
Abstract
Military service members are at increased risk for mental health issues, and comorbidity with mild traumatic brain injury (mTBI) is common. Largely overlapping symptoms between conditions suggest a shared pathophysiology. The present work investigates the associations among white matter microstructure, psychological functioning, and serum neuroactive steroids that are part of the stress-response system. Diffusion-weighted brain imaging was acquired from 163 participants (with and without military affiliation) and free-water-corrected fractional anisotropy (FAT) was extracted. Associations between serum neurosteroid levels of allopregnanolone (ALLO) and pregnenolone (PREGNE), psychological functioning, and whole-brain white matter microstructure were assessed using regression models. Moderation models tested the effect of mTBI and comorbid post-traumatic stress disorder (PTSD) and mTBI on these associations. ALLO is associated with whole-brain white matter FAT (β = 0.24, t = 3.05, p = 0.006). This association is significantly modulated by PTSD+mTBI comorbidity (β = 0.00, t = 2.50, p = 0.027), although an mTBI diagnosis alone did not significantly impact this association (p = 0.088). There was no significant association between PREGNE and FAT (p = 0.380). Importantly, lower FAT is associated with poor psychological functioning (β = -0.19, t = -2.35, p = 0.020). This study provides novel insight into a potential common pathophysiological mechanism of neurosteroid dysregulation underlying the high risk for mental health issues in military service members. Further, comorbidity of PTSD and mTBI may bring the compensatory effects of the brain's stress response to their limit. Future research is needed to investigate whether neurosteroid regulation may be a promising tool for restoring brain health and improving psychological functioning.
Introduction
Military personnel returning from Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), or Operation New Dawn (OND) show high rates of health problems in general 1,2 and mental health problems in particular. 3 Post-traumatic stress disorder (PTSD) and mild traumatic brain injury (mTBI) are the most common diagnoses and have therefore been described as “signature wounds” of military service members. 4,5 Further, comorbidity with other mental disorders such as depression, substance abuse, or anxiety disorder is common. 6 –9 In fact, up to 30% of veterans 8,9 are diagnosed with a mental disorder compared with 4–12% among the general population. 10
Importantly, even those service members who do not meet the diagnostic criteria for a mental disorder are at risk for experiencing low quality of life and psychological distress, which may lead to problems in their social and work life. 11,12 The largely overlapping symptoms of various psychiatric conditions in veterans, including general distress, exaggerated startle, sleep disturbances, depressed mood, anxiety, and impaired social functioning, 8 suggest a common underlying pathophysiology. 13,14 However, to date, most research has been focused on specific psychiatric diagnoses according to categorical diagnostic criteria, neglecting the complexity of comorbidity as well as the overlap in clinical features across diagnoses. 15
Given the high overlap of symptoms among various conditions, a second approach that has become more popular is to investigate psychosocial functioning on a continuum. 15 In fact, there is evidence that impairments in psychological functioning – the interplay of an individual's overall mental health, behavior, and social skills 16 – underlies almost all mental disorders, 15 suggesting a shared common pathomechanism. 15 Shared underlying symptom clusters can be identified using factor analysis, which has been widely used to facilitate the interpretation of multiple related variables of interest by reducing multicollinearity. 15,17 –19 Summarizing the clinical characteristics of military service members into one common factor that explains the majority of symptoms could relate them to objective measures of brain structure and function, thereby elucidating potentially common pathophysiological processes.
A major common feature underlying many psychiatric conditions is the dysregulation of the stress response system 20,21 which may explain similar symptom clusters among various mental disorders. Military service members in particular commonly face extended periods of stress associated with deployment, which activates their stress response system. 22 It is of note here that the neurosteroid allopregnanolone (ALLO) and its precursor pregnenolone (PREGNE) are involved in the neuroendocrinological stress regulation 23 –25 to normalize the hyperactivation in the hypothalamic–pituitary–adrenal (HPA) axis. 26 –28 In response to traumatizing stress or brain trauma, ALLO and PREGNE exert neuroprotective effects by promoting anti-inflammatory, 25,29 –32 anti-apoptotic, 33,34 and pro-myelinating processes. 35 Moreover, ALLO binds to γ-aminobutyric acid type A (GABAA) receptors, which leads to a positive receptor modulation and induces anxiolytic and analgesic effects. 28,36
Although acute stress stimulates an upregulation of neuroactive steroids, chronic stress has been shown to result in downregulation of ALLO levels. 37 –44 This may be explained by the fact that GABA receptor sensitivity decreases following repeated stress exposure as a result of excessive neurosteroid binding. 36 Therefore, it is possible that neurosteroid levels are compensatorily downregulated during chronic stress, to restore GABA receptor sensitivity. 36 Indeed, service members with TBI, 22 PTSD, 45 or comorbid mTBI and PTSD 46 exhibit decreased neurosteroid levels compared with healthy controls. In turn, the chronic stress-induced decrease in neurosteroid concentrations leads to hypersensitivity to new stressors, 42,43,47 dysfunctional behavior, 48 memory deficits, 49 sleep problems, 50 –52 and depressive symptoms, 53 thereby perpetuating the endocrine dysregulations.
Although neurosteroid dysregulations have been shown to lead to poor psychological outcome and impaired behavior, 42,43,47,48,50 –53 their underlying pathomechanisms remain largely unknown. There is initial evidence to suggest that brain structure likely plays a crucial mediatory role between neurosteroid dysregulation and psychological functioning. In fact, we recently revealed an association between neurosteroid levels and cortical thickness in veterans. 46 Additionally, animal studies of neurodegenerative diseases have reported an association between increased ALLO levels with markers of myelin and white matter regeneration. 54 The brain's white matter may in this way be responsible for some of the deficits in psychological functioning observed in service members. 55 Further, dense myelination is associated with faster signal transmission, 56 whereas impairments in myelination have been linked to impaired stimulus conduction. The latter translates into impairments in psychological functioning, as seen in various neuropsychiatric disorders. 55
Diffusion-weighted magnetic resonance imaging MRI (dMRI) has been used to study white matter microstructure in the most common diagnoses in military service members, including mTBI and PTSD. 57 –66 Most dMRI studies report widespread abnormalities of fractional anisotropy (FA), 67,68 suggesting demyelination or axonal degeneration. 69 However, the relationship between serum neurosteroid levels and white matter microstructure and its association with psychological functioning remains to be elucidated.
