
Abstract
Brain reorganization following spinal cord injury (SCI) has been well-established using animal and human studies. Yet, much is unknown regarding functional recovery and adverse secondary outcomes after SCI. Functional near-infrared spectroscopy (fNIRS) is a neuroimaging technique that offers methodological flexibility in a real-world setting. We used fNIRS to examine the cortical functional differences between 12 males with thoracolumbar SCI (46.41 ± 11.09 years of age) and 12 healthy males (47.61 ± 11.94 years of age) during resting state and task conditions—bilateral finger tapping (FT), mental imagery of bilateral FT with action observation (FTI+AO), and bilateral ankle tapping (AT). We found an overall decrease in hemodynamic response of the SCI group during all three task conditions. Task modulated functional connectivity (FC) computed using beta series correlation technique was compared using independent sample t-tests at α = 0.05. Connectivity between the right mediolateral sensorimotor network (SMN) and the right medial SMN was reduced during the FT task in SCI. A mixed analysis of variance revealed that the FC within the right mediolateral SMN was reduced during FT but preserved during FTI+AO (i.e., comparable to controls) in the SCI group. Lower FC of these regions was associated with longer injury durations. Additionally, we found a general decrease in resting state FC of the SCI group, specifically in the Slow-3 frequency range (0.073 to 0.1 Hz). These results, though preliminary, are consistent with past studies and highlight the potential of fNIRS in SCI and rehabilitative research.
Introduction
According to the National Spinal Cord Injury Statistical Center (NSCISC), approximately 296,000 individuals are living with spinal cord injury (SCI) in the United States as of 2021. 1 SCI occurs when there is damage to the spinal cord, either through an acute traumatic or chronic injury, altering its function. 2 After SCI, the recovery process can be spontaneous or facilitated through physical, pharmacological, or targeted interventional therapies. 3,4 Studies show that repetitive physical therapy can stimulate neuroplasticity in the form of neural rewiring, sprouting, and upregulation of brain-derived neurotrophic factors and neurotransmitters within the central nervous system. 5 Somatotopic reorganization 6 –8 and intrinsic functional reorganization of the sensorimotor cortex—among other regions—have been frequently reported in functional magnetic resonance imaging (fMRI) studies. 9 –11 fMRI has laid the foundation for non-invasively identifying, formulating, and understanding the mechanisms of such neuroplasticity. 9,12 –17 However, the physical constraints of MRI equipment make fMRI challenging for investigating brain functions during mobility and dynamic movements such as gait training or upper extremity manipulation training.
Alternatively, continuous-wave functional near-infrared spectroscopy (fNIRS) is a non-invasive neuroimaging technique that is suited for investigating the neural underpinnings of cortical reorganization and recovery in individuals with SCI in a real-world setting. 18 Continuous-wave fNIRS leverages the optical absorbance properties of oxy-hemoglobin (HbO) and deoxy-hemoglobin (HbR) molecules in the visible and near-infrared frequency range from 650 to 900nm 19 to indirectly quantify neuronal activity based on neuro-vascular coupling. 20 –22 It offers a unique, non-invasive and cost-effective approach to quantifying changes in hemoglobin concentration of the cortex during dynamic tasks. 20,23 Similar to fMRI, fNIRS can be used to study the brain during a stimulus-induced task and resting states, in which individuals are either actively performing a task or simply at rest, respectively. Although fNIRS does not rectify all shortcomings of fMRI and holds a few inherent limitations itself, the advantages include reduced susceptibility to head-motion artifacts, high temporal resolution of 1–2 msec, and effective removal of extra-cerebral noise using short source separation channels. 24 –26
The advantages of fNIRS also allow us to study motor behavior in the SCI population, particularly to examine cortical mechanisms underlying movements involved in rehabilitation. In one clinical trial, fNIRS was shown to successfully monitor the real-time cortical activity during robot-assisted gait training in three individuals with SCI. 27 fNIRS has also gained popularity in studies of traumatic brain injury and stroke to investigate the pathophysiology of cognitive deficits following acquired brain injury. 18 Nagaoka and colleagues have documented that fNIRS can be successfully used as a non-invasive neuroimaging technique to control hand-grasping and motor imagery tasks during electrical stimulation in healthy individuals. 28 Brain-computer interface (BCI) systems for rehabilitative therapy have also utilized fNIRS to support locomotive functions in patient populations with SCI, stroke, and other neurological disorders. 29,30 Additionally, it has been demonstrated that fNIRS can be used to measure significant hemodynamic activity in motor cortical areas of SCI patients during imagined foot movements. 31
Other fNIRS studies using motor paradigms report region-specific differences in the spatiotemporal characteristics of the hemodynamic response to various movements. 32 The ability of fNIRS to investigate the cortical correlates of motor and sensory tasks in real-world settings supports its unique advantages over other imaging technologies for both the prognosis and development of rehabilitative treatments after SCI. As fNIRS systems become more advanced in their mechanical design, an even more compact and portable system may offer rehabilitation studies a simpler imaging modality to simultaneously record cortical activity during regular gait or advanced robot-assisted physical therapy. 33 Thus far, no studies have systematically applied fNIRS to investigate cortical reorganization after SCI.
