
Abstract
Balanced crystalloids may improve outcomes compared with saline for some critically ill adults. Lower tonicity of balanced crystalloids could worsen cerebral edema in patients with intracranial pathology. The effect of balanced crystalloids versus saline on clinical outcomes in patients with traumatic brain injury (TBI) requires further study. We planned an a priori subgroup analysis of TBI patients enrolled in the pragmatic, cluster-randomized, multiple-crossover Isotonic Solutions and Major Adverse Renal Events Trial (SMART) (
Introduction
Traumatic brain injury (TBI) is common reason for hospital admission after falls, motor vehicle crashes, assault, and other mechanisms of injury. In 2014, TBI resulted in 2.5 million emergency department visits in the United States, with over 56,000 deaths. 1 Additionally, TBI results in significant morbidity for survivors, with physical, cognitive, and behavioral sequelae that can persist long after the initial injury. 2
Recently, the use of balanced crystalloids (e.g., Plasma-Lyte or lactated Ringer's) rather than saline (0.9% sodium chloride) has been reported to improve clinical outcomes for some groups of critically ill adults. 3,4 Saline has historically been the most common intravenous fluid administered to hospitalized patients, but its high concentration of chloride relative to plasma is associated with the development of hyperchloremia, metabolic acidosis, renal vasoconstriction, hypotension, and altered immune function. 5 –13 Balanced crystalloids contain more physiologic concentrations of electrolytes, including sodium and chloride compared with those found in plasma, aiming to mitigate the derangements associated with saline administration.
Although balanced crystalloids are commonly administered to critically ill and injured adults, their efficacy and safety for adults with TBI is uncertain. 4,14,15 On one hand, balanced crystalloid's more physiologic chloride content and acid-base composition could potentially prevent acute kidney injury, inflammation, and metabolic acidosis among severely injured trauma patients. On the other hand, the tonicity of balanced crystalloid solutions is lower than that of saline, which could potentially decrease serum osmolality, contribute to cerebral edema, and cause secondary injury among patients with TBI. Balanced crystalloids and saline have been compared among patients with TBI in one small pilot trial, which reported no difference in mortality or intracranial hypertension, and in a subgroup analysis of one recent, large, randomized trial, which reported a higher incidence of mortality with balanced crystalloids compared with saline. 16,17
To examine the effect of balanced crystalloids versus saline on clinical outcomes of adults with TBI, we performed a secondary analysis of the dataset from a large, pragmatic, clinical trial.
Methods
Study design and oversight
The Isotonic Solutions and Major Adverse Renal Events Trial (SMART) was a pragmatic, unblinded, cluster-randomized, multiple-crossover trial comparing balanced crystalloids with saline for intravenous fluid administration among critically ill adults admitted to Vanderbilt University Medical Center between June 1, 2015, and April 30, 2017. This study is a secondary analysis of the subgroup of patients with TBI enrolled in the SMART trial. The SMART trial was approved by the Institutional Review Board (IRB# 190159) at Vanderbilt University Medical Center with waiver of informed consent (see Supplementary Appendix), was registered online prior to initiation (NCT02444988, NCT02547779), and was overseen by an independent Data and Safety Monitoring Board (DSMB). Further details regarding the original study protocol, statistical analysis plan, and outcomes were reported previously. 4,18 Notably, fluid therapy in the emergency department and operating room was coordinated with the intensive care unit (ICU) to which patients were being admitted to avoid confounding fluid administration prior to ICU admission.
Role of the funding source
The funding institutions had no role in: 1) conception, design, or conduct of the study; 2) collection, management, analysis, interpretation, or presentation of the data; or 3) preparation, review, or approval of the manuscript.
Patient population
In the original SMART trial, all adults (age ≥18 years) admitted to a participating ICU during the study period were enrolled at the time of ICU admission. Patients in the SMART dataset with the diagnosis of TBI were included in this secondary analysis. TBI was considered to be present if billing records for the hospitalization contained any International Classification of Disease, 10th Edition, Clinical Modification System (ICD-10-CM) codes for intracranial injury (S06-) in the first five billing codes.