The aims of this study are to investigate (1) whether serum levels of ALLO and PREGNE are associated with psychological functioning, (2) whether serum levels of ALLO and PREGNE are associated with white matter microstructure, and (3) whether changes in white matter microstructure are associated with psychological functioning. Moreover, we will assess whether these associations are moderated by the most common diagnoses in military service members, mTBI and/or PTSD.
Methods
Ethics approval
This study was approved by the institutional review boards of all involved sites and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all study participants before enrollment.
Study design and participants
Participants were recruited as part of the Injury and Traumatic Stress (INTRuST) Clinical Consortium (W81XWH-08-2-0159,
To be included in the INTRuST study, participants had to be between 18 and 70 years old and have English as their primary language. Exclusion criteria were English as a second language acquired after the age of 5 years; history of a learning disability; uncontrolled hypertension; taking more than one antihypertensive medication; diagnosis of bipolar I disorder, psychotic, delirium, or dementing disorders; uncontrolled chronic disease; history of moderate to severe TBI; oral or intramuscular steroid use within the last 4 months; or currently taking medication affecting brain function (other than psychotropic medications). Exclusion criteria specific to participants who underwent MRI included general MRI contraindications, disorders of the central nervous system affecting the brain, and pregnancy/lactation.
Study enrollment was open from 2008 to 2013, and a total of 771 participants (both with and without military affiliation) were included. Four hundred and twenty-six participants underwent cranial MRI at 6 of the 10 study sites. In the present study, we included participants with both available MRI and serum neurosteroid data, resulting in a sample of 205 participants. MRI data was excluded from another 42 participants because of insufficient MRI data quality, yielding a final sample of 163 participants. Participants were to complete self-report questionnaires and imaging as well as blood draw within 30 days. The final sample did not differ significantly from the excluded participants in demographics (age, sex, race, education, income, employment status), PTSD and mTBI diagnosis, and psychological functioning (PTSD and depressive symptoms, insomnia, alcohol and drug use, functional disability, and health-related quality of life).
Clinical assessments and questionnaires
Assessment of PTSD
PTSD diagnosis was based on the Mini-International Neuropsychiatric Interview (MINI) 76 in 22 subjects, the PTSD Checklist (PCL) 77 in 21 subjects, the Clinician-Administered PTSD Scale for DSM-5 (CAPS) 78 in 9 subjects, and the Structured Clinical Interview for DSM-4 (SCID) 79 in 1 subject.
Assessment of mTBI
History of mTBI was assessed with a self-report mTBI screening instrument consisting of three items assessing (1) past brain injury, (2) immediate loss or alteration of consciousness or unawareness of the event, and (3) amnesia before or after the event. The INTRuST mTBI Screening Instrument was developed following the diagnostic criteria by the American Congress of Rehabilitation Medicine 80 and has been used in previous publications of the INTRuST Clinical Consortium. 46,64,71,74,75
Assessment of addiction
Alcohol or drug addiction was assessed according to the Drug Abuse Screening Test (DAST-20) 81 and the Alcohol Use Identification Test (AUDIT-10). 82
Assessment of psychological functioning
From the comprehensive INTRuST Clinical Consortium psychological test battery, questionnaires assessing psychiatric symptoms, functional impairment, and health-related quality of life were chosen in the present study (Table 1).
Psychological Functioning
Neurosteroid quantification
Serum neurosteroid quantifications were performed by gas chromatography/mass spectrometry (GC/MS) preceded by high-performance liquid chromatography
A constant amount of deuterated internal standard was combined with varying known quantities of steroids (Steraloids) to prepare the standard curve for the steroid of interest. Identical to the experimental samples, each standard curve sample was extracted three times in ethyl acetate prior to HPLC purification and GC/MS injection; standard curve r2 = 0.99 for each neurosteroid. The area under the peak of a known quantity of each steroid was divided by the area under the peak of the internal standard. The resulting ratio was plotted on the y-axis against known quantities of each steroid, generating a standard curve. Only integrated peaks with a signal-to-noise ratio ≥5:1 were integrated. The limit of neurosteroid quantification with this methodology is 1 pg for ALLO and PREGNE (femtomolar sensitivity).
MRI
Image acquisition
The current study used dMRI sequences acquired on three different types of 3-Tesla scanners (Tim Trio, Siemens Healthineers, Erlangen, Germany; GE 750, GE Healthcare, Chicago, IL, USA; or Achieva, Philips Healthcare, Best, The Netherlands) at 6 out of the 10 INTRuST acquisition sites (for imaging sequence details for each MRI system see Table 2).
Acquisition Parameters for Diffusion-Weighted Magnetic Resonance Imaging (dMRI)
Multi-site study; dMRI data acquisition on Tim Trio, Siemens Healthineers, Erlangen, Germany; GE 750, GE Healthcare, Chicago, IL, USA; Achieva, Philips Healthcare, Best, The Netherlands.
TE, echo time; TR, repetition time.
Image processing
Image harmonization and pre-processing
Data harmonization is indispensable when attempting to accurately analyze a large data sample acquired through different types of MRI scanners. Therefore, dMRI data were harmonized across the six data acquisition sites using a validated harmonization algorithm.
72
The harmonization approach accounts for scanner-specific differences such as spatial variability of the diffusion signal in different brain areas, while at the same time, the inter-subject variability is maintained at each site and scanner.
72
Pre-processing of the harmonized dMRI data was performed using scripts of our in-house image processing pipeline (
White matter fiber clustering
White matter fiber clustering was conducted according to an open-source pipeline of the whitematteranalysis software (
The white matter fiber clustering bases the white matter parcellation of each subject on a pre-provided fiber clustering atlas: a neuroanatomist-curated set of tracts covering the white matter (
Next, each subject's tractography was registered with the pre-provided atlas tractography. By following up with this step we were able to largely reduce the known tractography issue of false-positive tracking. 92 False-positive fiber tracking is a contributing factor affecting white matter parcellation reproducibility. 92 With our approach, false positive fibers in the atlas have been annotated and rejected via expert judgment. 90 Usage of the atlas therefore can ameliorate potential subject-specific false-positive fibers that are inconsistent with respect to known neuroanatomical knowledge. In this study, subject-specific fibers that had improbable fiber geometric trajectories were automatically removed.
