
Abstract
Traumatic brain injury (TBI) leads to cognitive linguistic deficits that significantly impact on quality of life and well-being. Digital health offers timely access to specialized services; however, there are few synthesized reviews in this field. This review evaluates and synthesizes reports of digital health interventions in TBI rehabilitation and caregiver education. Systematic searches of nine databases (PsycINFO, MEDLINE, CINAHL, Embase, Cochrane Library, Scopus, Web of Science Core Collection, speechBITE, and PsycBITE) were conducted from database inception to February 2022. Studies were included of interventions where the primary treatment focus (> 50%) was on improving communication, social, psychological or cognitive skills of people with TBI and/or communication partners. Data on participants, characteristics of the interventions, outcome measures and findings were collected. Risk of bias was accounted for through methodological quality assessments (PEDro-P and PEDro+, Risk of Bias in N-of-1 Trials) and intervention description. Qualitative data was analyzed using thematic synthesis. Forty-four articles met eligibility criteria: 20 randomized controlled trials, three single-case experimental designs, six non-randomized controlled trials, nine case series studies, and two case studies. Studies comprised 3666 people with TBI and 213 carers. Methodological quality was varied and intervention description was poor. Most interventions were delivered via a single digital modality (e.g., telephone), with few using a combination of modalities. Five interventions used co-design with key stakeholders. Digital health interventions for people with TBI and their caregivers are feasible and all studies reported positive outcomes; however, few included blind assessors. Improved methodological rigor, clearly described intervention characteristics and consistent outcome measurement is recommended. Further research is needed regarding multi-modal digital health interventions.
Introduction
Traumatic brain injury (TBI) refers to brain injury acquired through a traumatic incident such as a road traffic accident, sporting injury, assault or fall. 1,2 This insult to the brain, caused by an external force, initially produces a diminished or altered state of consciousness 3 and in cases of severe TBI, the recovery trajectory can be protracted over a period of months or years. 4 TBI typically affects young people (predominantly males age 18-35 years old) at the beginning of their working lives. 5 People with TBI have been reported to have worse general health, higher incidences of depression and social isolation, and reduced labor force participation rates compared with people without TBI. 6 Even a mild TBI can produce ongoing psychosocial problems. 7 Those who sustain moderate and severe TBIs may face the challenge of lifelong deficits requiring intensive rehabilitation efforts and ongoing supports to facilitate community reintegration. The majority of people with severe TBI require expensive long-term care due to loss of independence, reduced work capacity and relationship breakdown. 8
People with TBI continue to experience challenges with their cognition, behavior, social life, and emotions many years after their injury, which can negatively impact on psychosocial outcomes and quality of life. 9,10 Cognitive, behavioral and emotional difficulties are the most widely reported, persistent and detrimental consequences of TBI. 11 -13 Over the long term, injuries may compromise a range of high-level cognitive–linguistic functions 14 as a result of cognitive disruptions in the frontal lobe. 4,15,16 These communication deficits are defined as “cognitive communication disorders” 17 and can lead to difficulty having conversations with families, engaging in workplace interactions, reading complex information or writing for study or work. 18 Caregivers experience high levels of burden and depression, as caring for people with TBI can be stressful. 19 Significant sources for this stress have been identified as problems communicating with the person with TBI, 20 -22 behavioral disturbance, 23 and the level of cognitive processing difficulties of the person with TBI. Friends, caregivers, and family frequently begin avoiding the person with TBI, which impacts on their ability to maintain pre-injury relationships. 24 -26 It is therefore essential that people with TBI and their caregivers are able to access long term services. However, these are currently not readily available, especially for those in rural and remote locations. 4
Digital health
Digital health is a healthcare model that encompasses the use of various digital modalities such as health information technology, telehealth, eHealth, telemedicine, web-based modules, and wearable devices. 27 The terminology and definitions pertaining to digital health continue to evolve. 28 These various modalities of digital health can be applied in assessment, intervention, and information-sharing processes to facilitate timely, financially sustainable, personalized, and empowered treatment management. 27 The growth of digital health modalities has facilitated the development of intervention programs that allow people with TBI timely and cost-effective access to specialized services, allowing them to increasingly take control of and play a more active role in their health. 28 Digital health rehabilitation approaches facilitate interactions between the person with TBI, their caregiver, and the clinician in meaningful environments. 27 People with TBI have the opportunity to apply, internalize, and practice skills and tasks within their own home during therapy sessions and receive real-time feedback from their clinician. 29
Digital health also supports interdisciplinary practices, which is essential in the rehabilitation process for people with TBI, which then enables universal access to cost-effective and high-quality care, particularly in rural and remote regions. 30 The implementation of digital health modalities into services has shown to be effective in overcoming key challenges such as the need to travel (for people with TBI, their caregivers, and clinicians) improved cost efficiencies and processes, improved clinical outcomes, and education opportunities for clinicians. 31
Digital health interventions can be delivered synchronously or asynchronously. Synchronous interventions pertain to interventions delivered in real-time with the clinician present and providing immediate feedback and support. This can occur within the same location or context, for example in a clinic room or remotely, for example via videoconference or telephone. Asynchronous interventions do not require real-time consultation from a clinician or dedicated appointment times. These interventions are typically completed in the patient's own time and are often self-guided. Data collection can be patient or caregiver driven; however, many current technologies allow for automated data collection such as apps, computer programs or web-based interventions in which data is remotely shared with the clinician.
Whether an intervention is delivered synchronously or asynchronously can impact on the patient's engagement and efficacy of the intervention. This is illustrated in Ownsworth and colleagues' systematic review 32 of telehealth platforms for people with primary brain tumors and their caregivers, where findings indicated that for interventions delivered synchronously the uptake and adherence to intervention was higher, and clinical gains in response to intervention were more likely, compared with delivered online, self-guided interventions. The timing of delivery of intervention is an important factor to consider when evaluating the efficacy and effectiveness of digital health interventions.
Current applications of digital health
Recent literature investigating telerehabilitation for people with TBI, has produced mixed results. Ownsworth and colleagues' systematic review 33 concluded that structured telephone interventions led to improvements in global functioning, post-traumatic symptoms, sleep quality and depressive symptoms. However, while the feasibility of internet-based interventions was largely supported, the efficacy could not be determined due to insufficient studies that met the review criteria. Coleman and colleagues 34 also found limited results in their systematic review evaluating the assessment and treatment of cognition and communication skills in adults with acquired brain injury using telepractice. They reported insufficient data on diagnostic accuracy and treatment efficacy and the heterogeneity of assessments and interventions impacted on the efficacy and evaluation of possible clinical implications of telepractice application. Studies included in the review, predominantly delivered assessment and intervention services via videoconference or telephone and other digital modalities were not explored.
Similarly, Betts and colleagues 35 concluded that the current evidence base is limited for understanding the effect of telerehabilitation for cognitive and psychological interventions for people with TBI. Despite limitations such as lack of standardized intervention parameters, outcome measures and small sample size, they suggest that there is some evidence that telerehabilitation may be as equally effective as other forms of care; however, uncertainty remains as to whether telerehabilitation results in better outcomes compared with usual care. These findings are echoed in a systematic review conducted by Rietdijk and colleagues, 36 where it was concluded that telephone-based interventions for family members of people with TBI are feasible and yield positive outcomes for both the carer and the person with TBI. Although there is limited high quality evidence of the application of diverse digital health interventions in TBI cognitive communication rehabilitation, findings from the field of aphasia communication rehabilitation indicate that there is potential for similar, TBI-specific digital programs to have positive communication and quality of life outcomes for people with TBI and their caregivers.
While digital health is a fast-emerging model of care with a broad spectrum of digital health modalities available, there is limited evidence regarding the evaluation of digital health approaches for people with TBI and their caregivers. A systematic review is required to evaluate and synthesize current literature addressing the use of a range of digital health interventions in the rehabilitation of people with TBI and the education of caregivers of people with TBI.
Aims
The aim of this systematic review is to evaluate the current literature in relation to efficacy and effectiveness of digital health cognitive and behavioral interventions for people with traumatic brain injury (TBI) and their caregivers (close others and paid caregivers). This systematic review addresses the following questions: What are the characteristics of digital health interventions in TBI rehabilitation? What is the efficacy and effectiveness of digital health intervention or education programs for people with TBI in improving rehabilitation outcomes? What is the efficacy and effectiveness of digital health intervention or education programs for caregivers of people with TBI and/or the person with TBI?
Methods
A systematic search was conducted in May 2020 and repeated in February 2022 to identify studies that addressed the use of digital health intervention in rehabilitation and education for people with TBI and their caregivers. A systematic review protocol was registered for this study on PROSPERO (ID: CRD42020152218). The study method and reporting were guided by the Preferred Reporting Items of Systematic reviews and Meta-Analyses (PRISMA) Expanded Checklist 37 and relevant appraisal tools as outlined below.