Therefore, the objective of the current study was to use fNIRS to identify cortical reorganization within the sensorimotor cortex following SCI, during both stimuli-induced task states and resting state. It is hypothesized that somatotopic reorganization after SCI can be detected using an fNIRS-derived hemodynamic response to motor activity. The proposed hypothesis was tested by comparing 12 healthy controls (HCs) with 13 individuals with paraplegic SCI. Alterations in the representation of the unaffected limb in the cortex after paraplegic SCI were evaluated by comparing finger tapping (FT) movement with the movement of the affected limb (by means of an attempted ankle tapping [AT] movement). Additionally, to ensure the cortical differences were, in fact, a result of abnormal brain activity from the injury, FT movement was also compared with an intact motor action (FT imagery) as a control paradigm. It was hypothesized that thoracolumbar SCI would result in reorganization of sensorimotor networks (SMNs) toward intact function, that is, affect cortical activation related to execution of FT but not FT imagery that predominantly involves premotor cortex and supplementary motor area. The findings of this study using fNIRS lay the groundwork for future studies employing flexible task designs to study cortical correlates of movements in neurological populations with lower-body paralysis. Advanced signal processing strategies combined with longitudinal recordings could also expand the application of fNIRS as a therapeutic intervention tool.
Methods
Participants
Thirteen males (2 left-handed, 48.46 ± 12.93 years of age) with SCI and 12 age-matched able-bodied males (1 left-handed, 47.61 ± 11.94 years of age) were recruited for this study (Table 1). Both SCI patients and their able-bodied counterparts were recruited from the Center for Neuropsychology and Neuroscience Research at Kessler Foundation, East Hanover, New Jersey, USA. Patients with SCI with an injury below the cervical level of the spinal cord and healthy control (HC) participants with complete control of their upper and lower extremities were selected for this study. All patients with SCI had intact sensory and motor control of the upper limbs. Eligible participants had no history or current diagnoses of brain trauma, or neurological or psychiatric disorders. All participants could read and write in English. All procedures were performed at the New Jersey Institute of Technology campus and were reviewed and approved by the Institutional Review Board of New Jersey Institute of Technology. All individuals were informed and provided written consent before participation in the study.
Demographics of Individuals With Thoracolumbar Spinal Cord Injury Enrolled in This Study
NA indicates the score is not available.
Participant was excluded due to age outlier.
ASIA, American Spinal Cord Injury Association.
Experimental design
The experimental protocol consisted of: 1) one resting-state run for a duration of 6 min; 2) four runs of motor tasks for 6.3 min each; and 3) one breath-hold task for 5 min. Only the resting-state and motor tasks data sets were analyzed as part of this study. Participants were seated comfortably and were instructed to follow the directions on the computer screen; patients with SCI remained in their wheelchair. During the resting-state run, the participants were instructed to remain awake with their eyes open and fixated on a crosshair on a computer screen. During the motor tasks, the participants were instructed to follow the instructions on the computer screen. The motor tasks consisted of three different task stimuli: bilateral FT, mental imagery of bilateral FT with action observation (FTI+AO), and bilateral AT. Mental imagery of bilateral FT was reinforced with an animation of the same movement on a computer screen to direct the participant's attention toward the motor movement. All participants performed four runs of the tasks in a pseudorandom order, with task block durations of 20 sec interleaved by rest periods of 20 sec (Fig. 1). Whereas the control group executed the AT movement, individuals with SCI were asked to attempt to perform the movement as well as possible.