Data collection
The current study used data from two sources: the dataset for the original SMART trial and a trauma registry prospectively maintained by the institution as part of clinical care. 9,19 Data from the SMART trial dataset and the trauma registry were matched using patients’ medical record numbers and dates of admission. The SMART trial dataset included information on: patient demographics; diagnoses; orders for intravenous fluids and blood products; plasma electrolyte and creatinine values; receipt of renal replacement therapy (RRT); and vital status at hospital discharge. The trauma registry included information on: mechanism of injury; Injury Severity Score (ISS) and head Abbreviated Injury Score (AIS); Glasgow Coma Scale (GCS) scores at admission and discharge; admission systolic blood pressure and pulse; and discharge disposition.
Study outcomes
The primary outcome was 30-day in-hospital mortality. Secondary outcomes included discharge disposition (home with or without assistance, medical facility, or death) and final GCS before discharge. Additional secondary clinical outcomes included: hospital length of stay and the number of days alive and free of mechanical ventilation (ventilator-free days), the intensive care unit (ICU-free days), and RRT (RRT-free days) during the 28 days after enrollment.
Statistical analysis
With 1157 patients in the SMART dataset admitted to the ICU with a diagnosis of TBI, we calculated that this secondary analysis would have 80% statistical power at an alpha level of 0.05 to detect a 7% absolute difference between the balanced crystalloid and saline groups in the primary outcome of 30-day in-hospital mortality, assuming 18% mortality in the saline group based on prior data. 20,21
The primary analysis was an intention-to-treat comparison of 30-day in-hospital mortality between patients assigned to the balanced crystalloids group and patients assigned to the saline group using a logistic regression model accounting for pre-specified baseline covariates. These baseline covariates included three used in the primary analysis of the original trial (age, gender, race) and injury-specific covariates (inter-facility transfer, head AIS, best GCS motor score within 24 h of ICU admission, systolic blood pressure at presentation, and heart rate at presentation).
To evaluate the consistency and robustness of the findings of the primary analysis, we performed five sensitivity analyses: 1) population restricted to patients receiving ≥2000 mL of isotonic crystalloid in the 72 h after enrollment; 2) population restricted to patients receiving ≥500 mL of isotonic crystalloid in the 72 h after enrollment; 3) exclusion of patients admitted in the week prior to a crossover; 4) exclusion of patients who transferred between ICUs or remained in the ICU through a crossover; and 5) population restricted to each patient's first ICU admission (Supplementary SMART Trauma Data).
We compared outcomes between the balanced crystalloid and saline groups in the primary study population using the same set of pre-specified baseline covariates in logistic regression modeling for dichotomous outcomes and proportional odds modeling for ordinal and continuous outcomes. Results are presented comparing the balanced crystalloid group to the saline group (referent) with adjustment for covariates. Accordingly, an odds ratio greater than 1 in the setting of an ordinal or continuous variable represents a higher incidence or value of the outcome for patients in the balanced group compared with the saline group. We compared patients’ receipt of hypertonic saline and mannitol over the 14 days after enrollment between the balanced crystalloid and saline groups. We assessed whether baseline plasma sodium, chloride, or bicarbonate concentration modified the effect of study group on in-hospital mortality using tests of interaction in a multivariable logistic regression model.
Other between-group comparisons were made with the Mann-Whitney U test for continuous variables and chi-square test for categorical variables. Continuous variables were presented as mean and standard deviation or median and interquartile range; categorical variables were presented as frequency and proportion. A two-sided p value <0.05 indicated statistical significance, and no adjustments were made for multiple comparisons. All analyses were performed using R version 4.1.1 software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Of the 15,802 patients in the SMART trial dataset, 1157 (7.3%) had a diagnosis of TBI. Mean (standard deviation [SD]) age was 51 (21) years and 64% were male. The 588 patients with TBI assigned to the balanced crystalloids group had similar baseline characteristics to the 569 patients assigned to the saline group (Table 1). The median (IQR) maximum head/neck AIS scores were 3.0 (2.2-4.0) and 3.0 (3.0-4.0) in the balanced crystalloid and saline groups, respectively. Mean (SD) ISS scores were 19.3 (10.2) and 18.6 (9.7), respectively. Plasma creatinine at admission was similar between the groups (Table 1).