Risk of bias in individual studies
Randomized control trials (RCTs) are considered a gold standard of evidence in evaluating the effectiveness of healthcare interventions. However, preliminary searches indicated very few RCTs in the scope of digital health interventions. As a result, this systematic review included: 1) all quantitative designs (including RCTs, case series, and case control studies); 2) qualitative designs; and 3) mixed-methods designs. The primary reviewer (PA) evaluated the quality of included articles using an appraisal tool matched to the appropriate study design (RCTs were rated using the PEDro-P 38 and PEDro+ 39 scales; single case experimental designs were rated using the Risk of Bias in N-of-1 Trials [RoBiN-T] scale). 40 Quality appraisal ratings were compared with existing ratings available on PsycBITE, where possible and the remainder of papers were rated by a second reviewer. Consensus was reached through discussion for any discrepancies between ratings.
Articles were assessed according to the National Health and Medical Research Council (NHMRC) levels of evidence (Table 1). 41
Levels of Evidence for Questions of Treatment Benefits
Based on National Health and Medical Research Council levels of evidence. 41
Inclusion and exclusion criteria
The inclusion criteria included articles that reported on all of the following: 1) digital health intervention (computer/online/web-based—i.e., any intervention delivered at a distance using technology, including telephone, websites, or videoconferencing); 2) intervention delivered to a person with TBI of any severity, and/or their caregivers (parents, partners, siblings, extended family or close friends who had taken on a caregiving role); 3) participants with TBI were adults (18 years and older); 4) in studies involving a mixed sample of conditions, at least 50% of the sample were people with a TBI and/or their caregivers; and 5) peer reviewed journal article. There were no inclusion criteria imposed on the outcomes of the intervention or on the study design.
Exclusion criteria included those publications which: 1) do not relate to TBI rehabilitation; 2) do not relate to a person with TBI and/or caregivers of a person with TBI; 3) less than 50% of participants were people with TBI or their caregivers; 4) not related to training/support for people with TBI or caregivers of a person with a TBI; 5) not delivered via digital health; 6) duplicates other results reported more fully elsewhere; 7) did not have at least an abstract available for review; 8) did not report data on outcome measures or process measures relating to the program; 9) addressed augmentative and assistive communication technology; 10) did not address cognitive or behavioral related interventions e.g., physical/gross motor therapy, upper limb intervention; and 11) only addressed assessment practices.
Search strategy
The search strategy was as follows: (traumatic brain injur* OR brain injur* OR acquired brain injur*) AND (digital health or telecommunication* OR teleconference* OR apps or ehealth OR e-health OR emedicine OR e-medicine or etherap* OR e-therap* OR (information and communication technolog*) OR multimedia messag* OR podcast* OR smartphone* OR smart phone* OR social media OR telecare OR tele-care OR telehealth OR tele-health OR telemedicine OR tele-medicine OR telerehabilitation OR tele-rehabilitation OR web-based OR web based) AND (intervention* OR treatment* OR therap* OR rehabilit*). The following search restrictions were applied: peer reviewed journal publication and population age 18 years and older. An example of the search strategy as applied in MEDLINE (Ovid, 1946-present) is shown in Table 2.
Search Strategy Example, Medline (OVID, 1946-present)
The following databases were searched using the search strategy: PsycINFO (Ovid), MEDLINE (Ovid), MEDLINE (PubMed), CINAHL (EBSCO), Embase (OVID), Cochrane Library (Wiley; including Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled trials), Scopus (via Elsevier), Web of Science Core Collection, speechBITE, and PsycBITE. MeSH and keyword search terms were adapted for the specific requirements of each database. Supplemental searching included gray literature and additional papers were sourced via hand searching the reference lists of included papers and any relevant systematic reviews. 33,42
During the hand searching process it was noted that intervention studies based on telephone interventions were not sourced using the initial search strategy. A secondary search using an adjusted search strategy was performed to capture these studies. The search strategy was as follows: (traumatic brain injur* OR brain injur* OR acquired brain injur*) AND (intervention* OR therap* OR treatment* OR rehabilitat*) AND (telephone).
Study selection
Search results from each database/source were downloaded into EndNote X8 and duplicates removed. Following this, the articles were exported to Covidence, a screening and data extraction tool. The title and abstract of each article were examined against review eligibility criteria in an initial round of screening. To increase reliability, a second reviewer screened 25% of the article titles and abstracts. A total of 336 titles and abstracts were screened by the second reviewer and 88.8% reliability was achieved (Cohen's k = 0.58, 95% confidence interval = 0.475-0.702 indicative of moderate to substantial agreement). 43 A second reviewer also screened 51 full text articles and 96% reliability was achieved (Cohen's k = 0.91, 95% confidence interval = 0.78 to 1 indicative of an almost perfect level of agreement). 43 Consensus was reached for any discrepancies in ratings through discussion. Once reliability was established, a second round of screening consisted of assessing full texts of potentially relevant articles against the same eligibility criteria.
Data extraction
Data was extracted from included articles using a template containing the following fields: 1) author, year of publication; 2) study design; 3) study population and characteristics; 4) context of intervention (including dose and type of digital health tool or resource); 5) methodology; 6) outcomes assessed; 7) findings; 8) theoretical model; and 9) intervention category (psychological, cognitive, communication, education).
Quality appraisal
The RCTs were appraised using the PEDro-P 38 and PEDro+ 39 scale. The PEDro+ 39 scale is an adaptation of the PEDro-P 38 scale as the original scale does not address treatment fidelity or treatment replicability. These elements are essential when evaluating the rigor of behavioral treatment research. These items were added to the original scale by Cherney and colleagues 39 in their review of communication partner training in aphasia, to create a 12-item scale. The RoBiN-T scale 40 was used to assess methodological quality for single case experimental design studies. Ratings were used from the SpeechBITE and PsycBITE websites where available. Where no rating was available, two independent raters evaluated the papers, and any disagreements between the two ratings were resolved through discussion and 100% consensus was achieved.
Statistical analysis
Descriptive results are presented in a table format. This includes details regarding: methodology, participants, interventions, outcome measures, follow-up interventions, statistical significance, effect sizes and results. A mixed-methods synthesis included both quantitative and qualitative data analysis as per the following:
Quantitative analysis: The content of the included articles determined the nature of the comparison. Given the broad nature of the research question (i.e., interventions addressed by the included studies may vary across different digital health approaches, such as app, web-based, telephone, etc.), findings are reported in a narrative summary. Limitations within the evidence base are discussed and the possible influences of publication/small study biases are considered and presented.
Qualitative analysis: A thematic synthesis was conducted to facilitate further investigation regarding types and modes of interventions
Mixed-methods synthesis (quantitative and qualitative): Findings from the narrative synthesis and thematic synthesis were collated into a summary in response to the research questions. As per the PRISMA protocol, 37 the findings are presented, discussed and then conclusions drawn based on this evaluation. Additionally, implications for clinical practice and research and limitations are subsequently outlined.
Results
Study selection
Figure 1 depicts the search results and the process of exclusion of articles. A total of 2004 sources were identified from the initial search strategy in May 2020. A further 13 sources were identified using the additional search strategy and handsearching. Following removal of duplicates and application of exclusion criteria, there were a total of 40 articles that met the inclusion criteria for review. The search strategy was repeated in the February 2022 and an additional four articles met the inclusion criteria. Figure 1 was updated accordingly to give a total of 44 articles.
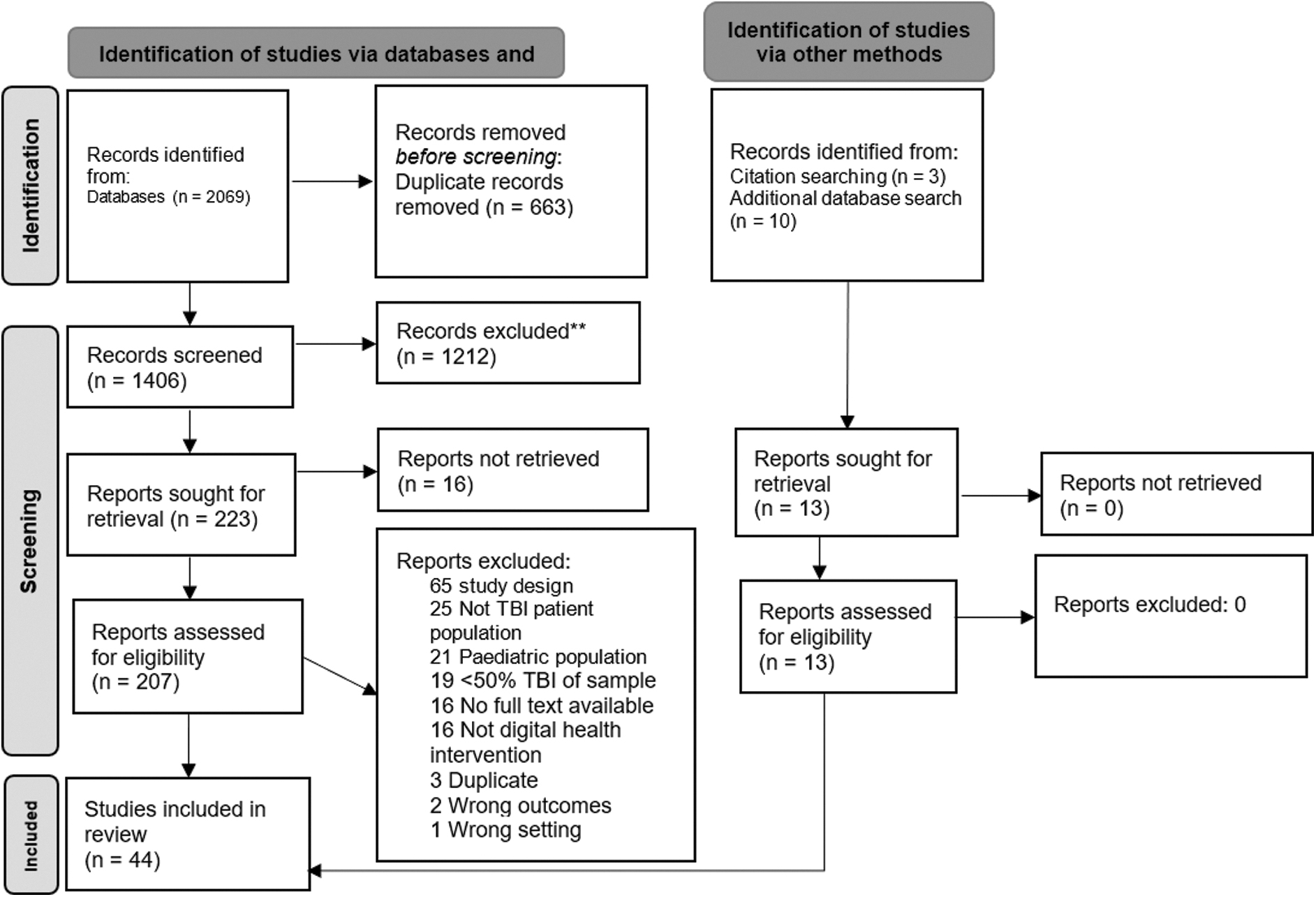
Study selection flow-chart.
