
Abstract
Mild traumatic brain injury (mTBI) is the most common form of brain injury. While most individuals recover from mTBI, roughly 20% experience persistent symptoms, potentially including reduced fine motor control. We investigate relationships between regional white matter organization and subcortical volumes associated with performance on the Grooved Pegboard (GPB) test in a large cohort of military Service Members and Veterans (SM&Vs) with and without a history of mTBI(s). Participants were enrolled in the Long-term Impact of Military-relevant Brain Injury Consortium-Chronic Effects of Neurotrauma Consortium. SM&Vs with a history of mTBI(s) (n = 847) and without mTBI (n = 190) underwent magnetic resonance imaging and the GPB test. We first examined between-group differences in GPB completion time. We then investigated associations between GPB performance and regional structural imaging measures (tractwise diffusivity, subcortical volumes, and cortical thickness) in SM&Vs with a history of mTBI(s). Lastly, we explored whether mTBI history moderated associations between imaging measures and GPB performance. SM&Vs with mTBI(s) performed worse than those without mTBI(s) on the non-dominant hand GPB test at a trend level (p < 0.1). Higher fractional anisotropy (FA) of tracts including the posterior corona radiata, superior longitudinal fasciculus, and uncinate fasciculus were associated with better GPB performance in the dominant hand in SM&Vs with mTBI(s). These findings support that the organization of several white matter bundles are associated with fine motor performance in SM&Vs. We did not observe that mTBI history moderated associations between regional FA and GPB test completion time, suggesting that chronic mTBI may not significantly influence fine motor control.
Introduction
Traumatic brain injury (TBI) is a highly heterogenous and prevalent injury. Mild TBI (mTBI), or concussions, account for approximately 82% of all TBIs in the general public. 1,2 In 2016, they accounted for 85.9% of all TBIs in United States military personnel 3 and pose a serious concern as a history of mTBI(s) can cause chronic cognitive and physical disabilities. 4
Mild TBIs may result from a variety of forces to the head, including blunt force trauma and intense over-pressurization from nearby explosions. These insults often cause histological changes to the underlying neural tissue, 5 which may have functional consequences on several domains, including motor control. Several studies have investigated magnetic resonance imaging (MRI) signatures of mTBI and have identified candidate biomarkers of injury in distributed white and gray matter brain regions. A large meta-analysis of military brain injury, the Enhancing NeuroImaging Genetics through Meta-Analysis (ENIGMA) consortium, reported pronounced alterations in the diffusivity of the superior longitudinal fasciculi (SLF) in Service Members and Veterans (SM&Vs) with a history of mTBI(s) relative to controls. 6 A meta-analysis of white matter alterations following mTBI found frequent abnormalities in the corpus callosum, internal capsules, SLF, and corona radiata. 7 Recent investigations have also highlighted gray matter alterations in the cingulate gyrus, 8 insular cortex, 9 thalamus, 10 and accumbens. 10
Although the mechanisms, locations, and force of the TBI-producing insults are heterogeneous, the adverse effects of mTBI(s) on cognitive domains, postural control, and motor functions are generally convergent across studies. 11 –14 This convergence has mechanistic underpinnings, and in particular, fine motor control (i.e., the coordinated and controlled movement of small muscles such as those in the hands and fingers) is supported by distributed gray and white matter regions that are affected by mTBI, including the SLF, corona radiata, internal capsule, thalamus, and basal ganglia. 7,10 However, less is known about the long-term impact of mTBI occurring in military settings compared to civilian settings. Brain and behavioral differences have been reported in studies that compare military and civilian groups. 15 Further, in an investigation of military mTBI, Tate and colleagues 10 reported several aberrant associations between subcortical shape and cognitive functions.
