. Accordingly, individuals with SCI have some of the lowest aerobic capacities compared with uninjured individuals of any age, 6 commonly not even reaching 21 mL/min/kg, regardless of AT. Given the cardiometabolic morbidity prevalent in this population, 7,8 it is imperative to seek aerobic training paradigms that maximize the engaged muscle mass to improve both VO2max and AT.
One approach is to use functional electrical stimulation (FES) to activate paralyzed muscles via electrically induced contractions to enable rowing, cycling, and other forms of hybrid FES-exercise. Although we previously found an increase in VO2max up to 37% after six months of FES-assisted row training in those with SCI, 9,10 it is unknown whether this training can improve AT across a range of time since injury and injury level.
Adaptations in mitochondrial content and capillary density intrinsic to the muscle are primarily responsible for setting oxidative capacity 11 and hence are determinative of AT. 12 Percutaneous electrical stimulation, however, predominantly engages fast-twitch muscle fibers, 13,14 which are best suited for anaerobic activity. Therefore, exercise training with FES may not be capable of increasing AT. In addition, in the first years after injury, the disproportionate atrophy of slow-twitch, oxidative muscle fibers results in lower oxidative capacity in paralyzed muscles. 15
These progressive changes in muscle composition could further limit the ability of FES-assisted exercise training to increase AT despite engaging more muscle mass. On the other hand, long-term FES has been shown to result in conversion of muscle fibers from fast-twitch glycolytic toward a more oxidative profile, 16 similar to that seen in able-bodied individuals with exercise training. Therefore, it is possible that weekly FES-assisted exercise training may increase AT, in addition to VO2max. Moreover, greater time since injury results in greater muscle atrophy and a proportional increase in glycolytic fibers. Hence, changes in AT in individuals with longer time since injury may be lesser than those less chronically injured.
Therefore, we retrospectively investigated whether six months of FES row training improved AT in individuals with SCI. Based on the previously demonstrated improvement in aerobic capacity after this training regimen, we hypothesized that AT would increase with aerobic capacity and that this effect would differ between participants with early (<3 years) compared with late (>3 years) chronic SCI.
Methods
Subject population
Data were retrospectively assessed from 47 individuals (3 women) who had participated in the Exercise for Persons with Disabilities program at Spaulding Hospital Cambridge or our research group's formal exercise studies, all of which followed the same protocol for exercise testing and training. Descriptive statistics of demographics are shown in Table 1, with injuries indicated according to the International Standards for Neurological Classification of Spinal Cord Injury. 17
Participant Characteristics (n = 47)
bpm, beats per minute; NLI: neurological level of injury; AIS, American Spinal Injury Association Impairment Scale.
All values are presented as mean ± standard deviation. Maximal heart rate determined during graded exercise test. Early chronic <3 years, late chronic >3 years since spinal cord injury.
All participants were at least three months since injury given the need to be medically stable and on outpatient status to participate in the study. Time since injury was dichotomized to <3 years (early chronic) and >3 years (late chronic) after empirically recognizing that differentiation in the data was present at this cutoff. The early and late chronic groups were balanced with regard to neurological level of injury such that the proportions of those with paraplegia and tetraplegia were roughly even in both groups.
Individuals were excluded if they were taking cardioactive medications or had a history of cardiopulmonary disease, diabetes mellitus, neurological disorders (other than SCI), ongoing pressure injuries, peripheral nerve compression, or rotator cuff tears that would limit ability to row. The Institutional Review Board at Spaulding Rehabilitation Hospital approved all procedures, and all participants provided written informed consent.
FES row training and testing
To facilitate high intensity exercise, individuals with SCI used a hand-activated electrical stimulator (Odstock 4 Channel Stimulator Kit, Odstock Medical Limited Inc., Salisbury, UK) and indoor rowing ergometer (Model D Indoor Rower, Concept2 Inc., Morristown, VT) with adaptations (Paddlesport Training Systems/Vermont Waterways Inc., East Hardwick, VT). These have been described previously, 18 but briefly, a hand activated button on the rower handle allowed the synchronization between voluntary upper body rowing movements and electrical stimulation of lower body rowing movements.
Subjects participated in training sessions at a goal of three days/week at 45–60 min per session consisting of multiple short intervals of FES rowing. Exercise intensity increased from 60–70% to 75–85% of heart rate reserve established from graded exercise testing at the beginning of the intervention. Duration of rowing, heart rate, power (watts), and total distance rowed were recorded on a per-visit basis.