Schematic of the task paradigm with the tasks color-coded: finger tapping (gray), finger tapping imagery + action observation (red), and ankle tapping (blue). Each task is interleaved with 20 sec of rest and each task block has a duration of 20 sec, with a total duration of 360 sec for each run. Patients with spinal cord injury attempted to perform ankle tapping or ankle dorsiflexion, whereas the control group performed ankle dorsiflexion physically. S, second. Color image is available online.
fNIRS data acquisition
fNIRS measurements were performed using a continuous-wave fNIRS (CW6 system, TechEn, Milford, Massachusetts, USA) system at wavelengths of 690 and 830 nm to quantify changes in HbO, HbR, and the total hemoglobin. A custom 26-channel layout on a Neoprene rubber headpiece was used to place the optodes on each participant's scalp. The optodes were positioned with the help of the Brain Sight neural navigator (Rouge Research Inc.'s Neuronavigation System, Canada) such that the optodes recorded hemoglobin concentration changes from the bilateral premotor, sensorimotor, and prefrontal cortices (PFCs). Based on the anatomical landmarks (left and right ear, nasion, and inion) of each participant, the neural navigator transformed the standard Montreal Neurological Institute (MNI) template of the brain into the expected three-dimensional brain image of each individual subject, which was then used to guide the placement of the optodes onto the scalp. Participant's hair was parted so that the optode was placed in direct contact and perpendicular to the scalp.
The channels were placed according to predefined regions of interest (ROIs) from fMRI literature, such that channel 3 (Source B to Detector 2) and channel 8 (Source D to Detector 5) measured hemoglobin concentration changes from the right and left primary motor cortex or mediolateral SMN (M1), respectively, channels 21 (Source F to Detector 3) and 22 (Source F to Detector 4) measured hemoglobin concentration changes from the supplementary motor area (SMA), and channels 7 (Source A to Detector 7) and 20 (Source E to Detector 12) measured hemoglobin concentration changes from the right and left lateral SMN (Fig, 2A). These ROIs were chosen due to the nature of the tasks and the deficits observed in the SCI population. Out of the 26 channels used, 25 channels were placed at a distance of 30 mm from the source to record cortical hemoglobin concentration changes, whereas 1 channel was placed at a distance of 8.4 mm from the source to record the physiological hemoglobin concentration changes from extra-cerebral tissue such as the scalp and skull. 24 To minimize the influence of ambient light on the fNIRS recording, data collection was implemented with opaque clothing placed over the optodes.
Preprocessing
All analyses were performed using custom scripts in the MATLAB (R2018b) (Mathworks, Natick, MA, USA) platform. The preprocessing pipeline is depicted in Figure 2B, with the following processing procedures conducted within the following order: intensity to optical density conversion, head-motion correction using a wavelet-based algorithm, 34 bandpass filtering from 0.0 to 0.15 Hz for task data and 0.01 to 0.1 Hz for resting-state data, conversion of optical density to concentration using the hmrOD2conc function in the HOMER2 toolbox, 35 and linear temporal regression of the HbO time series of each cortical channel using the physiological channel recording (Channel 23) as a nuisance regressor. The residuals of the HbO time series from temporal regression were then fit using a third order polynomial to remove non-linear drifts. Lastly, the data were corrected for linear drifts and converted to mM units.

(
Individual-level task-based analysis
Hemodynamic response
After preprocessing the task-based data, the average hemodynamic response was quantified using a block-averaging method. It was computed by averaging the HbO concentration changes in the blocks corresponding to a particular motor task—FT, FTI+AO, or AT—from all four runs for each of the 25 channels. A block was defined as the 5 sec before the start of the stimulus, 20 sec of the continuous task stimuli, and 20 sec of rest following the stimuli, with a total duration of 45 sec. Each block was normalized by the 5-sec period before the start of the task block. A block-averaged hemodynamic response was then estimated for each individual, for each task and each channel. HbO concentration changes were used due its high sensitivity to cerebral hemodynamic changes. 19
Task-based functional connectivity
Functional coactivation during the task conditions (i.e. functional connectivity [FC] between regions modulated by the task) were measured using beta series correlation, a technique regularly implemented in task-fMRI data. 36 It calculates the correlations in trial-by-trial activation to a task stimuli. First, it computes the stimulus function for every trial (numerical ones during the duration of the task period and zeros for the rest period), generating as many stimulus functions as the number of trials in a task condition. The stimulus function convolved with a double-gamma hemodynamic response function was then used to model brain activation to a trial where beta activation value was calculated using an ordinary least-squares approach. This was performed separately for every trial (total of 9 trials or stimuli; 3 FT, 3 FTI+AO, 3 AT) in each task run (total of 4 pseudorandomized task runs), yielding a beta series of n = 12 per task condition. The size of the beta series of a particular task condition was equal to the total number of trials corresponding to that task condition in all 4 task runs. Lastly, a Pearson's r correlation of the beta series of each task condition was performed to generate a correlation matrix per task condition in every subject.
