
Abstract
The identification of effective pharmacotherapies for traumatic brain injury (TBI) remains a major challenge. Treatment with heparin and its derivatives is associated with neuroprotective effects after experimental TBI; however, the optimal dosage and method of administration, modes of action, and effects on hemorrhage remain unclear. Therefore, this review aimed to systematically evaluate, analyze, and summarize the available literature on the use of heparin and low molecular weight heparins (LMWHs) as treatment options for experimental TBI. We searched two online databases (PubMed and ISI Web of Science) to identify relevant studies. Data pertaining to TBI paradigm, animal subjects, drug administration, and all pathological and behavior outcomes were extracted. Eleven studies met our pre-specified inclusion criteria, and for outcomes with sufficient numbers, data from seven publications were analyzed in a weighted mean difference meta-analysis using a random-effects model. Study quality and risk of bias were also determined. Meta-analysis revealed that heparin and its derivatives decreased brain edema, leukocyte rolling, and vascular permeability, and improved neurological function. Further, treatment did not aggravate hemorrhage. These findings must be interpreted with caution, however, because they were determined from a limited number of studies with substantial heterogeneity. Also, overall study quality was low based on absences of data reporting, and potential publication bias was identified. Importantly, we found that there are insufficient data to evaluate the variables we had hoped to investigate. The beneficial effects of heparin and LMWHs, however, suggest that further pre-clinical studies are warranted.
Introduction
Traumatic brain injury (TBI) is one of the leading causes of disability and death among the active population aged less than 45 years. It is caused by an external mechanical force to the head, and it is associated with incidents such as falls, motor accidents, bullet injury, industrial accidents, or sports-related injuries. With the increasing global incidence of TBI, it has been estimated that 69 million persons worldwide will have a TBI each year. 1
A TBI triggers a cascade of events that are classified as primary and secondary injury mechanisms. Primary injury, which includes axonal shearing, tissue destruction, and hemorrhage, results from the initial impact at the time of trauma. Secondary injury occurs within minutes to days and is characterized by a number of molecular, metabolic, and cellular processes, including disruption of the blood–brain barrier, brain edema, neuroinflammation, ischemia, apoptosis, oxidative stress, and lipid degradation, that may eventually result in additional brain dysfunction and chronic neurodegeneration. 2 –4
There is currently no effective drug treatment available for the ongoing brain damage associated with TBI despite many promising pre-clinical studies that have identified potential therapeutic agents over the years. 5 Moreover, drug development for TBI continues to face significant challenges because of the presentation of very diverse and varying pathophysiologies among patients with TBI. 6
One group of drugs that is of interest as a potential pharmacotherapy for TBI is heparins (including unfractionated heparin [UFH] and modified heparin 2,3-O-desulphated heparin, ODSH) and low molecular weight heparins (LMWHs). Heparins and LMWHs are well known for their use as anticoagulants. These glycosaminoglycans have a chemical structure consisting of recurring disaccharide units of uronic acid and
The highly negatively charged UFH has many unwanted characteristics, such as drug-induced adverse effects and an unpredictable dose-response after its administration, because it interacts with a wide range of proteins. 8,9 Conversely, LMWHs have fewer negative charges and exhibit low affinity for plasma proteins and, therefore, have a better safety profile, more predictable pharmacokinetic properties, and improved efficacy, with reduced risk of bleeding compared with heparin. 10 Hence, LMWHs are more preferred for clinical use.
Heparins and enoxaparin, one of the most frequently used LMWHs, have demonstrated promising neuroprotective effects in pre-clinical TBI models, including reduced cerebral edema and lesion size and improved motor and cognitive recovery. 10 Overall, the mechanisms underlying these pharmacological effects remain unknown; however, they are distinct from heparin and LMWHs' anticoagulant actions.
Importantly, despite the apparent benefits of heparin and LMWHs in TBI, these drugs are not used clinically, at least in the first 24 h after trauma, because of the potential risk of bleeding. 11 In the pre-clinical TBI literature, however, the incidence of hemorrhage after treatment with heparins/LMWHs remains unclear. It is also unclear whether UFH, modified heparins, or LMWHs have different protective actions, and what dosage and method of administration is optimal. As well, the overall efficacy of heparins/LMWHs to reduce specific secondary injury pathologies remains to be determined.
Therefore, this systematic review and meta-analysis aims to critically evaluate, summarize, and analyze data from the literature describing the use of heparins and LMWHs as treatment in animal models of TBI. In doing so, we will address the following questions: (1) do heparins and LMWHs (enoxaparin and dalteparin) have protective effects after TBI in animal models?; (2) what dose and route of administration produces maximal beneficial effects?; (3) what is the relative efficacy of heparins versus LMWHs?; and (4) does treatment increase brain hemorrhage after TBI?
Methods
A comprehensive systematic search of both PubMed and Web of Science was conducted based on the current guidelines of Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 12 (Supplementary Data S1). The protocol was registered with the international prospective register of systematic reviews (PROSPERO; CRD42020205574).
Sources of information and search strategy
Two electronic databases (Medline via PubMed and Web of Science) were searched since inception to August 2021 for relevant articles. Additional studies were sourced from the reference list of included articles.
Using Systematic Review Centre for Laboratory Animal Experimentation's (SYRCLE) guidelines, 13 a detailed search strategy was developed in collaboration with a research librarian. Comprehensive synonyms and alternate words/terms were generated (Supplementary Data S2) for each of the main keywords (heparin/LMWHs, traumatic brain injury, and animal model) to search titles and abstracts in the databases mentioned above. More alternate terms were added from PubMed MeSH terms as searches were performed and from the references of the relevant articles that were included in the study.
The advanced search tools of PubMed and Web of Science were employed to search for both titles and abstracts. The Boolean operators “OR, AND, NOT, or AND NOT” were used to combine or exclude keywords in the searches for this review. Once the search was completed, duplicate references were removed using the EndNote citation management software (EndNote version X9, Thomson Reuters, New York). Detailed information on the search strategy can be found in Supplementary Data S3.
Inclusion criteria and exclusion criteria
We included peer-reviewed primary research articles describing the use of heparin (including modified heparins) and/or LMWHs as potential treatment for TBI in any animal model of TBI, including TBI transgenic models. We also included randomized controlled studies with control and experimental groups that clearly stated the number of animals in each group. Studies that administered heparin and/or LMWHs irrespective of the dose, route, frequency, duration, and time after brain injury were included.
We included studies that assessed functional and/or neuropathological outcomes of TBI, such as: motor, behavioural, or cognitive function, lesion volume, blood–brain barrier permeability, brain edema, neuroinflammation, hemorrhage, and the recruitment of immune cells from the blood. Finally, to be included, studies were required to report data as group means and variance (standard error of the mean or standard deviation). (No studies were excluded for violating this criterion.)
We excluded review articles and studies published in languages other than English. Studies involving other drugs as co-treatment were also excluded.
Study selection and data extraction
Two authors (MA and XYL) independently screened the titles and/or abstracts to identify publications that met the eligibility criteria, and differences were resolved in cases of no consensus by discussion with a third reviewer (NB).
The studies were exported to Rayyan QCRI (Qatar Computing Research Institute) software after the removal of duplicates.
All articles approved after the initial title and abstract screening underwent a further full-text screening step by two independent reviewers (MA and XYL), and disagreements between the independent reviewers were resolved by a third reviewer (NB).
Data were extracted from the manuscripts by text or by extrapolating numerical values from graphs in eligible studies. We extracted data for study identification elements, including the title, name of authors, journal, and publication date of articles; components of study design including animal details, injury characteristics, time, route, dose, frequency and duration of drug administration; and TBI pathological and behavioral outcomes assessed and the method of assessment.
Data were extracted and treated as independent experiments when a single study reported more than one experiment, and, as recommended by the Cochrane collaboration, the groups were combined to generate a single pair-wise comparison against the control group. 14 Authors were contacted directly for further clarification or more information in cases of missing data.