Study design and quality appraisal
The search identified 22 RCTs (Level II), three single case experimental design studies (Level III-I; reported in Table 3), 44 –88 six non-randomized controlled trials (non-RCTS; Level III-2), nine case series studies (Level IV), and four case studies (Level IV). All studies were published in the last 25 years. Figure 2 shows the distribution of studies at each level according to the study population.
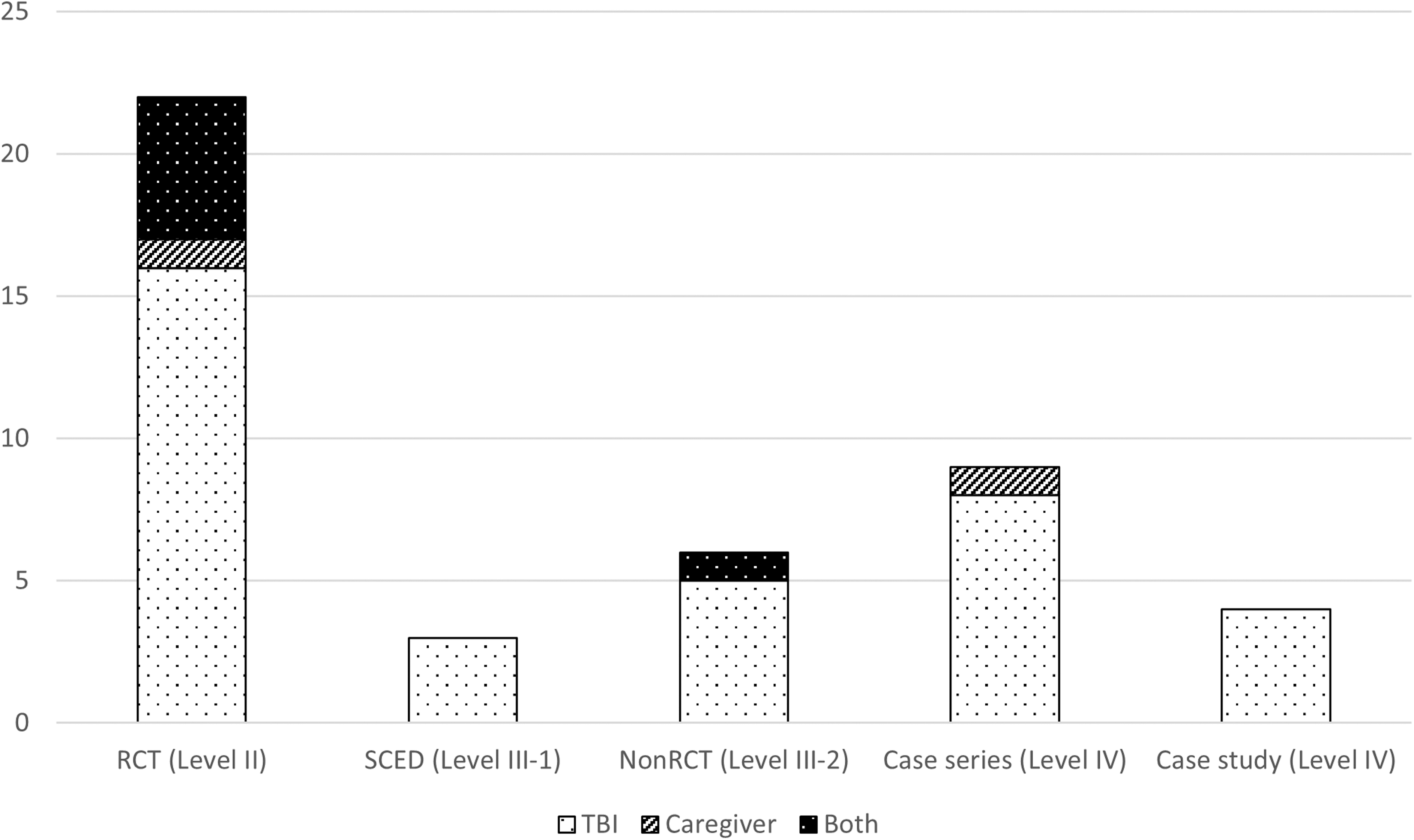
Distribution of studies across National Health and Medical Research Council levels.
Description of Intervention Characteristics
The quality appraisal and distribution of results for each of the studies is shown in Figure 3. Results of quality reviews of the communication partner training studies include both a PEDro-P rating and a PEDro+. The mean PEDro-P rating for the RCTs was 5.6/10.0 (range 3/10 to 7/10) and the mean PEDro+ rating was 6.3/12.0 (range 4/12 to 9/12).
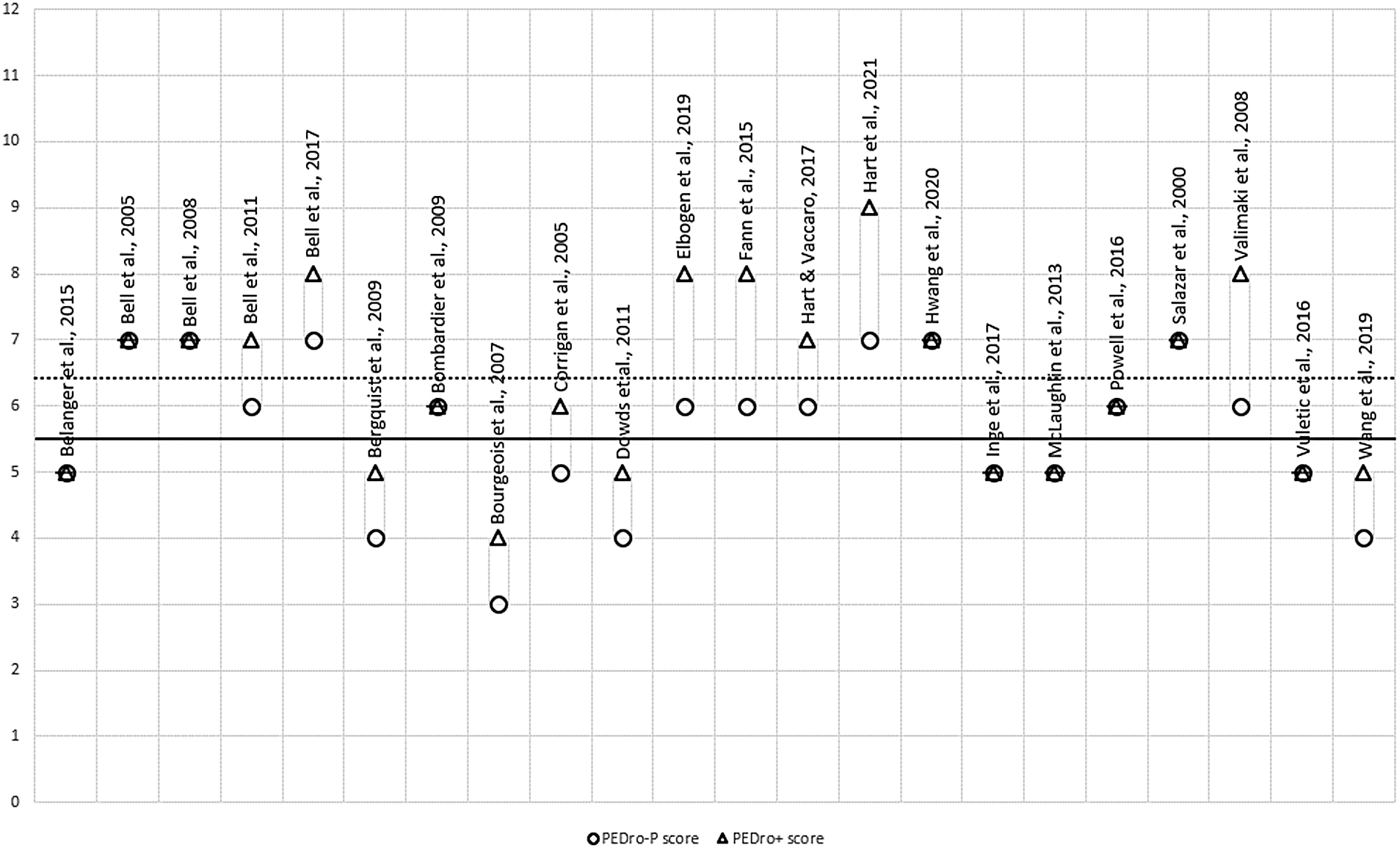
Quality appraisal scores on the PEDro-P and PEDro+ for randomised controlled trial studies. The circles represent the PEDro-P scores, which are scored out of 10. The solid line indicates the mean PEDro-P score. The triangles represent the PEDro+ scores, which are scored out 12. The dotted line indicates the mean PEDro+ score.