Participant Characteristics at Admission
A total of 31 patients in balanced crystalloid group and 28 in the saline group did not have a baseline creatinine value available.
One patient in the balanced crystalloid group and three in the saline group did not have a baseline GCS score available.
Nine patients in balanced crystalloid group and 10 in the saline group did not have GCS scores available.
SD, standard deviation; IQR, interquartile range.
Fluid therapy and electrolytes
Because fluid therapy in the emergency department and operating room was coordinated with the ICU to which patients were being admitted, the majority of pre-ICU isotonic fluid administered was consistent with study group assignment (Supplementary SMART Trauma Data Table S5). The mean (SD) volume of isotonic crystalloid between ICU admission and the first of hospital discharge or 30 days was 2037 (3470) mL in the balanced crystalloid group and 1723 (2923) mL in the saline group (p = 0.18). Crossover to the non-study isotonic crystalloid was limited, with the mean volume of balanced crystalloids between ICU admission and the first of hospital discharge or 30 days being 1609 (2849) mL in the balanced crystalloid group compared with 179 (886) mL in saline group. Mean volume of saline was 428 (1409) mL in the balanced group compared with 1544 (2608) mL in the saline group (Fig. 1; Supplementary SMART Trauma Data Table S5). Of the balanced crystalloid administered, 82.9% was comprised of Plasma-Lyte and 17.1% was comprised of lactated Ringer's (Supplementary SMART Trauma Data Table S5). The median volume of non-study intravenous fluid, blood products, and medications did not differ between groups (Supplementary SMART Trauma Data Table S6). The proportion of patients who received hypertonic saline (17% vs. 18%) and/or mannitol (9% vs. 8%) was similar between the balanced crystalloids and saline groups over the first 14 days (Supplementary SMART Trauma Data Tables S3 and S4).
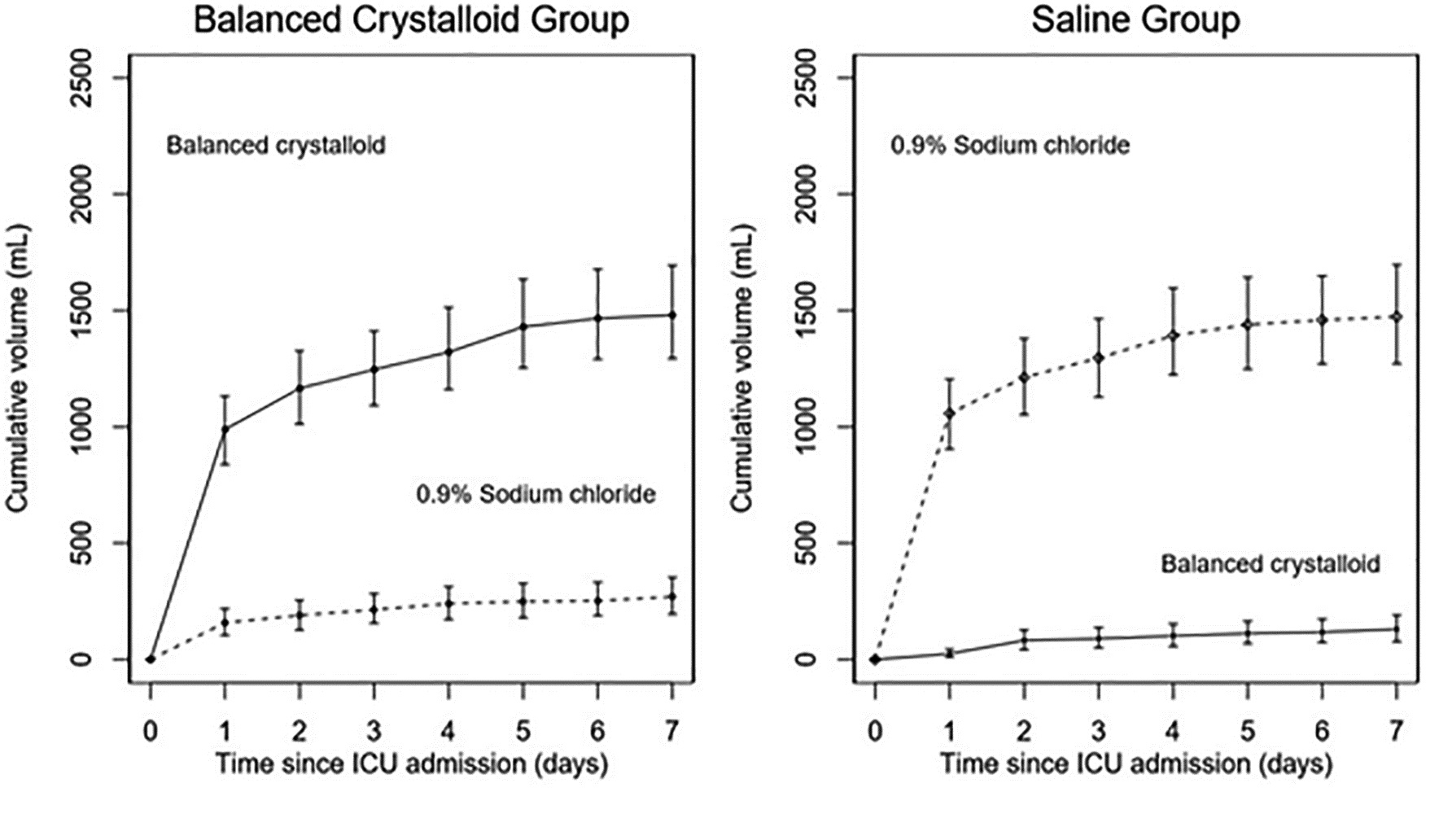