Risk of bias/quality assessment
The risk of bias (RoB) of the included studies was assessed with SYRCLE's RoB tool, 15 and the quality assessment of all studies was evaluated according to a modified checklist from the Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES) with slight modification. 16,17 The checklist comprised the following 10 criteria: (1) peer-review publication; (2) random group allocation; (3) blinded induction of injury; (4) blinded assessment of outcome measures; (5) use of an anesthetic/analgesic agent without marked neuroprotective activity; (6) statement of compliance with animal welfare regulatory requirements; (7) statement of potential conflicts of interest; (8) use of appropriate animal model; (9) calculation of sample size; and (10) explanation of excluded animals. One point was given to indicate the presence of each criterion.
Data analysis
In this review, a meta-analysis and a narrative synthesis were both employed. The effect of heparins and LMWHs on brain edema, leukocyte rolling, microvascular permeability, hemorrhage/hemorrhagic contusion, neurological function, and body weight loss was estimated by calculating the standardized mean difference (SMD; mean difference between groups divided by the standard deviation of outcome effect) for each comparison and combining these values in a weighted mean difference meta-analysis using a random-effects model. 18 This method was chosen because it permits aggregation of data from studies measuring the same outcome in different ways. 19,20 For instance, evaluating neurological function using different neurological assessment tools. Results are presented as overall SMD and its 95% confidence intervals (CIs).
The presence of heterogeneity was assessed using the I2 statistic, the percentage of the variability in effect estimates that is because of heterogeneity rather than sampling error (chance). 14 Higher values indicate a greater degree of heterogeneity.
A priori examination of which experimental factors contribute to outcome heterogeneity was performed primarily by subgroup analysis. Subgroup analysis for drug types and their doses was conducted only for the brain edema outcome where data were most abundant. In addition, funnel plots and Egger tests were conducted to investigate the presence of small sample effects that might result from problems such as publication bias.
For all UFH studies, 21,22 the dose given was recorded as U/kg, and so was converted to mg/kg according to standard dosing guidelines (100 U/kg = 1 mg/kg). 23 After conversion, doses of both enoxaparin and heparin were either categorized as low dose (≤1 mg/kg) or high dose (≥2 mg/kg).
In this review, the controls were untreated injured animals while the treatment groups received either heparin or enoxaparin at varied times and doses post-injury.
For the narrative synthesis, all 26 outcomes that were extracted from the included studies were summarized in tables based on, but not limited to, the drug dosage, drug type, and overall efficacy of the different drugs (heparin, ODSH, and enoxaparin), with their major findings discussed. Meanwhile, meta-analyses were conducted for outcomes where data were available from at least three publications. (See Supplementary Data S4 for a flowchart illustrating the relationship between the narrative and quantitative aspects of this review.)
All meta-analyses were performed using Review Manager (RevMan, Version 5.4, the Cochrane Collaboration, 2020) and/or StataSE software (version 16, StataCorp LP, Texas) with a significance level set at p < 0.05. The effect estimates of all the outcomes in the summarized table (Table 3) were also performed using RevMan. For data represented as forest plots, the central lines and lateral tips of the diamond signify pooled point estimates and the corresponding 95% CIs, respectively. The solid black vertical line indicates the line of no effect while the red vertical line is the overall effect size line.
Results
Study selection
Our search found 339 potentially relevant publications. Sixty-three were replicates because of database overlap and were removed. Of the remaining 276 publications subject to title and abstract screening, 12 were selected for full-text review. One of these was excluded for not meeting our pre-specified inclusion criteria. Eleven publications 21,22,24 –32 were included in the review (Fig. 1). From the included studies, meta-analysis was conducted on the data from seven publications 21,22,24,25,28,29,32 for brain edema, neurological function, hemorrhage/hemorrhagic contusion, microvascular permeability, leukocyte rolling, and body weight (see Supplementary Data S5 for number of comparisons of each outcome).
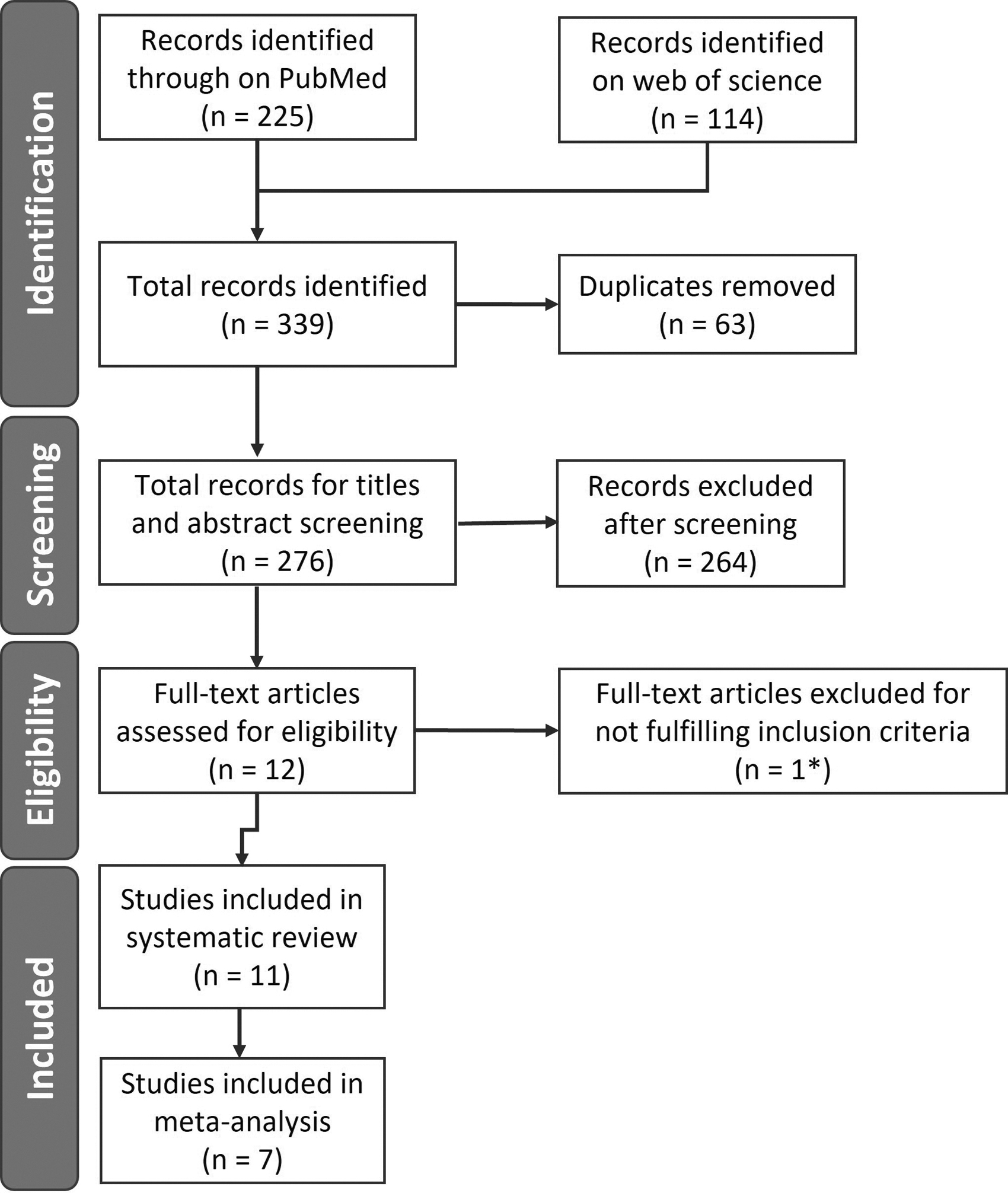
Flowchart of study process. A total of 11 studies were included in this review after the literature search process, and meta-analysis was conducted on seven studies. *One study was excluded during full-text screening because enoxaparin was administered in combination with another drug.
Study characteristics
The characteristics of the included studies, published between 2000 and 2020, are shown in Table 1. Of the 11 studies, seven administered enoxaparin, 24 –30 two studies administered unfractionated heparin, 21,22 and one study each administered ODSH, 32 and heparin oligosaccharides, 31 respectively. All the animals studied were male. The CD-1 mouse strain was the most commonly used animal, 21,22,24,32 followed by Sprague-Dawley 25,28,29 and Wistar 30,31 rats. One study each used the C57BL/626 and BALB/c 27 mouse strains, respectively. Mice ranged in weight from 20 to 32 g and rats ranged from 100 to 450 g. Six studies reported using adult animals but did not specify an exact age, 21,22,24,28,30,32 four studies reported using mouse models aged between 4 to 12 weeks, 25 –27,31 and one study failed to report the age of animals used. 29
Characteristics of Included Studies
QA, quality assessment; NR, not reported, CCI, controlled cortical injury, IV, intravenous; IP, intraperitoneal; SC, subcutaneous; FPI, fluid percussion injury; LFPI, lateral fluid percussion injury, *Adult as specified by the authors of the different studies.
