
Abstract
This study aimed to address the risk factors of second decompressive craniectomy (DC) in patients with traumatic brain injury (TBI) who initially underwent mass lesion evacuation, but no primary DC. Patients were enrolled if they had had a hospital visit to Xiangya Hospital, Central South University with acute closed TBI from January 1, 2017 to December 31, 2019 and had undergone craniotomic mass lesion evacuation. Sociodemographic information, computed tomography (CT) information, clinical profiles, and surgical information were obtained from an electronic database. Twenty-four patients who had undergone a second decompressive craniectomy (SDC) and 39 patients who had not (NSO) were included in the analysis. The prevailing lesions differed between the groups (p = 0.010). The SDC group had more compressed/obliterated basal cisterns than the NSO group (p = 0.028). After closure of the dura, the SDC group also had higher intracranial pressure (ICP) than the NSO group (10.9 mm Hg vs. 6.5 mm Hg, p = 0.005). Binary logistical regression indicated that ICP after dura closure was an independent predictor of second DC (odds ratio [OR] = 1.317, p = 0.011). A model using ICP after dura closure alone had an area under the curve value of 0.757 in its receiver operating characteristic curve. An ICP >10.5 mm Hg after closure of dura for the prediction of a second DC had a sensitivity of 56.3% and a specificity of 92.6%.
Introduction
Traumatic brain injury (TBI) is a leading cause of disability and mortality worldwide. 1,2 Traumatic intracranial mass lesions, including epidural hematoma, subdural hematoma, and cerebral contusions, comprise ∼45% of all TBI cases. 3 –5 Mass lesions take up intracranial space, raise intracranial pressure (ICP), compromise cerebral perfusion, and damage surrounding brain tissue through edema formation and direct toxic effects, 6 and in some cases surgical evacuation may be necessary. 7 Intracranial hypertension, secondary to either traumatic mass lesions or cerebral swelling, is an independent predictor of mortality and poor neurological outcome. 8
Decompressive craniectomy (DC) is a widely performed treatment modality for the effective control of intracranial hypertension and reduction of mortality. 9 However, it has vast, debilitating complications and a large socioeconomic impact. 10 –12 In the updated guidelines for severe TBI by the Brain Trauma Foundation (BTF) in 2020, DC is recommended for “late” intracranial hypertension to improve survival and neurological outcome. 13,14 However, there are ongoing debates on whether a primary (or preventive) DC, 8 which is performed concomitantly with the initial mass lesion evacuation surgery, could improve patient outcome, 15 –20 and related high-quality studies (randomized controlled trials and comparative effectiveness research) are underway. 21,22 The lack of evidence contributes to substantial variations in treatment practice for primary DC. 18,23 –25
For the reasons stated, many patients would have the bone flap placed back after hematoma evacuation. However, a significant proportion could develop refractory intracranial hypertension afterwards and require a second operation to remove the bone flap (second DC), which increases the risk of perioperative complications. 26,27 Currently, there is no literature addressing the topic of predicting the second DC after the initial craniotomy. In this article, we present a consecutive series of TBI patients visiting our hospital who underwent emergency operations for mass lesion evacuation with craniotomy. We investigated whether the patients would undergo a second cranial surgery to remove the bone flap (second DC), and analyzed the risk factors in patients with and without a second DC.
Methods
Subjects
In the initial screening from the electronic medical record database, patients were enrolled if they had had a hospital visit to Xiangya Hospital, Central South University for acute closed TBI from January 1, 2017 to December 31, 2019. Patient records were further inspected using the inclusion and exclusion criteria. The inclusion criteria were as follows: (1) being 16–70 years of age; (2) having a head computed tomography (CT) that demonstrated intracranial, supratentorial mass lesions; and (3) having undergone emergent surgical evacuation, with a bone flap placed back (craniotomy). Exclusion criteria included (1) open TBI and (2) having undergone surgical evacuation in other medical centers prior to being transferred to our center. All patients provided signed informed consent, and this study was approved by the hospital's ethics committee (No. 202103048).