For each subject, we performed atlas-based white matter parcellation 90,93,94 using a robust machine learning approach that has been shown to consistently identify white matter tracts across the full human lifespan, across health conditions including brain tumors, and across different image acquisitions. 90 This approach produces consistent tracts across subjects, 95 is reproducible in test-retest data sets 96 and is robust to anatomical variability. 94 The approach has also been employed for quantitative tractography analyses 97 in many recent studies. 98 –105
Subject-specific anatomical fiber tract identification was conducted for both hemispheres by linking the registered tractography to the annotated atlas clusters for each tract. Fiber tracts of the entire brain (Fig. 1) were combined into one whole-brain white matter variable, given that we aimed to investigate global white matter effects in association with neuroactive steroids and psychological functioning and did not specify hypothesis for individual tracts. A quantitative quality assessment of the number of streamlines (NoS) and FA was performed to make sure that there were not individual subjects with outlier values. A visual quality assessment of each subject's whole-brain white matter tracts was also performed to ensure anatomical correctness. These quality check processes follow best practices in recent studies. 98,102,106 –109 All data passed quality checks.
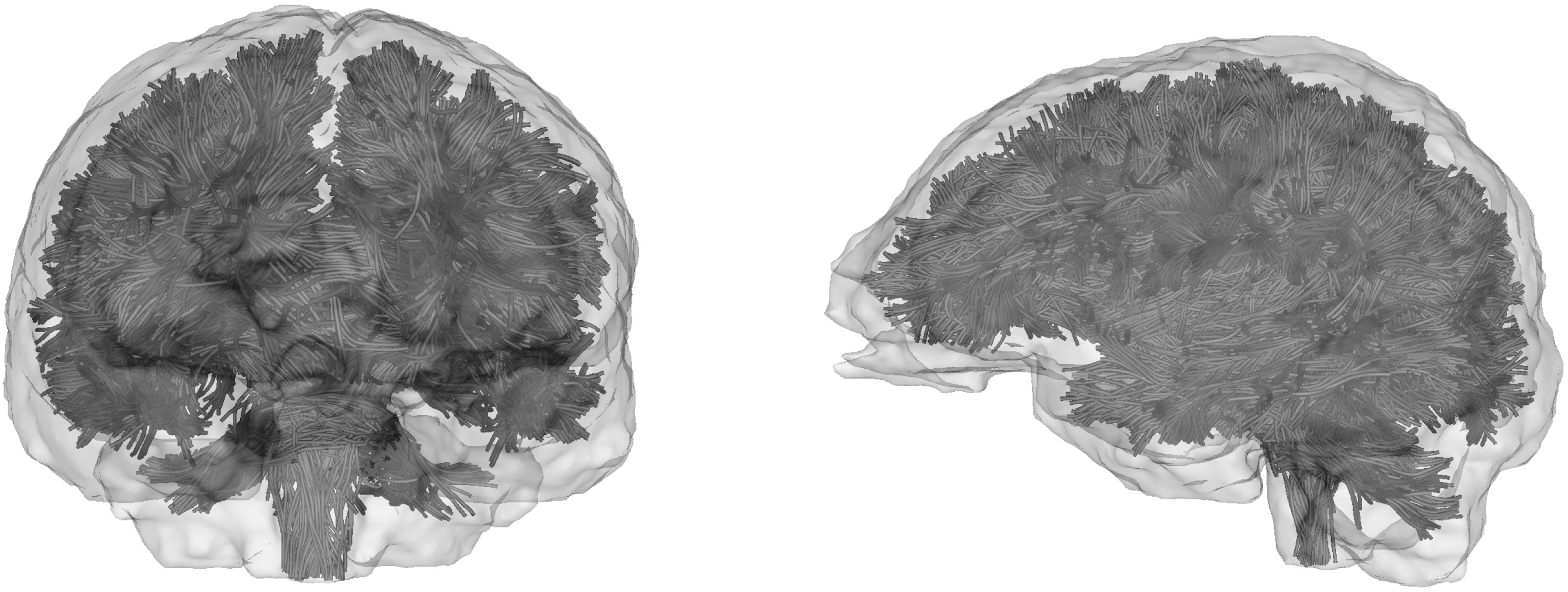
Whole-brain white matter tractography. This figure shows the whole-brain white matter of one participant derived from the fiber clustering output (in the sagittal and coronal plane).
Diffusion parameter extraction
Diffusivity of the extracted whole-brain white matter tracts was calculated and corrected for the relative contribution of extracellular free water in each voxel using free-water modeling. 110 The resulting diffusivity represents the tissue compartment in each voxel from which the tissue's free-water-corrected FA (FATissue, i.e., FAT) was calculated. Compared with FA, FAT serves as a more accurate marker for cellular white matter microstructure that is less susceptible to partial volume effects with CSF, and is thus more sensitive to the degree of myelinization of fiber tracts, axonal density, and fiber orientation. 111 Subject-specific average whole-brain FAT values were extracted from the whole brain's white matter fiber clustering output.
Statistical analysis
SPSS software (version 25.0; IBM Statistics for Mac, Armonk, NY, USA) was used for all statistical analyses. A Bonferroni-corrected p value of <0.05 was considered statistically significant.
Psychological functioning
Given the variety of psychological symptoms among veterans, we investigated whether a common psychological functioning construct was underlying the different psychological dimensions present in the current sample (assessed with the questionnaires presented in Table 1). A factor analysis using the Anderson–Rubin method to extract one or more underlying psychological functioning factors was performed. Varimax rotation was applied to ensure the orthogonality of the estimated factors. Only factors with an eigenvalue >1 were extracted. The assumptions for the conduction of a factor analysis were investigated using Bartlett's tests of sphericity.