The mean ROBiN-T rating for internal validity was 4/14 (range 3/14 to 5/14), the mean external validity rating was 7.3/16.0 (range 4/16 to 10/16) and the total mean rating was 11.3/30.0 (range 7/30 to 14/30). The results for each study are shown in Figure 4.
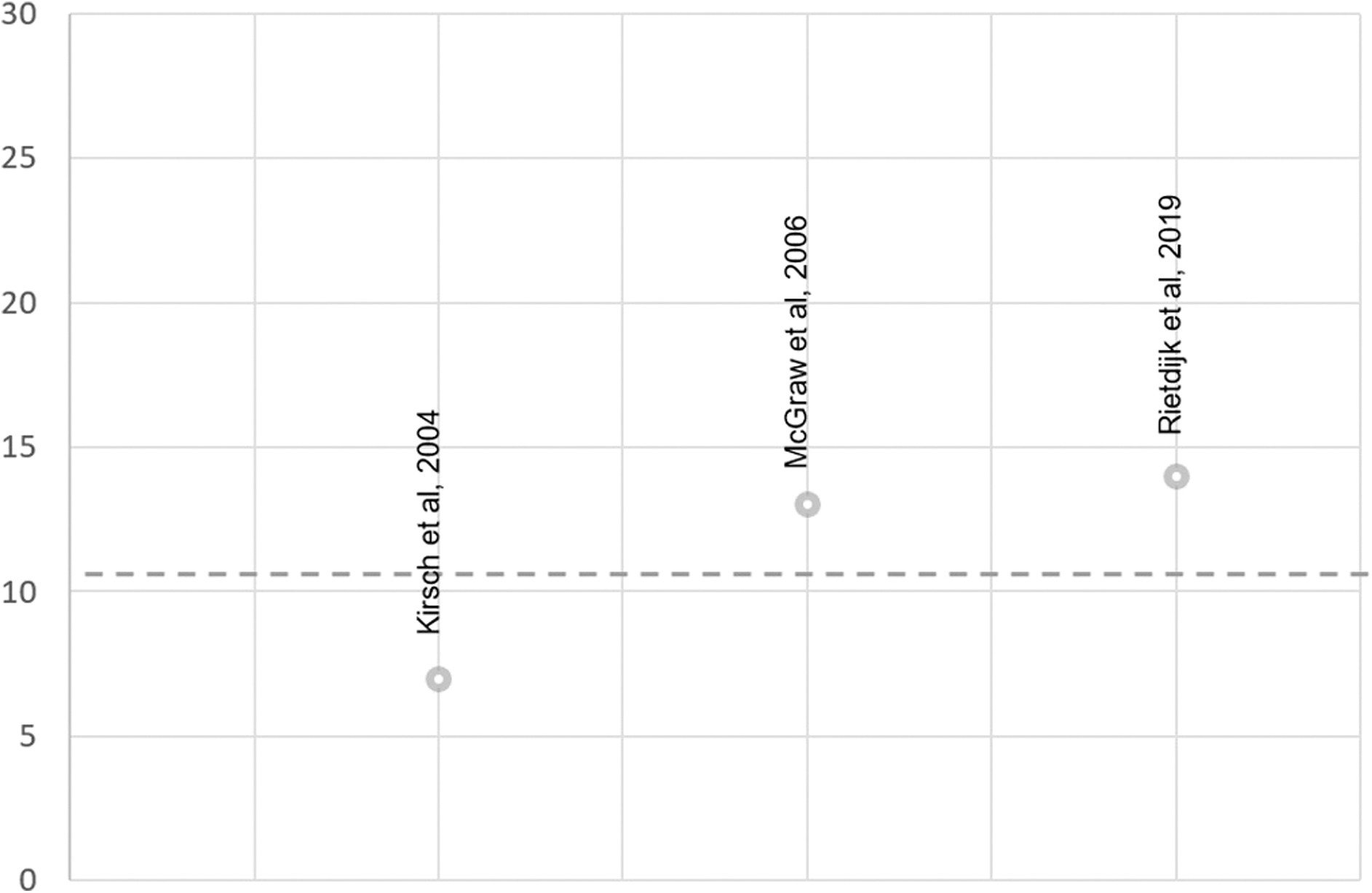
Scores on the Risk of Bias in N-of-1 Trials (RoBiNT) scale for single case experimental design studies. Dotted line indicates the mean ROBiNT score.
Further detail on the quality appraisal and scores for each criterion can be found in Supplementary Table 1 for PEDro-P and PEDro+, and Supplementary Table 2 for ROBiN-T ratings.
Study characteristics
Participants
People with TBI
The description of participants is presented in Table 4. Of the 44 studies in this review, 35 studies included people with TBI resulting in a total of 3823 participants with TBI. For 11 studies, the participants had a range of conditions with at least 50% of the sample including participants with TBI and 27 studies including participants with TBI only. The number of participants in the studies ranged from 169 to 746 participants. 82 There was considerable heterogeneity in sample characteristics. For studies reporting age (n = 42), the age ranged from 18 to 90 years. In those reporting severity (n = 26), 14 studies included participants with moderate to severe TBI, five studies included participants with mild TBI, four studies included participants with a range of mild to severe TBI, two studies included participants with severe TBI only and one study included a participant with moderate TBI. The remainder of the studies did not specify severity.
Description of Participants
TBI, traumatic brain injury; Rx, treatment; Ctrl, control; pwTBI, person/s with traumatic brain injury; CCT, computerized cognitive training; TC, tai chi; UC, usual care; MOPS-VI, Military On-Line Problem Solving Intervention; PTSD, post-traumatic stress disorder; ITA, intelligent therapy assistant; PST, problem solving treatment.
Caregivers
Across the 44 studies, two studies included only caregivers of people with TBI (n = 213) as their participants and seven studies included both people with TBI and caregivers (combined total of n = 908). Studies included a heterogeneous sample of caregivers, including parents, siblings, partners, and friends of people with TBI. For the one study 72 that reported the age range of participants that were specifically caregivers, ages ranged from 18 to 61 years.
Interventions
The intervention characteristics are presented in Table 3.
Asynchronous or synchronous
Of the 44 studies, 20 studies evaluated interventions that were delivered asynchronously and 13 studies examined interventions that were delivered synchronously. There were 11 studies that included both an asynchronous and synchronous component to the intervention. Figure 5 depicts the delineation of synchronous and asynchronous approaches within each modality. Interventions delivered by telephone and videoconferencing were exclusively synchronous; however, intervention modalities such as mobile use, computer programs and social media demonstrated a combination of synchronous and asynchronous approaches across the studies. The use of personal digital assistants (PDA) was exclusively asynchronous.