Mean cumulative volume of normal saline and balanced crystalloid solutions by treatment group over the first 7 days of admission. The cumulative mean volume of intravenous balanced crystalloids (solid line) and 0.9% sodium chloride (dotted line) between admission to the intensive care unit (ICU) and hospital Day 7 is shown for patients in the balanced-crystalloids group (left) and the saline group (right). bars indicate 95% confidence intervals.
Serum sodium levels did not differ over the first 7 days and a comparable number of patients in the balanced crystalloid and saline groups had a measured plasma sodium greater than 145 mmol/L (19% vs. 19%; p = 0.92) or less than 135 mmol/L (22% vs. 22%; p = 0.91) during the first 7 days of hospitalization (Fig. 2A). Patients in the balanced crystalloid group had lower serum chloride concentrations (Fig. 2B) and higher serum bicarbonate concentrations (Fig. 2C) over the first 7 days. Patients in the balanced crystalloids group were less likely to experience a plasma chloride concentration greater than 110 mmol/L (34% vs. 41%; p = 0.014) and more likely to experience a plasma bicarbonate concentration greater than 30 mmol/L (14.5% vs. 9.7%; p = 0.02). Mean serum creatinine did not differ between groups over the first 7 days (Fig. 2D), and mean creatinine change from baseline to highest recorded value through study Day 28 was also similar between the balanced crystalloids and saline groups (0.039 ± 0.44 vs. 0.043 ± 0.44; p = 0.92).

Electrolyte concentrations according to group. Mean plasma
Primary outcome
A total of 94 patients (16%) in the balanced crystalloid group died before the earlier of study Day 30 or hospital discharge, compared with 82 patients (14%) in the saline group (adjusted odds ratio [aOR], 1.03; 95% confidence interval [CI], 0.60 to 1.75; p = 0.913; Table 2; Fig. 3). Results were similar in all pre-specified sensitivity analyses (Supplementary SMART Trauma Data Sections 4.1.1-4.1.5 and Supplementary SMART Trauma Data Tables S12–S21). An additional 12 patients—eight (1.3%) in the balanced crystalloid group and four (0.7%) in the saline group—died after day 30 but prior to hospital discharge.