The purpose of this study was to identify associations between regional white matter organization, cortical thickness, and subcortical volumes and fine motor performance evaluated by the Grooved Pegboard (GPB) test in a large cohort of SM&Vs with and without a history of mTBI(s). We first hypothesized that GPB performance would be significantly worse on dominant and non-dominant hands among SM&Vs with a history of mTBI(s) relative to those without a history of mTBI(s). Second, we hypothesized that lower regional white matter organization of frontoparietal tracts and subcortical volumes of the basal ganglia would be associated with poorer performance on the GPB test among SM&Vs with a history of mTBI(s). Lastly, we hypothesized that we would observe interactive effects—that is, associations between regional imaging measures with respect to GPB performance would be moderated by mTBI history.
Methods
Participants
This study is a secondary analysis of data collected for the Long-term Impact of Military-relevant Brain Injury Consortium-Chronic Effects of Neurotrauma Consortium (LIMBIC-CENC) Prospective Longitudinal Study (PLS). We included two groups: 1) SM&Vs with a history of at least one mTBI (n = 847, mean age = 39.9 ± 9.5, 88% male); and 2) SM&Vs with a negative history of mTBI (n = 190, mean age = 39.9 ± 10.4, 78% male). A detailed description of the LIMBIC-CENC PLS cohort has been previously published. 16,17 The ongoing parent study collects longitudinal cognitive, mental health, neuroimaging, and physical data on post-9/11 era SM&Vs with deployment histories and either positive or negative mTBI histories at sites distributed throughout the U.S. All participants in the current report were recruited and evaluated at eight participating sites. Inclusion criteria were: 1) deployment in Operation Enduring Freedom, Operation Iraqi Freedom, Operation New Dawn, or follow-on conflicts; 2) history of combat exposure defined by the Deployment Risk and Resiliency Inventory Section D (DRRI-2-D) score >1 on any item 18 ; and 3) at least 18 years of age. Exclusionary criteria were: 1) any history of moderate, severe, or penetrating TBI; or 2) history of major neurologic disorder or psychiatric disorder causing a significant reduction in independent living status (e.g., complete spinal cord injury, schizophrenia). This study was approved by the Institutional Review Boards at all performing sites and each participant signed an informed consent document prior to undergoing study activities.
Assessment of TBI history
Lifetime history of all potential concussive events (PCEs) was evaluated using a modified version of the Ohio State University TBI Identification interview. 19 A detailed structured interview with an embedded algorithmic preliminary diagnosis based on the Department of Defense/Veterans Affairs common definition of mild TBI, the Virginia Commonwealth University retrospective Concussion Diagnostic Interview was employed for each identified PCE and was followed by site PI review and central quality assurance to confirm or rule out mTBI diagnosis. 20 A binary approach was used in this investigation and each participant was assigned as “with mTBI” or “without mTBI” based on the results of that structured interview and adjudication. Participants' demographics and deployment-related information were also collected. TBI history was collected at baseline and updated at each follow-up visit.
Grooved Pegboard test
The Grooved Pegboard (GPB) test (Lafayette Instruments, Lafayette, IN) is a timed test used to evaluate visual-motor coordination on the dominant and non-dominant hand. 21 The pegboard is a square 5 × 5 grid of 25 holes, with slots oriented randomly on the edge of each hole. Pegs have a one-sided notch that must be manipulated and rotated between two fingers (usually the thumb and index finger) to be inserted into a pegboard hole. The score of the GPB test is the time (in seconds) taken to fill all 25 pegboard holes (completion time) for each hand. The GPB Test was collected on the same day as imaging.
Image acquisition
At their baseline visit, participants underwent MRI scanning at 3T field strengths following a standardized protocol overseen by a central site to ensure compliance. Site-specific scan parameters are reported in Supplementary Table S1.