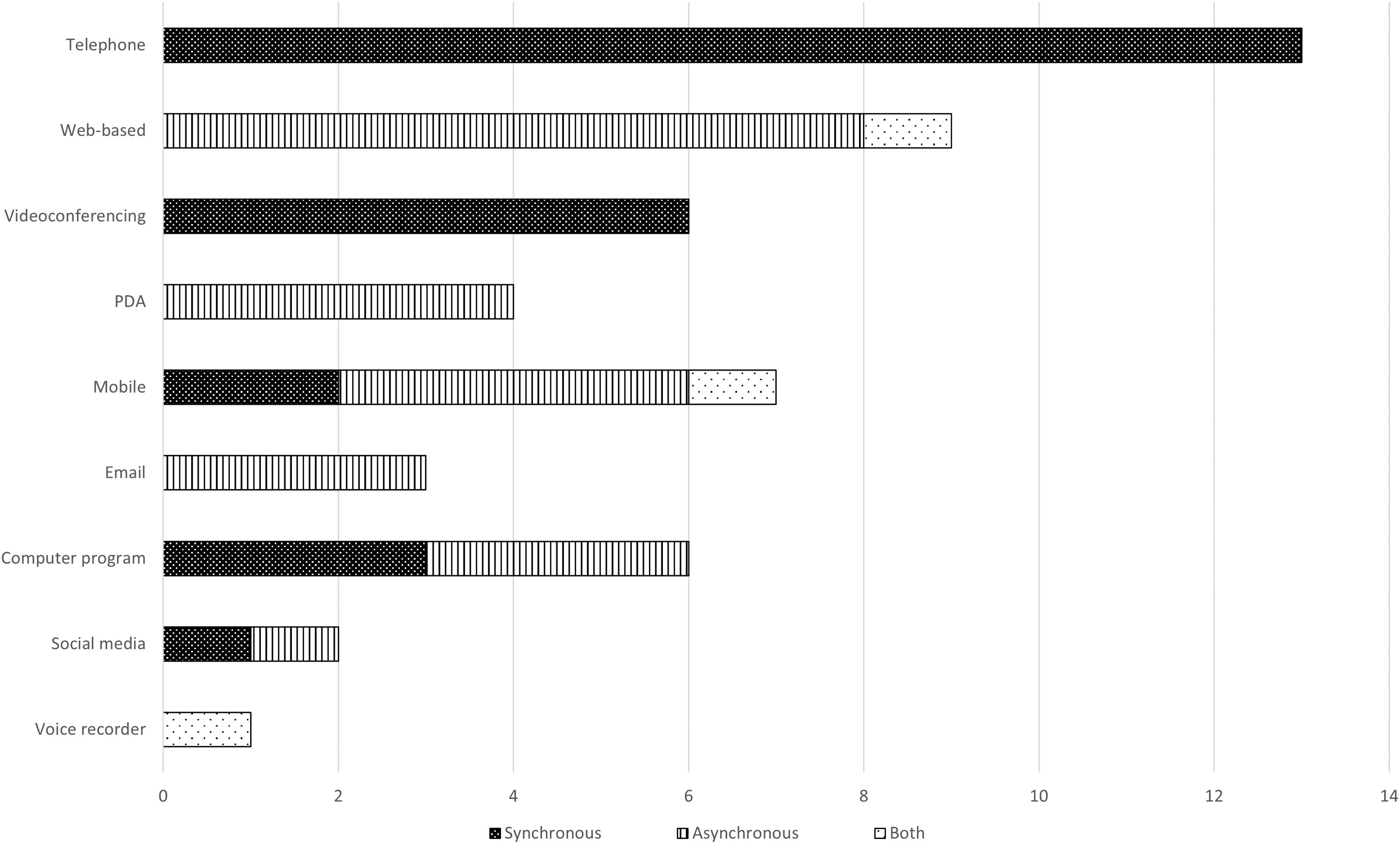
Modalities of intervention.
Modality
From the 44 studies included in this review, there was a range of nine different digital health modalities (Fig. 5). The most frequently used modalities include telephone (n = 12), web-based (n = 8) and videoconferencing (n = 6). Four studies used a combination of two digital health modalities, with one of these studies 82 using a PDA during the main intervention period and then text messaging during the follow-up period. Five studies compared two digital health interventions, including Inge and colleagues 68 who delivered an intervention using social media (Facebook) and email. Figure 6 demonstrates the distribution of modality types across the years of publication.
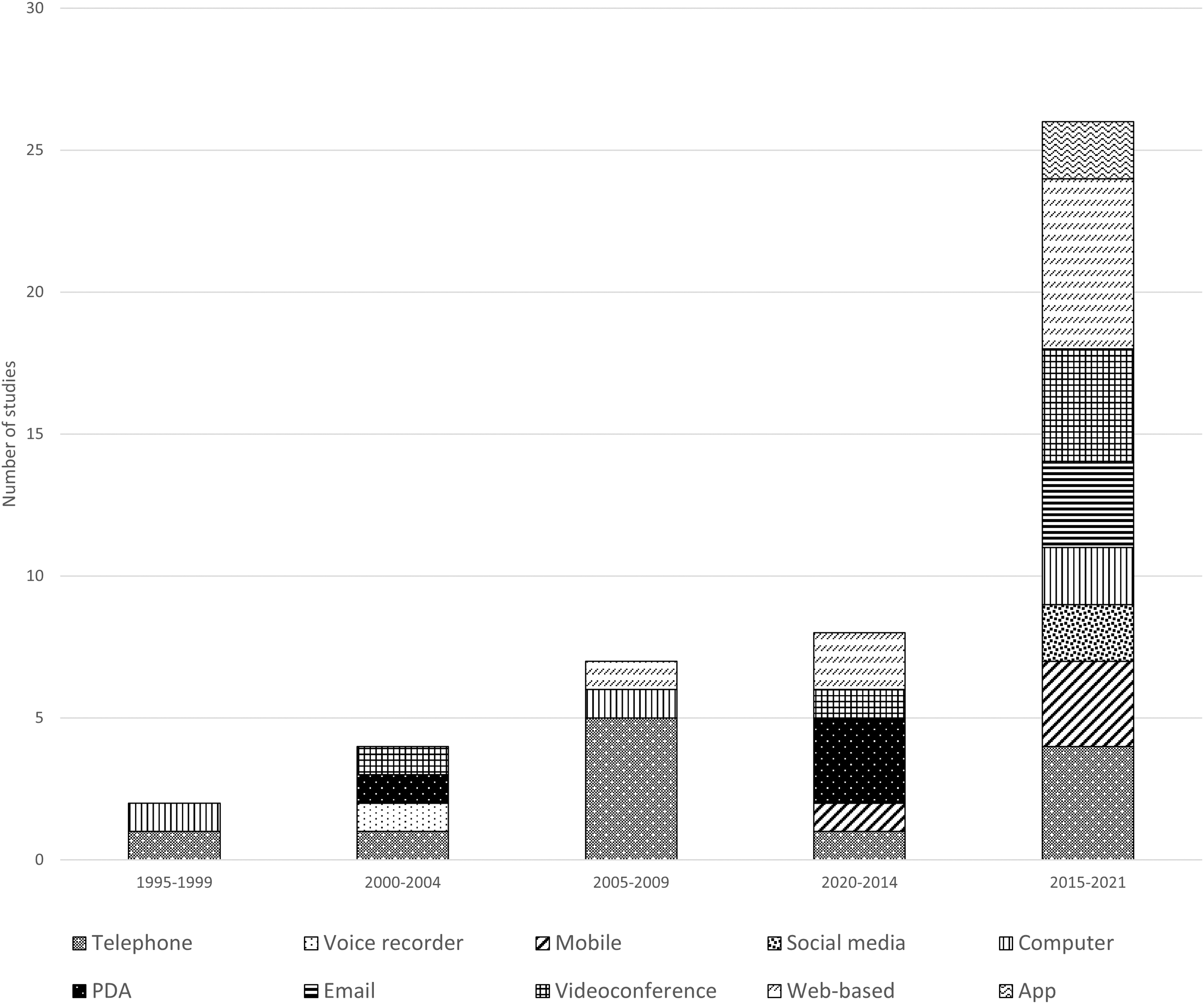
Distribution of modalities across the years of publication.
Provision of intervention
Interventions were delivered by a variety of health professionals. Five of the studies included interventions that were delivered by counselors, five by speech pathologists and three by occupational therapists. Other health professionals included: neuropsychologists (n = 2), psychologists (n = 2), nurses (n = 3), social worker (n = 1), case manager (n = 1) and vocational rehabilitation counselor. Nine studies did not specify the discipline of the therapist. Four studies implemented a multi-disciplinary approach with interventions being delivered by: 1) a psychologist, sociologist, and anthropologist 48 ; 2) a psychologist, neuropsychologist, and social worker 54 ; 3) an occupational therapist and a speech pathologist 69 ; and 4) a speech pathologist, an occupational therapist, and a vocational counselor. 75 Three studies 45,59,67 included interventions that were self-directed by the participants and four studies 60,63,65 included interventions that were a combination of self-directed and therapist-led components.
Individual or group
Of the 44 studies included in this review, 38 studies involved interventions delivered to individual participants. Three studies 54-55 were delivered in a group model and three studies 75,78,82 included a combination of both individual and group service delivery models.
Location
The interventions were predominantly delivered remotely (n = 27), with this including participant homes, workplaces, or other sites within the community. Four interventions were delivered synchronously using a digital modality (e.g., a computer-based program) with the clinician in person and five studies did not specify the location of service delivery. There were seven studies that were delivered involving a combination of both on-site sessions with the clinician and remote sessions (for example in the participants' homes). On-site locations included rehabilitation units, laboratories, and clinics. There was one intervention that required the participants to engage in the intervention asynchronously (self-directed content) both on-site and remotely.
Dosage
Number of sessions ranged from one session to 60 sessions, with interventions most frequently ranging in duration between six and ten sessions. Length of interventions ranged from a single session (n = 1) to 2 years (n = 1). For the interventions that were over 6 months in duration, these programs included multiple follow-up or maintenance sessions that were up to 3 months apart. The interventions were delivered mostly over 8-12 weeks. Sessions were predominantly scheduled fortnightly (n = 5), weekly (n = 5) or used a tapered approach to include follow-up and maintenance sessions (n = 4). Session duration ranged from an 8-min phone call 48 to sessions that were up to 3 h in length, 70 with 60-min sessions being the most common (n = 7) followed by 30-45 min sessions (n = 6). Total hours of intervention ranged from 40 min to 60 h. From the studies that reported the total number of sessions and the duration of each session, the mean dosage (number of sessions × duration of session) was 17.5 h.