Association between serum neuroactive steroids and psychological functioning
The association between serum neurosteroid levels and psychological functioning was assessed using two multiple regression models with independent variable serum ALLO/PREGNE and dependent variable psychological functioning (p < 0.025, Bonferroni-corrected for two tests). Age, sex, and alcohol and drug use were included as covariates. In case of a statistically significant association, we additionally assessed the effect of mTBI and PTSD+mTBI comorbidity on the association between serum neurosteroid levels and psychological functioning using Hayes PROCESS 112 (double moderation model – Model 2). Bonferroni correction was applied for two tests (p < 0.025). PTSD diagnosis without mTBI comorbidity was not investigated as an individual effect because of the small number of participants with PTSD only (n = 10).
Association between serum neuroactive steroids and whole-brain FAT
The association between serum neurosteroid levels and whole-brain FAT was analyzed by conducting two multiple regression models with independent variable serum ALLO/PREGNE and dependent variable whole-brain FAT (p < 0.025, Bonferroni-corrected for two tests). Age, sex, and alcohol and drug use were included as covariates. In case of a statistically significant association, we additionally assessed the effect of mTBI and PTSD+mTBI comorbidity on the association between serum neurosteroid levels and whole-brain white matter FAT using Hayes PROCESS 112 (double moderation model – Model 2). Bonferroni correction was applied for two tests (p < 0.025).
Association between whole-brain FAT and psychological functioning
The association between psychological functioning and whole-brain FAT was investigated using a multiple regression model with whole-brain FAT as independent variable and psychological functioning as dependent variable. Age, sex, and alcohol and drug use were included as covariates. In case of a statistically significant association, we additionally assessed the effect of mTBI and PTSD+mTBI comorbidity on the association between whole-brain FAT and psychological functioning using Hayes PROCESS 112 (double moderation model – Model 2).
Results
Sample characteristics
A sample of 163 participants from the INTRuST study were included. The demographic characteristics of the participants are displayed in Table 3. Neuropsychiatric comorbidities among the sample are visualized in Figure 2.
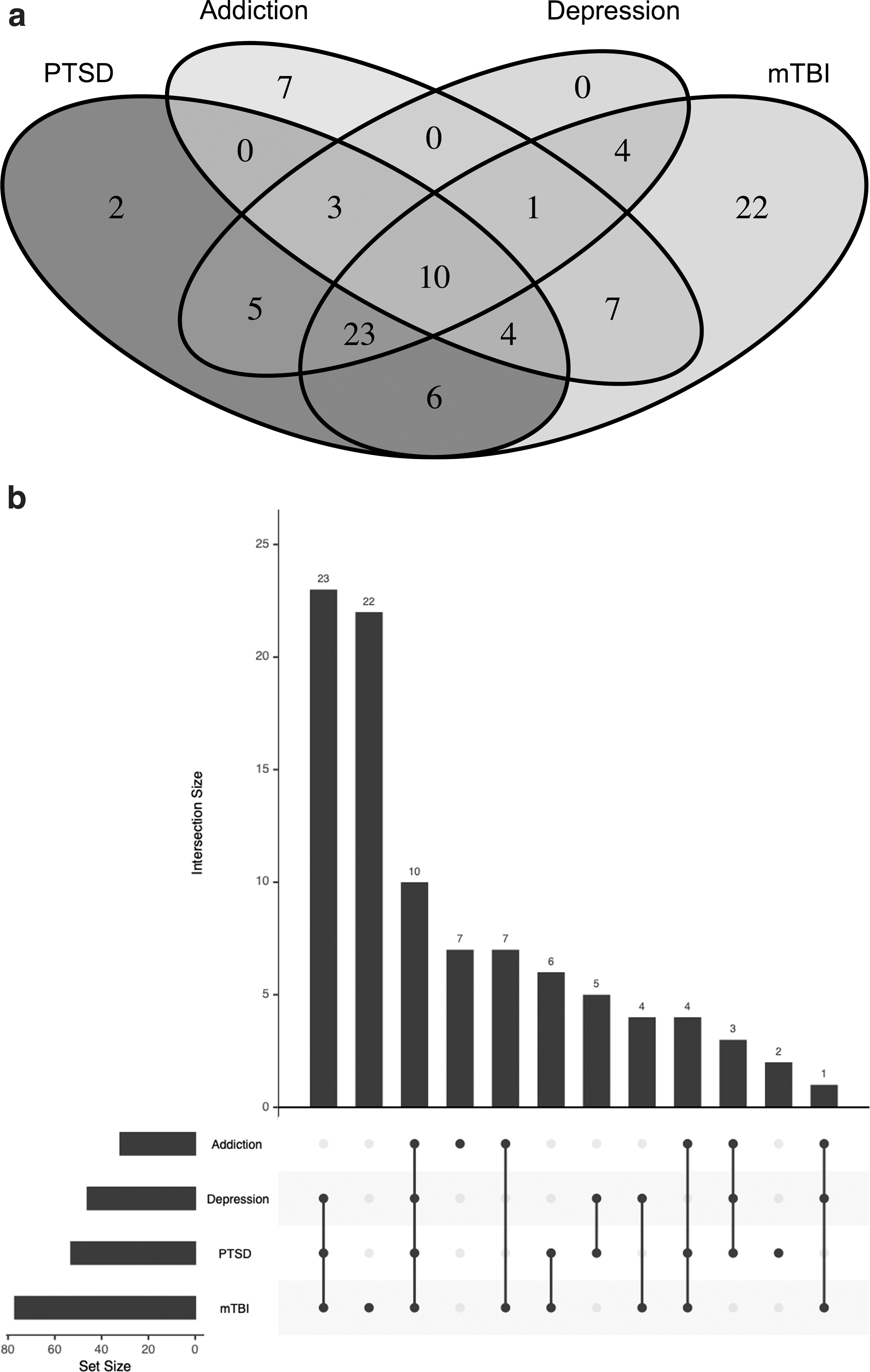
Neuropsychiatric comorbidities.
Sample Characteristics
SD, Standard deviation; PTSD, Posttraumatic stress disorder; mTBI, Mild traumatic brain injury; ME; IQR, interquartile range; ALLO, allopregnanolone; PREGNE, pregnenolone; AUDIT-10, Alcohol Use Identification Test; DAST-20, Drug Abuse Screening Test. For other test acronyms, see Table 1. Analyses of covariance (ANCOVAs) were corrected for age and sex (except for age and education).