Image processing
All MRI images were centrally processed on the high-performance computing system at the Office of Research Computing at Brigham Young University. The raw MRI DICOM-format data was converted to the NIfTI format, using the dcm2niix conversion software, which automatically created the magnetic resonance-images' relevant sidecar files in Brain Imaging Data Structure
22
format, containing information about the MR acquisition parameters. The acpcdetect tool from the Automatic Registration Toolbox was used to put T1-weighted images into standard alignment. Intensity correction on T1-weighted data was performed using the Advanced Normalization Tools (ANTs; version
Diffusion MRI (dMRI) data was similarly centrally processed using standardized Enhancing Neuroimaging and Genetics Meta-Analysis (ENIGMA) diffusion tensor imaging (DTI) Working Group pipelines. dMRI data preprocessing steps included eddy current correction, brain extraction, and tensor fitting. Diffusion metrics, including fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD), for 24 white matter tracts based on the Johns Hopkins University white matter atlas were extracted using fMRI (functional magnetic resonance imaging) Software Library (FSL) tract-based spatial statistics (TBSS) tools. 24 –27 In brief, subjectwise diffusion data was nonlinearly aligned to a common space. A skeletonized image representing the averaged centers of each tract was created and aligned diffusion data was then projected onto the skeletonized image. The projected data were then used for analysis.
As neuroimaging measures may be affected by non-biological scanner and site-specific artifacts 28,29 including manufacturer, field strength, gradient nonlinearity, and subject positioning, we used the ComBat algorithm 30,31 to harmonize all region of interest (ROI) properties to reduce these effects. A summary of the non-harmonized imaging data distributions is given in Supplementary Table S2.
Statistical analysis
Our primary outcome for all analyses was GPB completion time of the participant's dominant hand; however, post hoc analyses also evaluated GPB completion times of the non-dominant hand. We used linear regression models to identify associations between GPB completion time and regional subcortical volumes, cortical thickness, and tract-wise FA measures; collectively referred to as ROIs. Within the cohort of SM&Vs with a history of mTBI, we regressed GPB completion times on ROI values while adjusting for participant age, sex, time since index injury (years), number of lifetime mTBIs, alcohol use disorder (assessed by the Alcohol Use Disorders Identification Test-Concise [AUDIT-C]), handedness, and acquisition site; i.e.,
where
Here, with negative and positive mTBI histories coded as 0 and 1, respectively, the interaction term is zero for those without an mTBI history, and the effect of ROI on GPB completion time is
for those with a positive mTBI history. We adjusted for multiple comparisons across all ROIs grouped within the set of volumetric and diffusion models (and separately for FA, RD, MD, and AD diffusion models) and again by models including an interaction term. Multiple comparisons corrections were done using the false discovery rate method with a standard 0.05 alpha level of significance. All statistics were computed using R version 3.6.3.
Results
Sample characteristics
Our study included 1037 SM&Vs. Of these, 863 had usable diffusion data, and an overlapping 970 had usable subcortical volume and cortical thickness data. Clinical and demographic characteristics of the full cohort and modality-specific cohorts are provided in Table 1. The mean age of the full cohort was 39.9 ± 9.6 years and age did not differ by TBI status. In total, 847 SM&Vs reported at least one mTBI. Our sample included 139 women, and the proportion of female participants with a positive mTBI history was significantly lower than males (χ 2 = 10.8, df = 1, p < 0.001). The mean dominant hand GPB completion time was 71.8 ± 13.9 seconds. On average, SM&Vs with a history of at least one mTBI took 1.41 sec longer than the comparison group to complete the dominant hand GPB task; however, this difference was non-significant (t = -1.30, df = 289.06, p > 0.05). Age was associated with GPB completion times (t = 8.00, df = 1034, p < 0.001) in the whole sample, with older participants performing more slowly. Female SM&Vs had shorter GPB completion times than males (t = 2.24, df = 169.45, p < 0.05), on average. Time since injury was not significantly associated with GPB completion time after adjustment for participant age. Non-dominant hand GPB completion time was higher in SM&Vs with at least one mTBI compared with those without a history of mTBI(s) at a trend level (mean difference = 2.3 sec, t = -1.93, df = 312.22, p < 0.1). This trend persisted following adjustment for age, sex, and time since injury.
Clinical and Demographic Data
TBI; traumatic brain injury; SD, standard deviation; mTBI, mild TBI; GPB, Grooved Pegboard.