Resting-state analysis
Resting-state functional connectivity (RSFC) analysis was performed using the Pearson's correlation coefficient (r-value). Each channel's HbO concentration time-series data was pair-wise correlated with itself and all remaining channels, resulting in a 25 × 25 correlation matrix for each subject. To investigate frequency-dependent activity, the preprocessed data were further separated using a fourth order Butterworth bandpass filter, into the following three frequency ranges: Slow-5 (0.01–0.027 Hz), Slow-4 (0.027–0.073 Hz), and Slow-3 (0.073–0.1 Hz). The values of these frequency ranges were defined based on previous electrophysiological studies investigating the slow oscillations of neural activity. 37,38 The decomposition of resting-state data into different frequency bands allows for greater specificity of information, with RSFC being frequency-dependent on a global brain scale. 37 –40 For each of the three frequency groups, Pearson's r correlation was performed in the same procedure carried out for RSFC of the full-frequency band.
Group-level data analysis
After performing individual-level analyses, group-level analyses were performed to compare differences between the HC and SCI groups. All group-level statistics were carried out using MATLAB (R2018b) (Mathworks).
Hemodynamic response
The block-averaged hemodynamic response curves calculated in the first-level analyses were subsequently averaged across all subjects within each group, for each task and each channel. Each channel was further grouped into the following ROIs based on their anatomical location: right SMN, left SMN, supplementary motor area + medial SMN (SMA + mSMN), and PFC. To evaluate differences in the hemodynamic response of each ROI between HC and SCI groups, a two-tailed independent-samples t-test was performed on the HbOpeak measures for each of the task conditions (FT, FTI+AO, and AT). HbOpeak was defined as the maximum increase in HbO concentration after task onset (i.e., 10–20 sec after task onset) while subtracting the baseline HbO concentration (i.e., 5 sec of rest, and first 10 sec of task). Benjamini and Hochberg's false discovery rate (FDR) correction was implemented at α = 0.0541 to account for multiple comparisons and reduce type-1 errors.
Task-based functional connectivity
Each individual's correlation values were converted to z-scores using Fisher's r to z transformation. An independent sample t-test was performed to identify significant differences between HC and SCI groups for each of the following task conditions: FT, FTI+AO, and AT. Additionally, a mixed analysis of variance (ANOVA) was used to test the mean effect of task conditions (repeated measures), that is, FT and FTI+AO, mean effect of group (HC vs. SCI groups), and their interaction (FT vs. FTI+AO in HC when compared with FT vs. FTI+AO in SCI). Similarly, the aforesaid analysis was repeated to compare the task conditions FT and AT between the two groups. A statistical threshold of α = 0.05 was used for all analyses and Benjamini-Hochberg FDR correction was applied to account for multiple comparisons. Subsequently, for channels with a significant difference in brain activation between HC and SCI groups, a correlation analysis was performed to identify potential relationships between brain activation and duration of injury and level of injury in the SCI group.
Resting-state functional connectivity
The mean correlation matrix was calculated for the SCI and HC groups, by averaging the r correlation values from each channel pair across subjects. Each subject's Pearson's r-scores were then transformed to Fisher's z-scores and an independent-samples t-test was performed between the z-scores of the SCI and HC group, for all channel pairs. To correct for multiple comparisons, the Benjamini-Hochberg FDR procedure was performed at an alpha value of 0.05. Subsequently, the significant channels surviving FDR correction were correlated with the duration of injury for the SCI group. Group-level differences were also evaluated between HC and SCI groups for each frequency range (Slow-5, Slow-4, and Slow-3) in the same protocol as the full-frequency band data (0.01 to 0.1 Hz).