Data acquisition
All data were retrospectively collected from the patients' medical records using the electronic database. Sociodemographic characteristics and baseline clinical profiles, including sex, age, date of injury, mechanism of injury, Glasgow Coma Scale (GCS) score, and pupil light reflex status, were collected upon admission to the hospital. CT images obtained at admission were carefully inspected by an experienced traumatic neurosurgeon. Characteristics were summarized by recording the type of prevailing lesion (i.e., the direct target of hematoma evacuation) and by using subscales of the Rotterdam score, including the status of the basal cistern, midline shift, presence of epidural mass lesion, and intraventricular hemorrhage (IVH), or traumatic subarachnoid hemorrhage (tSAH). 28 Information about the surgical interventions were also collected, including names of the initial craniotomic mass lesion evacuation surgery, whether an ICP monitor was inserted, intraoperative ICP after closing the dura but before replacing the bone flap (closing ICP), whether the patient underwent a second cranial surgery during hospitalization, and whether a second DC was undertaken and, if so, the reason for performing it. The choice of placing back the bone flap was based on both the surgeon's discretion and that brain tissue after evacuation of hematoma did not bulge beyond the inner plate of the skull, thus preventing a safe placement. 18 During DC, duraplasty was performed with autologous temporal fascia or neuropatches by non-water-tight closure.
Statistical analysis
Statistical analysis was performed using SPSS software (version 23.0; IBM Corp., Armonk, NY, USA). Categorical variables were interpreted based on the count and frequency. Normally distributed, continuous variables are presented as mean values ± standard deviation (SD); non-normally distributed variables are presented as median values and interquartile range (IQR). Rank variables such as the GCS and Rotterdam scale total scores were interpreted using mean values only. Monovariate analysis was applied to compare the baseline characteristics between patients who underwent a second DC and those who did not undergo a second cranial