
Abstract
The main treatment strategy for chronic subdural hematoma is surgical intervention. When a conservative pharmacological approach is considered in symptomatic patients, mainly dexamethasone therapy is applied. Recent trials revealed dexamethasone therapy to be an ineffective treatment in symptomatic patients with chronic subdural hematoma. Whether the efficacy of dexamethasone therapy differs in radiological hematoma subtypes is unknown. The aim of this substudy was to identify which hematoma subtype might be favorable for dexamethasone therapy. As part of a randomized controlled trial, symptomatic chronic subdural hematoma patients received 19-days dexamethasone therapy. The primary outcome measure was the change in hematoma size as measured on follow-up computed tomography (CT) after 2 weeks of dexamethasone in six hematoma (architectural and density) subtypes: homogeneous total, laminar, separated and trabecular architecture types, and hematoma without hyperdense components (homogeneous hypodense, isodense) and with hyperdense components (homogeneous hyperdense, mixed density). We analyzed hematoma thickness, midline shift, and volume using multi-variable linear regression adjusting for age, sex and baseline value of the specific radiological parameter. From September 2016 until February 2021, 85 patients were included with a total of 114 chronic subdural hematoma. The mean age was 76 years and 25% were women. Larger decrease in hematoma thickness and midline shift was revealed in hematoma without hyperdense components compared with hematoma with hyperdense components (adjusted [adj.] b -2.2 mm, 95% confidence interval [CI] -4.1 to -0.3 and adj. b -1.3 mm, 95% CI -2.7 to 0.0 respectively). Additional surgery was performed in 57% of patients with the highest observed rate (81%) in separated hematoma. Largest hematoma reduction and better clinical improvement was observed in chronic subdural hematoma without hyperdense components after dexamethasone therapy. Evaluation of these parameters can be part of an individualized treatment strategy.
Introduction
Chronic subdural hematoma is a frequently encountered neurological and neurosurgical disease with an increasing prevalence in the elderly. 1 -3 The preceding event is generally a head trauma with a higher risk of chronic subdural hematoma development in patients using antithrombotic therapy compared with patients without this therapy. 4,5 The diagnosis is established with computed tomography (CT), which reveals a crescent shaped fluid collection in the subdural space with a hematoma density that varies from hypodense to slightly hyperdense relative to adjacent brain parenchyma. 6 Hematoma density appearance on CT reflects the chronicity of the hemorrhagic degradation products, with hypodense areas representing hematoma of older age and hyperdense components more recent or active bleeding. 7 -9 In addition, CT architecture types have been proposed to describe the natural development of chronic subdural hematoma from a homogeneous type, into a laminar, then separated type, and finally absorbed as a trabecular hematoma. 10
The main treatment strategy of chronic subdural hematoma consists of surgical evacuation through burr-hole craniostomy, which provides an immediate relief of pressure on the ipsilateral hemisphere, resulting in a fast neurological improvement. 11 Surgical treatment is indicated in symptomatic patients with impeding, progressive, or severe neurological symptoms.
A conservative observational approach is generally considered in asymptomatic patients or patients with mild symptoms such as headache only. Conservative pharmacological strategies, however, are also proposed as monotherapy in symptomatic patients in an attempt to avoid surgery and as adjunctive therapy to surgery to lower the post-operative recurrence risk of 2-33%. 12 –24 The main target of these nonsurgical strategies is the postulated inflammatory response in the subdural space, which could be responsible for hematoma persistence and enlargement. 25 –28
In current literature, most research has been performed with the corticosteroid dexamethasone in symptomatic patients. The implementation of dexamethasone, however, is highly variable in daily clinical practice and based on expert opinion. Depending on the extent of clinical and radiological improvement during the first days to weeks, the treating physician decides whether the dexamethasone (tapering) scheme can be safely completed or additional surgery is required to achieve good recovery. Potential dexamethasone-related side effects, such as cognitive or behavioral disturbances or hyperglycemia, can also hamper treatment. In addition, a pharmacological approach usually requires an intensive clinical and radiological follow-up to assess whether sufficient improvement is achieved and if additional surgery is still required. Clarity on the effectiveness of dexamethasone therapy is therefore of great clinical importance.
Recent randomized controlled trials (RCTs) revealed poorer effect of dexamethasone therapy on functional outcome compared with surgery in symptomatic patients (IP Miah, Dexamethasone versus surgery for chronic subdural hematoma, DECSA-trial: a randomized controlled trial, 2022, in submission). 29 A proportion of patients in the Dexamethasone therapy versus surgery for chronic subdural hematoma (DECSA) trial (39%) did achieve a favorable functional outcome on dexamethasone monotherapy. In surgical studies, higher recurrence rates and poorer functional outcome in chronic subdural hematoma with hyperdense components or a separated or laminar architecture type have been identified. 30 The response of specific chronic subdural hematoma subtypes to dexamethasone monotherapy has not been investigated. Theoretically, the response to dexamethasone therapy could be different in light of the inflammatory pathogenesis hypothesis with radiological subtypes reflecting a different hematoma age and stage of inflammation. Little is known about the radiological and associated clinical short-term effects of initial dexamethasone therapy. This information, however, is essential in defining subsequent treatment.