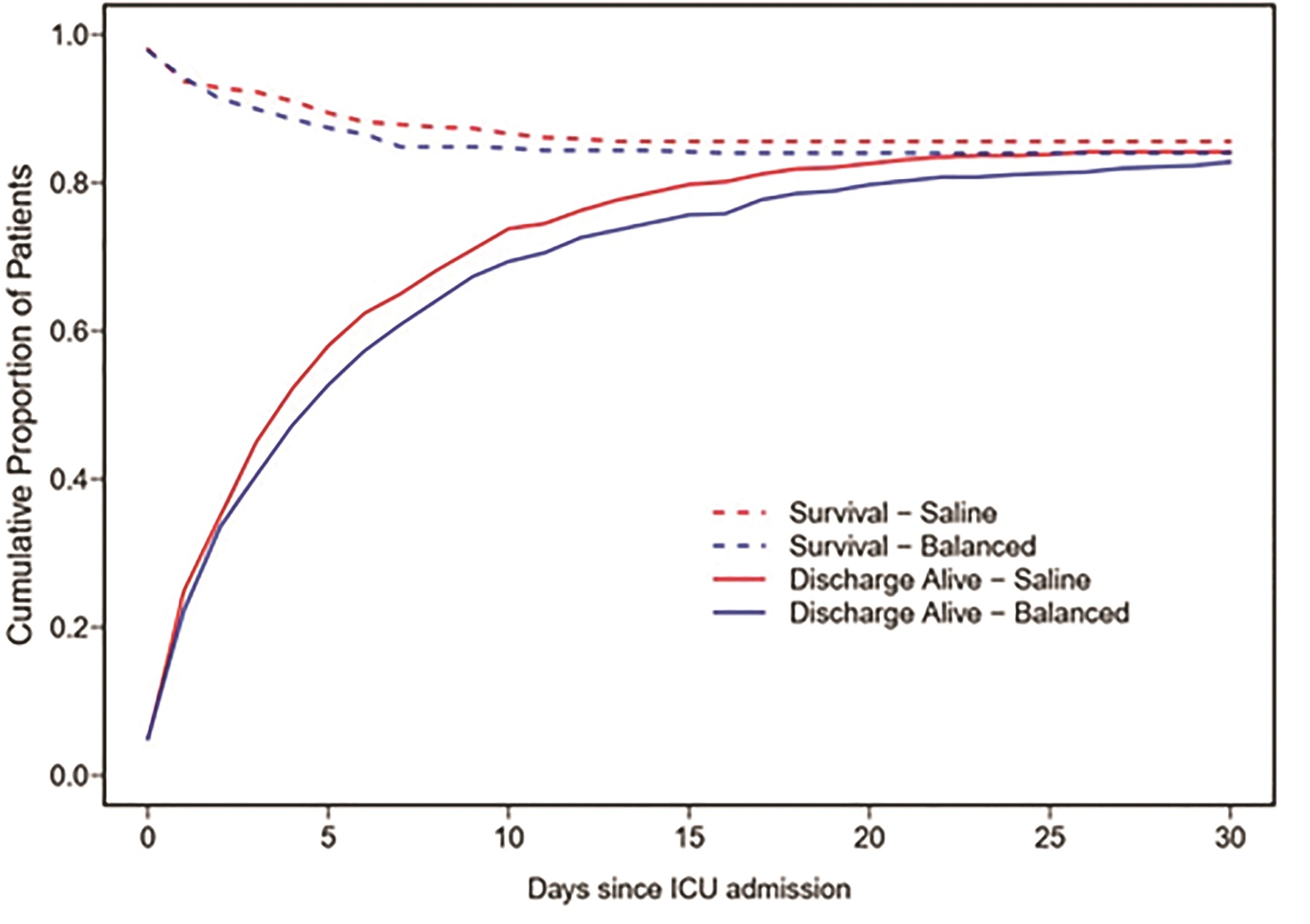
Probability of survival and of being discharged home during the first 30 days following intensive care unit (ICU) admission in patients in both groups. Cumulative proportion of patients surviving (dotted lines) and being discharged from the hospital alive (solid lines) for the balanced crystalloids (blue) and saline (red) groups. Patients above the dotted lines are deceased. Patients between the dotted and solid lines are alive and still in hospital. Patients below the solid lines are alive and discharged from the hospital. Color image is available online.