Participants completed peak graded FES rowing exercise tests pre- and post-six months of FES row training. The pre-test was conducted once the participant developed sufficient muscle strength and endurance to allow continuous rowing for >10 min. Before testing, individuals had not eaten for 2 h and had refrained from caffeine and alcohol for 24 h and vigorous activity for 48 h. 19 The graded exercise test consisted of an increase in work output every 1–2 min until volitional exhaustion for a total testing duration goal between eight and 12 min.
The VO2 was determined from computer-assisted open circuit spirometry (TrueOne 2400, Parvo Medics Inc., Sandy, UT). Ventilation and expired oxygen and carbon dioxide were measured to determine oxygen uptake, carbon dioxide output (VCO2), and respiratory exchange ratio (RER). Attainment of VO2max was defined as meeting at least three of the following validated criteria: (1) plateau in oxygen consumption despite increasing workload, (2) RER ≥1.1, (3) 85% of age-predicted maximal heart rate (220–age), (4) fingerstick lactate >8 mmol/L (Lactate Plus Meter, Nova Biomedical, Waltham, MA) between 120–180 sec after test completion, (5) rate of perceived exertion (RPE) on Borg scale ≥17 (scale range 6–20), as well as (6) decline in power >20 watts despite maximal leg stimulation. 20
The AT during graded exercise testing was determined by the V slope method validated by Beaver and associates, 21 in which VO2 is plotted against VCO2 (Fig. 1). This automated method uses a piecewise regression analysis to identify a breakpoint where increases in VCO2 exceed those in VO2, resulting in a steeper slope. Past this breakpoint, excess CO2 production indicates bicarbonate buffering of lactic acid from anaerobic metabolism. The V slope method provides a sensitive index for AT even in those individuals with higher-level, motor-complete SCI. 22 Moreover, this method may be more appropriate than methods using minute ventilation for assessing AT in individuals with SCI because of known differences in peripheral ventilatory chemosensitivity. 23

Example of V slope plot during graded exercise test. Individual data points represent 10-sec averages in gas exchange. At the anaerobic threshold, increases in carbon dioxide production (VCO2 in L/min) exceed increases in oxygen uptake (VO2 in L/min).
Data and statistical analysis
Maximal values for oxygen consumption, minute ventilation, respiratory exchange ratio, and heart rate were determined from the highest, non-overlapping 10-sec averages during graded exercise tests generated with custom code (MATLAB R2018b, Mathworks Inc., Natick, MA). Neurological level of injury was treated as a dichotomous variable (tetraplegia vs. paraplegia). Average training intensity was calculated from the difference between average training heart rate (across all training sessions) and resting heart rate divided by heart rate reserve; this method has been validated for endurance training. 24 Training impulse was determined by multiplying cumulative training duration by average training intensity. The VO2max and AT values were analyzed both as absolute values and relative to body mass because of the correlation between oxygen consumption and body mass; AT was also analyzed relative to VO2max.
Differences between pre- and post-tests and between early chronic and late chronic groups were assessed via two-way repeated measures analysis of variance (ANOVA) and post hoc paired and unpaired t tests. The Pearson r was used to assess relationships between training variables and maximal exercise parameters. Significance was set at p < 0.05. Tests were run using SPSS Statistics 28.0 (IBM, Armonk, NY). Values are presented as means ± standard deviation.
Results
In response to the graded exercise tests, there were no significant differences between early and late chronic groups in average maximal heart rate (baseline: 151 ± 29 vs. 149 ± 20 bpm, p = 0.841; 6 months: 154 ± 27 vs. 154 ± 21), average maximal RER (baseline: 1.26 ± 0.09 vs. 1.28 ± 0.12, p = 0.630; 6 months: 1.26 ± 0.11 vs. 1.26 ± 0.10), or average maximal RPE (baseline: 18 ± 1 vs. 18 ± 1, p = 0.881; 6 months: 18 ± 2 vs. 18 ± 1). Both amount and intensity of exercise training were equivalent between early and late chronic groups (Table 2).
Exercise Training Parameters in Early Chronic and Late Chronic Groups
HR, heart rate; TRIMP, training impulse (training intensity
All values are presented as mean ± standard deviation.