Psychological functioning
Bartlett's test of sphericity was used to test the overall significance of all correlations within the matrix, which was statistically significant (χ 2 [15] = 1010.27, p < 0.001). As significant correlations between all variables were shown, conducting a factor analysis to identify the underlying factor behind the correlating variables is statistically justified. The factor analysis revealed one underlying psychological functioning factor based on PTSD symptoms (PCL-C); depression (Patient Health Questionnaire [PHQ]-9); psychological distress (Brief Symptom Inventory [BSI]); insomnia (Insomnia Severity Index [ISI]); functional impairment of work, social, and family life (SDS), and health-related quality of life (Short Form 12 Health Survey, General Health [SF12-GH]), with factor loadings between -0.75 and 0.96, and an eigenvalue of 4.97, accounting for 82.85% of the variance in the data (Table 4). The next factors had an eigenvalue of 0.41 and 0.24 and explained 6.8% and 4% of the total variance.
Association between serum neuroactive steroids and psychological functioning
There was no significant association between serum ALLO (p = 0.193) or PREGNE (p = 0.703) and the psychological functioning measure derived by the factor analysis.
Association between serum neuroactive steroids and whole-brain FAT
The multiple regression analyses revealed a significant positive association between serum ALLO and whole-brain FAT (β = 0.24, t = 3.05, p = 0.006). There was no statistically significant association between serum PREGNE and whole-brain FAT (p = 0.380).
The moderation analysis showed that the association between serum ALLO and whole-brain FAT was significantly moderated by PTSD+mTBI comorbidity (b = 0.00, t = 2.50, p = 0.027, Figs. 3 and 4), whereas an mTBI diagnosis alone did not impact this relationship (p = 0.088).
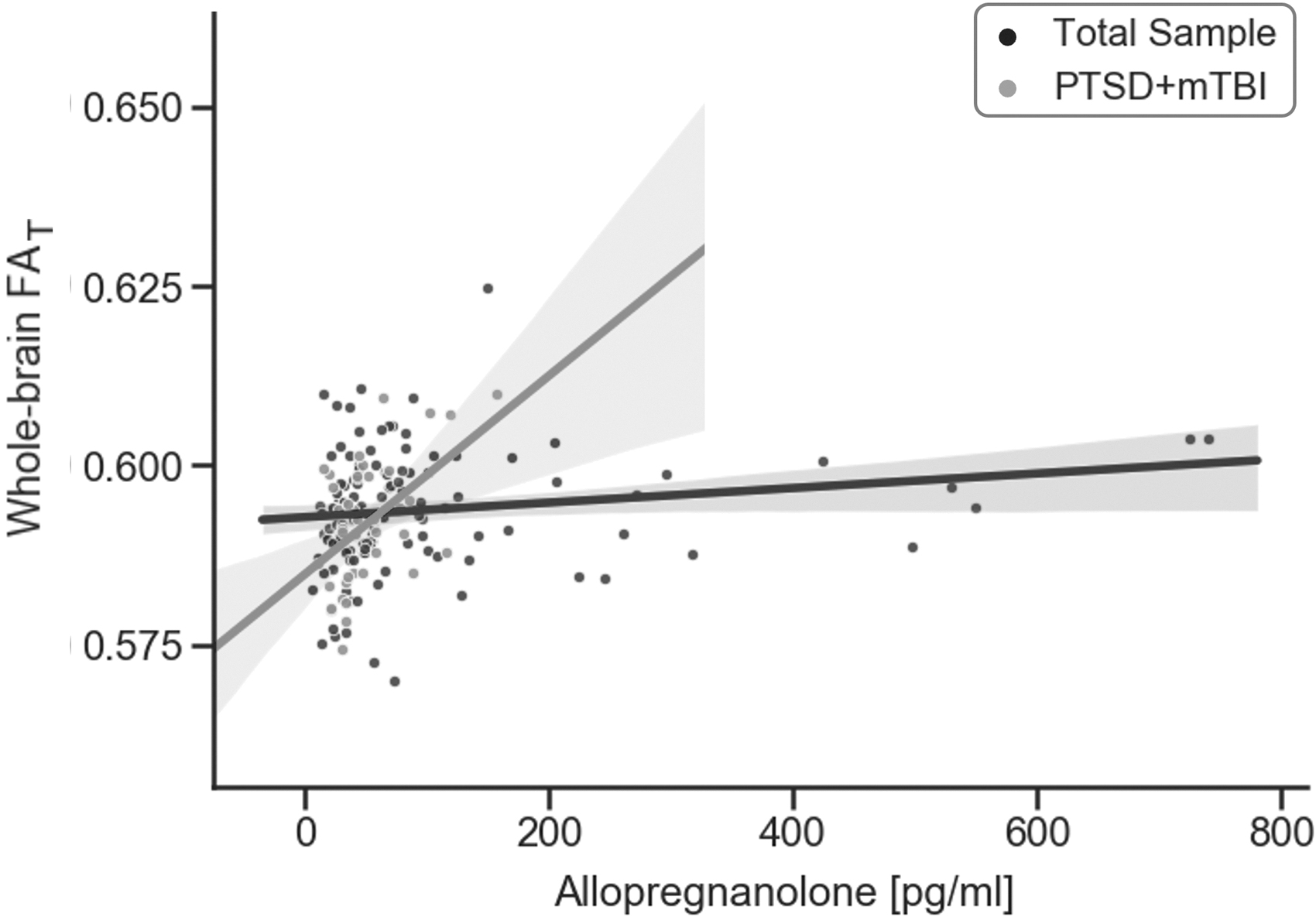
Association between allopregnanolone (ALLO) and whole-brain FAT. This figure illustrates the significant moderating effect of PTSD+mTBI comorbidity on the association between ALLO (pg/mL) and whole-brain FAT. mTBI, Mild traumatic brain injury; PTSD, Post-traumatic stress disorder; FAT, Fractional anisotropy Tissue
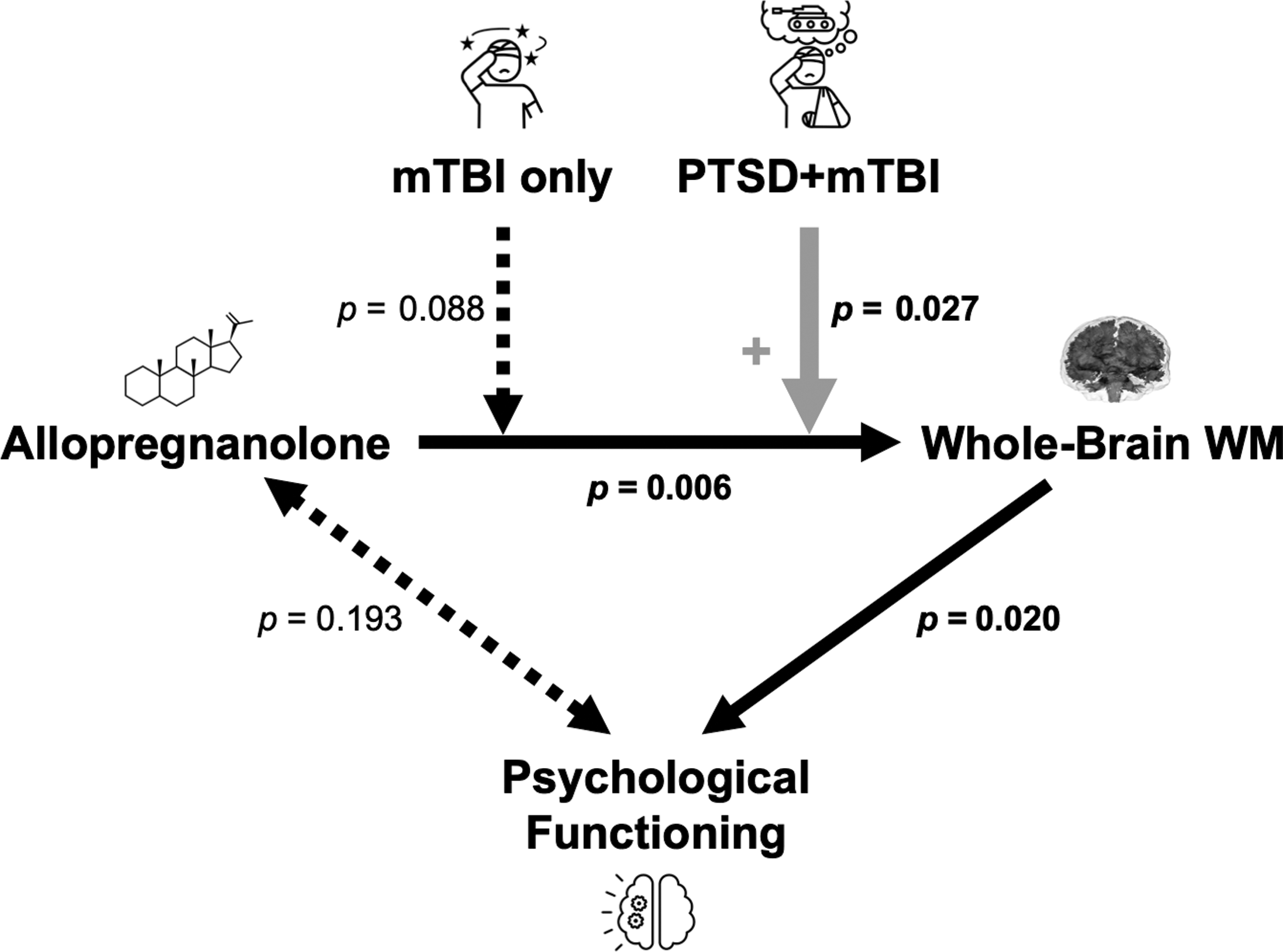
Summary of findings. This figure illustrates the significant associations between allopregnanolone (ALLO) and whole-brain white matter and between whole-brain white matter and psychological functioning. Comorbidity of PTSD and mTBI significantly alters the strength of the observed relation between ALLO and whole-brain white matter. PTSD, Post-traumatic stress disorder; mTBI, Mild traumatic brain injury.