The aim of this study is to identify which radiological chronic subdural hematoma subtype is most responsive to dexamethasone therapy as evaluated on CT and whether this subsequently contributes to clinical improvement. The present radiological evaluation is a post hoc analysis of the DECSA trial.
Methods
Study design and population
This study is part of the recently completed multi-center RCT DECSA trial. 31 Participating centers in this substudy were three Dutch neurotrauma centers: Haaglanden Medical Center The Hague, Haga Teaching Hospital The Hague, and Leiden University Medical Center. Symptomatic chronic subdural hematoma patients with a symptom severity score of 1 (headache only, mild neurological deficit such as reflex asymmetry), 2 (patient drowsy or disoriented with focal neurological deficits), or 3 (severe focal deficit with impaired consciousness) on the Markwalder Grading Scale, were eligible for inclusion. 32 Patients with a Markwalder Grading Scale score 0 (asymptomatic) and 4 (comatose) were excluded. In addition to the inclusion and exclusion criteria of the DECSA-trial, patients were eligible if a baseline CT was present and patients received dexamethasone treatment after randomization. 31
Study treatment
Dexamethasone therapy, combined with a proton-pump inhibitor (pantoprazole 40 mg daily), was administered twice daily in a daily dosage of 16 mg on Days 1 to 4, 8 mg on Days 5-7, 4 mg on Days 8-10, 2 mg on Days 11-13, 1 mg on Days 14-16, 0.5 mg on Days 17-19, and stopped at Day 20, resulting in a total amount of 110.5 mg dexamethasone. Dexamethasone therapy was discontinued for the following reasons: 1) insufficient improvement of neurological condition 2 weeks after initiation of dexamethasone therapy with unchanged or increased hematoma on follow-up cranial CT; 2) clinical deterioration observed by neurological examination at any time; 3) the occurrence of severe dexamethasone-related side effects or complications; and 4) pre-term discontinuation of dexamethasone treatment left to the discretion of the treating physician when severe clinical condition with relevant comorbidities interfered with recovery. In the latter group, additional surgery was then deemed to be beneficial and the safest option for patient recovery. At the primary follow-up at 2 weeks, a follow-up CT and neurological examination was performed to evaluate the radiological and clinical change in order to decide whether additional surgery by burr hole craniostomy was deemed necessary.
Study procedures and data collection
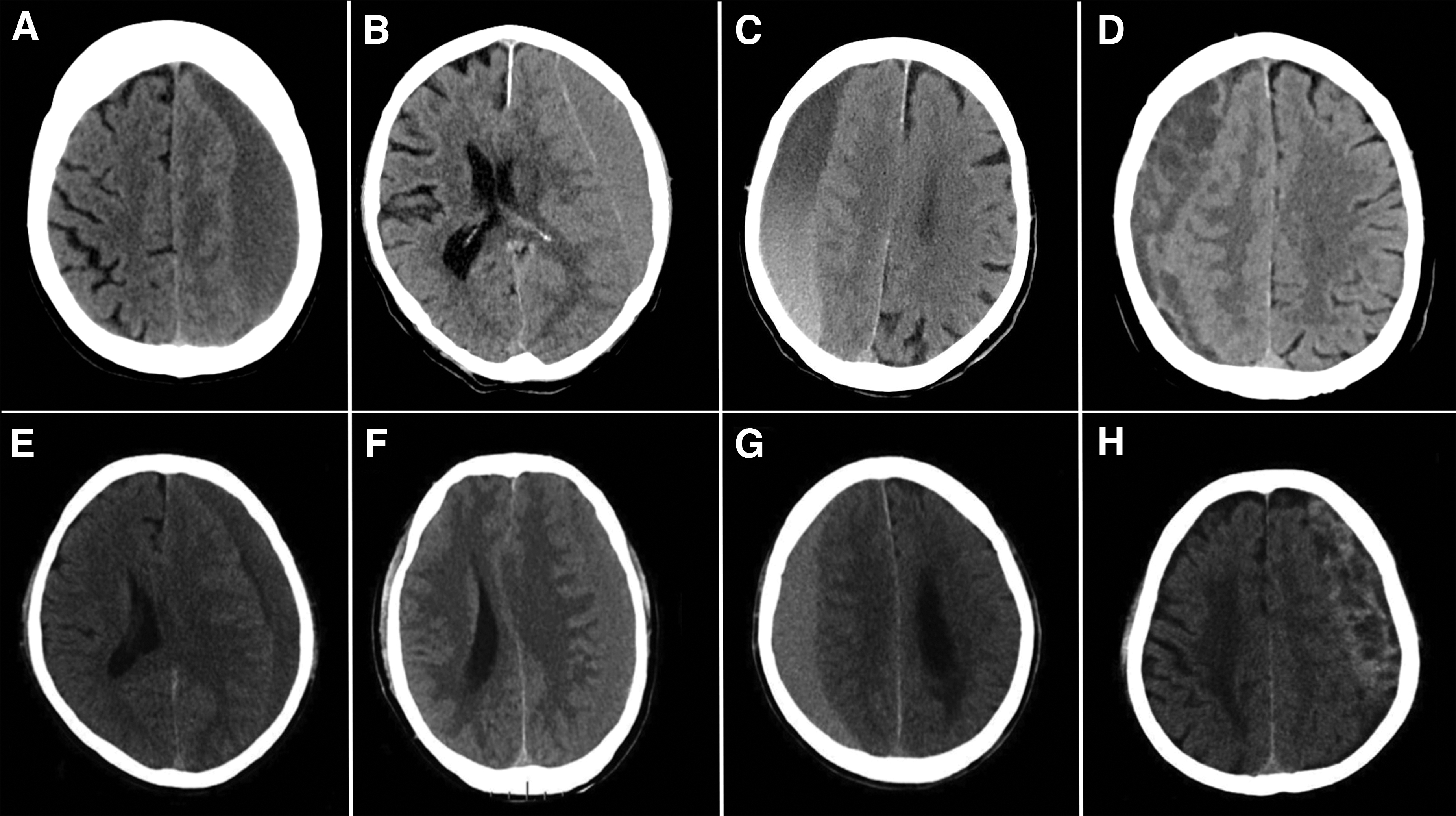