Fractional anisotropy of several white matter tracts is inversely related to GPB completion time
We identified no significant associations between GPB completion time and interactions between imaging measures and mTBI status, suggesting the observed associations are not moderated by mTBI history. Within the cohort of SM&Vs with a history of mTBI(s), we identified associations between GPB completion time on the dominant hand and the FA of several white matter tracts. Whole–brain average FA was assessed alongside specific white matter structures including the bilateral anterior and posterior subdivisions of the corona radiata (CR); the whole CR; left and whole superior longitudinal fasciculus (SLF); the left and whole uncinate fasciculus (UNC). Several tracts exhibited significant inverse associations between GPB completion time and tract-wise FA: the whole posterior corona radiata (PCR; B = -62.32, t = -3.08, q < 0.05), right PCR (B = -54.13 t = -2.97, q < 0.05), left SLF (B = -61.52 t = -3.12, q < 0.05), and left UNC (B = -28.67, t = -2.97, q < 0.05). No associations between regional volume, cortical thickness, or other diffusion metrics (MD, AD, or RD), and GPB completion time were observed on the dominant hand. Model parameters are tabulated in Table 2. Significant associations between GPB completion time on the dominant hand and regional FA measures are illustrated in Figure 1. No associations between GPB completion time and regional diffusivity or volume were observed in the non-dominant hand.
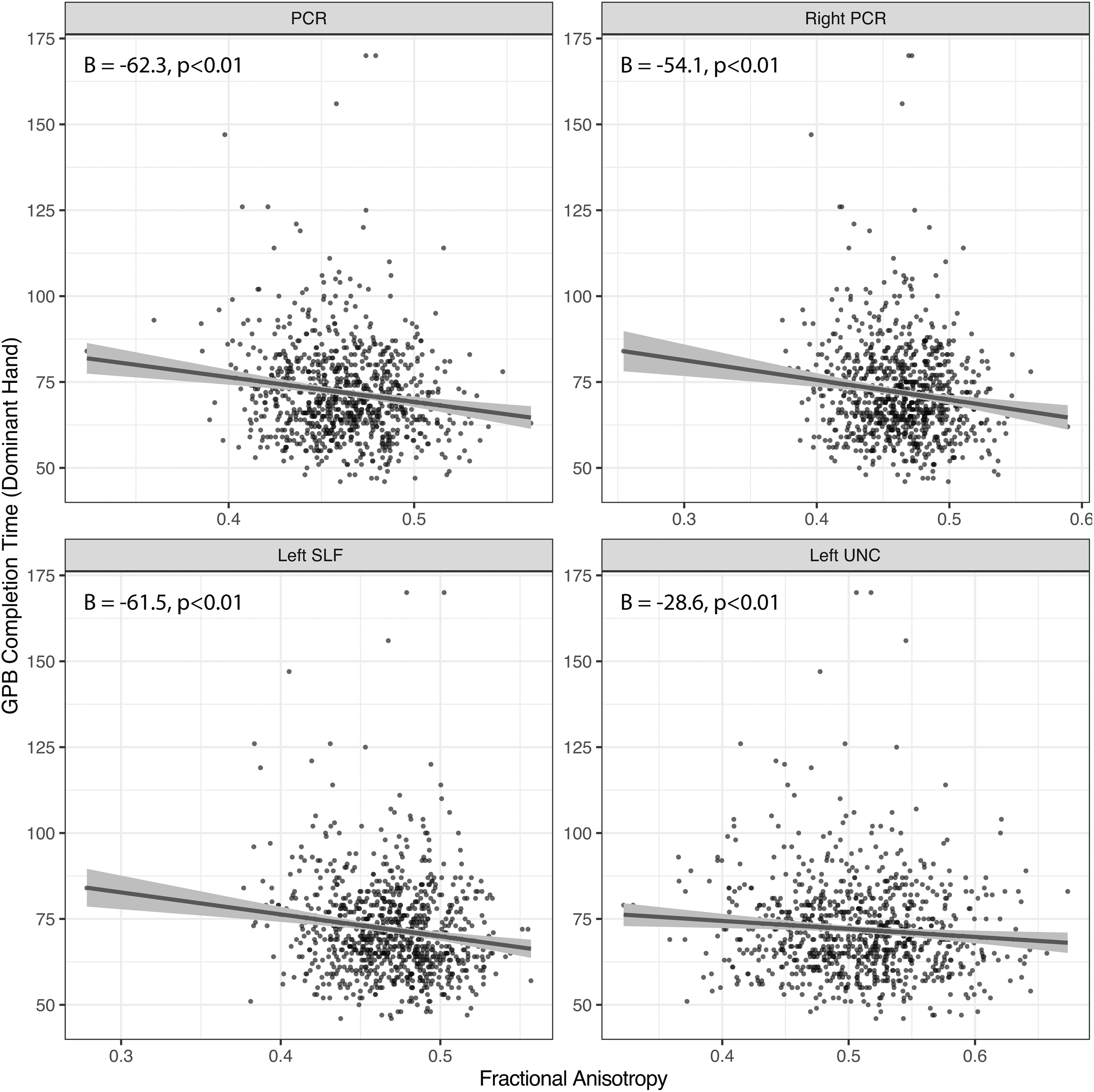
Significant associations between dominant hand Grooved Pegboard (GPB) completion time (y-axis) and regional fractional anisotropy (x-axis).
Model Estimates for Significant Associations Between Fractional Anisotropy and Dominant Hand GPB Completion Time
PCR, posterior corona radiata; SLF, superior longitudinal fasciculus; UNC, uncinate fasciculus
Discussion
We examined relationships between regional white matter microstructural organization and gray matter volumes with respect to motor function captured by the Grooved Pegboard (GPB) test in a large cohort of SM&Vs with and without a history of mTBI(s). We hypothesized that GPB completion time would be significantly slower in SM&Vs with a history of mTBI(s), that regional diffusivity and volumetric measures associated with motor functioning would be associated with GPB completion time, and that mTBI history would moderate associations between GPB completion times and regional imaging measures—that is, that magnitudes of associations between imaging measures and GBP time would vary between SM&Vs with and without history of mTBI(s). Notably, dominant hand GPB completion time did not significantly differ between SM&Vs mTBI groups; however, non-dominant hand time differed at a trend level between groups.
