
Abstract
Vitamin D may be important for neuroprotection after traumatic brain injury (TBI) by modifying the inflammatory response. The objective of this study was to evaluate the association between vitamin D deficiency and functional and survival outcomes in patients with TBI and intracranial injury. This study was a prospective multi-center cohort study conducted on adult TBI patients, with intracranial hemorrhage or diffuse axonal injury confirmed by radiological examination, admitted to five participating emergency departments (EDs) from December 2018 to June 2020. The study outcomes were good functional recovery at hospital discharge and survival at 6-months after injury. The primary exposure was serum vitamin D deficiency (0–10 ng/mL). Multi-level logistic regression analysis was performed to estimate the association between vitamin D deficiency and the study outcomes. Among 606 patients, 101 (16.7%) patients had vitamin D deficiency at the time of ED arrival. Good functional recovery was observed in 65.2% (395/606) of total population, and this proportion was significantly lower in the vitamin D deficiency group than the non-deficiency group (56.4 vs. 66.9%, p = 0.04, adjusted odds ratio (OR; 95% confidence interval [CI]): 0.56 (0.36–0.88)). Overall survival rate at 6 months after injury was 79.5% (434/546), and patients with vitamin D deficiency had significantly lower likelihood of survival at 6 months than patients without deficiency [75.0 vs. 80.3%, adjusted OR (95% CI): 0.59 (0.39–0.89)]. Vitamin D deficiency is associated with poor functional outcomes at hospital discharge and mortality at 6-months after injury in TBI patients with intracranial hemorrhage or diffuse axonal injury.
Introduction
Traumatic brain injury (TBI) is the leading cause of death and lifelong disability. Approximately 2.8 million people sustain TBI annually, 282,000 are hospitalized, and 50,000 die each year following injury, representing one-third of all injury-related deaths in the United States. 1 One study estimated that direct and indirect medical costs of TBI totaled $76.5 billion in the United States in 2010. 2 Neuroendocrine dysfunction leading to post-TBI pituitary hormone deficiencies is one of the contributing factors to the lifelong sequelae, and 5-20% of TBI patients have been reported to suffer hypothalamic-pituitary dysfunction. 3
Vitamin D is a hormonal factor that influences the prognosis and recovery of TBI patients. 4 Vitamin D is a group of fat-soluble secosteroids involved in the increased intestinal absorption of phosphate, calcium, and magnesium, and is synthesized primarily in the skin when exposed to sunlight. 5,6 Vitamin D has a multifaceted and widespread effect on multiple organ systems, including the skeletal system. TBI stimulates a series of metabolic events, including ion exchange disruption, cell membrane damage, axonal injury, inflammation, decreased cerebral blood flow, and cell death. 7 Acute release of inflammatory cytokines stimulates neuroprotective action by promoting tissue repair, whereas persistent inflammation causes oxidative stress and neurotoxicity. This secondary inflammatory response contributes to long-term sequelae after brain injury and is a target for therapeutic strategies. 8 Recent studies have suggested that vitamin D may be important for nervous system development and may play a role in neuroprotection by modifying the inflammatory response. 9 Low serum vitamin D levels are associated with several neurological disorders, including spinal cord injury, 10 epilepsy, 11 multiple sclerosis, 12 Alzheimer's disease, 12 Parkinson's disease, 13 and stroke. 14 Vitamin D deficiency is frequent in patients with TBI and is associated with cognitive impairment and more severe depressive symptoms. 15 Therefore, there have been a number of studies that have investigated the association between vitamin D and prognosis of severe TBI patients. 4,15 -17
Given the evidence that vitamin D plays an important role in brain pathology, we hypothesized that a low serum vitamin D status is associated with poor functional recovery and mortality after TBI with intracranial injury. This study aimed to determine the association between vitamin D deficiency and functional/survival outcomes among TBI patients with intracranial injury and to determine whether the effects would be modified according to the patient's age.