For this substudy, patients were evaluated at presentation, during admission, discharge, and at 2 weeks (or last day of dexamethasone monotherapy, whichever came first) from randomization combined with follow-up CT at 2 weeks. If dexamethasone therapy was prematurely terminated, the last day of dexamethasone treatment with corresponding follow-up CT was maintained as primary follow-up evaluation. The following radiological parameters at diagnosis and follow-up were assessed: hematoma laterality, hematoma architecture and density type, hematoma size by measurement of hematoma thickness, midline shift and volume. Hematoma volume was measured using the ABC/2 formula. 33 Hematoma architecture subtypes were reported using the architectural classification as described by Nakaguchi: (A) homogeneous total, (B) laminar, (C) separated, and (D) trabecular (Fig. 1). 10 Hematoma density subtypes were categorized as hematoma without hyperdense components including (E) homogeneous hypodense (< 30 HU) and (F) isodense hematoma (30-40 HU) and hematoma with hyperdense components consisting of (G) homogeneous hyperdense (40-50 HU), and (H) mixed density hematoma (Fig. 1). 34 -36
Radiological hematoma subtypes by architecture and density
Radiological parameters were assessed by one vascular neurologist (IPM) and emergency radiologist (YT) independently. Inter-observer agreement was calculated for the density and architecture type analyses using Cohen's kappa. In case of disagreements, consensus was reached. Neurological outcome at primary follow-up evaluation was assessed by neurological examination combined with the Markwalder Grading Scale score and subsequently scored into three categories after comparison to neurological function at presentation: 1) no change, 2) improvement, and 3) deterioration. Based on the extent of clinical and radiological improvement, the need for additional surgery was determined by the treating physician.
Additionally, the modified Rankin Scale score was assessed at primary follow-up. Occurrence of dexamethasone-related side effects or complications was assessed during hospital admission and at the 2-week follow-up evaluation by the treating physician. The study protocol was approved prior to data collection by the local Medical Ethics Committee (METC Zuid West Holland, No. 16-024). Ethics review criteria conformed to the Helsinki declaration. Written informed consent was obtained from all patients or by next of kin when neurological symptoms impaired the patient to provide written informed consent. 31 Study data were processed in a clinical trial management system (Castor EDC, Amsterdam, the Netherlands).
Study outcomes
Primary outcome was to identify which chronic subdural hematoma subtype was the most responsive to dexamethasone therapy at the primary evaluation moment of dexamethasone therapy at 2 weeks, by examining the change in the following radiological parameters: hematoma thickness (mm), midline shift (mm), and hematoma volume (mL).
Secondary outcome measures were change in neurological function, symptom severity (Markwalder Grading Scale score) and functional outcome (modified Rankin Scale score) at the primary follow-up evaluation at 2 weeks, clinical onset of improvement on dexamethasone (days), number of patients requiring additional surgery (dexamethasone failure), and dexamethasone-related complications or side effects.