Within the mTBI group, we observed several associations between GPB completion time on dominant hand and regional white matter organization of the whole PCR, right PCR, left SLF, and left UNC. Two of the associations with GPB completion time were tracts in the left-hemisphere, which may reflect the contralateral control of participant's dominant hands in a predominantly right-handed sample (∼88% of participants were right-handed) 32 ; however, our models adjusted for handedness. We also observed that mTBI status did not moderate associations between regional imaging measures and GBP completion times. Further, no associations were observed between regional gray matter volumes and GPB completion time.
Lesion-based studies have previously highlighted that global white matter lesion (WML) burden worsens individual performances on motor and manual dexterity tasks. For example, the Northern Manhattan Study reported that participants with WML volumes at or above the 75th percentile performed more poorly on tests of manual dexterity. 33 Additional studies by the Leukoaraiosis And DISability Study (LADIS) group have highlighted associations between age-related white matter changes and disorders of gait and balance. 34,35 WML volumes in middle-aged individuals have also been associated with poorer performance on the GPB test, 36 suggesting that this effect is not restricted to elderly individuals.
The FA of the PCR was associated with GPB completion time for the dominant hand. To date, only a limited number of studies have reported on associations between motor function and the organization of the broader set of CR white matter fibers. The CR is composed, in part, of fibers descending from both frontal and parietal lobes projecting to the basal ganglia and spinal column that subserve a variety of motor and cognitive functions. An earlier study by Moulton and colleagues reported that axial diffusivity of the CR 24 h post-stroke was predictive of upper limb NIH Stroke Scale motor scores 7 days following a stroke. 37 In a smaller cohort of 15 patients with CR strokes, Koyama and colleagues reported that the FA of the cerebral peduncles was associated with subsequent upper and lower extremity function. 38 Taken together, these findings support that the organization of CR white matter is critical to the execution of fine motor or manual dexterity tasks.