Changes in VO2max differed with time since injury; greater increases were demonstrated in those with less time since injury (Fig. 2). The early chronic group significantly increased VO2max by 11% from a baseline of 1.65 ± 0.54 L/min to 1.83 ± 0.66 L/min (p < 0.05, Table 3); relative to body mass, VO2max increased from 20.41 ± 6.2 mL/min/kg to 22.28 ± 7.3 mL/min/kg (p < 0.05). In the late chronic group, even though 10 of 16 individuals increased VO2max by an average of 0.19 L/min (16.6%) from baseline, VO2max in the group as a whole did not increase significantly (1.42 ± 0.44 L/min to 1.47 ± 0.41 L/min, p = 0.36; 17.76 ± 5.50 mL/min/kg to 18.72 ± 6.18 mL/min/kg, p = 0.22). Moreover, cumulative duration of exercise training was positively correlated to change in VO2max (r = 0.475, p < 0.05) only in the early chronic group.
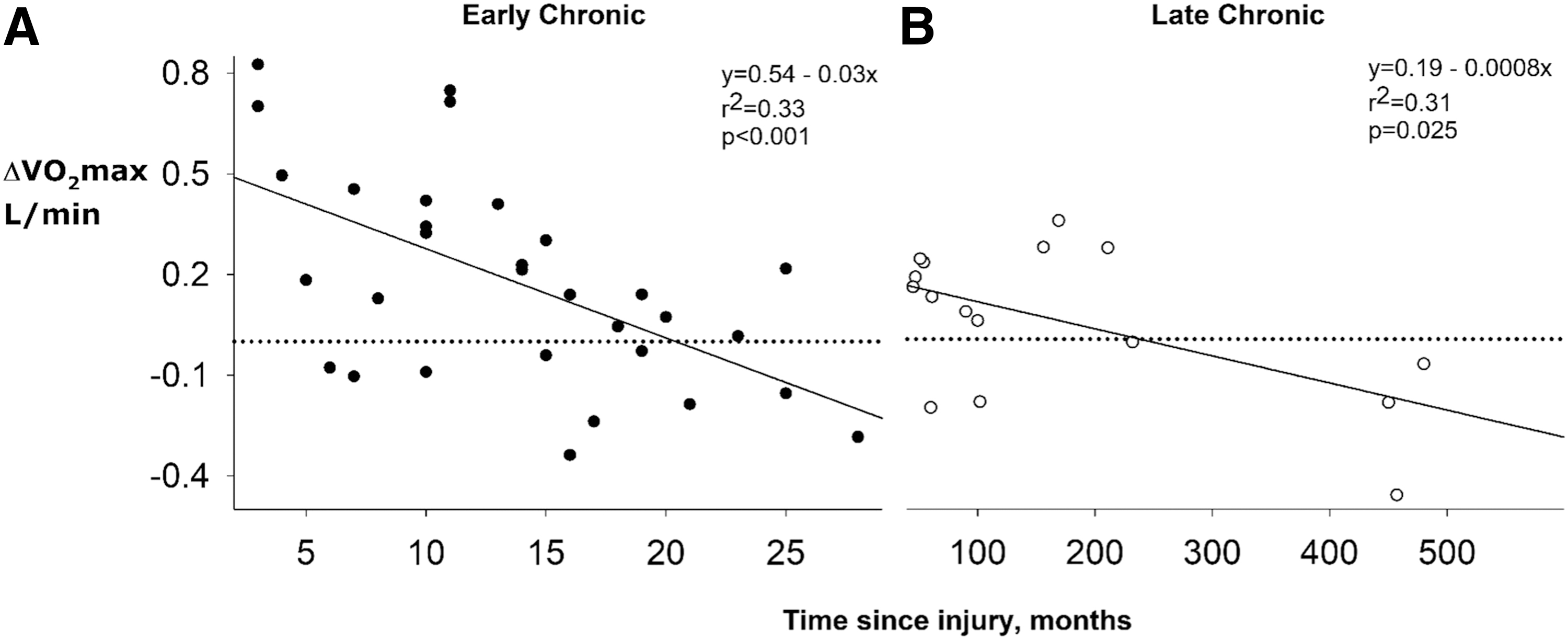
Relationship between time since injury (months) and change in maximal oxygen uptake. (
Changes in Metabolic Parameters from Baseline to Post-Training in Early and Late Chronic Spinal Cord Injury
SCI, spinal cord injury (early chronic <3 years, late chronic >3 years); ANOVA, analysis of variance; VO2max, maximal oxygen uptake; AT, anaerobic threshold; AT%VO2max, AT as percent of VO2max.