Controlled cortical impact was the most frequently used model of TBI, 21,22,24,26,32 while two studies used the weight-drop impact model. 25,28 In most studies, the injury induced was severe, 21,22,24,26,28,32 while two studies reported moderate injury 29,30 and one study reported a mild injury. 25 Two studies failed to report injury severity. 27,31
Drugs were either administered immediately after trauma induction or between 15 min and 2 h after injury as a single dose 26,27,31 or multiple doses. 21,22,24, 28 –30,32 The subcutaneous (SC) injection was the most used mode of drug delivery as reported by six studies 21,22,24,25,30,32 ; two studies used both intravenous (IV) and SC injections. 28,29 Direct administration into the wound cavity, 31 intravenous, 26 and intraperitoneal (IP) 27 injection were each reported in one study, respectively. Drugs, dosing, time to first administration, and frequency of administration are detailed in Table 2.
Details of Treatment Intervention from the Included Studies
TBI, traumatic brain injury; ODSH, 2,3-O-desulphated heparin.
As detailed in Table 3, of the 26 outcomes extracted, brain edema and neurological function were the outcomes most commonly assessed, being reported in five studies, 21,22,24,29,32 followed by leukocyte rolling, 21,24,32 body weight loss, 21,22,24 microvascular permeability, 21,24,32 hemorrhage, 24,25,28 and apoptosis, 27,28,30 all with three studies each. Brain infarct volume 27,29 and leukocyte adhesion 21,22 were reported by two studies each, and the remaining outcomes including oxidative stress, 30 cognitive function, 29 learning, 32 hemoglobin levels, 22 motor function, 32 inflammation, 28 glial scar formation, 31 interleukin (IL)-1β, 26 pro-IL-1β, 30 caspase-1, 26 cyclooxygenase (COX) expression, 30 reactive gliosis, 30 lesion surfaces, 29 polymorphonuclear (PMN) sequestration, 22 neurodegeneration, 30 as well as total antioxidant status and total oxidant status, 27 were reported by one study each.
Summary and Findings of All Outcomes from Included Studies
UFH, unfractionated heparin; ODSH, 2,3-O-desulfated heparin; TBARS, thiobarbituric acid-reactive substances; SOD, Superoxide dismutase; GSH-Px, glutathione peroxidase; H&E, Haematoxylin and Eosin; PBS, phosphate-buffered saline; CS-A, chondroitin sulfate-A; GFAP, glial fibrillary acidic protein; PMN, Polymorphonuclear; IL-1, Interleukin-1; COX-2, Cyclooxygenase-2; CIBI, cold-induced brain injury; CCI, controlled cortical injury; WDI, weight drop injury; FPI, fluid percussion injury; LFPI, lateral fluid percussion injury.
(Only low dose was assessed)
The wet/dry weight ratio method was used to assess brain edema, while the validated, modified Garcia Neurological Test and the Neurological Severity Score were the most frequent methods used to assess neurological function. The summary of the method of assessment of the other outcome measures used is included in Table 3.
RoB and quality assessment
The RoB analysis, as shown in Figure 2, highlights the possible sources of bias in the included studies. Baseline characteristics were generally well reported (91% of studies) with only one study failing to report these key details. 29 Most other facets of study reporting, however, suggest the data are at significant risk of bias. No studies described random housing, random outcome assessment, or blinding of assessors. Of all the included studies, 70% had evidence of selective outcome reporting 21,22,24 –26,28,31,32 because the sample size planned or analyzed was not reported. Only three studies did not have selective outcome reporting because they reported all outcomes and sample sizes evaluated and analyzed. 27,29,30
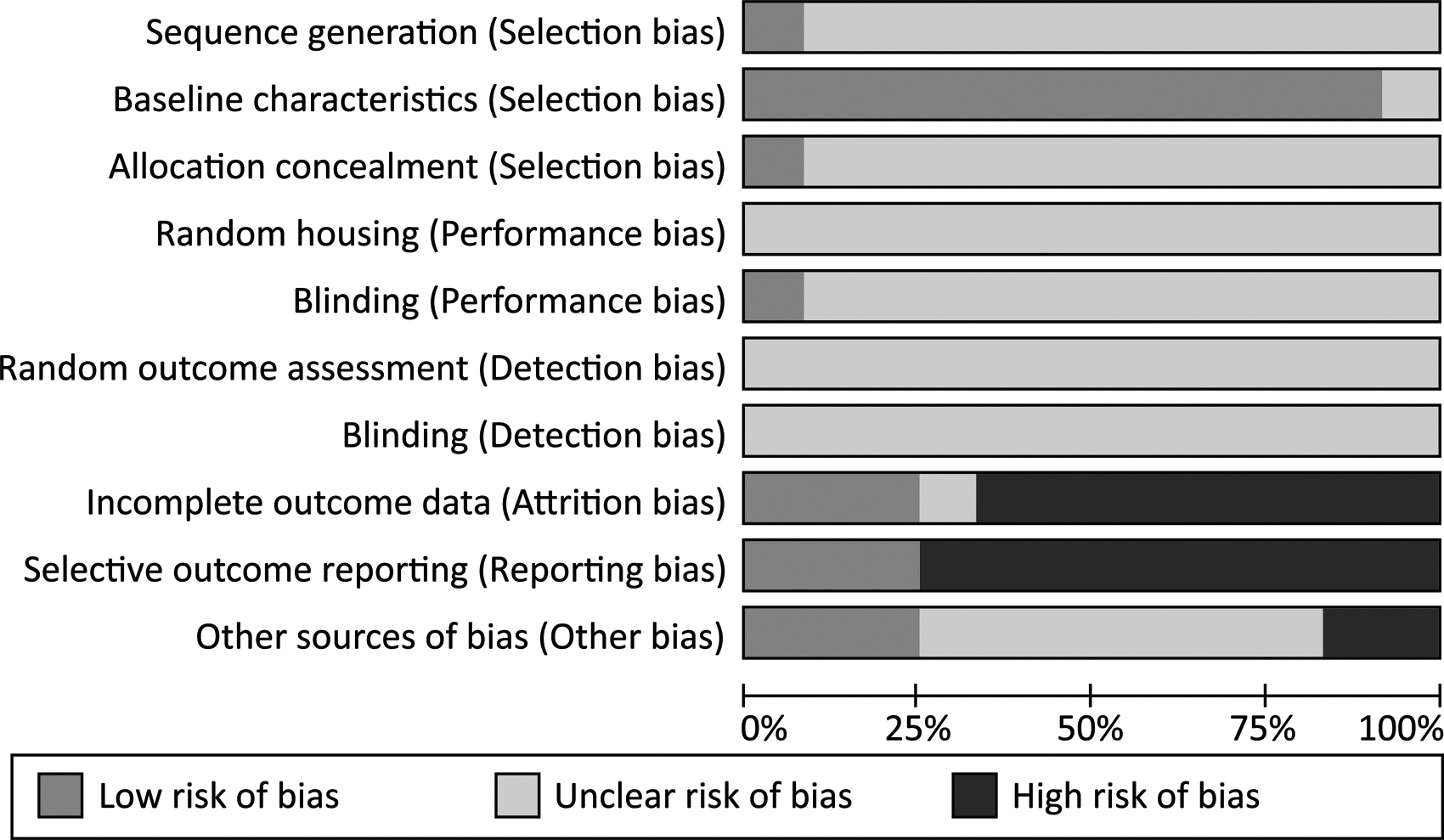
Risk of bias (RoB) graph of included studies evaluated by SYRCLE's RoB tool. Baseline characteristics was the most reported in the included studies (91%) while more than 70% of studies demonstrated selective outcome reporting and no study described random housing, random outcome assessment, and blinding of assessors (detection bias). Each risk of bias item is presented as percentages.