Aims of intervention
The primary purpose of the interventions included in this review was to address cognitive rehabilitation (n = 16), with other studies focusing on education and improving knowledge about brain injury (n = 4), improving problem solving skills (n = 4), symptom management (n = 3), improving task completion and efficiency (n = 4), goal setting skills (n = 3), acquisition of new functional skills (n = 2), social communication (n = 2), improving management of mental well-being (n = 3) and compensatory strategies (n = 3). Two studies addressed cognitive-communication skills.
Theoretical models
Nine studies clearly stated the underpinning theoretical model of the included interventions. This included; cognitive behavioral theory (n = 4), Spacing Effect theory (n = 1), neuroplasticity (n = 1), Supervisory Attentional System (n = 1), mindset theory of action phases (n = 1) and Theory of Reasoned Action (n = 1).
Co-designed interventions
Five interventions 52,66,68,72,75 involved elements of co-design. However, these studies only partially applied the co-design process to the development of intervention programs and excluded a diverse range of key stakeholders. Elements that were considered included seeking advice or consultation from clinicians, 52 clinician-based focus groups 66 and feedback from people with TBI via interviews or focus groups. 68,75 McLaughlin and colleagues 72 incorporated a combination of different elements, such as: 1) evidence-based interventions for caregivers of people with TBI; 2) interviews with family members of people with TBI and experienced professionals; and 3) adaptation of a text-based program. 89
Outcomes
A summary of key findings and outcomes is presented in Table 5.
Summary of Key Findings and Outcomes
TBI, traumatic brain injury; FIM, Functional Independence Measure; DRS, Disability Rating Scale; CIQ, Communication Integration Questionnaire; FSE, Functional Status Examination; GOS-E, Glasgow Outcome Scale (Extended); NFI, Neurobehavioral Functioning Inventory; PQOL, Perceived Quality of Life Scale; SF-36, Short Form-36; BSI, Brief Symptom Inventory; PST, problem solving treatment; mTBI, mild traumatic brain injury; RCT, randomized controlled trial.
Telephone interventions
Five 47 -49,51,86 of the 10 studies investigating the effectiveness of telephone-based intervention for people with TBI reported outcomes that were better than usual care intervention, such as face-to-face interventions, for all of the aforementioned intervention aims. Regarding long-term outcomes, there was no significant difference at 12 months follow-up for most studies, although Nakase-Richardson and colleagues 86 reported better overall sleep quality for their telephone problem-solving treatment group compared with the education-only group at 6 months post-treatment. The other five studies 46,53,56,61,81 reported improved outcomes for both the usual care intervention groups and the telephone interventions groups; however, there were no statistically significant differences in long term outcomes.
Two studies 54,75 investigated the effectiveness of telephone-based interventions for caregivers of people with TBI. Brown and colleagues 54 reported that education, skill development and counseling for rural families of a person with TBI delivered via telephone resulted in less burden and less distress in their role as caregivers than the usual care group. Powell and colleagues 75 found that intervention targeting quality of life and emotional well-being of caregivers, resulted in improvements for both the telephone intervention group and the usual care group and there was no statistically significant difference between the groups.
Computer and web-based interventions
Ten studies 45,50,55,59,67,70,80,82 -84 investigated the use of computer and web-based interventions for people with TBI. One study 45 reported better outcomes in reducing post-concussion symptoms for people with TBI completing intervention via computer and web-based modalities compared with those receiving in person intervention. Another study 67 reported better outcomes post-intervention for participants that completed computerized cognitive treatment compared with participants that were in the Tai Chi group and usual care group. However, these cognitive improvements were not maintained at follow-up. Two studies 80,82 reported improvements for both the web-based intervention group and the in-person intervention group; however, no statistical differences were found. Four studies 55,59,70,83 did not include a usual care condition; however, they found that participants showed improvements in cognitive and neuropsychological skills compared with baseline measures. One study 84 investigated the effectiveness of three different web-based video games in improving cognitive functioning and well-being for people with TBI in comparison to usual care. There were no significant differences between all three gaming groups in improvement on the outcome measures with all groups showing improvements in test performance across three time points. Additionally, Bergquist and colleagues 50 used internet based instant messaging to investigate the effectiveness between an active condition (use of a calendar) and a control condition (use of a diary). They found that there were no significant differences between conditions for changes in functioning on any of the primary or secondary outcome measures.
One study 72 investigated the use of a web-based program in targeting active listening and problem-solving skills in families of people with TBI and identifying relevant support services and strategies for stress reduction. There were greater improvements in skill application, intention, and knowledge related to the targeted areas at post-test for the web-based intervention group compared with the control group, which received usual care. However, at 3 months follow-up, there was no difference between the intervention group and the control group regarding knowledge acquired and satisfaction with life.
Videoconferencing interventions
Two studies 62,73 investigated the effectiveness of using videoconferencing in the provision of intervention for people with TBI without a comparison to usual care. Ng and colleagues 73 found that intervention delivered via videoconferencing resulted in positive changes for the participants with self-reported improvements in both trained and untrained goals. There was also a trend toward fewer symptoms of executive dysfunction and greater community integration. Forducey and colleagues 62 found in a single case study that neuro-developmental treatment delivered via videoconferencing resulted in minimal improvement in physical skills; however, the patient showed qualitative improvement in his alertness and basic neurocognitive skills.
Two studies investigated the effectiveness of delivering intervention via videoconferencing for people with TBI and their caregivers. Rietdijk and colleagues 77 found that the use of videoconferencing in targeting social communication skills, showed positive change on blinded ratings of conversation and self-reported measures of conversational skills for two participants with TBI using single case experimental design. In a separate non-randomized controlled trial, Rietdijk and colleagues 78 found that participants and their caregivers who received this videoconferencing-based intervention had similar outcomes in participation in conversations compared with an in-person intervention group on most outcomes, although two secondary outcomes showed medium to large effect sizes favoring the in-person group. Studies that used videoconferencing as the intervention modality focused on participants within the moderate-severe or severe TBI population.
PDA interventions
Four studies 58,69,81,86 investigated the inclusion of a PDA in intervention programs for people with TBI. Dowds and colleagues 58 found that the use of a PDA as memory aid resulted in significantly higher task completion rates for participants in the intervention group compared with the usual care, paper memory aid group. The other three studies did not compare the outcomes of intervention to usual care; however, they did find improved outcomes for people with TBI compared with their baseline scores prior to intervention. Kirsch and colleagues 69 found that the use of a PDA to provide verbal cues for reducing utterance length resulted in no change in utterance frequency; however, total utterance time (and therefore, length) was reduced. Further, Smith and colleagues 82 demonstrated that participants showed increased participation in intervention and improvements in attitudes, behaviors, and experiences in real time in their natural environments when messages were provided via PDA. Waldron and colleagues 87 also found that using a PDA to improve compensatory skills for memory problems resulted in a higher number of tasks completed and remembered during the 2 weeks of intervention.
Mobile and smart phone interventions
Six studies 52,60,63 -65,88 included mobile and smart phones as a modality to deliver intervention. This included the use of text messaging, 64,65 apps 52,60,88 and adaptive manuals 63 on these devices. Elbogen and colleagues 60 investigated the use of an app and reported no significant change between the intervention group and the usual care group in cognitive or impulsiveness outcome measures. However, the intervention group showed a larger decrease in anger towards others and engaged in fewer maladaptive behaviors at 6 months follow-up. Two studies 52,63 did not involve a comparison to usual care; however, they did report improved outcomes for the participants compared with their baseline performance.
Hart and Vaccaro 65 compared two text messaging interventions, comparing the effectiveness between a goal intention-reminding intervention approach and a goal review intervention approach. Both groups showed improvements, with the goal intention group reporting greater participation in the community. Hart and colleagues 64 also compared two text messaging interventions, comparing the effectiveness between an intentional implementation approach and a motivational intervention approach resulting in better outcomes for the intentional implementation group. Wang and colleagues 88 investigated the effectiveness of an app-based intervention targeting completion of kitchen related sequencing tasks. Their findings showed improved performance for the group using the app compared with the usual care group. There was a statistically significant change in reducing the number of steps where participants needed external assistance.
Social media interventions
One study 68 compared the use of email and social media (Facebook) for knowledge translation in people with TBI by increasing their knowledge of employment-based practices. Both groups (email and Facebook) were reported to have gained knowledge in this area; however, there was no significant difference between groups, and no comparison to usual care. Another study 44 included the use of social media as part of a multi-method approach in improving memory activation in a single case, along with cognitive remediation and neurologic music therapy. The participant showed significant improvements on the neurocognitive outcomes as a result of this multi-method approach.
Recording device interventions
Two studies investigated the inclusion of recording devices as part of their rehabilitation approach for people with TBI. Hart and colleagues 66 found that the use of a voice recorder to recall therapy goals and plans showed that recorded goals were recalled better than unrecorded goals and appeared to be associated with better awareness or follow-through with therapy objectives. McGraw-Hunter and colleagues 71 found that teaching a cooking skill via video-feedback using a digital camera resulted in increased independent completion of the task compared with baseline performance, as well as generalization of skills to a novel food item for those that maintained their skills at 2- and 4-weeks post-training.