Methods
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board of all participating hospitals (approval No. CNUH-2018-297; SNUH-1806-078-951; KNUH-2018-10-014-007; CBNUH-2018-09-018; BMC-30-2018-85). Informed consent was obtained from the patient or guardian. All methods were performed in accordance with the relevant guidelines and regulations.
Study design and protocols
This multi-center prospective cohort study was based on the Pan-Asian Trauma Outcome Study (PATOS) registry. 18 The PATOS-TBI study is a collaborative research network that started in 2018 at five participating university hospitals throughout Korea for in-depth research on TBI (ClinicalTrials.gov, ID: NCT04718935).
The study was conducted in five emergency departments (EDs) of National University hospitals: 1) Seoul National University Hospital, operating a total of 1348 beds, has a Level 1 ED with approximately 70,000 ED visits annually; 2) Seoul Metropolitan Government-Seoul National University Boramae Medical Center, operating a total of 786 beds, has a Level 2 ED with approximately 40,000 ED visits annually; 3) Chonnam National University Hospital, operating a total of 1062 beds, has a Level 1 ED and a regional trauma center with approximately 50,000 ED visits annually; 4) Kyungpook National University Hospital, operating a total of 919 beds, has a Level 1 ED and a regional trauma center with approximately 40,000 ED visits annually; and 5) Chungbuk National University Hospital, operating a total of 820 beds, has a Level 1 ED and a regional trauma center with approximately 40,000 ED visits annually.
This multi-center prospective study aimed to identify nutritional and metabolic biomarkers that are related to the prognosis of severe TBI, such as cognitive and physical dysfunction after brain injury and quality of life in patients with TBI, and to develop a prognostic predictive model that applies them to select high-risk populations. The inclusion criteria were patients with TBI over 18 years of age who visited the participating hospitals' ED using emergency medical services (EMS) within 72 h of injury and who were diagnosed with intracranial injury, defined as intracranial hemorrhage or diffuse axial injury confirmed by a radiological examination. Patients with neurological disorders, psychiatric disorders, terminal cancer, pregnant women, penetrating brain injury, and those transferred to the participating hospital EDs after surgery at other hospitals were excluded from the study.
Upon confirmation of intracranial injury on radiological examination, an emergency physician obtained informed consent for enrollment in the study from the patient or the patient's next of kin in the ED. A research coordinator from each participating hospital collected and entered the registry, using multiple data sources. Serum biomarker levels were not reported to physicians, and patient management was not altered by the study. Follow-up data were captured via telephone surveys from the patient or the patient's next of kin at 1 and 6 months after the injury. Data were collected using a standardized data collection protocol, a case report form, and a web-based data collection system. The aggregated data were cleaned up and managed by the Quality Management Committee (QMC), and monthly data feedback was conducted to address incomplete and/or invalid entries. Education and training for research coordinators were periodically conducted at each hospital.
Study populations
This study enrolled patients over 18 years of age with TBI with intracranial injury who visited the participating hospitals' ED between December 2018 and June 2020. Patients with unknown information regarding vitamin D levels at the time of ED arrival were excluded.
Main outcomes
The main outcome measure was functional recovery at hospital discharge, as measured by the modified Rankin Scale (m-RS) score. 19,20 The m-RS was scored from 0 to 6 as follows: 0 (no disability), 1 (no significant disability), 2 (slight disability), 3 (moderate disability), 4 (moderately severe disability), 5 (severe disability), and 6 (death). Good functional recovery was defined as an m-RS score of 0, 1, and 2. The secondary outcomes were survival to hospital discharge and survival at 6 months after the injury.
Analysis of serum biomarkers
Upon confirmation of intracranial injury on brain imaging and patient consent to study enrollment in the ED, 24 mL of blood was drawn via venipuncture within 6 hours of ED arrival. Centrifugation was performed at 3000 rpm for 10 min at room temperature within 1 h of blood sampling.