surgery. Chi-square tests were used to compare the categorical variables. For χ 2 tests yielding significant results, post-hoc χ 2 tests were performed in the categorical subgroups in a two-by-two manner using Bonferroni correction. Student's t tests were used to compare continuous, normally distributed variables, and Mann–Whitney non-parametric tests were used to compare non-normally distributed variables. Rank variables such as the Rotterdam basal cistern subscale, total Rotterdam score, GCS motor, and total GCS scores were compared using non-parametric Mann–Whitney tests. Pupil light reflex status was transformed into a rank variable by assigning “bilateral present,” “unilateral absent,” and “bilateral absent” to values of 1, 2, and 3, respectively, and compared using the Mann–Whitney test. Subsequently, a binary logistical regression was performed to search for independent risk factors for second DC. For all statistical tests, p values <0.05 were considered significant.
Results
Demographics
A total of 169 consecutive patients passed the initial database screening. After careful inspection of medical records, 63 patients (24 patients who underwent second DC and 39 patients who did not) were included in the final analysis. A flow chart of the recruitment process is shown in Figure 1. The mean age of the patients included was 51 ± 13.8 years old, ranging from 18 to 71 years. The age distribution of patients with and without a second DC is shown in Figure 2. Fifty-three (84.1%) patients were male. The mechanisms of injury included traffic accidents (31 cases, 49.2%), falling (28 cases, 44.4%), assault (1 case, 1.6%), and others (3 cases, 4.8%). Demographics between patients who underwent a second DC (n = 24) and those who did not undergo a second cranial operation (n = 39) were compared, and the results are summarized in Table 1. Demographics, including age, sex, and mechanism of injury, did not differ between the two groups.
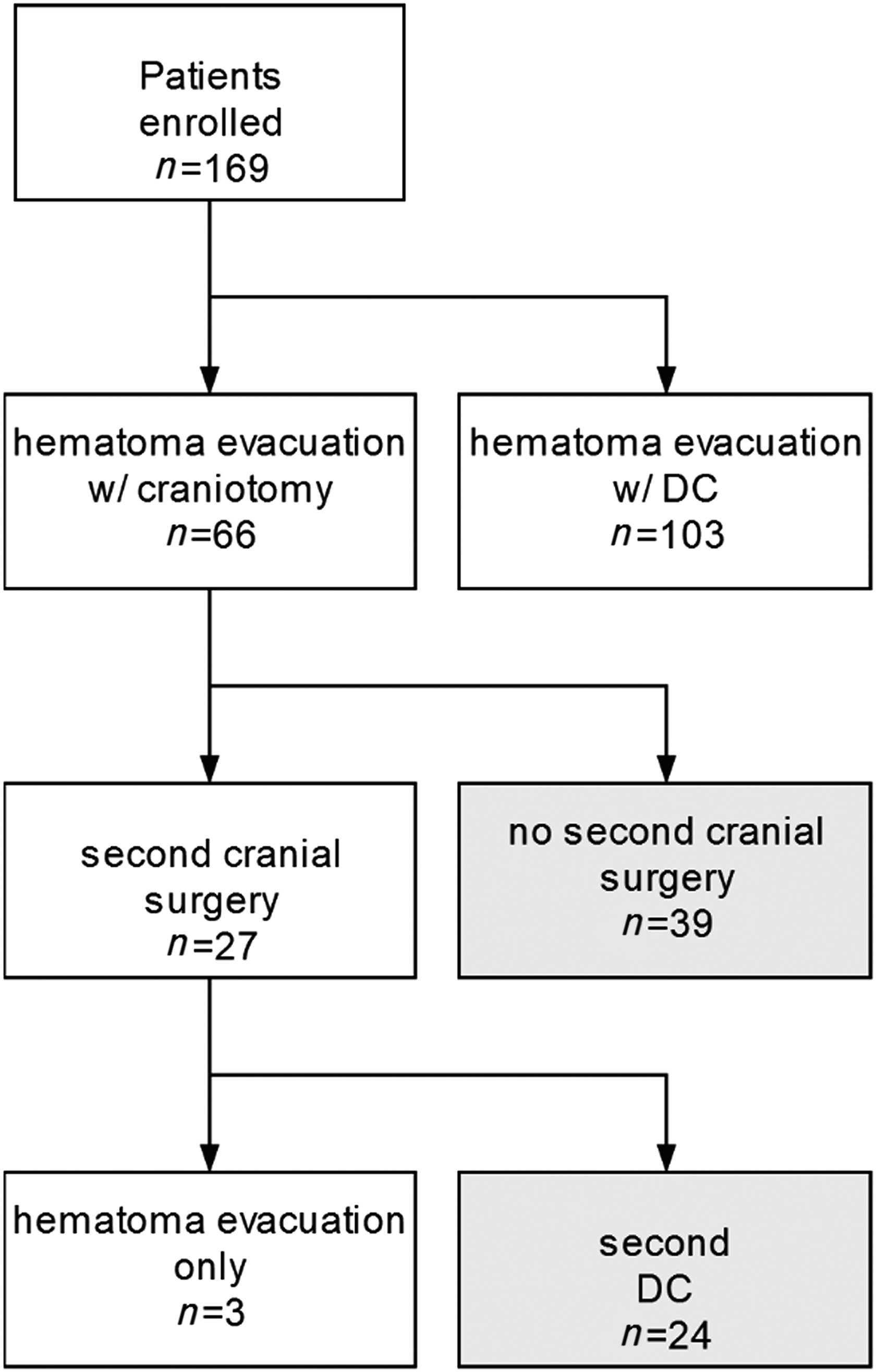
Patient inclusion flow chart. A total of 169 consecutive patients passed the initial screen, but only 63 patients entered the analysis, of whom 24 underwent second decompressive craniectomy (DC) and 39 did not receive a second cranial surgery.