Association between whole-brain FAT and psychological functioning
There was a significant negative association between whole-brain FAT and psychological functioning (β = -0.19, t = -2.35, p = 0.020, Fig. 4). Lower scores on the psychological functioning scale represent better functioning. Mild TBI (p = 1.000) or PTSD+mTBI comorbidity (p = 1.000) did not significantly alter this relation, suggesting that psychological functioning is associated with white matter structure independently of these diagnoses.
Discussion
This study investigated the association among serum levels of the neuroactive steroids ALLO and PREGNE, psychological functioning, and whole-brain white matter microstructure. Moreover, effects of mTBI and comorbidity of PTSD and mTBI on these associations were assessed.
Higher serum levels of ALLO were associated with increased white matter FAT. This suggests that higher levels of ALLO may have neuroprotective effects on white matter microstructure. Further, our results demonstrate that the association between ALLO and white matter FAT is stronger in individuals with PTSD and mTBI comorbidity (Figs. 3 and 4), indicating that a decrease in ALLO leads to a stronger decrease in FAT in these individuals. We suspect that these clinically highly burdened individuals are more sensitive to alterations in neuroactive steroids. Importantly, lower FAT is associated with poor overall psychological functioning in the entire sample and independent of mTBI or PTSD diagnosis (Fig. 5).

Association between psychological functioning and whole-brain FAT. This figure shows the association between the psychological functioning and whole brain FAT (β = -0.20, t = -2.38, p = 0.019). Lower scores on the psychological functioning scale represent better functioning. Scores are standardized z-scores with a mean of 0 and a standard deviation of 1.
Association between serum neuroactive steroids and psychological functioning
We demonstrate that a common factor is underlying the different symptom domains of psychological functioning. This result suggests that the different psychological questionnaires measure a common overall construct. This result is also in line with previous research showing that psychological symptoms in military service members assessed with different diagnostic tools are strongly correlated, 15 emphasizing further the shared nature of symptoms.