Statistical analysis
Summaries using appropriate descriptive statistics were provided for all clinical and radiological variables, including demographic and baseline characteristics. In addition to the summary data in tables, graphical presentations of summary data were provided when indicated using SPSS 27.0 (IBM Corporation, New York) and GraphPad Prism 8.0 (GraphPad Software, San Diego, California USA). Multi-variable linear regression analysis was performed to evaluate the change in primary radiological outcome (regression coefficient, b) in each hematoma architecture subtype (A-D) as well as combined density subtypes indicating hematoma without (type E, F) and with (type G, H) hyperdense components. All regression analyses were conducted, with adjustment for age, sex and baseline value of the specific radiological parameter assessed. Regression analysis of the primary (radiological) outcome was performed in all chronic subdural hematoma (unilateral and bilateral combined). Regression analysis regarding (the change in) secondary clinical parameters in relation to hematoma subtype and change in hematoma size (hematoma thickness, midline shift, hematoma volume), were assessed by evaluating the hematoma on the symptomatic side in bilateral chronic subdural hematoma since this side contributed to the symptoms. If the symptomatic side was unknown, the side that caused midline shift, thus contributing the most to the clinical condition, was used for analysis. A p value of less than 0.05 was used to indicate statistical significance.
Results
Baseline
In total, 180 patients were screened for this study (Fig. 2). Of these, 85 patients fulfilled the study criteria and could be included during the entire study period of the DECSA-trial from September 2016 until February 2021 (Table 1). The mean age was 76 years (SD ±11), with 21 female patients (25%). Antithrombotic therapy was used in 50 patients (59%) and discontinued immediately at diagnosis in all patients. Symptom severity at diagnosis was Markwalder Grading Scale score 1 in 12 (14%) and Markwalder Grading Scale score 2 in 73 (86%) patients. A total of 114 chronic subdural hematomata were assessed of which 56 were unilateral (Table 1). Of the hematoma architectural subtypes, 56 were homogeneous, eight laminar, 20 separated, and 30 trabecular. Density type classification showed 37 hematomas without hyperdense components and 77 hematomas with hyperdense components (Table 1). For the four architectural subtype classification substantial agreement was reached between both raters (kappa 0.768). Interobserver agreement was excellent for the dichotomized density subtypes (kappa 0.928). Consensus was reached for all hematoma.
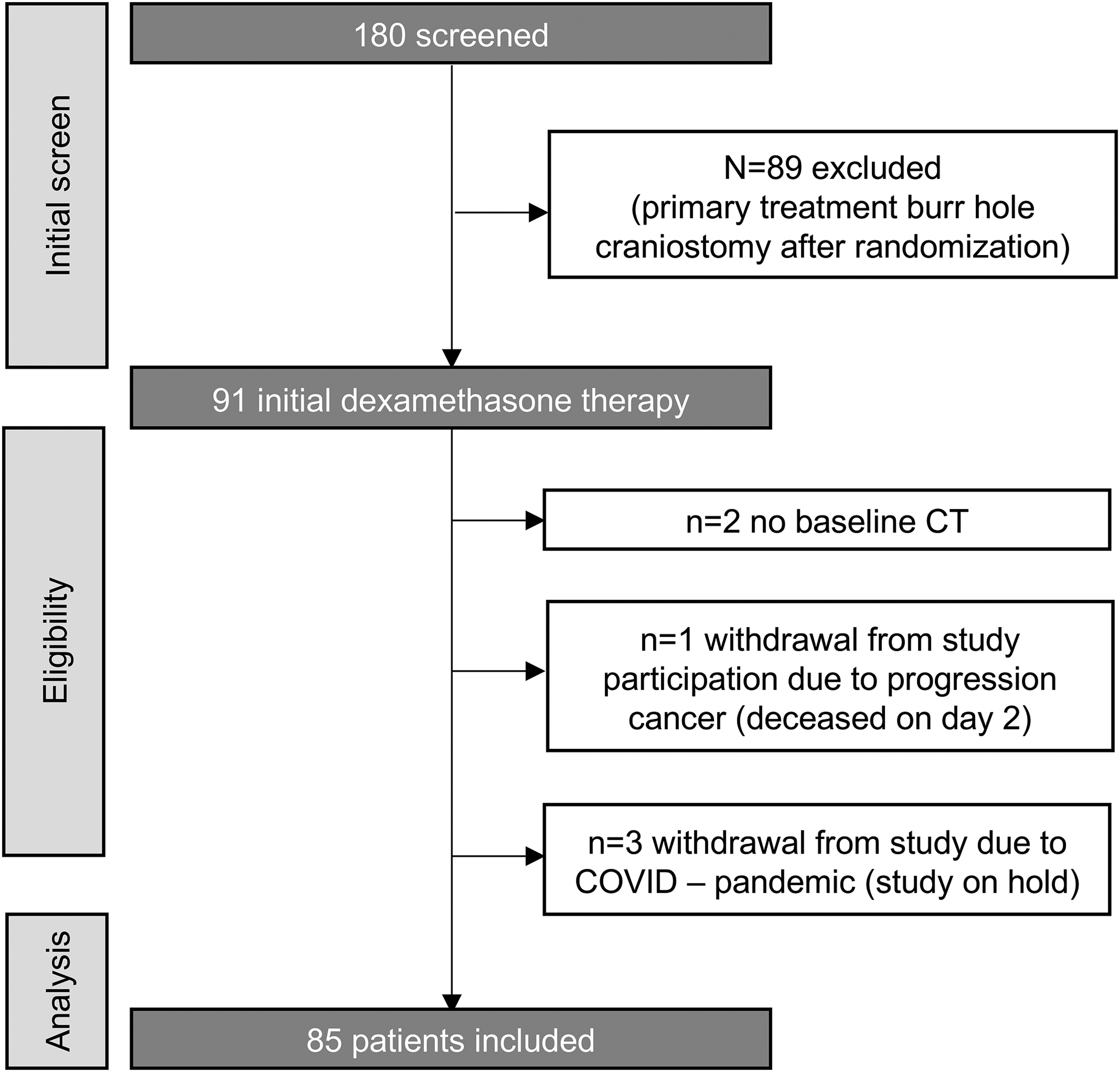
CONSORT (CONsolidated Standards of Reporting Trials) flowchart of patient inclusion.