In three studies, attrition bias was not evident 27,29,30 but was present in seven studies (more than 60%) where the number of sample size did not equate to the final number that was analyzed and an explanation was not provided for the missing data. 21,22,24 –26,28,32 One study made no mention of the sample size used or analyzed. 31 Nine studies reported randomization into experimental groups, two studies did not report whether randomization was performed, and only one study (about 9%) actually described sequence generation achieved by a double coin toss. 22
Of the included studies, only one reported allocation concealment, achieved by using an investigator who was not involved in treatment delivery or analysis. 26 The same study was the only one that reported that blinding was achieved by masking treatment bottles with opaque tape. 26 No studies indicated whether outcome assessment was blinded.
While perhaps less critical than the factors discussed above, another potential source of bias identified was potential conflicts of interest from sources of funding or materials; these are important to report because the financial interests of authors could lead to biased interpretation of the data. A total of six studies did not report on whether a potential conflict of interest from sources of funding existed, 21,22,24,27 –29 although two of the six did state that they had no potential conflict of interest but without specifically referring to their source of funding. 22,27 The remaining five studies did declare their sources of funding: two of the five stated that this did not pose a conflict of interest, 25,30 one did not indicate whether the funding created a potential conflict of interest, 31 and two did appear to have a potential conflict of interest because of their funding and material source. 26,32
A modified CAMARADES checklist gave a median quality score of six with scores ranging from four to seven out of 10 (Supplementary Data S6). In this assessment, by definition, all included studies came from peer-reviewed articles and used the appropriate animal models. Nine of the 11 included publications (81%) reported compliance with animal welfare regulations, and six studies (55%) reported whether a potential conflict of interest existed. 22,25 –27,30,32 No study, however, reported blinded induction of injury by the investigator or blinded assessment of outcome measures.
Random group allocation was reported in nine of the 11 included publications. 21,22,24 –28,30,32 Most studies used ketamine alone or in combination with other agents such as xylazine and acepromazine for anesthesia, only three used gaseous anesthetics, 25,29,30 and one used pentobarbital. 31 Two publications described the sample size calculation, 22,26 and two others provided an explanation for excluded animals. 29,30 One study did not have to provide an explanation because there were no excluded animals. 27
Meta-analysis
Overall, there was significant heterogeneity between studies investigating drug efficacy on both brain oedema and neurologic function outcomes, which subgroup analyses accounted for.
Overall effect of treatment on brain edema
Five of the publications used in the meta-analysis assessed the effect of treatment on brain edema. 21,22,24,29,32 The data on therapeutic efficacy of heparins/LMWHs and its derivatives on brain edema was contained within the 27 experimental comparisons (Supplementary Data 5). We limited our analysis, however, to data from the ipsilateral cortex, because it best answers our research questions. The efficacy of treatment on brain edema was evaluated based on 17 comparisons involving a total of 407 animals. Taken together, drug treatment reduced brain edema with an overall estimated effect of -1.69 (95% CI: -2.55, -0.82, p < 0.001, Fig. 3) but with substantial heterogeneity, I2 of 90.46% among studies (Fig. 3).
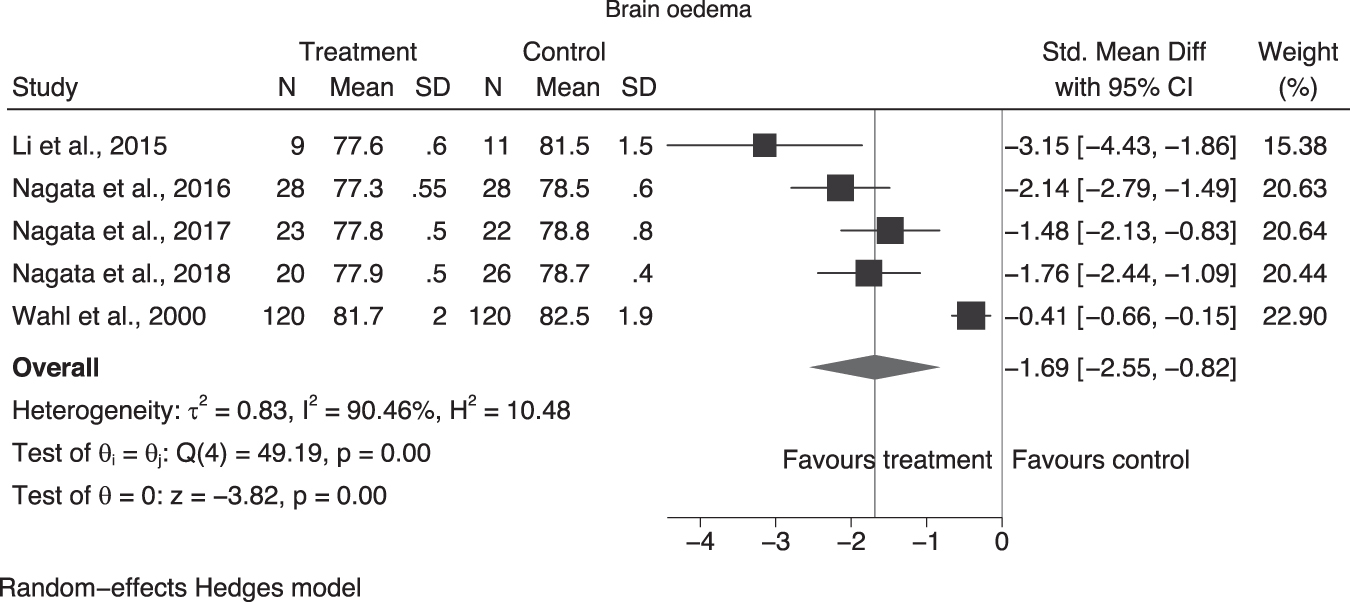
Effect of all treatments on brain edema after trauma. The forest plots represent the pooled analysis of data on the use of heparin and enoxaparin on brain edema. The overall effect estimates favor treatment compared with untreated control (-1.69 (95% cofidence interval [CI]: -2.55, -0.82, p < 0.001). Heterogeneity was significant (I 2 = 90.46%), however. The square symbols and their error bars (95% CI) are the individual studies contributing to the pooled estimates. The central lines and lateral tips of the diamonds indicate the pooled point estimates and the corresponding 95% CIs, respectively. The solid black vertical line indicates the line of no effect while the gray vertical line is the overall effect size line. This annotation is used in all subsequent forest plots. SD, standard deviation.
Effect of heparin and enoxaparin treatment on brain edema
Comparing the two studies that examined the effect of UFH 21,22 with the two that examined enoxaparin 24,29 on brain edema revealed similar point estimates for both (test of group difference, brain edema, p = 0.96, Fig. 4) but the degree of heterogeneity differed markedly (enoxaparin I2 = 94%, UFH I2 = 34.38%).

No difference in drug subgroup analysis on brain edema. For enoxaparin and unfractionated heparin (UFH), the overall effect favored treatment compared with the untreated control for brain edema (-1.67 (95% confidence interval [CI]: -2.78, -0.56; p < 0.001). There was no difference, however, between the effect estimates for the two drugs although heterogeneity differed substantially (I 2 enoxaparin = 93%, I2 UFH = 34.38%). SD, standard deviation.
Effect of different doses of heparin and enoxaparin on brain edema
Segregating the data for enoxaparin and UFH into low and high dose regimes on brain edema suggested a trend toward greater effect for low doses (low dose: -2.40 (95% CI: -3.01, -1.80; high dose: -1.40 (95% CI: -2.42, -0.38); however, no statistical difference between the doses was detected (test of group difference, Qb, 2.76, p = 0.10; Fig. 5). While heterogeneity was not significant in the low dose group (I 2 = 6.55%), it was moderate in the high dose group (I 2 = 60.81%).