To calculate serum vitamin D level, 25-OH vitamin D levels were measured using an electrochemiluminescence immunoassay (ECLIA). The assay utilizes a three-step incubation process with a duration of 27 min. In step 1, the sample was incubated with a pretreatment reagent, which releases bound 25-OH vitamin D from the vitamin D binding protein (VDBP). In step 2, the pretreated sample was incubated with ruthenium-labeled VDBP, creating a complex between 25-OH vitamin D and ruthenylated VDBP. The third incubation step involves the addition of streptavidin-coated microparticles and biotin-labeled 25-OH vitamin D. 21
Variables and measurements
The main exposure variable was the serum vitamin D level at the ED. The patients were divided into groups according to their serum vitamin D levels: Vitamin D deficient (0–10 ng/mL), insufficient (10–20 ng/mL), adequate (20–30 ng/mL), and optimal (> 30 ng/mL) groups in accordance with international standards. 22 Subsequently, the study population was re-classified into two groups: vitamin D deficient and non-deficient (insufficient, adequate, and optimal) groups.
We included data regarding patient demographics (age, sex, and comorbidities (hypertension, diabetes mellitus, and coagulation disorder), body mass index, and pre-injury disability), injury characteristics (mechanism of injury, place of injury, alcohol intake shortly before injury, and injury severity score), clinical findings (initial mental status at the ED, type of intracranial injury found on brain imaging, laboratory findings, treatment in the ED, need for surgery, and disposition after ED treatment), and patient outcomes at the time of hospital discharge and follow-up.
Statistical analysis
Descriptive analysis was conducted to compare the characteristics of patients depending on vitamin D deficiency and age group using the chi-square test for categorical variables and Wilcoxon rank-sum test for continuous variables.
Multi-level logistic regression analysis was performed to test the associations between vitamin D deficiency and the study outcomes in TBI patients after adjusting for hospital clustering. Crude and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Potential confounders were selected based on directed acyclic graph (DAG) models.
An interaction analysis model was used to investigate whether the effects of vitamin D deficiency were modified by age. An interaction term between vitamin D deficiency and age was added to the final multivariable logistic regression model. We conducted an interaction analysis using various age cut-offs (65 years old, 70 years old, and 75 years old) because the cutoff of age group could affect the magnitudes of the interaction effects.
All the variables included in the final model were assessed for multicollinearity. No significant collinearity was observed. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC). All p values were two-tailed, and statistical significance was set at p < 0.05.
Results
During the study period, 606 TBI patients with intracranial injury who were transported by EMS were registered in the PATOS-TBI study. There was no unknown information on serum vitamin D levels, and all of them were enrolled.
The distribution of serum vitamin D levels in the study population is shown in Figure 1 and Supplementary Figure S1. The median (interquartile range) vitamin D level was 16.8 ng/mL (11.4–23.3); 101 patients (16.7%) included in the deficient, 285 patients (47.0%) in the insufficient, 161 patients (26.6%) in the adequate, and 59 patients (9.7%) in the optimal group, respectively.