Baseline Characteristics per Hematoma Subtype
due to rounding, sum of percentages might not add up to 100.
SD, standard deviation; F, female; MGS, Markwalder Grading Scale score.
Follow-up
Median time to primary follow-up evaluation was 15 days (1-86 range, interquartile range [IQR] 12-18). Due to clinical deterioration, earlier evaluation was performed within 7 days in 10 patients (12%). One patient with good recovery (Markwalder Grading Scale score 0) did not manage to appear at follow-up evaluation (with CT) on Day 14, but on Day 86. Dexamethasone treatment schedule of 19-days was completed in 50 (59%) patients, and terminated earlier in 35 (41%) patients when the clinical situation prompted for additional surgery (Table 2). Median administered dexamethasone dose was 103 mg (IQR 100-111).
Clinical Outcome at Primary Follow-Up per Hematoma Subtype (Two Weeks)
Due to rounding percentages might not add up to 100.
DXM, dexamethasone; IQR, interquartile range; MGS, Markwalder Grading Scale score; n.a., not available.
Radiological hematoma evolution
At follow-up, five of the 114 chronic subdural hematoma showed complete hematoma resolution. Overall change in hematoma thickness, midline shift and volume after 2 weeks of dexamethasone treatment was -3 mm (standard deviation [SD] 7), -2 mm (SD 4) and -14 mL (SD 45) respectively. Hematoma without hyperdense components showed the largest decrease of hematoma thickness of -5 mm (SD 4) and midline shift -3 mm (SD 3) compared with other subtypes. Decrease in hematoma volume was largest in separated hematoma with a mean change of -28 mL (SD 48; Table 3; Fig. 3).
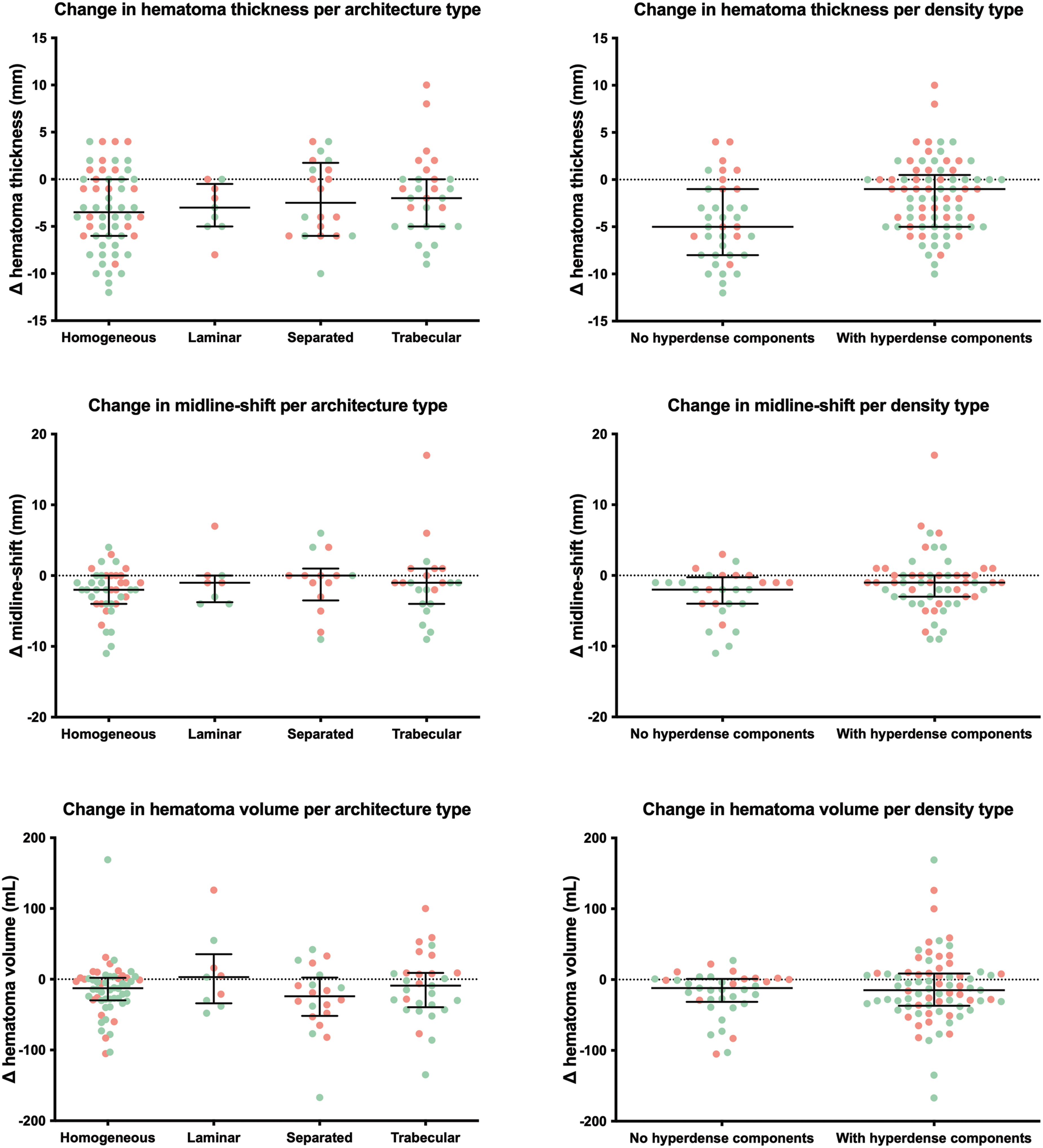
Boxplot of change in radiological parameter per hematoma subtype
Radiological Hematoma Evolution – Change in Hematoma Size per Hematoma Subtype (Two Weeks)
SD, standard deviation.
Multi-variable linear regression analysis revealed a significant group effect for change in hematoma thickness between the two hematoma density groups. A larger decrease in hematoma thickness was observed in hematoma without hyperdense components compared with hematoma with hyperdense components (adj. b -2.2 mm, 95% CI -4.1 to -0.3). No significant group effect for change in hematoma thickness was found between the hematoma architecture subgroups (A-D; p = 0.53).