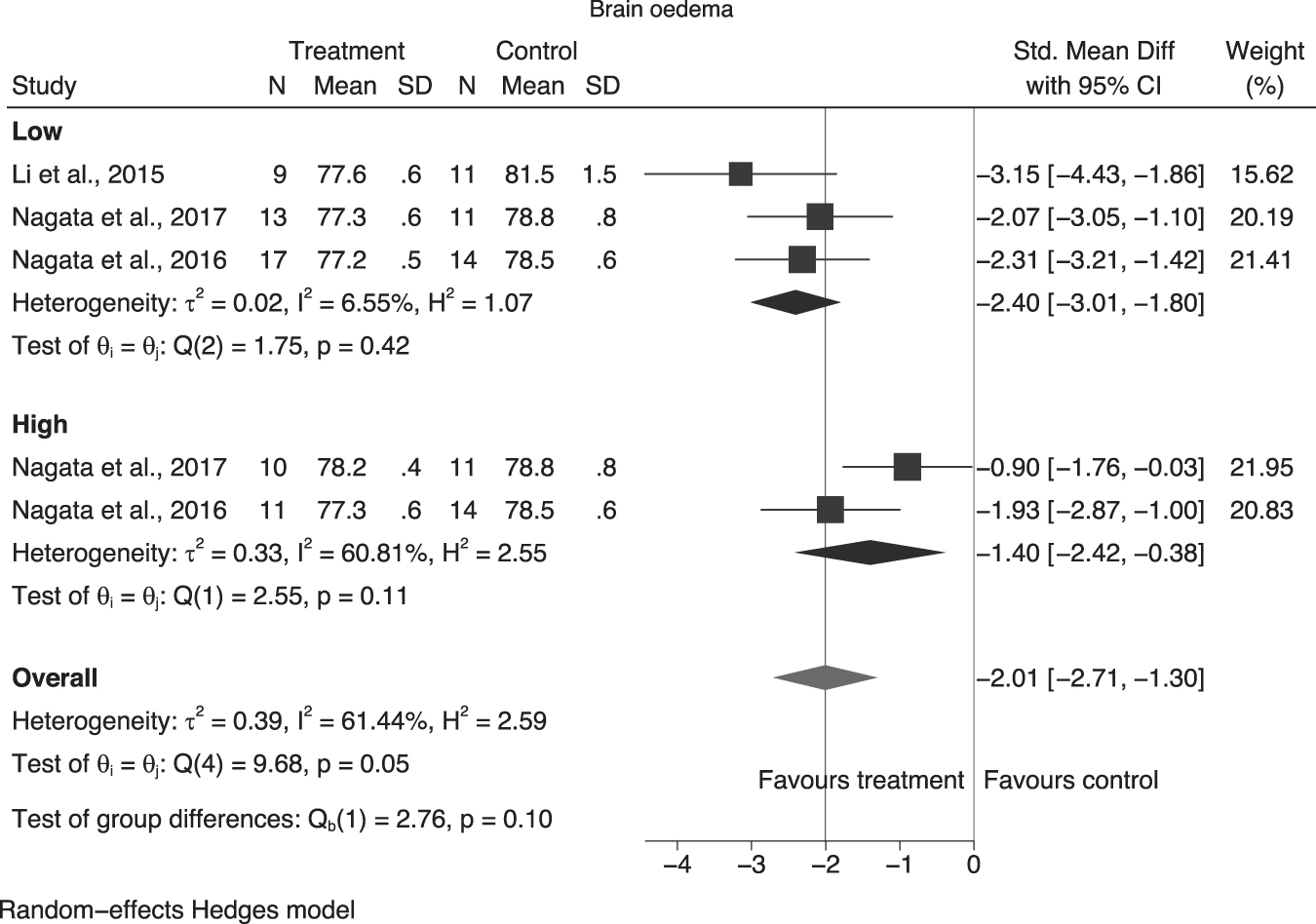
Effect of low and high doses on brain edema after trauma. The drug doses were grouped into either low or high dose regardless of the mode of administration. Overall, the pooled estimate of both doses favored treatment compared with control with a substantial heterogeneity (I 2 = 61.44%). There was no significant difference between the effect of low and high dose on brain edema (p = 0.10). Heterogeneity was moderate in the high dose group (I 2 = 60.81%) and not significant in the low dose group (I 2 = 6.55%). SD, standard deviation.
The study from Wahl and associates, 200029 was excluded from this analysis; we could not categorically group the dose administered as either a low or high dose because the authors used a combination of drug doses at various times. For example, they started with an IV administration of a low dose a few minutes or hours post-injury and afterward with a SC injection of a high dose. Overall, the pooled estimate of both low and high drug doses favored treatment compared with the untreated controls, and the heterogeneity (I 2 = 61.44%) was reduced slightly but remained substantial.
Effect of treatment on neurological function
Four studies assessed neurological function at 24 h and 48 h post-TBI, 21,22,24,32 with one study also including 72 h and 96 h time points, 22 while a fifth study assessed this outcome at weekly intervals for four weeks post-TBI, 29 We selected the 48-h time point data for meta-analysis because it was the longest post-injury interval with the most data. The four studies assessing neurological function at 48 hours post-TBI 21,22,24,32 were evaluated after treatment with heparin and its derivatives based on seven comparisons involving 129 animals. Overall, the pooled adjusted estimated effect of 1.51 (95% CI: 0.31, 2.72, p = 0.01, Fig. 6) favored treatment. There was significant heterogeneity (I 2 = 88.58%), however.
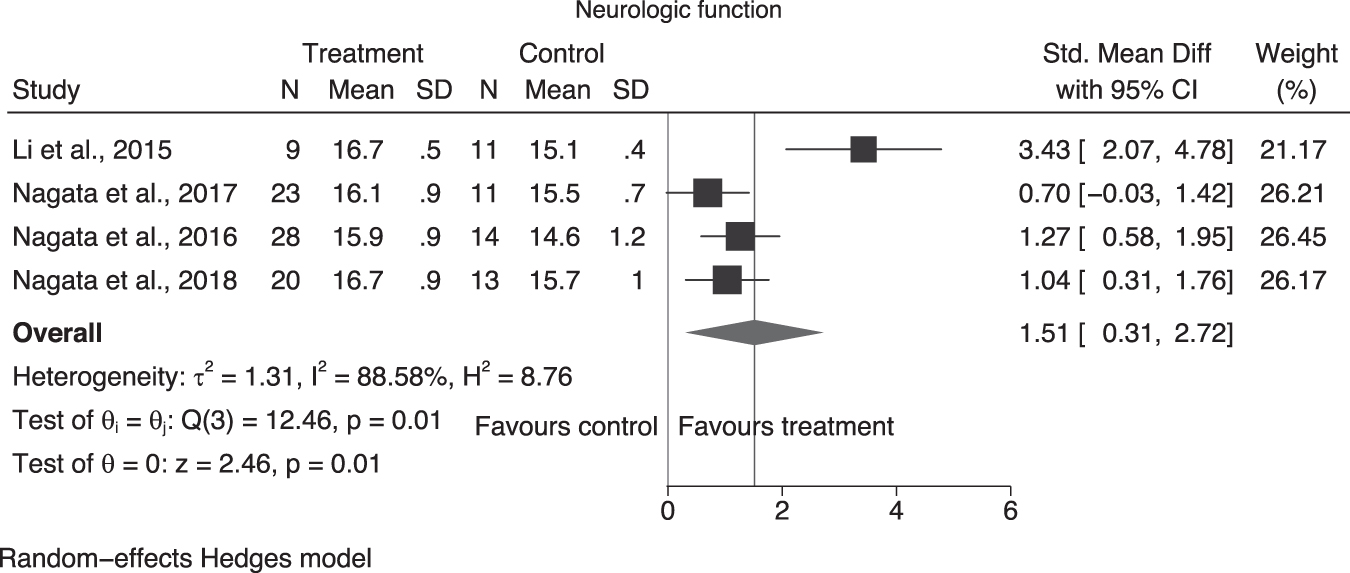
Effect of all treatment on neurological function after trauma. The forest plots represent the pooled analysis of data on the use of heparin and its derivatives on neurological function. The overall effect estimates favor treatment compared with control (1.51 (95% confidence interval [CI]: 0.31, 2.72, p = 0.01). Drug treatment improved neurological function after trauma. Heterogeneity was significant (I 2 = 88.58%), however. The central lines and lateral tips of the diamonds indicate the pooled point estimates and the corresponding 95% CIs, respectively. The solid black vertical line indicates the line of no effect while the gray vertical line is the overall effect size line. SD, standard deviation.
Effect of treatment on hemorrhage/hemorrhagic contusion
Only three studies examined the effect of treatment on bleeding using two different methodologies—detection of red cells/clot on hematoxylin and eosin stain 25,28 and visualization of hemorrhage on the surface of the brain. 24 Based on four comparisons involving 70 animals, together, these studies with a pooled estimate of 0.95 (95% CI: 0.44, 1.46, p = 0.0003, Fig. 7A) found that treatment did not increase bleeding. Heterogeneity was not significant (I 2 = 0%).