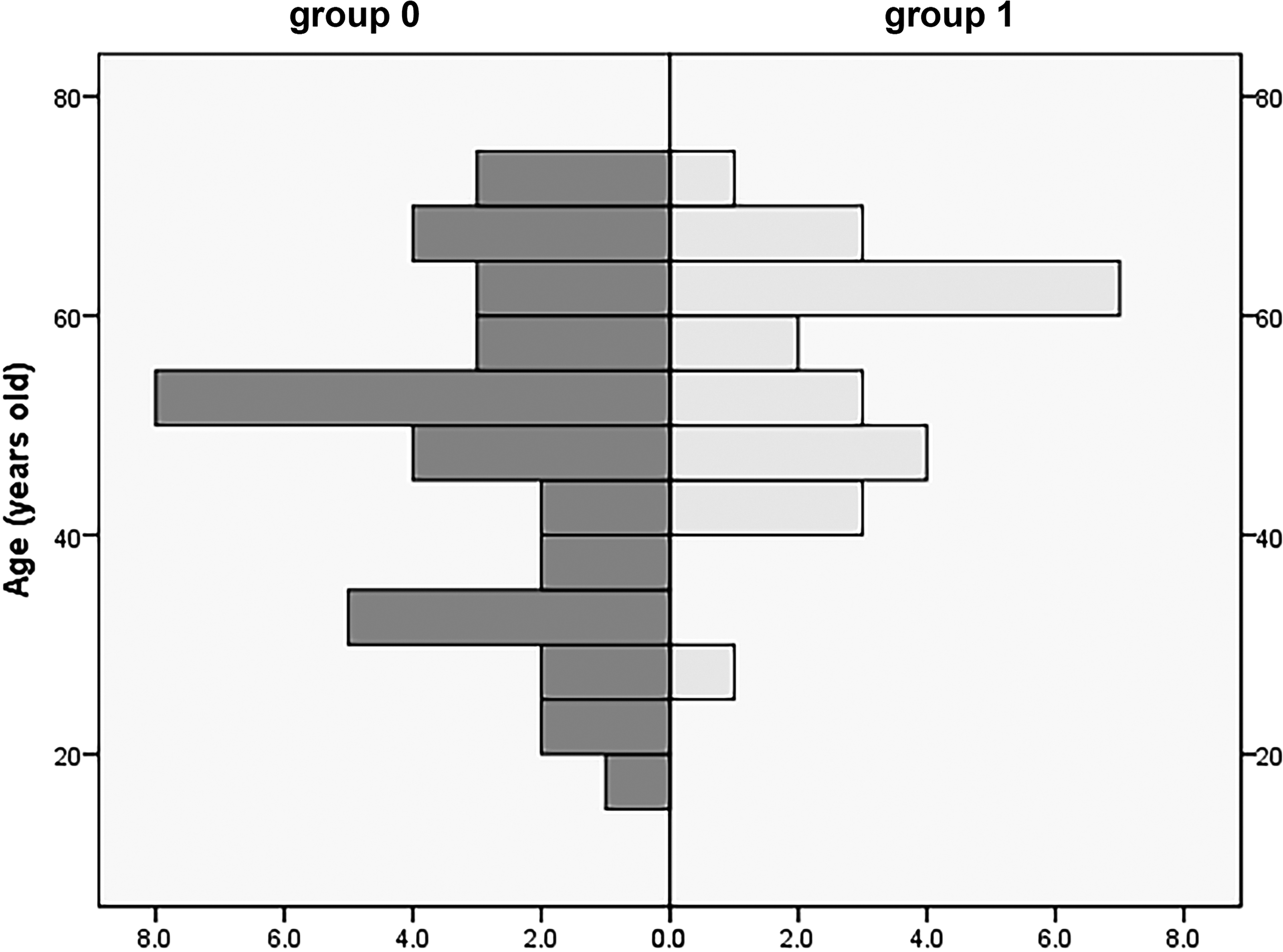
Age distribution of patients who underwent second decompressive craniectomy (group 1) and those who did not (group 0).
Comparison of Demographic, Clinical, and CT Characteristics
Comparison of demographic, clinical, and CT characteristics between patients who underwent a second decompressive craniectomy (DC) (SDC, n = 24) and those who did not (NSO, n = 39).
p values of statistical analysis using non-parametric tests.
Significant differences between groups in post-hoc χ 2 tests using Bonferroni correction.
Pupil light reflex score is defined by assigning “bilateral reflex present,” “unilateral reflex absent,” and “bilateral reflex absent” to values of 1, 2, and 3 respectively.
CT, computed tomography; GCS, Glasgow Coma Scale; ICP, intracranial pressure; IVH/tSAH, intraventricular hemorrhage/traumatic subarachnoid hemorrhage.
CT characteristics
The characteristics of the CT images upon admission are summarized as follows.
Prevailing lesions
Among the 63 patients included, 19 (15.9%) had epidural hematoma as the prevailing lesion, 8 (12.7%) had subdural hematoma as the prevailing lesion, and 36 (57.1%) had contusions as the prevailing lesion.
Basal cistern
Twenty-one (33.3%) patients had a normal basal cistern, 31 (49.2%) had a compressed basal cistern, and 11 (17.5%) had a completely absent basal cistern.
Midline shift
A total of 36 (57.1%) patients had no or <5 mm of midline shift, whereas 27 (42.9%) had a midline shift of ≤5 mm.
Epidural mass lesion
A total of 27 (42.9%) patients had epidural mass lesions, whereas 36 (57.1%) patients did not.
Intraventricular hemorrhage or traumatic subarachnoid hemorrhage
Five (7.9%) patients did not have either, whereas 58 (92.1%) patients had at least one finding.
Rotterdam score
The total Rotterdam score was calculated by adding all the subscores and adding 1. Two (3.2%) patients scored 1 point, 6 (9.5%) scored 2 points, 14 (22.2%) scored 3 points, 26 (41.3%) scored 4 points, 13 (20.6%) scored 5 points, and 2 (3.2%) patients scored the highest possible 6 points. The distribution of the total Rotterdam scores between patients with and without a second DC is displayed in Figure 3.