A significant group effect for change in midline shift was found in the combined density analysis with a larger decrease of midline shift in hematoma without hyperdense components compared with hematoma with hyperdense components (adj. b -1.3 mm, 95% CI -2.7 to 0.0). No significant group differences were found between the individual architectural subtypes for change in midline shift (p = 0.1 and p = 0.9, respectively), nor for change in hematoma volume in the architectural (A-D; p = 0.2) or combined density (p = 0.5) group analyses.
Clinical course
In 47 patients (55%) an improvement in neurological function was observed at primary follow-up evaluation (Table 2), with a median onset of improvement on Day 2 (IQR 1-4), corresponding to a daily dexamethasone dose of 16 mg. Multi-variable linear regression analysis revealed a larger decrease in hematoma thickness (b -4.0, 95% CI -5.6 to -2.4), midline shift (b -3.1, 95% CI -4.1 to -2.0), and hematoma volume (b -33.5, 95% CI -49.9 to -17.0) in patients with neurological improvement compared with patients without neurological improvement. No significant group differences in neurological improvement were found in the architecture or combined density type analysis (p = 0.8 and p = 0.1, respectively).
An improvement in Markwalder Grading Scale score at the primary follow-up evaluation was reported in 32 out of 85 patients (38%), with unchanged and deteriorated scores in 45 (53%) and eight (9%) patients, respectively (Table 2; Fig. 4). Improvement rates were higher in patients with hematoma without hyperdense components (52%) compared with hematoma with hyperdense components (31%). Lowest improvement rates were observed in patients with separated hematoma (10%). No significant group differences in Markwalder Grading Scale score were found in the hematoma subtype analyses. Functional independence (modified Rankin Scale score 0-2) was achieved in 35 (41%) patients after 2 weeks dexamethasone therapy (Fig. 5). No significant group differences in functional independence were found in the hematoma subtype analyses. Complications were reported in 46 (57%) patients, with falls (17%), hyperglycemia (16%), and delirium (16%) occurring most (Table 4).