Diffusivity of the SLF was also significantly associated with GPB completion time in the dominant hand. The SLF is a large fiber bundle connecting regions of the occipital, parietal, and temporal lobes to the frontal lobe 39,40 and is classically divided into four components, SLF I – IV. 40 Although we did not report on SLF subdivisions, SLF I projects from the superior parietal lobule to the supplementary and premotor areas of the frontal lobe and thus is thought to contribute to regulation of higher-order motor functions involving proprioception and initiation of motor activity. 40,41 Reported associations between SLF diffusivity and GPB performance are sparse; however, in a recent study of 55 children with ADHD and 61 matched controls, Hyde and colleagues 21 reported reduced performance on the GPB test on the non-dominant hand in children with ADHD. The degree of impairment in the non-dominant hand was further associated with reduced fiber density in SLF I. Recent studies in typically-developing controls have also demonstrated that microstructural properties and volumes of the SLF and its subcomponents are strongly associated with individual differences in fine motor control. 42,43 Collectively, these findings, along with our own, further support that the organization of white matter fibers such as the SLF, which subserve a broad range of visuospatial and higher-order motor functions, are key in supporting fine motor control.
We further identified an association between the UNC FA and dominant hand GPB completion time. The UNC projects from medial and lateral regions of the orbitofrontal cortex to the anterior portion of the temporal lobes 44 and is thought to subserve language processing as well as other cognitive functions, including object recognition. 45,46 To our knowledge, the UNC has not previously been implicated in serving a role in fine motor function. However, a study of patients undergoing surgical resection of portions of the UNC to treat gliomas found no significant effect of UNC resection, Trail Making, Verbal Fluency, or Word Learning tasks. 46 The same study, however, found no significant effect of UNC resection on other tasks including Trail Making, Verbal Fluency, or Word Learning. Further work needs to be done to characterize the role of the UNC in fine motor or visuospatial skills.
Our divergent findings identifying trend-level differences in GPB completion time on the non-dominant, but not dominant, hand is consistent with the limited literature in this area. While previous studies on mTBI have not observed this association, two previous studies in adolescents with ADHD have reported poorer GPB performance in the non-dominant, but not the dominant, hand relative to controls. 21,47 Although it is unclear why differences may be more pronounced on the non-dominant hand, it has been suggested that practice effects (i.e., the daily use of the dominant hand) may diminish between-group differences. 48 Additionally, we did not observe differential associations between regional patterns of diffusivity and GPB performance as a function of mTBI history. Nevertheless, previous reports have highlighted that the organization of major fiber bundles including the CR, SLF, and UNC, are widely affected by mTBI/TBI both acutely and longitudinally. 6,49 -51
Limitations
There are several limitations to consider for this study. Multi-site neuroimaging data are commonly confounded by site- and scanner-specific idiosyncrasies; thus, there may have been systematic imaging and GPB performance differences across sites. ComBat harmonization was used to mitigate potential site-based differences in imaging measures; though, GPB scores were not harmonized. Additionally, ComBat harmonization is applied to post-processed data and successfully removed site-based associations in our imaging data (Supplementary Fig. S1); however, it remains unclear whether this method of harmonization is as effective as harmonization methods applied directly to magnetic resonance images. It is also noted that antidepressant medications can alter regional brain structures, but medication status was not evaluated in this study. We were further unable to account for pre-deployment mood disorders. Additional limitations include the wide range of times since injury within the SM&V cohort with a history of mTBI(s) and the cross-sectional nature of the study.