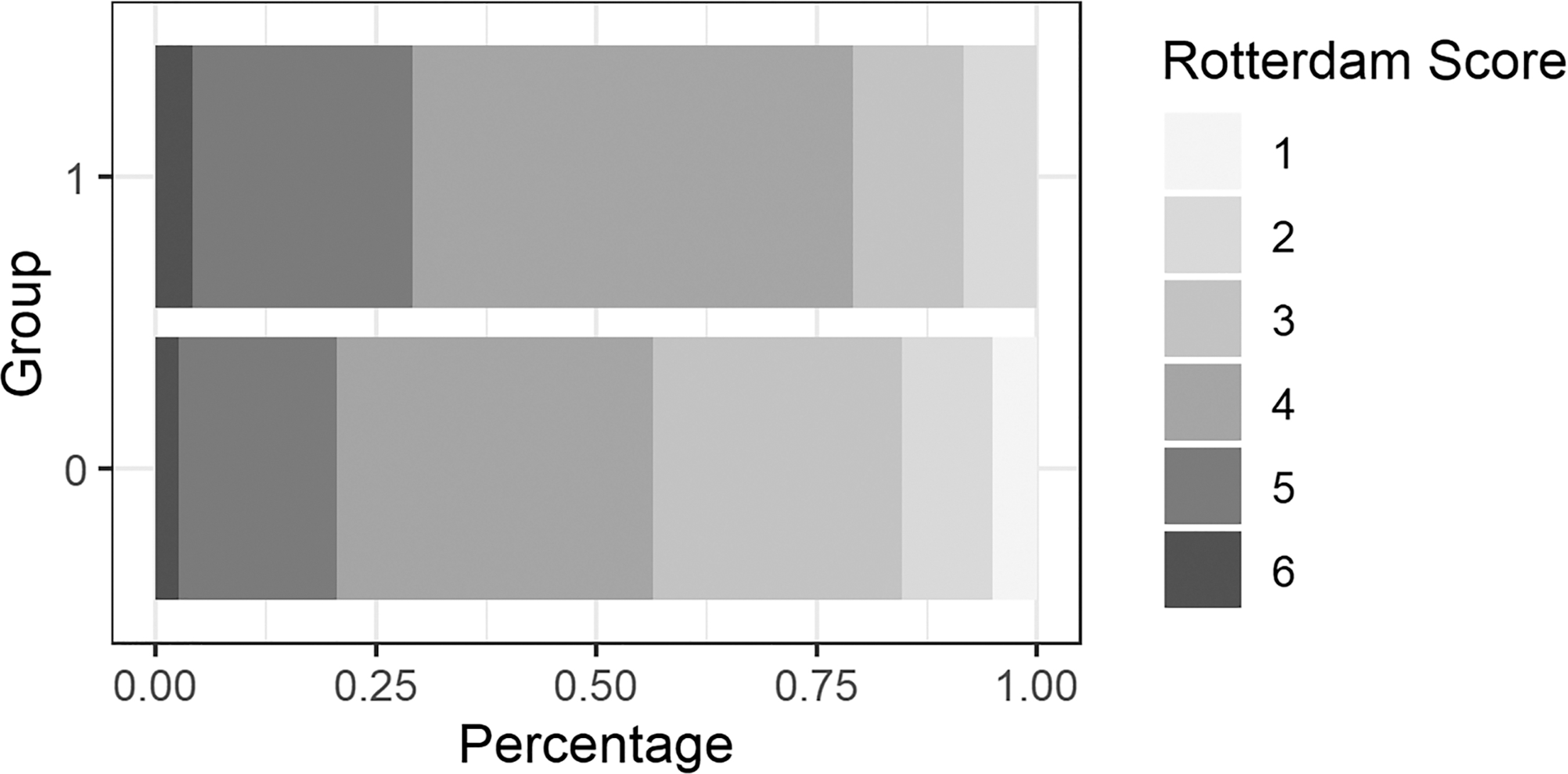
Distribution of total Rotterdam score for patients who underwent a second decompressive craniectomy (SDC, group 1) and those who did not (NSO, group 0).
CT characteristics
The CT characteristics between patients who underwent a second DC (n = 24) and those who did not (n = 39) were compared and are shown in Table 1. Patients with different prevailing lesions differed in the relative risks of having a second DC (p = 0.010). More specifically, post-hoc tests (with Bonferroni-corrected significance values of 0.05/3 = 0.017) indicated that patients harboring subdural hematoma had higher risks of a second DC than patients harboring epidural hematoma (p = 0.006), whereas no difference was observed when comparing patients with contusions with those with epidural hematoma (p = 0.047) or with subdural hematoma (p = 0.094). Patients with higher basal cistern scores (toward compressed/absent) were more likely to undergo a second DC (p = 0.028). Patients in the second DC group also had a higher total Rotterdam score, although this did not reach statistical significance (p = 0.109). The status of midline shift, presence of epidural mass lesion and IVH/tSAH did not differ significantly between the groups.