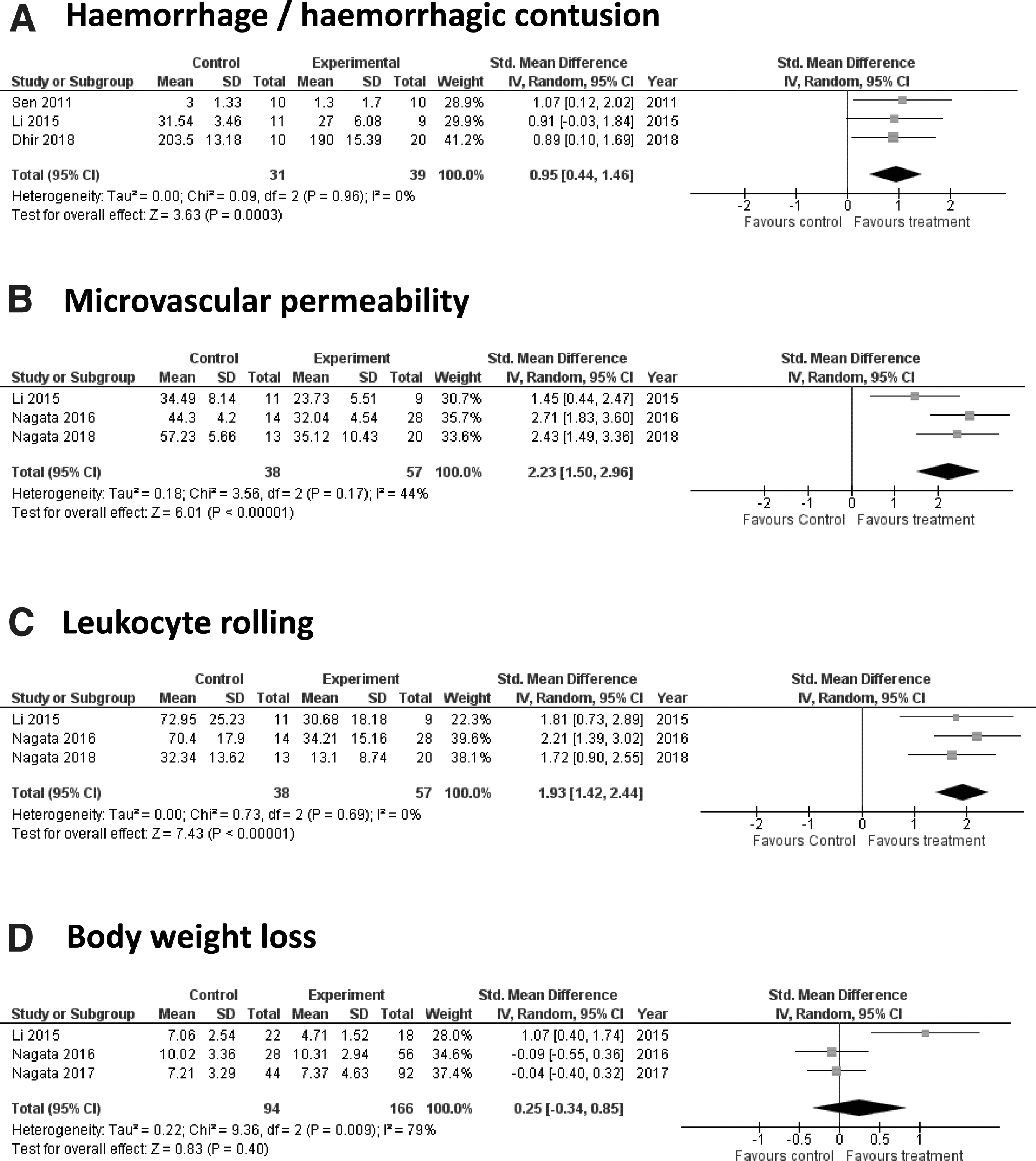
Effect of all treatments on hemorrhage, inflammation, and vascular permeability. Leukocyte rolling and microvascular permeability were decreased after treatment with unfractionated heparin, enoxaparin, and 2,3-O-desulphated heparin. Varying effects of both enoxaparin and unfractionated heparin were observed on body weight loss. Enoxaparin treatment did not increase hemorrhage and treatment. SD, standard deviation; CI, confidence interval.
Effect of treatment on microvascular permeability and inflammation
Three studies, 21,24,32 all in mice involving five comparisons in 95 animals, quantified FITC-labelled albumin fluorescence at 48 h post-TBI. The authors found that enoxaparin, UFH, and ODSH, respectively, improved blood–brain barrier permeability (2.23 (95% CI: 1.50, 2.96, p = 0.00001; I2 = 44%, Fig. 7B). The same three studies (five comparisons involving 95 animals) also reported decreased leukocyte rolling with an overall pooled estimate of 1.93 (95% CI: 1.42, 2.44, p = 0.00001, Fig. 7C) and an insignificant heterogeneity (I 2 = 0%).
Effect of treatment on body weight
When body weight was examined in the same three studies as above, 21,24,32 albeit with 14 comparisons involving 260 animals, treatment with enoxaparin was associated with reduced body weight loss while treatment with either UFH or ODSH was not. Overall, there was no effect of treatment on body weight loss (0.25 (95% CI: -0.34, 0.85), p = 0.40, I2 = 79%, Fig. 7D).
Other variables we had hoped to investigate, including the optimal time at which the drug produced the most effect and the best route of administration, could not be evaluated because of insufficient data.
Potential publication bias
Publication bias was assessed using funnel plot on the overall therapeutic effect of treatment on brain edema and neurological function after trauma. Four studies were evaluated, and we found that there was funnel plot asymmetry for both outcomes, which was confirmed with Egger regression test (brain edema, z = -4.86, p < 0.001; neurological function, z = 3.25, p = 0.0012). Contour-enhanced funnel plot explored funnel plot assymetry at 1%, 5% and 10% (Fig. 8A, 8B) for each outcome, suggesting the possibility of publication bias. This finding, however, should be interpreted with caution because of the low number of studies evaluated.