Clinical Outcomes
For failure-free day outcomes, odds ratio (OR) <1 indicates fewer days alive and free of the failure for the balanced crystalloids group.
This OR indicates that the odds of being more severe at discharge among balanced crystalloids is 1.38 times the odds among saline (1.38 times lower probability of discharge to a more independent discharge disposition in the balanced crystalloid group compared with the saline group).
CI, confidence interval; IQR, interquartile range; SNF, skilled nursing facility; GCS, Glasgow Coma Scale.
Secondary outcomes
A total of 969 patients (83.8%) survived to hospital discharge; 307 patients (52.2%) in the balanced crystalloid group were discharged to home, as compared with 343 (60.3%) in the saline group (p = 0.009). Patients in the balanced crystalloid group were more likely to die or be discharged to another medical facility (aOR, 1.38; 95% CI, 1.02 to 1.86; adjusted p = 0.04). The mean (SD) GCS at death or discharge was 13.0 (4.1) in the balanced crystalloid group and 13.3 (3.8) in the saline group (p = 0.61; (Supplementary SMART Trauma Data Table S8). After controlling for multiple variables, including best GCS within 24 h of admission, GCS at discharge did not differ significantly between the balanced crystalloid group and the saline group (aOR, 0.91; 95% CI, 0.65 to 1.29; adjusted p = 0.61). Hospital length of stay, ventilator-free days, ICU-free days, and RRT-free days did not differ between groups (Table 2). Only two patients, both of whom were in the balanced crystalloid group, received new renal replacement therapy during their hospitalization.
Discussion
In this secondary analysis of a clinical trial, use of balanced crystalloids was not shown to decrease mortality for critically ill adults with TBI compared with use of saline. The findings that use of saline was associated with a numerically lower in-hospital mortality and higher rate of discharge to home may support the hypothesis that use of saline results in better outcomes than use of balanced crystalloids for critically ill adults with TBI.
The results of this secondary analysis differ from the finding of benefit from balanced crystalloids compared with saline in the overall SMART trial, and among subgroups of patients with sepsis, diabetic ketoacidosis, and hyperkalemia. 3,18,22,23 Several potential explanations exist for the difference in findings between this secondary analysis and the results of the overall trial. First, among patients with TBI, the lower tonicity of balanced crystalloid solutions compared with saline might predispose to the development or worsening of cerebral edema, increasing the risk for mortality or functional impairment sufficiently to outweigh any potential beneficial effects of balanced crystalloid solutions on renal function or acid base physiology. This appears consistent with the results of the recent Balanced Solutions in Intensive Care Study (BaSICS), which found at higher 90-day mortality with balanced crystalloids compared with saline among critically ill adults with TBI. 17 Second, patients with TBI are generally at lower risk of acute kidney injury and renal replacement therapy—a mechanism by which fluid composition has been proposed to potentially affect clinical outcomes. 4,24,25 Third, as a subgroup analysis of a clinical trial, these findings may have inadequate power to detect true differences (type II error) or risk identifying differences that are not true due to multiple testing (type I error).
Many patients with TBI receive hyperosmolar treatments, such as hypertonic saline or mannitol, in order to try to reduce cerebral edema. The hypertonicity of these treatments may obviate the overall effect of administering a slightly hypo-osmolar solution such as balanced crystalloids. Serum sodium concentrations did not differ between groups over the first 7 days, potentially reflecting the practice of administering hypertonic saline to target a specific serum sodium value. As such, any potential beneficial or detrimental effect of the hypo-osmolar balanced crystalloid solutions may be attenuated in our subgroup by the use of hypertonic treatments. The high chloride concentration of hypertonic saline may also increase serum chloride levels regardless of the differing concentrations of chloride in balanced crystalloid or saline. Despite this, chloride levels were higher over the first 7 days in the saline group in this study.