Clinical profiles
Pupil reflex status was classified into (1) bilateral reactive, (2) unilateral unreactive, and (3) bilateral unreactive. Among the 63 patients, 57 (90.5%) had bilaterally reactive pupils, 1 (1.6%) had unilaterally reactive pupils, and 5 (7.9%) had bilaterally unreactive pupils.
The results of the GCS examination upon patient admission are summarized as follows. For patients who were intubated, the V subscale was recorded as “VT” and was added as 1 point to the total score. With the exception of 8 patients who had unidentifiable GCS examination results, among the remaining 55 patients, 18 patients (32.7%) scored 13–15, 23 patients (41.8%) scored 9–12, and 14 patients (25.4%) scored 3–8.
Clinical profiles of patients who underwent a second DC (n = 24) and those who did not (n = 39) were compared and are shown in Table 1. Their clinical profiles, including pupil light reflex score, GCS motor score, and total score, did not differ significantly between the groups.
Surgery
Standard unilateral fronto-temporo-parietal craniotomies (12 × 15 cm) were used for patients undergoing hematoma evacuation. If a patient was to receive a second DC, the bone flap was not replaced. Among the 63 patients included in the analysis, 24 (38.1%) underwent a second DC, and the remaining 39 (61.9%) patients did not undergo a second cranial operation. Fifty-eight (92.1%) patients underwent concomitant intraventricular ICP monitor insertion and five (7.9%) patients received extraventricular drainage with the ICP measured by hydraulic coupling during the initial surgery for hematoma evacuation. The mean value of intraoperative ICP after closure of the dura (closing ICP) was 8.1 ± 4.42 mm Hg, ranging from 1 to 20 mm Hg. As demonstrated in Table 1, the closing ICP significantly differed between the groups. Patients who underwent a second DC had a higher closing ICP (10.9 ± 5.0 mm Hg) than patients who did not undergo a second cranial surgery (6.5 ± 3.12 mm Hg) (p = 0.005).
Prediction of second DC
Univariate analysis revealed that patients who underwent a second DC and those who did not undergo a second DC differed in prevailing lesion (p = 0.010), basal cistern status on CT (p = 0.028), and ICP after closure of the dura (p = 0.005). For further exploration, a binary logistical regression was performed using the prevailing lesion, Rotterdam basal cistern subscale, and closing ICP as predictive factors, demonstrated in Table 2. The basal cistern status was binarized (“present” and “compressed/absent”). The model demonstrated that the closing ICP served as an independent predictor of second DC (odds ratio [OR] = 1.317, 95% confidence interval [CI] 1.066–1.628, p = 0.011). Basal cistern status approached statistical significance (OR = 0.157, 95% CI 0.018–1.413, p = 0.099). The model had a predictive accuracy of 72.1%, and the area under the receiver operating characteristic (ROC) curve (AUC) value was 0.817 (Fig. 4A).
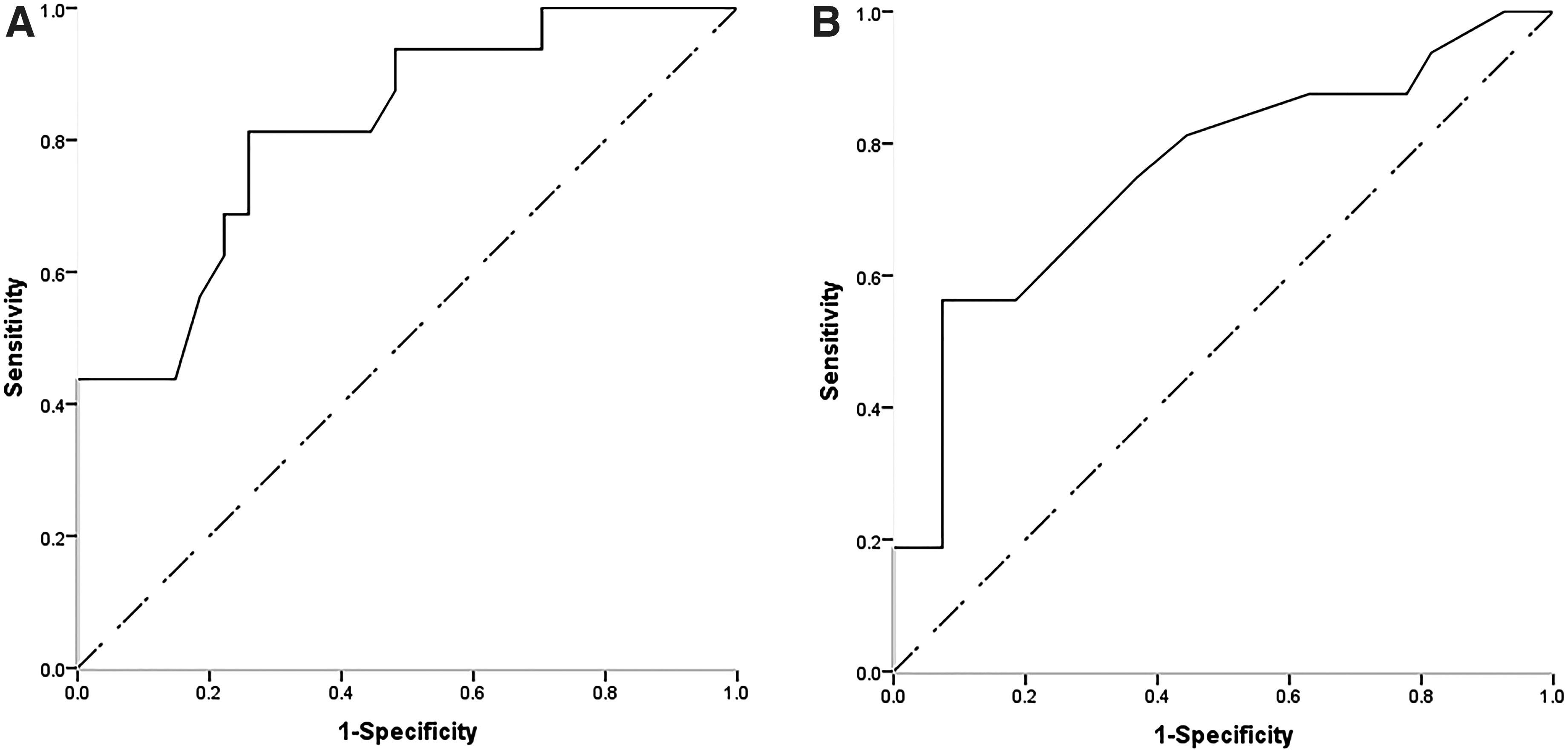
Receiver operating characteristic (ROC) curves for predictive models of second decompressive craniectomy (DC).
Prediction of Second DC Using Logistical Regression
Prediction of second DC using logistical regression for patients receiving hematoma evacuation but not craniectomy.
CI, confidence interval; DC, decompressive craniectomy; ICP; intracranial pressure; OR, odds ratio.