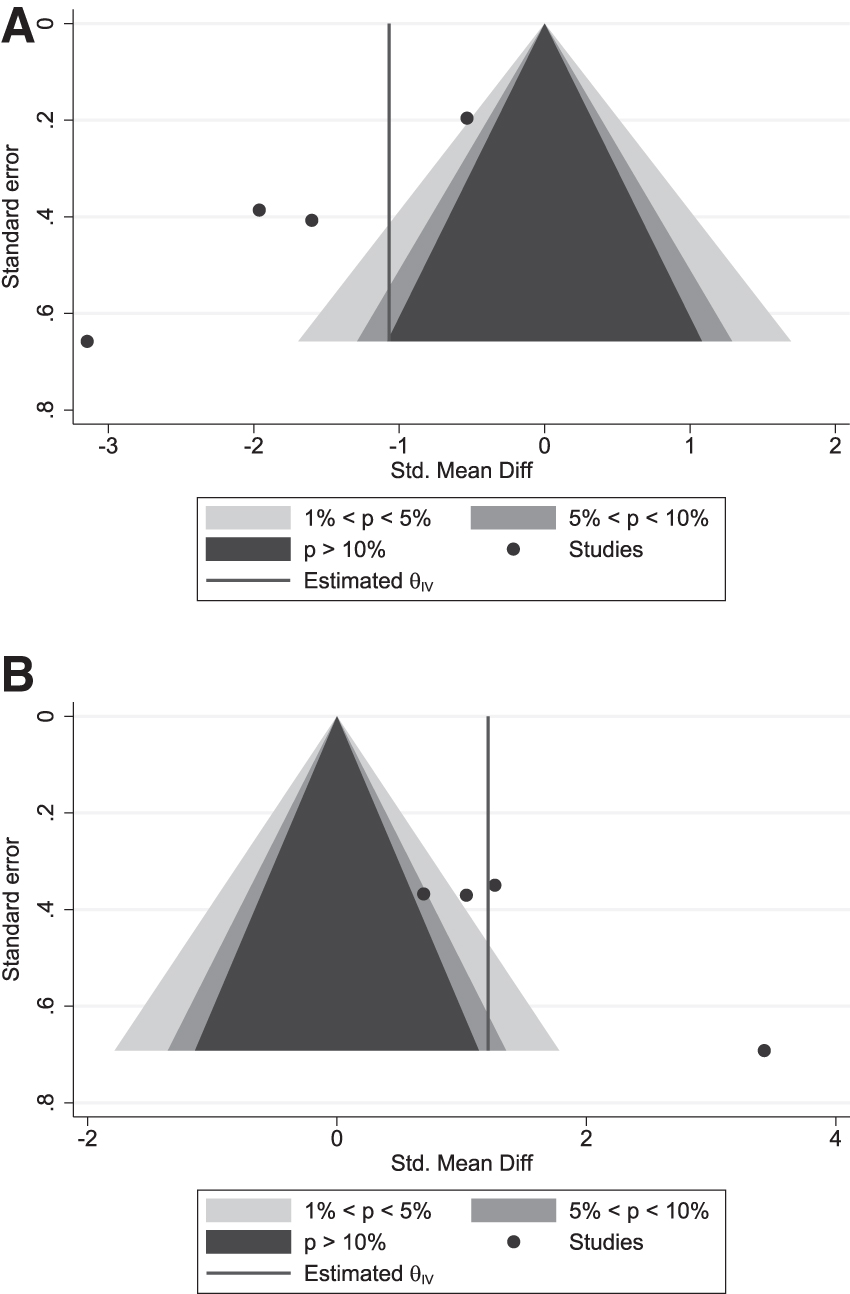
Funnel plot asymmetry in the studies evaluated for brain edema and neurological function after trauma. Contour-enhanced funnel plot assessed at 1%, 5%, and 10% show marked asymmetry in reporting of brain edema (
Discussion
In this review, we have evaluated the pre-clinical data supporting the potential use of heparins/LMWHs as treatments for TBI. To our knowledge, this review is the first to systematically collect and analyze all available evidence in the literature regarding the therapeutic efficacy of heparins and LMWHs in animal models of TBI.
There is a significant body of work examining this potential. We were surprised, however, at the paucity of data suitable for inclusion in a meta-analysis. Indeed, of the 276 publications that appeared relevant on screening, only 11 met our overall eligibility criteria and only seven contained sufficient data for inclusion in meta-analysis. Moreover, within the studies, the injury models and outcome assessments were variable. This is not surprising, because the presentation of TBI with respect to age, sex, site, and nature of injury, severity, and pathophysiology is complex and diverse. 33
The paucity of data is in part because of the strict criteria that are applied to facilitate valid meta-comparisons across sometimes disparate datasets. For example, many articles were the only reports for a particular outcome and could not sensibly be grouped with others for analysis. Also, we were only able to use data from experiments that provided controlled studies (in this case, untreated injured animals) where cohort sizes and outcome data and its variability were provided or could be reliably imputed.
This speaks to the need for coordination across the field, particularly with respect to core standardized analyses 34,37 and better application of current reporting standards such as ARRIVE (Animal Research: Reporting of In Vivo Experiments) 35,36 and the pre-clinical TBI Common Data Elements (CDEs) developed by the National Institute of Neurological Disorders and Stroke, describing experimental parameters and outcome measures. 38,39 These guidelines facilitate reproducible reporting of key variables, which enables the comparison of results between studies. 40
As mentioned above, we were limited in our ability to utilize the analytical power of systematic review 41,42 by the breadth of different analyses performed and the overall paucity of suitable numerical data; this is an important observation for the field and common in pre-clinical analyses 43,44 where exploration of pathobiology is usually combined with evaluation of potential therapeutic efficacy. Nevertheless, these limitations and the meta-analysis itself provide some important additional insights.
Because all the animals used were male (Table 1), we were unable to explore the role of sex on the efficacy of heparins/LMWHs for TBI. This indicates that researchers are ignoring this important facet of human TBI where sex clearly affects outcome, 45,46 the female hormones estrogen and progesterone are known to be neuroprotective, 47 –49 and published guidelines recommend use of both sexes in studies of TBI. 50
We did find studies that analyzed multiple outcomes using multiple model systems as detailed in Tables 1–3. The main themes were that heparin and its derivatives modify lesion size, 27,29 neurological function, 21,22,29,32 brain edema, 21,22,24,32 blood–brain barrier dysfunction, 21,24,32 neuroinflammation, 21,22,24,26,28,30 –32 a variety of mechanisms of cell death, 26 –28,30 the pathobiology of bleeding in the face of heparin-based drug treatments, 22,24,25,28 and a range of other markers of injury such as oxidative stress. 30 Here, we first summarize the main findings from the individual articles and report the meta-analysis of components of these data.
Increased lesion volume after TBI, whether because of ischemic or other secondary changes, is associated with unfavorable outcomes. 51,52 Of the studies included in this review, only two studying the effects of enoxaparin explicitly examined lesion volume. One reported that high dose enoxaparin (10 mg/kg IP) decreased lesion volume, 27 but the other found no effect at high doses (0.5 mg/kg IV + 4 × 2 mg/kg SC) and detected a decrease at low doses (0.5 mg/kg IV + 4 × 1 mg/kg SC). 29 These differences might be a consequence of the different models and species used—cold-induced TBI in mice for the former 27 and fluid percussion in rats for the later. 29 Unfortunately, there were insufficient data to explore this by meta-analysis.
Poor neurological function, as a consequence of both the initial lesion and subsequent damaging changes, is perhaps the most critical consequence of TBI. 53,54 The studies reported here that examined enoxaparin, UFH, and ODSH all improved neurological function and enhanced recovery up to four weeks post-TBI. 21,22,29,32 Motor and cognitive function were also reported to be improved by ODSH 32 and enoxaparin. 29
Brain edema, which is a common pathology in TBI, could worsen outcomes by increasing intracranial pressure causing secondary ischemia and reducing cerebral perfusion and tissue oxygenation. 55,56 The studies we assessed reported that enoxaparin, UFH, and ODSH all decreased brain edema after experimental TBI. 21,22,24,29 The effect of dosing in these studies is unclear. Low dose enoxaparin 24 and both low and high dose UFH 21,22 but only high dose ODSH 32 were reported to reduce edema. In related studies in photothrombotic stroke, only higher doses of enoxaparin are reported to improve cerebral edema. 10 These edema outcomes are discussed further in the meta-analysis section below.
One contributor to brain edema and worse TBI outcome is damage to the blood–brain barrier, the complex structure that controls the movement of nutrients, proteins, and immune cells among others in and out of the brain. 57 Assessed here as microvascular permeability, enoxaparin, UFH, and ODSH all reduced blood–brain barrier leakage in the controlled cortical impact model at 48 h post-TBI irrespective of the drug dose, mode of delivery, or drug type. 21,24,32
Overall, our meta-analysis suggests that UFH and enoxaparin do appear to reduce brain edema (Fig. 3) and improve neurological function (Fig. 6) in animal models of TBI. Moreover, it appears that enoxaparin and UFH provided very similar effects, albeit with considerable differences in experimental heterogeneity, which we cannot currently explain (Fig. 4). Intriguingly, there was a trend suggesting that lower doses (0.75 mg/kg minimum, not greater than 1 mg/kg) might be more effective than higher doses (≥2 mg/kg) (Fig. 5).