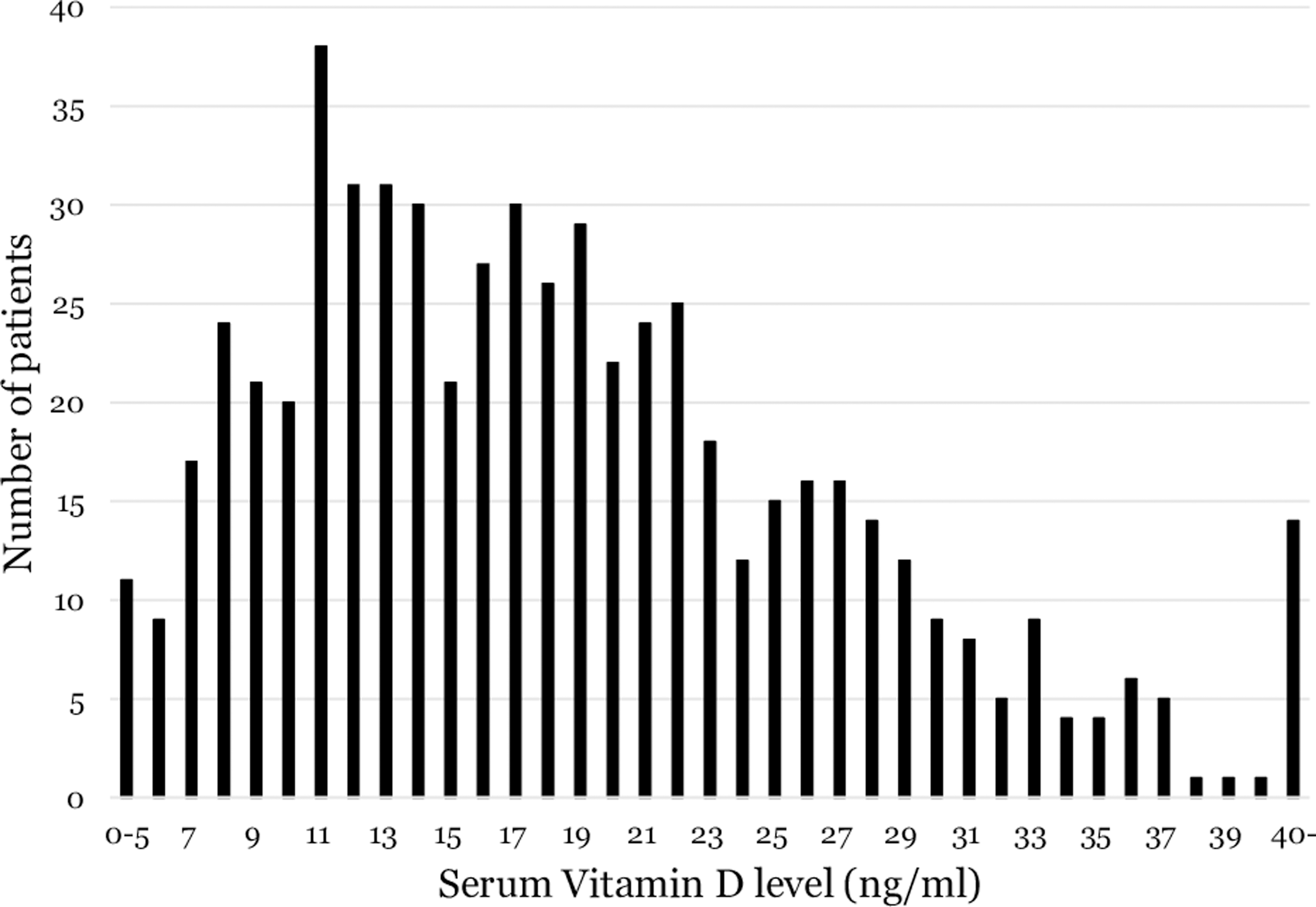
Distribution of participating patients' serum vitamin D level.
The characteristics of the study population according to vitamin D deficiency are shown in Table 1 and Supplementary Table S1. Vitamin D deficiency was observed in 101/606 (16.7%) of the study population. The proportion of good functional recovery was 65.2% (395/606) in study population: 56.4% (57/101) in the vitamin D deficiency group and 66.9% (338/505) in the non-deficiency group, respectively (p = 0.04). Survival to hospital discharge was 89.1% (90/101) in the vitamin D deficiency group and 91.1% (460/505) in the non-deficiency group, respectively (p = 0.53).
Characteristics of the Study Population According to the Vitamin D Deficiency
IQR, interquartile range; m-RS, modified Rankin Scale; ED, emergency department; AIS, Abbreviated Injury Scale; TBI, traumatic brain injury; NISS, New Injury Severity Score.