For the sake of simplicity in clinical scenarios, we used closing ICP alone as a predictor of second DC. The AUC of the ROC curve was 0.757 (Fig. 4B). A cutoff value of 10.5 mm Hg for the prediction of second DC had a sensitivity of 56.3% and a specificity of 92.6%.
Discussion
In this study, we investigated risk factors of second DC in patients who had undergone evacuation of a traumatic intracranial mass lesion, without primary craniectomy.
Factors that affect the risk of second DC can be roughly classified into two categories: one that takes place before the decision of primary DC is made (such as CT scan on admission and intraoperative ICP) and one that takes place after that (such as post-operative medical management). We focused on the former, hoping to provide a tool that helps with intraoperative decision making. We found that the prevailing lesion (p = 0.010), basal cistern status on CT (p = 0.028) and ICP after closure of the dura (closing ICP, p = 0.005) were risk factors for a second DC, with the closing ICP as an independent predictor, and the predictive value of basal cistern status being close to statistical significance.
The risk factors could be explained by their contributions to post-operative intracranial hypertension and therefore to the need for a second DC. 29 Many studies have shown that lesion types contribute differently to intracranial hypertension. Patients with intracranial traumatic mass lesions harbor a variety of situations, including epidural hematoma with minimal brain involvement and subdural hematoma with surrounding contusions and brain swelling. Not all of the foregoing will lead to refractory intracranial hypertension that requires a second DC. The incidence of intracranial hypertension in patients with evacuated epidural hematoma varies from 11.7% to 62.5%, depending on the coexisting intracranial pathologies such as brain swelling and neighboring contusions, 26,30 whereas pure epidural hematoma seldom results in intracranial hypertension. Therefore, in most cases, DC may not be essential. 31 The incidence of intracranial hypertension in patients with evacuated acute subdural hematoma ranged from 43% to 67%, in which a significant proportion might need a second DC. 26,27 This was in accordance with our finding that the risk of requiring a second DC was higher in patients with acute subdural hematoma than in those with epidural hematoma as prevailing lesion (p = 0.006). Patients with evacuated contusions have a varied incidence of intracranial hypertension, 26 and currently there is no evidence or consensus regarding primary DC following evacuation of intraparenchymal lesions. The choice may be highly dependent on the surgeon's discretion. 29
Basal cistern status and ICP after closure of dura were both predictive of second DC. According to the Monro–Kellie doctrine, brain swelling, namely an increase in water content inside the brain, could also contribute to ICP. 32 The status of the basal cistern, whether visible, compressed, or obliterated, could reflect brain swelling and might explain its predictive value for a second DC. ICP after dura closure was actually a “decompressed” ICP, and therefore indicative of future ICP and the need for a second DC. The basal cistern status approached (but did not reach) statistical significance (p = 0.099), likely because of the limited number of cases in our study.