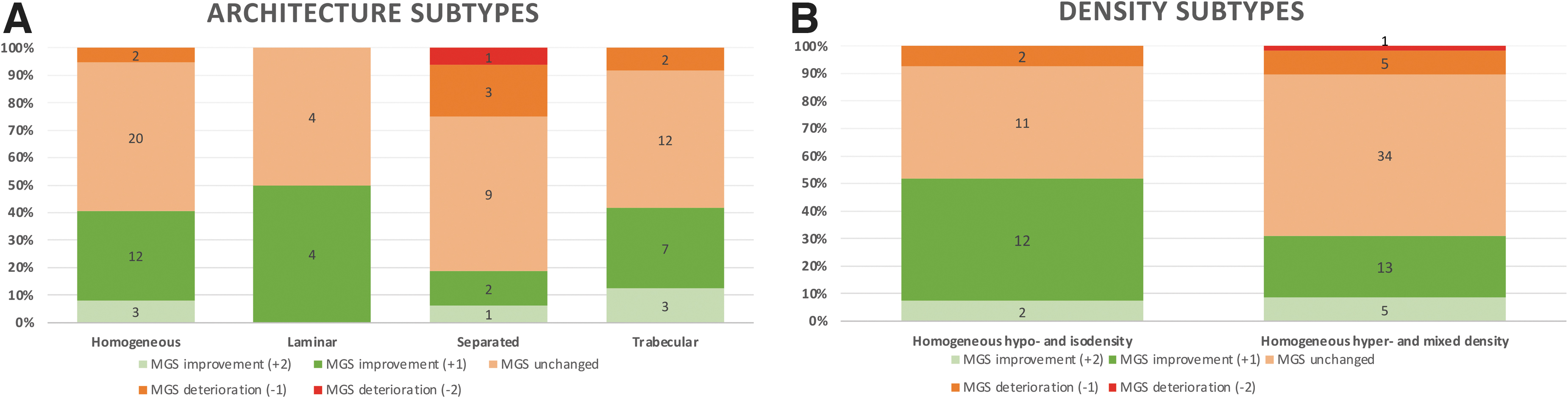
Change in symptom severity (Markwalder Grading Scale score) by hematoma subtypes at primary follow-up evaluation (2 weeks).

Change in functional outcome (modified Rankin Scale) at primary follow-up evaluation (2 weeks). Numbers indicate total number of patients with specific mRS-score. mRS, modified Rankin Scale score.
Complications
Additional surgery
Decision to perform additional surgery at the primary follow up evaluation, was made in 48 patients (57%) with a median duration to surgery of 16 days (range 1-71; IQR 8-28; Table 2). Clinical deterioration and unchanged radiological appearance were the main reasons to discontinue dexamethasone therapy in all radiological subtypes (Table 2). The need for surgery was highest in separated hematoma type, observed in 13 (81%) patients.
Discussion
The present study showed the largest reduction in midline shift and hematoma thickness in chronic subdural hematoma without hyperdense components, after dexamethasone treatment in symptomatic patients. Clinical improvement was also higher in hematoma without hyperdense components compared with other hematoma subtypes. Additional surgery was performed in 57% of patients, with the highest observed rate (81%) in separated hematoma.
Our results show a difference in radiological response in the different chronic subdural hematoma subtypes after dexamethasone therapy. Four previous studies have reported on (overall) radiological response in relation to clinical outcome or chronic subdural hematoma recurrence after dexamethasone treatment for symptomatic chronic subdural hematoma. 12,13,15 These studies did not differentiate the response in specific chronic subdural hematoma (density or architecture) subtypes. Smaller midline shift and hematoma thickness, as well as lower attenuation measurements in Hounsfield units—values at diagnosis, were suggested to favor beneficial effects of dexamethasone on clinical outcome or chronic subdural hematoma recurrence risk. The finding that low density hematoma respond more favorably to dexamethasone therapy, is consistent with our results that show the largest reduction in hematoma thickness and midline shift in hematoma without hyperdense components. This decrease in hematoma size is also reflected by a larger mean reduction in hematoma volume in hematoma without hyperdense components, although not reaching statistical significance. This is probably a methodological power issue, as a previous report demonstrated that midline shift in chronic subdural hematoma is associated with volume reduction. 37
The observed midline shift reduction in hematoma without hyperdense components after dexamethasone therapy underlines a decrease of hematoma pressure on brain parenchyma, favoring clinical improvement. Overall, we have demonstrated that greater reduction in hematoma size is associated with clinical improvement. Accordingly, higher rates of improvement in symptom severity expressed by the Markwalder Grading Scale score were observed in patients with hematoma without hyperdense components (52%) compared with hematoma with hyperdense components (31%). Because more subtle clinical improvements are likely to be missed by the five simplified categories of the Markwalder Grading Scale and the small subgroups in our data set, statistical significance in neurological improvement might have been missed.
At the initial homogeneous stage of chronic subdural hematoma development an inner and outer membrane mature around the subdural space. 10,27,38 Possibly, a balance is maintained during this homogeneous phase between the inflammatory cascade induced by hematoma degradation products, coagulation and fibrinolysis. 25,39,40 Recurrent hemorrhages, most likely triggered by head motion, have the opportunity to homogenize with the subdural collection. The anti-inflammatory effect of dexamethasone is presumably most effective at this phase because this stage encompasses the onset of inflammation in a steady-state. 39,41,42 In the subsequent two phases, defined as laminar followed by a separated hematoma, vascularity increases by formation of neo-capillaries and neo-membranes, which are vulnerable structures prone to rupture, resulting in hematoma growth and progression of the inflammatory response. 10,43,44 An increase in fibrinolytic activity also contributes to further hematoma enlargement in this phase. Chronic subdural hematoma recurrence rates have been reported highest during these hyper-fibrinolytic stages. 10,29,39 This underlying pathophysiology might explain why our fixed dexamethasone regimen was less effective in hematoma reduction in hematoma with hyperdense components compared with hematoma without. Dexamethasone might be insufficient in its inhibitory action on inflammatory and fibrinolytic mediators once the stage of separated hematoma is reached. 17,40,44 Although we observed higher rates of additional surgical treatment in separated type hematoma compared with other hematoma subtypes, this higher rate might also be influenced by the higher occurrence of bilateral chronic subdural hematoma in this group.