Contrary to previous findings, 42,43,47,48,50 –53,113,114 however, we did not detect a statistically significant association between serum neuroactive steroids and psychological functioning. Although most research studies to date have shown a link between neuroactive steroids and several dimensions of psychological functioning, one other study also did not find a direct influence of neuroactive steroids on psychological symptoms. 115 It should be noted that many of the previously published studies were conducted in animal models and that most studies examined group comparisons rather than correlations. 42,43,47 Moreover, previous research has focused only on specific facets of psychological functioning (such as in PTSD, 113,114 depression, 116 or sleep 50 –52 ), whereas studies on overall psychological functioning in relation to neuroactive steroids are currently missing. Further, the few studies with human subjects examined either men 114 or women 113 and included much smaller sample sizes than those in our study. 53,113,114
It is not yet clear to what extent sex might have affected the association between neuroactive steroids and psychological functioning. Therefore, future research should specifically investigate whether the measured values are affected by sex, using larger sample sizes.
Association between serum neuroactive steroids and whole-brain white matter microstructure
We demonstrate an association between serum levels of the neurosteroid ALLO and white matter microstructure. Previous research has attributed the positive effects of ALLO on white matter microstructure to anti-inflammatory, 25,29 –31 anti-apoptotic, 33,34 and pro-myelinating 35 effects previously reported for ALLO. In fact, ALLO increases markers of myelination 117 and reduces inflammatory cytokines in the brains of mice. 29 Moreover, ALLO promotes proliferation of neural progenitor cells and regulates cell-cycle gene and protein expression, 118 thereby further benefitting white matter microstructure.
Notably, the association between ALLO and white matter microstructure was significantly stronger in participants with the comorbidity of PTSD and mTBI, indicating that a decrease in ALLO levels may potentially lead to a stronger negative effect on white matter microstructure in these clinically highly burdened individuals. This is in line with previous research demonstrating that white matter abnormalities are more severe in those with PTSD and mTBI than in those with either or neither condition. 63 –66 Additionally, a study in this same cohort found an association between neuroactive steroids and cortical thickness only among individuals with PTSD and mTBI comorbidity, but not in those with mTBI only or in healthy controls. 46
In contrast to comorbid PTSD and mTBI, mTBI alone did not show a statistically significant effect on the association between neuroactive steroids and white matter alterations. It is of note that although most of the participants with mTBI alone in our study still had prolonged post-concussive symptoms, those who additionally had PTSD were more severely impacted. Service members with an additional current diagnosis of PTSD face ongoing stress-related endocrine dysregulations, which adds to their brain trauma sustained a decade ago.
Our findings thus support the hypothesis that neuroactive steroids reveal their neuroprotective effects particularly in stress-related conditions. Stress and trauma cause a variety of acute responses, such as upregulation of the HPA axis 119,120 or neurodegenerative processes. 121,122 In an attempt to regulate the stress response, neuroactive steroids counteract these dysregulations by promoting neuroregeneration and release neuroprotective effects on white matter microstructure. 27,28,123 –127 Thus, the association between neuroactive steroids and white matter microstructure may be most apparent in individuals with PTSD and mTBI comorbidity, as endocrine dysregulation 46 and consequently brain alterations 63 –66 are most pronounced in these individuals.
Moreover, there could potentially be a threshold effect of neuroactive steroids, meaning that they only exert adverse brain effects when concentrations are at a critical level. 128 Individuals with a PTSD diagnosis in addition to mTBI may be more likely to reach a critically low level of neuroactive steroids than individuals with a distant history of mTBI or healthy individuals, 46 so that neuroprotective mechanisms are no longer effective enough. Additionally, individuals with a comorbid mTBI and PTSD diagnosis also have a high prevalence of other comorbidities, such as depression 5,129 –131 and alcoholism, 132,133 which may further increase the overall stress burden and consecutive stress response and possible endocrine dysregulation. 113,134
Association between whole-brain white matter microstructure and psychological functioning
In the present study, we found an association between greater white matter microstructure alteration (decrease in FAT) and worse psychological functioning. Our finding is in line with previous studies, showing that various psychopathological conditions such as depression 64 or PTSD 135,136 are related to alterations in white matter tracts in military service members. 64,66,135,136 Moreover, our comprehensive approach adds to the existing literature by showing that whole-brain white matter microstructure is associated with overall psychological functioning, independent of mTBI or PTSD diagnosis. This association highlights the essential role of white matter microstructure for psychological functioning in general and, more importantly, suggests a common pathophysiology of psychological symptoms in military service members.
There is a growing research interest in redefining neuropsychiatric diseases as symptomatic expressions of cellular and molecular dysfunctions of brain circuits. 137 The association between white matter changes and psychological functioning can be attributed to the fact that white matter fiber tracts connect various nodes of brain networks involved in psychological functioning. 138,139 Therapeutics that enhance white matter microstructural integrity may thus also facilitate intra- and inter-communication of brain networks and consequently benefit psychological functioning.
Initial evidence of neuroactive steroids as a favorable treatment option for service members comes from a pilot randomized controlled trial with an 8-week course of exogeneous PREGNE administration after mTBI that reported enhanced psychological functioning compared with administration of a placebo. 45 The findings suggest that exogenous supplementation with neuroactive steroids after trauma may benefit brain health and ultimately also benefit psychological outcome. Future research is needed to further investigate the therapeutic potential of neuroactive steroids in the context of brain trauma by also relating the effects of therapeutically administered neuroactive steroids to neuroimaging findings.
Limitations
We acknowledge several limitations of this study. We were not able to separately examine the effect of PTSD because of the very small number of participants with PTSD only (n = 10). Therefore, we cannot entirely rule out that PTSD and not the comorbidity of PTSD and mTBI accounted for some of our findings. Moreover, we were not able to assess differences between participants with PTSD+mTBI and those with PTSD+mTBI+depression given the limited sample sizes. Future research should consider depressive disorders in the relationship between neurosteroids and brain structure.
Similarly, we were not able to assess the effect of current or past military service (e.g., active duty or veteran, branch, deployment, and combat exposure) on our outcome measures because of missing information. Future studies are, therefore, needed to compare neuroactive steroid levels, brain structure, and psychological functioning between military and civilian PTSD and mTBI samples.
Moreover, although the INTruST mTBI screening tool is a validated instrument, the newest gold standard for retrospective TBI assessment post-combat is the Boston Assessment of Traumatic Brain Injury-Lifetime (BAT-L) 140 and the Ohio State University Identification TBI Method (OSU-TBI-ID) 141 for both civilian and military TBI.