Results
Participants
Of the 13 males with SCI, 1 patient was excluded as an outlier (more than 2 standard deviations [SDs]) due to age, resulting in a total of 12 males (2 left-handed) in the SCI group with a mean age±SD of 46.41 ± 11.09 years. The 12 able-bodied males (1 left-handed, age 47.61 ± 11.94 years) were age-matched with the SCI group. Raw time series and power spectrum of the raw time series were visually inspected before data analysis. All 24 participants exhibited a cardiac component in the raw signal or in the power spectrum of the raw signal and were included for the next steps of the analysis (see Supplementary Figures S1 and S2).
Task-based hemodynamic response
The group averaged hemodynamic response to the three task conditions is provided in Figure 3. An increase in HbO concentration from baseline was observed in the left and right sensorimotor ROIs for all three task conditions of the HC group (Fig. 3A). The SCI group in general exhibited low activity to no activity to the different task conditions, although a net positive response in HbO concentration of a lower magnitude was observed in the left and right SMN and SMA of the SCI group during FT but not the other tasks. The SCI group also appeared to exhibit a small positive response in the SMA + mSMN region during the AT task condition (Fig. 3C). Independent sample t-tests comparing the HbOpeak between the two groups revealed greater HbOpeak during the FT task in the right SMN of the HC group when compared with the SCI group at uncorrected p < 0.05; greater HbOpeak in the SMA + mSMN and PFC regions of the HC group was observed during FTI+AO tasks at uncorrected p < 0.05, although a similar effect was observed for all regions (see Fig. 3B); and greater HbOpeak in the SMA+mSMN region of the SCI group during attempted AT condition at uncorrected p < 0.05.

Block-averaged group hemodynamic response during three types of task protocols in HC and SCI groups for four regions of interest:
Task-based functional connectivity
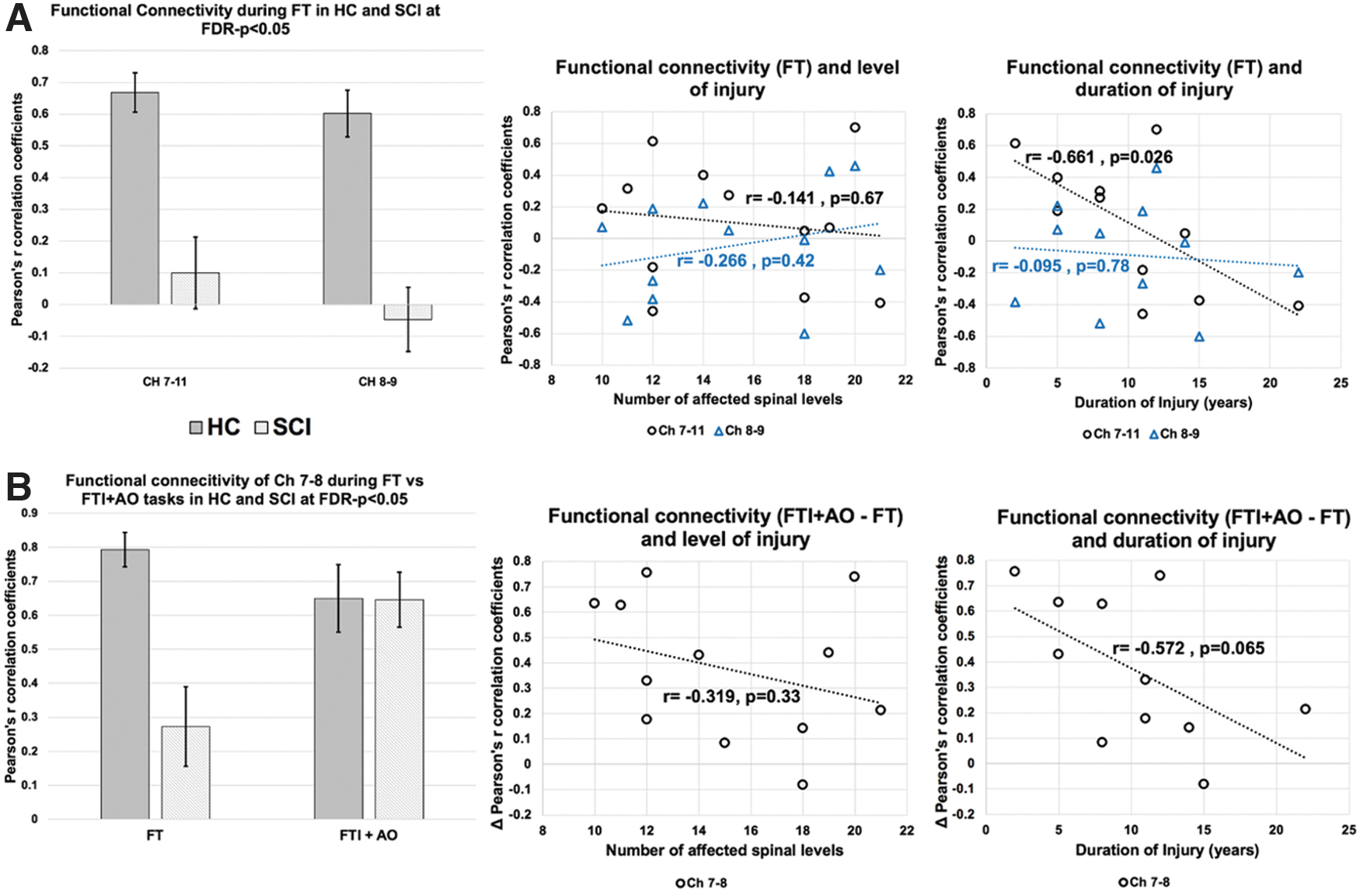
Task-based FC/coactivation of the 300 (k = 25*24/2) channel pairs (shown in Fig. 4A) were compared between the HC and SCI groups for each of the following: FT, FTI+AO, and AT task conditions. Task-based FC within the SMN channels was found to be overall lower in the SCI group during all three tasks (Fig. 4B,C). Particularly, the SCI group had significantly lower FC within the medial SMN, that is, channels 7-11 (uncorrected p = 2.432 × 10−4), and channels 8-9 (uncorrected p = 2.729 × 10−5) during FT task when compared with the HC group at FDR-corrected p < 0.05 (see Fig. 4C). The uncorrected p threshold for FDR-corrected p < 0.05 was 2.432 × 10−4. Similar trends within the SMN were observed between the two groups for the FTI+AO and AT tasks, although none of them survived multiple comparison correction.