The identification of a radiological chronic subdural hematoma phenotype most responsive to dexamethasone therapy is important to assess whether there is any place for dexamethasone in the treatment algorithm of symptomatic chronic subdural hematoma. To identify these subgroups, further research is necessary. Recent randomized trials showed a poorer effect of dexamethasone therapy combined with surgery as well as standalone therapy compared with surgery alone on achieving a good functional outcome (IP Miah, Dexamethasone versus surgery for chronic subdural hematoma, DECSA-trial: a randomized controlled trial, 2022, in submission). 29 Overall, we found 41% of patients to achieve functional independence (modified Rankin Scale score 0-2) after 2 weeks dexamethasone. This necessitated additional surgery in the majority of patients. Disabling complications such as delirium or falls which interfere with a prosper clinical recovery, were both reported in 17% of patients. It is therefore likely that further research with dexamethasone in chronic subdural hematoma will become scarce. It is important to notice that current trials applied dexamethasone in the general population of symptomatic (Markwalder Grading Scale scores 1-3) chronic subdural hematoma patients including all hematoma subtypes. Whether treatment effects differ in specific radiological subtypes and mild symptomatic patients (Markwalder Grading Scale score 1), remains unknown. With the knowledge of the expected (extent of) radiological change per hematoma subtype, treatment effects might be optimized and better estimated by an improved patient selection.
A limitation of this study was the absence of a placebo-arm to confirm the treatment effect of dexamethasone. But maintaining a placebo-arm in symptomatic chronic subdural hematoma patients (Markwalder Grading Scale score 1-2) in need of treatment during 14 days to explore the radiological effect was deemed unethical. Since the aim of this substudy was to evaluate (short-term) radiological change in different chronic subdural hematoma subtypes and the vast majority of patients showed slowly progressive symptomatology in weeks prior to diagnosis, it is likely that the observed improvement within the first 2 days to 2 weeks, is due to dexamethasone effect rather than the natural disease course. Given the results of this study, future research is necessary to confirm the effects of dexamethasone on hematoma size in hematoma without hyperdense components by including less severely affected patients (Markwalder Grading Scale core 1). This specific subgroup will make it possible to maintain a placebo group.
Further, the relatively small sample size in density and architectural subgroups hampered interpretation of results. This probably impaired the demonstration of significant differences in radiological and clinical improvement in the architectural categories as well, combined with the limited symptom severity classification by the Markwalder Grading Scale score. By the implementation of two larger density subtypes, we achieved balanced subgroups. Whether treatment effect differs in specific architectural subgroups of the composite density group containing hematoma with hyperdense components, still remains to be unraveled. Further studies are warranted to explore the full potential and prognostic value of the architectural classification.
Conclusion
In this prospective substudy, we found hematoma without hyperdense components to be most responsive to dexamethasone therapy in the reduction of hematoma size. Clinical improvement was also higher in hematoma without hyperdense components compared with other hematoma subtypes. The presence of hyperdense components in chronic subdural hematoma could therefore be of prognostic value for poor response to dexamethasone treatment. To explore whether dexamethasone has potential in specific patient groups, further research into the pathophysiology of chronic subdural hematoma is warranted. Specific patient factors, including symptom type and severity in addition to age and gender, but also radiological appearance are important factors in determining treatment effect and prognosis.
Footnotes
Acknowledgments
We want to thank the research bureau (Landsteiner Institute) of the Haaglanden Medical Center (HMC), the Jacobus Foundation (Stichting Jacobus), The Hague and the department of Epidemiology and Medical Statistics of the Leiden University Medical Center (LUMC) for their facilitation during this research.
This study was a part of a recently completed randomized trial registered at the European Union Drug Regulating Authorities Clinical Trials Database, EudraCT: 2015-001563-39.
Authors' Contributions
IPM designed the study, collected and analyzed the data, and wrote the manuscript. AIB and YT collected data together with IPM and contributed to manuscript synthesis. EWZ and FRR designed the study together with IPM and revised the manuscript. WCP, RD, DCH, HFL, HMH, KJ and NAG contributed to the manuscript synthesis and revised the manuscript together with IPM.
Funding Information
Non-commercial funding was received from the Jacobus Foundation (Sint Jacobus Stichting) The Hague, Research Bureau (Landsteiner Institute) Haaglanden Medical Center.
Author Disclosure Statement
No competing financial interests exist.