Further, we note that diffusion weighted imaging provides only an approximation of neural pathology. However, the correction for extracellular free-water adds to the specificity of diffusion tensor imaging (DTI) metrics. FAT is a more accurate marker of cellular processes than the conventional FA and, therefore, an improved index of white matter health in the living.
It should also be noted that we measured serum levels of ALLO and PREGNE and not CSF levels. Although studies in mice suggest that peripheral markers of neuroactive steroids are adequate proxies for central processes, 142 –144 additional research is needed. Further, ALLO and PREGNE levels might be influenced by factors that we are not accounting for, such as the time point of blood draw, the menstrual cycle phase, 145,146 or oral contraception use in women. 115,147 It is of note that there is some evidence that basal neurosteroid concentrations are higher in women than in men and that neurosteroid concentrations in women are more impacted by stress. 148 The limited female sample size in our study, however, prevented us from examining the sexes independently and should be targeted in future studies. Psychiatric medication use was not consistently assessed. We were therefore not able to control for this potential confounder.
Finally, although we report a relationship between neurosteroid levels and white matter microstructure, the interpretation of causal relationships is limited, given the cross-sectional study design. However, it should be noted that the present study represents one of the most extensive studies investigating the association between neuroactive steroids and brain structural alterations and is consistent with previous research regarding additive effects of mTBI and PTSD on brain structure. 57,63,149 Longitudinal research is needed to further explore the relationship among neuroactive steroids, white matter microstructure, and psychological functioning.
Conclusion
We report that higher neurosteroid levels are associated with increased FAT of the whole brain's white matter. This result underscores previous reports on the neuroprotective effect of neuroactive steroids. Importantly, white matter alterations are associated with worse psychological functioning.
Further, results from this study suggest that comorbidity of PTSD and mTBI may bring the compensatory effects of the brain's stress response to their limit, where lower levels of neuroactive steroids are associated with an even steeper increase in alterations of white matter microstructure. Thus, this study provides insight into what could potentially be a common pathophysiological mechanism underlying the high risk for various psychiatric symptoms and diagnoses in those with PTSD and mTBI: a dysregulated stress response system. Future research is needed to investigate whether neurosteroid regulation may be a promising tool for preserving or restoring brain health and for improving psychological functioning in veterans.
Footnotes
Acknowledgments
The authors thank all study participants and the whole INTRuST consortium for data collection and management.
Author's Contributions
L.F.U. was responsible for conceptualization and design; data curation; formal analysis and interpretation; writing – original draft, review and editing; and visualization. P.R. was responsible for conceptualization and design; data curation; formal analysis and interpretation; writing – original draft, review and editing; and visualization. J.S.H. was responsible for conceptualization and design; formal analysis and interpretation; and supervision, writing – original draft, review and editing. N.S. was responsible for conceptualization and design; writing – original draft, review and editing; and supervision. E.K. was responsible for conceptualization; formal analysis and interpretation; and writing – review and editing. P.K. was responsible for conceptualization; data curation; and writing - review and editing. F.Z. was responsible for methodology; software; and writing – review and editing. J.K. was responsible for conceptualization; formal analysis; and writing – review and editing. M.L. was responsible for formal analysis; and writing – review and editing. C.L.K. was responsible for visualizaition; and writing – review and editing. T.L.T.W. was responsible for visualization; and writing – review and editing. J.D.K. was responsible for acquisition and analysis; and writing – review and editing. J.C.N. was responsible for acquisition and analysis; and writing – review and editing. G.A.G. was responsible for conceptualization and design; acquisition and interpretation; and writing – review and editing. Y.R. was responsible for conceptualization and design; acquisition and analysis; and writing – review and editing. M.J.C. was responsible for conceptualization and design; acquisition and analysis; and writing – review and editing. S.B. was responsible for conceptualization and design; data curation; acquisition and analysis; and writing – review and editing. Y.T. was responsible for formal analysis; software; and writing – review and editing. O.P. was responsible for conceptualization and design; software; acquisition and analysis; and writing – review and editing. M.S.G. was responsible for conceptualization and design; acquisition; and writing – review and editing. T.W.M. was responsible for conceptualization and design; acquisition and interpretation; and writing – review and editing. R.Z. was responsible for concetualization and design; acquisition and interpretation; and writing – review and editing. M.B.S. was responsible for conceptualization and design; acquisition; and writing – review and editing. L.J.O. was responsible for conceptualization and design; methodology; software; and writing – review and editing. C.E.M. was responsible for conceptualization and design; acquisition; formal analysis and interpretation; writing – review and editing; and supervision. M.E.S. was responsible for conceptualization and design; acquisition; analysis and interpretation; writing – review and editing; and supervision. I.K.K. was responsible for conceptualization and design; analysis and interpretation; writing – original draft; review and editing; and supervision. This manuscript is part of the dissertation of L.F.U.
Funding Information
The current research was, in part, supported by the following grants: W81XWH-08-2-0159 (Imaging core principal investigator [PI]: M.E. Shenton; consortium PI: M.B. Stein; Site PIs: M.S. George, G.A. Grant, C.E. Marx, T.W. McAllister, and R. Zafonte), VA Mid-Atlantic MIRECC. Authors were also supported by research grants from the National Institutes of Health (NIH) (R01 MH111671 and R01 NS0860885, R01 NS100952, R01 HD090641), and from European Research Council (ERC Starting Grant 804326).
Author Disclosure Statement
Murray B. Stein has in the past three years received consulting income from Acadia Pharmaceuticals, Actelion, Aptinyx, atai Life Sciences, Boehringer Ingelheim, Bionomics, BioXcel Therapeutics, Clexio, Eisai, EmpowerPharm, Engrail Therapeutics, GW Pharmaceuticals, Janssen, Jazz Pharmaceuticals, and Roche/Genentech. Dr. Stein has stock options in Oxeia Biopharmaceuticals and EpiVario. He is paid for his editorial work on Depression and Anxiety (Editor-in-Chief), Biological Psychiatry (Deputy Editor), and UpToDate (Co-Editor-in-Chief for Psychiatry). Christine E. Marx is a co-applicant on pending patent applications focusing on neurosteroids and derivatives in central nervous system (CNS) disorders. No patents have been issued. No licensing is in place. VA 208 waiver is in place. The other authors report no biomedical financial interests or potential conflicts of interest.