Significant within-group change from pre- to post-training (p ≤ 0.05); †significant across group difference at same time point (p ≤ 0.05).
Values are presented as mean ± standard deviation.
There was a significant interaction between group and time for AT (F(1,45) = 5.807, p < 0.05); AT increased in the early chronic group by 16% (1.03 ± 0.31 L/min to 1.20 ± 0.40 L/min, p < 0.05; 12.82 ± 3.80 mL/min/kg to 14.77 ± 4.71 ml/min/kg, p < 0.05) but not in the late chronic group (0.99 ± 0.31 L/min to 0.99 ± 0.26 L/min, p = 0.92; 12.35 ± 3.98 mL/min/kg to 12.65 ± 4.06 mL/min/kg, p = 0.63). Similarly, AT as a percent of VO2max increased in the early chronic group 3.6% (63.7 ± 9.8% to 67.3 ± 7.8%, p < 0.05) but not in the late chronic group (69.4 ± 7.7% to 68.0 ± 5.6%, p = 0.55).
When data from only those who increased VO2max were analyzed, we found that the increase in AT was still greater in the early chronic group than in the late chronic group (0.25 L/min vs. 0.10 L/min, p = 0.05), consistent with greater increases in VO2max. Moreover, exploratory post hoc analysis showed a significant effect for level of injury on AT (F(1,45) = 5.193, p < 0.05). Across all participants, individuals with paraplegia increased AT (1.12 ± 0.23 L/min to 1.31 ± 0.34 L/min, p < 0.05; 14.41 ± 3.15 mL/min/kg to 16.64 ± 3.83 mL/min/kg, p < 0.05), whereas those with tetraplegia did not (0.89 ± 0.34 L/min to 0.93 ± 0.30 L/min, p = 0.35; 10.67 ± 3.59 mL/min/kg to 11.10 ± 3.44 mL/min/kg, p = 0.37).
Discussion
Anaerobic threshold is a critical determinant of the ability to exercise train at intensities that reduce health risks. Although hybrid-FES exercise can be effective for improving VO2max, our data show that it may be ineffective for improving AT in those more than three years since injury or in those with tetraplegia. Indeed, those with longer time since injury may not even improve VO2max with this form of exercise. Therefore, it may be critical to begin hybrid-FES exercise within three years of injury to garner the benefits of exercise training.
Improvement in VO2max and AT in the early chronic group and not in the late chronic group corroborate previous findings that those early since injury significantly increase both VO2max and AT with hybrid-FES row training 25 while those further from injury may not even increase VO2max. 26 To our knowledge, the present study is the first to compare changes in AT between those with early versus late injury following an exercise intervention and, moreover, in a relatively large sample. Given that both groups exercised, on average, with equivalent intensity and duration, group differences in AT changes were not because of unequal participation in training.
Although there was a difference in average age between the groups (29 vs. 42 years), previous research indicates that age does not influence changes in AT in response to endurance training. 27 When separated at the median age, younger participants did tend to increase AT more than older participants (0.15 L/min vs. 0.08 L/min, p = 0.33), but this difference was not nearly as strong as groups difference by time since injury (0.18 L/min in early chronic vs. 0.01 L/min in late chronic, p = 0.02). Further, when the analysis was restricted to only those participants under 40 years of age, the early chronic group increased AT (1.02 ± 0.30 L/min to 1.18 ± 0.40 L/min; p < 0.05) while the late chronic group did not (0.87 ± 0.31 L/min to 0.92 ± 0.25 L/min; p = 0.46).