Task-based functional connectivity between healthy controls and SCI groups.
The mixed ANOVA results for the interaction effect of group and task conditions is shown in the bottom row of Figure 4C. Interaction between group and task condition of FT versus FTI+AO, which is the difference in execution and imagination of FT movement, showed greater FC within the right medial M1 in the SCI group when compared with HCs. As indicated in Figure 4C, bottom row, the channel pair 7-8 (within right medial SMN) exhibited increased FC during imagination over execution of the FT task (F (2,22) = 21.73, uncorrected p = 1.984 × 10−4, FDR-corrected p < 0.05), whereas the HC group exhibited similar FC of the right medial SMN region during both execution and imagination of the FT task. The uncorrected p threshold for FDR-corrected p < 0.05 was 1.984 × 10−4. A similar effect (not statistically significant after multiple comparison correction) was observed in the mixed ANOVA results for the interaction effect of group and task conditions of AT (i.e., attempted AT in the SCI group) versus FT tasks, in which the SCI group showed greater FC during the attempted AT over FT in the medial and right SMN regions (channel pairs 7-11 and 11-12, respectively), as well as the left SMN (channel pairs 19-20 and 16-20). In contrast, FC between the right SMN and PFC was lower during AT than FT in the SCI group when compared with the HC group.
Further, the connectivity measures of channels with significant differences between the two groups were correlated with duration of injury and level of injury. Duration of injury and FC within medial SMN during FT exhibited a negative relationship (Fig. 5A, r = −0.661, p = 0.026, channel pair 7-11). Likewise, duration of injury and the difference in task modulated FC during FTI+AO versus FT was negatively associated (Fig. 5B, r = −0.572, p = 0.065, channel pair 7-8); that is, longer injury durations in individuals with SCI were associated with lower connectivity/coactivation within the SMN during the FT tasks. It is worth noting that, one patient's injury duration ( = 40 years) was identified as an outlier and was omitted from correlation analysis. Level of injury, which is the number of spinal segments below the level of injury (e.g., for a T5 injury, there are 12 affected spinal segments) showed no significant association with task modulated FC of any region (Fig. 5, middle column, p > 0.05).