Two prediction models were constructed in our study, one using the prevailing lesion, the basal cistern status, and closing ICP, and the other using closing ICP alone, both of which had comparable predictive values (AUC 0.817 vs. AUC 0.757). Although adding the prevailing lesion and basal cistern status seems to provide an information gain for the model, a simpler and surgeon-friendlier method of predicting a second DC using closing ICP alone might be a feasible choice. A cutoff value was provided in the Results section. We realize that there would be many factors to consider when deciding whether to remove the bone flap, many of which do not fall into the category of medical concerns. Therefore, the closing ICP can only serve as a reference. The ultimate choice should be made at the surgeon's discretion.
This study was based on the assumption that, if a patient was at high risk of second DC, then a primary DC along with hematoma evacuation might be beneficial rather than one hematoma evacuation surgery followed by a second surgery only to remove the bone flap, because the latter has increased medical costs as well as increased perioperative complications. 26,27 However, several aspects should be considered when making this deduction. First, a second DC cannot be readily predicted based on preoperative and intraoperative information. Many of the factors contributing to a second DC take effect post-operatively. For example, different medical treatment regimens, including osmotic agents, hyperventilation, sedation and analgesia, and hypothermia, can lead to different outcomes. 26,27,31 In our center, a set of general rules derived from guidelines and consensus was applied to all patients, but we could expect a different situation in centers with practices that differed from ours. 33,34 Second, a DC “in advance” is not necessarily good. DC performed at different stages of the disease could have different influences on brain physiology, clinical condition, and neurological outcome. Both the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC) consensus on the management of severe TBI patients with ICP monitoring and the Consensus REVised Imaging and Clinical Examination (CREVICE) consensus on those without ICP monitoring recommended DC as a tier 3 therapy against (suspected) intracranial hypertension. 33,34 Besides, in the 2020 update of DC in the BTF guidelines for severe TBI, an “early” DC is less recommended than a “late” DC regarding ICP control. 13 Although decompressive craniectomy as mentioned in the BTF guidelines only refers to secondary DC meant to control ICP, a deduction might be made that DC in some way should be regarded as a reserve instead of first-line treatment for intracranial hypertension, let alone as a “preventive” one in patients who currently do not exhibit signs of high ICP at all. This questions the benefit of primary DCs, even in patients who would possibly undergo a second DC in the future.
This study has several limitations. First, this was a retrospective study with a relatively small sample size. Second, no neurological consequences following DC were addressed in this study. Further prospective studies with larger sample size are warranted to better predict second DC following initial craniotomy.
Conclusion
Under certain circumstances, replacing the bone flap after hematoma evacuation could result in future DC in patients with traumatic intracranial mass lesions. In this study, we investigated risk factors for a second DC if patients had undergone evacuation of a traumatic intracranial mass lesion but no craniectomy. This study found that ICP after dura closure independently predicted a second DC with an AUC of 0.757. A cutoff value of 10.5 mm Hg had a sensitivity of 56.3% and specificity of 92.6%.
Footnotes
Authors' Contributions
Ziyuan Liu was responsible for idea synthesizing, data collection, manuscript writing, and revision. Shan Du was responsible for statistical analysis, manuscript writing, and revision. Yun Wu was responsible for clinical management of patients and manuscript drafting. Tiange Chen was responsible for statistical consult and revision. Xiangying Luo was responsible for technical support regarding ICP monitoring. Changlong Bi was responsible for consult regarding surgery. Song Lan was responsible for patient cohort management. Xin Chen was responsible for revision of manuscript and quality control. Jinfang Liu was responsible for general consult, supervision of the whole process, and quality control.
Funding Information
Provincial Key Research and Development Program of Hunan (2020SK2070); Health Commission Scientific Research Project in Hunan Province (C20180784); Xiangya Medical Big Data Foundation.
Author Disclosure Statement
No competing financial interests exist.