The characteristics of the study population according to the age group are shown in Table 2. Vitamin D deficiency was observed in smaller proportions in the elderly group: 51/247 (20.6%) for the 18–64-year-old, 14/143 (9.8%) for the 65–74-year-old, and 36/216 (16.7%) for the 75–120-year-old groups, respectively (p < 0.01). The proportions of good functional recovery were 69.6% (172/247), 70.6% (101/143), and 56.5% (122/216) in the 18–64-year-old, 65–74-year-old, and 75–120-year-old groups, respectively (p = 0.01).
Characteristics of the Study Population According to Age Group
IQR, interquartile range; m-RS, modified Rankin Scale; ED, emergency department; AIS, Abbreviated Injury Scale; TBI, traumatic brain injury; NISS, New Injury Severity Score.
In the multi-level logistic regression analysis, patients with vitamin D deficiency had lower odds of good functional recovery at hospital discharge (adjusted OR (95% CI): 0.56 (0.36–0.88)) and survival to 6-months after injury (adjusted OR (95% CI): 0.59 (0.39–0.89)) for patients with 6 months' follow up. There was no association between serum vitamin D and survival to hospital discharge [adjusted OR (95% CI): 0.71 (0.41–1.23)] (Table 3).
Multi-Level Logistic Regression Analysis on Study Outcomes in Relation to Vitamin D Deficiency
Model 1 adjusted for age and sex.
Model 2 adjusted for variables in Model 1, comorbidities (hypertension, diabetes mellitus, and coagulation disorder), body mass index (<18), pre-injury disability, and alcohol intake before injury.
Model 3 adjusted for variables in Model 2 and injury severity score.
aOR, adjusted odds ratio; CI, confidence interval.
In the interaction analysis, there were interaction effects between serum vitamin D levels and age on good functional recovery at hospital discharge. The effect of vitamin D deficiency was greater in younger TBI patients with intracranial injury than in the older population. Using 65-year-old cut-off (p for interaction <0.01), the effect value changed to significant odds in the 18–64-year-old group [adjusted OR (95% CI): 0.35 (0.18–0.69)], whereas it was not significant for the 65–120-year-old group [0.75 (0.37–1.51)]. Using 70-year-old cut-off (p for-interaction <0.01), the adjusted ORs 0.36 (0.19–0.68) for the 18–69-year-old group and 0.82 (0.39–1.74) for the 70–120-year-old group (Table 4).
Interaction Analysis between Vitamin D Deficiency and Age Group
OR adjusted for age, sex, comorbidities (hypertension, diabetes mellitus, and coagulation disorder), body mass index (<18), pre-injury disability, alcohol intake before injury, injury severity score, and interaction term.
AOR, adjusted odds ratio; CI, confidence interval.
Discussion
This prospective multi-center study to evaluate the association between vitamin D deficiency and functional/survival outcomes among TBI patients with intracranial injury found out that vitamin D deficiency was associated with lower odds for good functional recovery at hospital discharge [adjusted OR (95% CI): 0.56 (0.36–0.88)] and survival at 6 months after injury [0.59 (0.39–0.89)]. In the interaction analysis regarding patient age, the lower odds for better functional prognosis of vitamin D deficiency were more significant in the younger group, especially those younger than 70 years old. These results suggest that serum vitamin D can be considered a potential biomarker related to functional and survival outcomes in patients with TBI and intracranial injury, especially in the younger population.