Rather than amount of training or age, the mechanism for the lack of improvement in AT may instead be the progressive atrophy of type I oxidative fibers leading to the predominance of type II glycolytic fibers in late chronic SCI. These changes would predominate in the paralyzed muscles of the legs, leaving the arms relatively intact for hybrid exercise except in those with higher level cervical injuries. Biopsy data from Anderson and colleagues 16 demonstrate that weekly hybrid-FES exercise does not increase type I fibers substantially in paralyzed muscles in late chronic SCI, and interestingly, the only participant in this study with an increase in proportion of type I fibers had been injured for only three years. 16
This finding suggests that the late chronic group in our study, who had an average time since injury of 14.4 years, may not have increased AT because of inability to increase their muscle oxidative capacity with hybrid-FES exercise. In contrast, the early chronic group with an average time since injury of only 1.1 years may have retained ability to increase AT because they had not yet undergone such significant decline in muscle oxidative capacity.
Certainly, exercise confers health benefits, especially for sedentary individuals. Regardless of time since injury, those with SCI still are advised to regularly participate in aerobic exercise 28 despite the lack of consensus about the efficacy for improving physical health in this population. 29 The inadequacy of exercise interventions to increase AT in those individuals with SCI longer than 3 years, however, suggests greater difficulty reaching exercise training intensities that will help to reduce health risks.
Our data help to explain why recent longitudinal interventions including FES have found minimal cardiometabolic health improvements, 30,31 which raises the question of whether weekly sessions FES-assisted exercise are potent enough to induce the peripheral changes in muscle needed to raise AT in individuals greater than three years from injury. Individuals were successfully enrolled as soon as three months after their acute SCI, demonstrating this training is feasible at a high level of intensity shortly after injury in the outpatient setting. Further studies are needed to identify whether earlier intervention, potentially in the acute inpatient rehabilitation setting, is beneficial. Both from our experience and logistically, this is a realistic possibility as long as participants are stable.
Those with late chronic SCI had a higher ratio of AT to VO2max or relative AT before training. This derived from a lower VO2max and a similar absolute AT compared with the early chronic group. As described earlier, the absolute AT relates to the exercise level that can be maintained to optimally reduce health risk, whereas the relative AT is generally more indicative of training state. The higher relative AT in the late chronic group, however, was not indicative of greater fitness before training but merely because of a lower VO2max.
This is analogous to what has been observed in older populations without SCI. With aging, VO2max decreases disproportionately more than AT, resulting in a higher relative AT. 32,33 Hence, low baseline VO2max and high relative AT in the late chronic group may be because of significant muscle atrophy, 34,35 not unlike the effect of age-related sarcopenia. 36 This is in accord with the concept that chronic SCI represents an advanced state of aging. 37,38 Interestingly, the finding that absolute AT was equivalent in the early and late chronic groups may suggest that there is some level below which absolute AT will not fall.
Study limitations
A key limitation of the present study is the inability to provide a clear mechanism to explain changes, or lack thereof, in AT. A prospective, randomized study that includes tissue samples from the stimulated muscles may provide insight to whether the lack of adaptations in AT do relate to fiber type changes. In addition, the relatively short duration (6 months) of our hybrid-FES training intervention may not be sufficient to generate the changes in muscle needed to increase AT, especially given that the average participant exercised less than 4 h per month.
The strength training sessions in preparation for a graded exercise test before the intervention may have resulted in fitness improvements, although these effects could not have been observed because of the inability of obtaining an exercise test before participants being able to FES row up to high exercise intensities. Previous studies of hybrid-FES exercise have found that both metabolical 25 and muscle histological 16 changes in response to exercise continue to accrue beyond six months of training. Theoretically, the lack of improvement in muscle oxidative capacity with this duration of hybrid-FES exercises may not be indicative of the possible increase in AT with longer term training.
Conclusion
The FES row training is an effective method for increasing maximal oxygen consumption and can increase AT in individuals with SCI. Our findings, however, suggest exercise training should be initiated early after injury for maximal benefits. Given the significant cardiovascular morbidity and mortality associated with SCI, exercise interventions in this population should seek to achieve exercise intensities high enough to reduce cardiovascular risk, and these intensities are critically dependent on AT.
Footnotes
Acknowledgments
Dr. Solinsky's time was protected through a career development award, 1K23HD102663-01. We thank all the volunteers for their participation in this study and the exercise facility staff for setting up equipment, facilitating exercise training, and collecting data.
Funding Information
This work (clinical trial registration number NCT02139436) was supported by the National Institutes of Health (R01HL117037) and the National Institute on Disability, Independent Living, and Rehabilitation Research (90SI5021).
Author Disclosure Statement
Authors of the study have no commercial interest in the results of the research. The results of the present study are presently clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.