Combination of digital health modalities
Two studies 57,76 incorporated a combination of modalities in their intervention approaches. Damianakis and colleagues 57 found that intervention and support for caregivers delivered via website and videoconferencing resulted in improvements in cohesiveness, mutual identification, empathic support, and problem-solving strategies; however, there was no comparison with usual care. Similarly, Riegler and collealgues 76 delivered intervention via videoconferencing and asynchronous online modules when targeting cognitive functioning. This resulted in increased treatment adherence for people with TBI who would otherwise disengage with the service, compared with usual care. Memory improvements were observed for both the telehealth group and the usual care group, with no significant difference between the groups.
Discussion
This systematic review aimed to investigate the characteristics of current digital health interventions and the effectiveness and efficacy of these interventions. This paper showcases the large variety of digital health interventions used in the rehabilitation of people with TBI and to provide support and education for their caregivers. Overall, the findings supported the effectiveness of digital health interventions. In those studies which compared digital health with usual care, there was evidence that digital health interventions may be as effective, and in some cases potentially more effective, than usual care. This indicates that the application of this fast-emerging model of care in TBI rehabilitation is feasible and has potential to increase accessibility to specialist services for people with TBI and their caregivers throughout their life trajectory.
Characteristics of digital health interventions in TBI rehabilitation
This paper reported on interventions across seven categories of digital health modality: telephone, computer- and web-based, videoconferencing, personal digital assistants, social media, recording devices, and mobile and smart phones. Only two studies 57,76 incorporated the use of more than one digital modality in their intervention approach. Two studies 48, 49 included a combination of a traditional intervention modality (e.g., written resources) with a digital health intervention modality (e.g., telephone). Additionally, 10 studies used a combination of asynchronous and synchronous service delivery methods. However, despite using a combination of service delivery modes, these studies often used one digital health modality in combination with traditional face-to-face intervention. These results indicate that the effectiveness of using multiple digital health modalities has not yet been thoroughly explored and researched. Studies such as that of Riegler and colleagues 76 indicate that the use of multiple digital modalities (videoconferencing and online modules) compared with usual care can result in positive patient outcomes. This is also consistent with the findings of Damianakis and colleagues 57 where caregivers reported ease of access to services and improved outcomes in caregiver stress, self-efficacy, and coping capacity.
Advancements in technology have also facilitated improved efficiency and effectiveness for clinicians in providing interventions via digital health rather than traditional face-to-face approaches. Digital health modalities such as apps and computer and web-based interventions enable improved data collection efficiency and accuracy. Data collection is often completed by the digital program and reported to the clinician for further analysis and decision making. This improves clinical planning and accuracy for further intervention task and goal selection. However, automated data collection and decision making was integrated infrequently in the studies included in this review, with only one study, Solana and colleagues, 83 including algorithm technology to support clinical decision making and task selection. This enabled further tailored and individualized intervention approaches. Computerized clinical decision support is currently being explored in pharmacy and medicine, 90 with findings that electronic prescribing systems have good potential to improve medication safety. These modalities often have features that allow the clinician to document how often material is accessed. This encourages those completing the intervention to be more accountable in completing asynchronous tasks. It also facilitates the clinician to review and evaluate patterns or other ways to support the person with TBI and their caregiver in engaging with their therapy, such as the inclusion of reminders or follow-up calls or emails.
Multiple studies in this review reported improved engagement due to reduced need for travel, and ease of follow-up processes (for example, participants responding to telephone calls from clinicians). For studies that evaluated satisfaction with care, participants reported this to be high on most surveys. Most studies acknowledged that there is potential for technical issues to affect engagement and delivery of intervention. This was addressed by ensuring that participants were trained and educated in the relevant digital health modality prior to commencing intervention as well as including an investigator or clinician who was available to assist with technical issues.
Foundational work to evaluate and identify the active ingredients of interventions is vital in the development of digital health interventions in TBI, to ensure that strategies are efficacious and facilitate therapeutic improvement. The active ingredients that comprise the intervention and facilitate therapeutic improvement were rarely outlined in the included studies. Studies did report whether participants received feedback during their intervention; however, there was limited data on the frequency or type of feedback. This has substantial potential to impact fidelity, which is supported in the PEDRO+ ratings, where fidelity was rarely described in the randomized control trial studies. Additionally, studies often reported on the intervention approach; however, the theoretical underpinnings were not clearly reported or discussed in the paper. This emphasizes the importance of reporting theoretical foundations of intervention approaches as we move across modalities and embrace digital health in our practice. A clear understanding of active ingredients also further ensures that these elements are maintained and carried across into new digital modalities to confirm that therapeutic benefits are maintained. It is recommended that future intervention studies incorporate the Rehabilitation Treatment Specification System (RTSS) framework 91 or the Template for Intervention Description and Replication (TIDieR) checklist and guide. 92 An example of work in this field was undertaken by O'Rourke and colleagues, 93 who identified the common and distinct active elements of communication partner training interventions within the stroke, TBI, and dementia populations.
An interesting finding when investigating the intervention characteristics was that only five interventions 52,64,68,72,75 in this paper involved elements of co-design. However, these studies only partially applied the co-design process to the development of intervention programs and excluded a diverse range of key stakeholders. There is growing evidence of the application of co-design in interventions to ensure that the needs of all stakeholders are met. 94,95 Ownsworth and colleagues 96 emphasized the importance of investigating the perceived usability and acceptability of videoconferencing for delivering rehabilitation to people with acquired brain injury (ABI) from the perspective of people with ABI, their caregivers, and service coordinators. Ownsworth and colleagues, 96 were able to identify the facilitators and barriers to videoconferencing uptake from the perspective of each user group. For example, service coordinators identified that there is a growing demand for specialist brain injury rehabilitation services, especially in rural and remote communities, pointing to a service gap that videoconferencing has the potential to address. Additionally, caregivers and people with ABI were able to identify potential barriers such as cognitive-linguistic and behavioral impairments, access to internet and technology and lack of technical support. An understanding of the factors that influence uptake of technology in healthcare is essential to facilitating user experience and supporting healthcare providers in successful implementation of digital health in their practice.
Interventions can also be further enhanced by a wider range of available ideas, a better understanding of user needs, and reduction in development costs and time. Users may also benefit by receiving a more satisfactory intervention or higher quality of service and develop an understanding of future interventions through participation in the co-design process. Mulvale and colleagues 97 propose that co-design facilitators focus on the primary principles of co-design such as achieving meaningful engagement and management of power differentials when working with vulnerable and disadvantaged populations, rather than focusing on following a set of steps. This participatory approach is significantly more empowering for the consumer. The co-design process in the development of interventions is increasingly used across healthcare, including acute, rehabilitation, and outpatient or community contexts. 98 -100
Efficacy and effectiveness of digital health intervention or education programs for people with traumatic brain injury compared with face-to-face intervention approaches
The findings of this systematic review paralleled the findings from previous systematic reviews investigating telerehabilitation in TBI, 34 -36 where interventions were primarily delivered via telephone. Interestingly, there has been an uptake in videoconference and web-based interventions in the last 5 years. This may be in response to the increased availability and accessibility of this technology for personal and vocational use.
Although there were predominantly no statistically significant differences in outcome measurement between usual care groups and intervention groups post-intervention and at follow-up, there were a few studies that reported improved maintenance of skill acquisition and/or knowledge for people with TBI during the follow-up phase. 45,53,56,60,61 There was no significant difference between intervention and control immediately post-intervention; however, the intervention groups improved over the follow-up phase. Intervention modalities included web-based, mobile application, and telephone. With the exception of Belanger and colleagues, 45 these interventions were delivered synchronously. Elbogen and colleagues 60 also included an asynchronous component consisting of daily self-directed tasks that the person with TBI completed. Telephone and computer-based programs may be considered as a “staple” of digital health intervention modalities as they have been consistently implemented as part of rehabilitation over the last 20 years. However, this has changed to include new advances in technology, which have increased in demand due to COVID-19.
Over the last 5 years, intervention programs for people with TBI have predominantly been delivered via videoconference and web-based platforms. This is reflective of the improvements in accessibility, development, and technological literacy. These modalities in particular have shown some evidence that digital health interventions produce similar outcomes to face-to-face interventions. It is recommended that future interventions and studies continue to reflect and harness the evolving nature of technology. Additionally, videoconferencing appears to be the modality of choice when working with people with moderate-to-severe TBI. The opportunity for synchronous clinician input may influence the choice for this modality, as it may be more appropriate than self-guided digital health technologies for people with more severe injuries. From the studies that only included participants with severe TBI, videoconferencing was the only modality used in the intervention programs. It is imperative to consider the severity of brain injury when selecting digital health interventions and to also consider additional supports or adaptability required for this population to be able to effectively engage with their rehabilitation. As technology evolves, new technologies relevant to people with severe injuries can be expected, such as smart technologies and artificial intelligence technologies. For example, Project Euphonia 101 is an initiative by the Google AI for Social Good program aiming to improve the sensitivity of automated speech recognition (ASR) technologies through collecting speech samples from people with impaired speech patterns such as dysarthria and apraxia. Ensuring accessibility to everyday technology for people with TBI is essential and needs to be acknowledged as a rehabilitation priority.