Vitamin D exerts various effects on the nervous system by regulating function and neuroplasticity. Its role has been demonstrated in a wide range of neurological disorders including inflammatory and degenerative processes. 23 Intrinsic levels of vitamin D affect the inflammatory response to brain injury, and vitamin D deficiency is associated with cognitive dysfunction and severe depressive symptoms after injury. 15,16 In animal studies, vitamin D deficiency exacerbates the inflammatory response after TBI, and vitamin D therapy independently reduces inflammation and neuronal injury after TBI. 24 This has a more robust effect when administered in combination with progesterone. 24 -26 However, the data on supplementation of vitamin D and its translation into clinical benefit remains inconclusive. 27
Only 34.4% of Korean adult men and 31.8% of women had sufficient serum vitamin D levels (> 20 ng/mL) according to a previous study, 28 and only 36.3% of TBI patients in this study had sufficient vitamin D levels. By age, a previous study reported that vitamin D levels tended to decrease with age due to a reduction in vitamin D metabolism, outdoor activity, and nutritional status, 29 whereas a recent study found that adolescents and young adults are at risk for vitamin D deficiency due to their indoor lifestyle and nutritional behavior. 30 Interaction analysis showed a significant negative association between vitamin D deficiency and functional outcomes after TBI in younger patients (< 70 years of age), whereas there were no significant relationships in the elderly group (≥ 70 years of age). Age is closely associated with the incidence of severe TBI and might play an important role in mediating the response to and recovery from brain injury. 31 Although there are no clinical or animal studies related to the action of vitamin D in relation to aging, one mouse study found that reducing the expression of neuroprotective genes in aging may contribute to poor prognosis in the elderly following TBI. 32
In this study, vitamin D deficiency was associated with poor functional recovery and 6-months mortality in patients with TBI and intracranial injury, especially in the younger population. This may provide a theoretical basis for correcting vitamin D deficiency and supplementation before and after injury in patients with insufficient serum vitamin D levels. Nutritional health, including vitamin D level, is associated with recovery after severe TBI. 33 To reduce the burden of severe TBI, further studies are needed to rapidly determine the prognosis of patients with severe TBI and to develop strategies to improve functional and cognitive recovery after injury, especially in young TBI populations.
Limitations
This study had several limitations. First, serum vitamin D levels would be affected by elapsed time from injury; however, blood sample data in this study were collected only at the time of ED arrival and thus are missing data on the kinetics of serum vitamin D levels. Although there are no reports of changes in serum vitamin D levels after TBI, caution should be exercised when interpreting study results. Second, vitamin D levels may change by season and other extrinsic factors, 34 but this point was not considered in the analysis. Third, there were no available data on the history of vitamin D deficiency, diet diary, and/or nutritional status, which would have been related to serum vitamin D levels. Future studies are required to determine whether the associations between vitamin D levels and intracranial injury outcomes vary according to these differences. Finally, the study design was not a randomized controlled trial. There may have been significant potential biases that were not controlled.
Conclusions
Vitamin D deficiency was associated with a decreased functional recovery at hospital discharge and a low survival at 6 months after injury in TBI patients with intracranial hemorrhage or diffuse axonal injury, and these associations were more significant in younger patients. This study suggests that the serum vitamin D level is a potential biomarker for predicting the prognosis of patients with TBI with intracranial injury. Further studies are needed to develop strategies to improve functional recovery after severe TBI and to reduce the burden of TBI.
Footnotes
Acknowledgments
Authors' Contributions
Drs. Ro and Jung had full access to all of the data in the study and take responsibility for the integrity of the data as well as the accuracy of the data analysis.
Study concept and design: Drs. Ro and Shin.
Acquisition, analysis, or interpretation of data: Drs. Jung, Park (JHP), Moon, Lee, and Park (GJP).
Drafting of the manuscript: Drs. Ro and Jung.
Critical revision of the manuscript for important intellectual content: Drs. Shin and Ryu.
Statistical analysis: Drs. Ro and Jung.
Obtained funding: Dr. Ro.
Administrative, technical or material support: Drs. Jung, Park (JHP), Moon, Lee, and Park (GJP).
Study supervision: Drs. Ro, Ryu, and Shin.
Manuscript approval: All authors.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (Grant no.: NRF-2018R1C1B6007625, NRF-2021R1A2C4002898).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.