Conclusions
In summary, our findings indicate that among SM&Vs with a history of at least one mild TBI, performance on fine motor tasks captured by the GPB test is associated with the organization of major WM tracts, including the posterior corona radiata, superior longitudinal fasciculus, and uncinate fasciculus, and that these associations did not differ significantly from SM&Vs without a history of mTBI(s). In SM&Vs with a positive mTBI history, we also observed trend-level reductions in GPB performance only in the non-dominant hand, which may relate to effects of consistent dominant hand usage overriding mTBI-related deficits in manual dexterity or enhanced resilience of the motor skills in the dominant hand to mild injury. However, we did not observe differences in associations between white matter organization and GPB performance as a function of mTBI status, suggesting that mTBI-related abnormalities in fiber organization may not contribute to diminished performance on manual dexterity in this cohort. Future work should focus on elucidating specific effects of injury mechanisms; for example, whether blast-related mTBI(s) or repeated mTBI(s) relate to manual dexterity performance.
Footnotes
Acknowledgments
Disclaimer: The views, opinions, interpretations, conclusions and recommendations expressed in this manuscript are those of the authors and do not reflect the official policy of the U.S. Department of the Navy, Department of the Army, Department of Defense, Department of Veterans Affairs, or the U.S. government.
Ethics approval: This study was approved by the local Institutional Review Boards at all eleven prospective longitudinal study enrollment sites.
Consent to participate: All study participants signed an informed consent document prior to undergoing study procedures.
Consent for publication: Consent form signed by all participants included consent for publication of their deidentified data.
Availability of data and material: Available to the public in the Federal Interagency Brain Injury Research (FITBIR) Informatics System.
Code availability: not applicable.
Authors' Contributions
Benjamin Wade: Conceptualization, methodology, writing—original draft, software, investigation, formal analysis. David Tate: Supervision, data curation, investigation, conceptualization, funding acquisition, writing—review and editing. Eamonn Kennedy: Methodology, writing—review and editing. Erin Bigler: Supervision, writing—review and editing. Gerald York: Funding acquisition, writing—review and editing. Brian Taylor: Funding acquisition, project administration, writing—review and editing, resources. Maya Troyanskaya: Writing—review and editing. Elizabeth Hovenden: Writing—review and editing, data curation. Naomi Goodrich-Hunsaker: Data curation, writing—review and editing, software. Mary Newsome: Writing—review and editing. Emily Dennis: Writing—review and editing, funding afgcquisition. Tracy Abildskov: Data curation, resources. Mary Jo Pugh: Funding acquisition, writing—review and editing. William Walker: Funding acquisition, resources, writing—review and editing. Kimbra Kenney: Funding acquisition, writing—review and editing. Aaron Betts: Data curation, writing—review and editing. Robert Shih: Data curation, writing—review and editing. Robert Welsh: Funding acquisition, writing—review and editing. Elisabeth Wilde: Funding acquisition, project administration, supervision, resources, conceptualization, writing—review and editing.
Funding Information
This work is supported in part by a NARSAD Young Investigator Grant (27786 to BW) and a K99 Pathway to Independence Award (MH119314 to BW). The United States (U.S.) Department of Veterans Affairs Merit Review Awards Numbers I01 CX001820 (RS). R61NS120249 to ELD, DFT, and EAW. This work was supported by the Assistant Secretary of Defense for Health Affairs endorsed by the Department of Defense, through the Psychological Health/Traumatic Brain Injury Research Program Long-Term Impact of Military-Relevant Brain Injury Consortium (LIMBIC) Award/W81XWH-18-PH/TBIRP-LIMBIC under Awards No. W81XWH1920067 and W81XWH-13-2-0095, and by the U.S. Department of Veterans Affairs Awards No. I01 CX002097, I01 CX002096, I01 HX003155, I01 RX003444, I01 RX003443, I01 RX003442, I01 CX001135, I01 CX001246, I01 RX001774, I01 RX 001135, I01 RX 002076, I01 RX 001880, I01 RX 002172, I01 RX 002173, I01 RX 002171, I01 RX 002174, and I01 RX 002170, I01 CX001820. The U.S. Army Medical Research Acquisition Activity, 839 Chandler Street, Fort Detrick, MD 21702-5014 is the awarding and administering acquisition office. Additional funding was provided by VA Health Services Research and Development (IK6HX002608).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.