This study has several limitations. First, this was a secondary analysis of a single center trial encompassing mild to severe TBI. Second, the overall volume of fluid administered in each arm was relatively low. This reflects current practice in the study trauma ICU, as “maintenance fluid” is discouraged in favor of early enteral nutrition. The relatively low volume of fluid administered in both groups may decrease the ability to detect a difference in outcomes that might be present when patients receive much higher volumes of intravenous fluid.
Third, study fluid administration was not blinded. Unblinded clinicians might have altered the volumes of fluid given depending on the nature of the fluid assigned, although overall volumes of study fluids administered in the two groups were similar. Likewise, unblinded investigators could have treated patients differently in the two arms, especially with regard to use of hypertonic treatments. Overall, the use of hypertonic saline and mannitol was similar between groups, but subtle differences may still have occurred and intracranial pressures were not routinely measured. Fourth, this study only evaluates different isotonic crystalloid administration which represents one aspect of an often complicated and personalized treatment approach to patients with TBI. Finally, while the sensitivity analyses did not alter our conclusions, the subgroups were small and observed effects sizes were insufficient to generate hard evidence for a difference in conclusion.
This study also has several strengths. Patients with a diagnosis of TBI were an a priori defined subgroup of the original trial, were objectively identified using ICD codes from billing diagnoses, and are a group for whom choice of intravenous fluid could have significant effects on clinical outcomes. Second, although a subgroup of the overall ICU population enrolled in the SMART trial, this study represents the largest randomized comparison of balanced crystalloids versus saline in patients with objectively defined TBI. Third, randomization appeared to result in treatment groups with similar baseline characteristics, even within this subgroup of patients. Fourth, while clinicians were able to administer non-assigned fluid in clinical practice during the study, adherence to study group assignment was high and crossover between study fluids was limited.
Conclusion
In conclusion, use of balanced crystalloids was not associated with improved outcomes in critically injured patients with TBI, compared with saline. The confidence intervals cannot exclude a clinically relevant increase in mortality with balanced crystalloids compared with saline and patients receiving balanced crystalloids had a worse discharge disposition.
Footnotes
Authors' Contributions
Study concept and design: S.L., M.C.S., M.W.S., C.J.L., W.H.S, T.W.R. Acquisition of data: S.L., M.C.S., M.W.S., R.E.F., W.H.S, T.W.R. Analysis and interpretation of data: S.L., M.C.S., M.W.S., L.W., C.J.L., W.H.S, T.W.R. Drafting of the manuscript: S.L., M.C.S., M.L.D., W.H.S, T.W.R. Critical revision of the manuscript for important intellectual content: S.L., M.C.S., M.W.S., L.W., M.L.D, C.J.L., R.E.F., O.D.G., W.H.S, T.W.R. All authors had full access to all the data and accept responsibility to submit for publication.
Funding Information
The project described was supported by the VICTR Learning Healthcare System Platform under CTSA award No. UL1 TR002243 from the National Center for Advancing Translational Sciences. Matthew W. Semler was supported in part by the National Heart, Lung, and Blood Institute (NHLBI; K12HL133117 and K23HL143053). Robert E. Freundlich was supported in part by the NHLBI (K23HL148640). Todd. W. Rice was supported in part by the NIH (UL1 TR002243). Data collection used the Research Electronic Data Capture (REDCap) tool developed and maintained with Vanderbilt Institute for Clinical and Translational Research grant support (UL1 TR000445 from NCATS/NIH).
The funding institutions had no role in; 1) conception, design, or conduct of the study; 2) collection, management, analysis, interpretation, or presentation of the data; or 3) preparation, review, or approval of the manuscript. Authors were not precluded from accessing data in the study, and they accept responsibility to submit for publication.
Author Disclosure Statement
Todd. W. Rice reported serving as a consultant for Cytovale, Inc., and as the Director of Medical Affairs for Cumberland Pharmaceuticals, Inc. For the other authors, no competing financial interest exist.
Supplementary Material
Supplementary Appendix
SMART Trauma Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.