Efficacy and effectiveness of digital health interventions or education programs for caregivers of people with TBI and/or the person with TBI
Interventions and education programs for caregivers of people with TBI were delivered using three primary modalities: telephone, web-based tools, and videoconferencing. However, web-based interventions and programs delivered by videoconferencing platforms, have been more prevalent in the last 5 years. As technology evolves and accessibility and availability increases, it is vital that interventions and programs continue to advance with it.
There is limited research in caregiver specific interventions. Only two studies 57,72 investigated intervention and support programs that were designed specifically for the caregiver. Both programs demonstrated positive outcomes following the intervention, although neither demonstrated maintenance of these outcomes. The development of digital health interventions that address and support the long-term needs of carers of people with TBI is a priority for future development. There is also a lack of research in communication specific interventions for people with TBI and their caregivers. TBIConneCT 77,78 was the only conversation skills-based program in this review, with other interventions focusing on education and problem-solving treatment of post-concussive symptoms and/or emotional management. Social communication challenges are prominent at 1 year post-injury, 102 and these deficits can continue into the long-term resulting in relationship difficulties at 10 years post-injury. 103 This indicates a need to provide continuing services and supports to caregivers of people with TBI as rehabilitation needs and environments change, in particular, addressing communication needs across work, leisure and relationships during different life stages. Research should focus on examining resourceful methods of sustaining contact with caregivers, such as the consideration of a combination of digital health modalities as well as a combination of asynchronous and synchronous engagement.
Limitations
There are several limitations associated with this systematic review. Firstly, half of the included papers were a Level III or Level IV study as rated using the NHMRC levels of evidence. 41 While these studies indicated positive outcomes, it is essential that future research incorporate rigorous high-level studies comparing digital health interventions and modalities to usual care, other digital health interventions or modalities or control conditions. Additionally, there were only a small number of studies that directly compared a digital health intervention with an equivalent non-digital intervention, and therefore it is difficult to draw direct conclusions about relative efficacy of digital health approaches to traditional in-person care.
Secondly, this review examined evidence across a range of healthcare disciplines and intervention types, therefore, making comparisons between studies challenging due to the range of outcome measures specific to the intervention. However, the inclusion of interventions across disciplines, allows for the evaluation of current applications of digital health interventions across the board in TBI rehabilitation and assists in understanding how interventions and service delivery in this population are evolving. Additionally, examining digital health in the TBI population across disciplines, encourages researchers and clinicians to further review and develop outcome measures that are applicable in the digital health space itself, as digital health interventions may require more considerations compared with traditional outcomes. This is complemented by Curran and colleagues' recommendations 104 of applying hybrid designs to evaluate clinical effectiveness and implementation of intervention simultaneously to enable fast translational gains, increased effectiveness of implementation strategies and improved dissemination of useful information for decision makers. Lastly, the results here may be influenced by the publication bias towards studies with positive findings, which may skew the impression of the effectiveness of interventions.
Recommendations
The emergence of digital health in TBI interventions has improved accessibility to specialist TBI services, which has been increasingly important during recent years due to restrictions on in-person services related to the COVID-19 pandemic. 105 To ensure that the treatment components of existing evidence-based interventions are retained during the transition to digital health modalities, it is recommended that interventions are customized to these new environments. McLaughlin and colleagues 72 and Rietdijk and colleagues 77 demonstrated this in the adaptation of evidenced based treatment paper manuals allowing for the maximization of opportunities offered in the digital space. The investment in customized online versions of interventions, can be furthered with the consideration of a combination of modalities (particularly videoconferencing and web-based programs) within the same intervention and introduction of bespoke training guided by artificial intelligence. This may include integrated computer algorithms that configure treatment goals and tasks based on the input from the person with brain injury, or automated clinical decision-making tools.
Further, we recommend that researchers undergo a task analysis process when mapping current intervention into an online space. It is crucial to consider which treatment components can be completed synchronously or asynchronously and the inclusion of logistical mechanisms such as screensharing. When considering synchronous and asynchronous treatment components, it is imperative to also consider the impact that real-time or self-guided treatment delivery can have on user engagement and therefore, efficacy of intervention. It is also essential that future research provides a rigorous description of treatment methods and ensures that treatment materials are easily accessible to further accelerate translation of interventions into clinical practice.
The fast-evolving nature and accessibility of digital health has led to a proliferation of mobile applications (apps) available for download to personal mobile devices. Of the 44 studies included in this systematic review, only two studies 60, 88 reported data on the use of apps, focusing on improving executive function and emotional regulation, and completion of kitchen related tasks respectively. This supported by Vaezipour and colleagues, 106 where the researchers used the Mobile App Rating Scale (MARS), 107 a validated tool for assessing the quality of health mobile apps, to review widely available apps for speech-language therapy specific to people with acquired brain injuries. Of the 70 apps that met their inclusion criteria for review, only four apps referred to published empirical studies that assessed app effectiveness. These findings indicate an evidence-practice gap and the need for clinicians to investigate whether an app is supported by evidence prior to providing recommendations and education to people with brain injury and their family members. Educating people with brain injury and caregivers on the importance of evidence-based interventions may also empower them to make informed decisions throughout their rehabilitation journey.
Since the current COVID-19 pandemic, there has been increased lobbying for virtual care to remain a part of offered clinical services. 108 Virtual services have improved the flexibility and availability of financial and human resources and reduced administration time, for example, as a result of electronic data collection and management. 109 With the transition to the digital space, it is essential that clinicians maintain the use of validated assessment tools and outcome measures in psychosocial TBI practice and research. 110 Clinicians are also encouraged to be familiar with regulatory compliance with this new digital environment within their workplaces and services. Effective and successful clinical implementation of digital health interventions necessitates careful patient specific considerations. The severity of injury is an important consideration during clinical decision making when selecting an appropriate digital health modality and intervention.
For example, mobile apps are best considered when the person with brain injury has awareness and cognitive capacity to manage a self-guided intervention. Time post-injury and the stage of an individual's recovery can also impact on clinical decision making when ensuring unification between life goals and needs with the introduction of technology. Technology can improve everyday life and functional goals, such as engaging with family and friends, return to work and participating in education and learning. The studies included in this systematic review showcase how these goals can be targeted using a range of digital modalities, such as Salazaar and colleagues 80 using telephone-based interventions to target return to work for military personnel, or Powell and colleagues 74 targeting quality of life and emotional well-being of caregivers through a web-based program.
It is essential to note that technology, on its own, will not improve functioning, but rather it is a tool to be used as part of a holistic rehabilitation program focused on person centered goals. By choosing digital health modalities that correspond to the patient's life goals and functional needs, clinicians can support individuals with brain injury to regain necessary skills to return to their life roles. With the application of technology in rehabilitation, people with TBI and their caregivers can benefit from the capacity to monitor their own feedback and practice, as well as engage with their therapist. Metacognitive strategy instruction 111,112 can be embedded in the technology itself to encourage self-monitoring and goal setting. These findings and new understandings can inform future work in the development of forthcoming digital health interventions to ensure that the active ingredients within an intervention are maintained during the transition to digital modalities.
The current COVID-19 pandemic has illuminated the value of technology in maintaining social connection, and continuing work and education. Social media, in particular, has been an important way for people with TBI to engage with others and self-advocacy. 113 However, cognitive communication and social cognition 114 difficulties can lead to vulnerability for people with TBI in online environments due to challenges with understanding social cues, detecting humor or sarcasm, and inferencing from written communication. For people with TBI, eHealth safety can be a significant issue; however, social media specific training and education can assist in addressing this. The evidence-based 115 online social media training program, social-ABI-lity, 116 is a novel free self-guided web-based course aiming to increase understanding and knowledge of support people and organizations for safe and successful social media use for people with brain injury and others involved in their care such as family members, friends, support workers and health professionals. The development and use of training and education resources in digital health TBI rehabilitation is critical in ensuring safe and effective implementation of technology.
Conclusion
Overall, this review has found that digital health interventions are as effective and efficacious as traditional face-to-face interventions, and in some cases have potential to produce better outcomes for TBI rehabilitation. However, an appreciation of the active components within these interventions is limited, resulting in a lack of understanding of specific strategies and components that facilitate therapeutic improvement across modalities.
Additionally, it is imperative that further research and intervention development adopt a co-design approach to ensure that the needs of all stakeholders are met. This can then be furthered by using a hybrid research design to simultaneously evaluate clinical effectiveness and implementation of the intervention. A rapid translation of research into clinical practice is essential in the field of digital health, given the fast-evolving improvements in access to and quality of technology.
Footnotes
Acknowledgments
The authors would like to thank Sophie Brassel for her assistance with reliability ratings for this review.
Authors' Contributions
All authors contributed to the study design, data collection and analysis, decision to publish, and preparation of the manuscript.
Funding Information
This work was supported by the University of Sydney Faculty of Medicine and Health Traumatic Brain Injury Scholarship. Author RR is supported by funding from icare NSW. Author LT is supported by an Australian NHMRC Senior Research Fellowship.
Author Disclosure Statement
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LT is Director of speechBITE, and EP is a speechBITE board member.
The authors acknowledge that two of the included papers in the systematic review were authored by the members of the team (RR, LT, EP, and MA) and in this case these papers were not reviewed by those authors.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.