As an additional note of caution, however, heterogeneity in the two high dose studies was high despite coming from the same research team and employing very similar methodologies including animal species, mode of drug delivery, and dose of drug. 21,22 Conversely, heterogeneity was very low between the low dose studies. 21,22,24
The studies included in this review did not report an increase in hemorrhage after the administration of enoxaparin post-trauma 22,24,25,28 ; indeed the meta-analysis (Fig. 7A) would appear to suggest that the treatment improved hemorrhagic outcome, suggesting that drugs like enoxaparin may be relatively safe. This suggestion, however, has to be weighed against the risk of clinically significant bleeding complications because early use of drugs with anti-coagulant properties 11,58 might be expected to worsen outcome by increasing intracranial/cerebral hemorrhage, which is commonly observed after TBI. 59 It should be noted, however, that the early administration of enoxaparin in patients with severe TBI did not show significant increase in cerebral hemorrhage in a human clinical trial. 60
Neuroinflammation is a critical secondary injury mechanism that interacts with blood–brain barrier damage after TBI, contributing to ongoing neuronal damage and death. 61,62 It encompasses infiltration of peripheral immune cells into the brain, increased circulating and brain concentrations of inflammatory mediators, and consequent astrogliosis and microgliosis. 61,63 In related models of subarachnoid hemorrhage, heparin is reported to reduce microglial activation and expression of the inflammatory cytokines, tumor necrosis factor-α and IL-1β. 64
Eight of our included studies together investigated the effect of UFH, ODSH, and enoxaparin on leukocyte rolling, leukocyte adhesion, PMN cell sequestration, pro-IL-1β, COX-2 expression, reactive gliosis, and glial scar formation after experimental TBI. 21,22,24,26,28,30 –32 Overall, these inflammatory outcomes were improved by heparin, 21,22,31 enoxaparin, 24,26,28,30 and ODSH 32 regardless of dose. There were no effects reported on leukocyte adhesion, 21,32 pro-IL-1β concentration, 30 or astrogliosis, however. 30 While most of these parameters provided insufficient data for meta-analysis, three studies that examined both vascular permeability and leukocyte rolling did provide evidence for a consistent beneficial effect (Fig. 7B, 7C).
In the studies evaluated here, reduced apoptosis was reported in response to enoxaparin. 27,28,30 One study compared between doses and actually demonstrated that the decrease observed was dose-dependent. 27 Similarly, enoxaparin also decreased the expression of inflammasome proteins IL-1β and caspase-1. 26 There were insufficient data to examine this by meta-analysis.
Oxidative stress is one of many other important contributors to the pathophysiology of TBI that were investigated in the studies we reviewed. In TBI, markers of oxidative stress such as thiobarbituric acid-reactive substances (TBARS) are increased in the brain while antioxidant defence enzymes such as superoxide dismutase and glutathione are reduced. 65 –67
The studies we report that examined the effects of enoxaparin on oxidative stress found decreased concentrations of TBARS and oxidized proteins in the hippocampus in the lateral fluid percussion injury rat model of TBI at 48 h after injury, 30 while serum levels of “total antioxidant status” were increased after administration of high dose enoxaparin in a cold-induced TBI model. 27 It remains to be seen whether antioxidant actions are important contributors to the effects of heparins/LMWHs overall.
We had originally pre-planned for the possibility of a range of subgroup analyses (PROSPERO; CRD42020205574; e.g., drug type, mode of drug administration, drug dose, sex of animal, animal species, timing, and frequency of treatment) to explore the factors that contributed to experimental heterogeneity. Most proved impractical to analyze effectively, and some could not be analyzed at all. For example, many injury models were used but none sufficiently often to allow comparison.
Controlled cortical impact producing a severe TBI was the most common way to induce TBI. 21,22,24,26,32 Similarly, multiple routes of drug delivery were used, including within studies, 28,29 all with apparent benefit. No study, however, provided data indicating that any route of delivery was to be preferred, and we found that insufficient data were available for meta-analysis to provide guidance for this important practical question. 68,69 Similarly, the timing of treatment was also considered important but not possible to analyze.
The potential for bias is another reason for caution. While systematic review and meta-analysis are important tools for finding, aggregating, and helping interpret data, 70 –72 it must be remembered that if the input data are biased, the output data will also be influenced by this bias. While we have endeavored to not do so, it is also possible for introduction of bias during the process of systematic review and meta-analysis. 73 –75
Overall, the studies we were able to find were generally of low quality (median four of 10) based on the modified checklist from CAMARADES. 16,17 Despite having been subjected to peer review, there were notable absences of data reporting: for example, whether measures such as blinding had been taken to help avoid the introduction of bias. These absences are particularly well highlighted by use of the SYRCLE Risk of Bias tool (Fig. 2). Sadly, this finding is consistent with the analyses of the use of these measures across in vivo pre-clinical research 76 where such absences are associated with inflated effect sizes. 77,78
It was reassuring to discover, however, that random allocation into groups was very well reported by virtually all the studies included in this review. Funnel plots asymmetry and Egger regression, albeit based on a small sample size (Fig. 8), also indicates the possibility of publication bias or some other source of asymmetry in these data. 79,80 Debray and colleagues, 81 however, have suggested that funnel plot should be avoided for reviews with few studies because it could be unreliable.
The search for a treatment in TBI is a truly long and challenging one. Despite demonstrating efficacy in pre-clinical studies, several potential therapeutic agents such as progesterone 82 failed to achieve clinically meaningful primary end points in large scale phase III clinical trials. Improved clinical methodology, such as selection of patients and adaptive Bayesian phase II trials, have been suggested as some of the key factors to be considered for future trials. 83
In addition to optimizing clinical trial designs, robust pre-clinical data on pharmacokinetics-pharmacodynamic (PKPD) of a therapeutic candidate, in this case, heparins/LMWHs, to support the design of later clinical trials are needed. Although being used clinically in many disorders, the understanding of the PKPD relationship of the heparins/LMWHs in the context of neuroinflammation and neurological injuries is still insufficient. 84 Future investigations to capture these data will provide better insights on the function and effects of heparins/LMWHs, including where and how they act, whether they cross the blood–brain barrier, dose-response relationship, risk/benefit ratio at different doses, as well as optimization of time and route of administration.
Limitations
To our knowledge, this is the first systematic review and meta-analysis investigating the therapeutic effects of heparins and LMWHs in animal models of TBI. The study has important limitations, especially with respect to the small sample size available and presence of substantial heterogeneity, and more than 50% of the studies included for meta-analysis coming from one research group. 21,22,24,32 Further, we found that there are insufficient data to evaluate the experimental variables we had hoped to investigate, including dose, timing, and route of administration, as well as the relative efficacy of heparins and LMWHs on different TBI outcomes.
Despite these shortcomings, we have identified that across the 11 studies included in our review, treatment with UFH, enoxaparin, and/or ODSH shows consistent beneficial effects, including decreased cerebral edema, inflammation, microvascular permeability, recruitment and accumulation of leukocytes, apoptosis, and brain contusion volume, and improved neurological function. These pharmacological outcomes were elicited using different dosing regimens and different rodent models of TBI, demonstrating a robustness to these findings that suggests further pre-clinical studies are warranted.
Our review highlights areas where more work needs to be done, such as comparing alternate dosing regimens within single studies, because the effect of dosing remains unclear. Also, while assessing a variety of outcome measures will be important to elucidate the range of therapeutic effects of heparins and LMWHs, it would be valuable for future studies to also include analyses of key TBI outcomes, such as those identified by the Operation Brain Trauma Therapy consortium 37 to facilitate the comparison of therapeutic efficacy across different studies. Finally, the possibility of publication bias that we've identified speaks to the need for publishing negative results to prevent the exaggeration of beneficial findings.
Conclusion
Overall, in this review, we found that heparins and LMWHs, including UFH, ODSH, and enoxaparin, appeared to improve outcome after TBI with no increased hemorrhage. With enoxaparin's better bioavailability profile, more predictable dose-response relationship, longer half-life, less anti-IIa (thrombin) activity, and half the anti-Xa (prothrombinase) activity than heparin, 10,85 it may have advantages for clinical use. The inferences made above, however, are based on a very limited number of animal studies, and therefore these findings must be interpreted with caution. Nevertheless, there is a clear need for more detailed pre-clinical studies to evaluate the therapeutic potential of heparins and LMWHs as a treatment for TBI.
Footnotes
Acknowledgments
We would like to thank the University of Tasmania research librarian, Michaela Venn for her assistance in developing the final search strategy. Mimieveshiofuo Aiyede was supported by an Australian Government Research Training Program (RTP) Stipend and RTP Fee-offset Scholarship through the University of Tasmania.
Authors' Contributions
MA and NB devised and coordinated the study. MA, DWH, and NB developed the search strategy and registered the protocol. MA and XYL reviewed the studies and extracted data. MA and AAMR designed the statistical analysis, and MA conducted the risk of bias assessments and statistical analysis. MA, DWH and NB performed the data interpretation. MA drafted the manuscript. MA, XYL, AMR, RPP, NG, DWH and NB helped to revise the manuscript. All authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.