(
Resting-state functional connectivity
An overall decreased RSFC was observed in the SCI group compared with the HC group, particularly in the SMN, as seen in the full-, Slow-5, Slow-4, and Slow-3 frequency bands (Fig. 6A). Significant differences were only observed in the Slow-3 category, in channel pairs 10-12 and 10-22, located in the sensorimotor area and SMA, respectively. The mean RSFC scores from both channel pairs were: 0.84 (HC) and 0.48 (SCI) for channel 10-12 and 0.73 (HC) and 0.30 (SCI) for channel 10-22. For channel pair 10-12 (uncorrected p = 2.32*10−4, FDR-corrected p < 0.05) and channel pair 10-22 (uncorrected p = 2.39*10−4, FDR-corrected p < 0.05), the mean RSFC score was significantly lower in the SCI group than the HC group. The uncorrected p threshold for FDR-corrected p < 0.05 was 0.0352. The activity in these Slow-3 channel pairs were correlated with the duration of injury, ranging from 2 to 22 years for the SCI group; however, no significant effects were observed (Fig. 6B) (p > 0.5). As noted earlier, data for one patient were removed as an outlier where the injury duration was 40 years.

(
Discussion
Our study challenged the utility of fNIRS in measuring the cortical hemodynamics following SCI. We examined cortical functional differences between individuals with SCI and age-matched HCs in stimulus-induced task states and resting states, by calculating the hemodynamic response, task-based FC, and RSFC using fNIRS. Overall, patients with SCI exhibited reduced HbO changes in response to the various motor tasks compare with their able-bodied counterparts. Resting-state analysis revealed diminished FC in the Slow-3 frequency bin (0.073–0.1 Hz) within the medial SMN and between medial SMN and SMA regions in the SCI group. Although preliminary in nature, our study demonstrates the feasibility of this technique in detecting neuroplasticity after SCI offering a myriad of opportunities for SCI research including the use of fNIRS in naturalistic movements involved in physical therapy to understand and improve therapeutic strategies.
Our results show a general trend of reduced hemodynamic activity in patients with SCI during tasks involving affected motor function (AT) as well as unaffected motor functions (FT and FT imagination). Although, attempted AT in the SCI group resulted in increased activation in the SMA while a short and reduced HbO response was observed in the bilateral SMN regions (although not statistically significant from healthy controls). fMRI studies of attempted ankle/foot movement report reduced activation magnitude 42 and activation volume 43 in the primary motor cortex associated with ankle movement, with recruitment of secondary regions—such as SMA—in thoracolumbar injuries. 42,44 These findings are contrary to fMRI studies that either report no differences or increased compensatory activation in the primary motor cortex (M1) and secondary association areas. 45 This discrepancy may be attributed to differences in the completeness of injury, level of injury, and duration since injury, among other factors.
Jurkiewicz and colleagues showed progressive reduction of activation in M1 and associated cortical sensorimotor areas in the first year following cervical-level injury in patients who did not regain function. 46 Therefore, the diminished activation we observed in the SMN regions during AT may reflect the progression and level of motor function in these individuals since injury. Of note, none of the patients were able to execute the ankle movement. Nonetheless, increased activation in the SMA with a net positive response to ankle movement in the bilateral SMN regions may reflect possible preservation of descending cortical inputs for initiation of movement with the help of additional secondary sensorimotor regions. Further, FT revealed reduced activation in the bilateral SMN regions of patients with SCI; no differences were noted in SMA or PFC. It is unclear if this results from cortical reorganization, in which there is a spatial displacement or reassignment of activity (finger movement) within the cortex that was not captured effectively by this protocol. Alternatively, one may speculate whether the increased dependency on upper limbs (fingers) in these individuals with lower-body paralysis is associated with a sensorimotor system that is efficient or on overdrive.
Intriguingly, the FT imagination with AO was additionally found to result in positive activation in healthy individuals, whereas this resulted in minimal activity in bilateral SMN, and SMA, and a delayed increase in the PFC of patients with SCI. Imagination while observing the same action has been suggested to more effectively activate the motor executive network and improve rehabilitative training. 47 However, the lack of activity in response to the task in patients with SCI may be explained as the result of poor performance on the imagination task by the SCI group; systemic changes in hemodynamic activity of the SCI group that are linked to non-neuronal factors such as autonomic, and physiological processes; deafferentation and the resulting reorganization affecting the cortical systems involved in both the execution and the imagination of preserved function; and incorrect spatial coverage of cortical areas involved in FTI+AO as observation of a task is thought to primarily activate the visual and visuomotor processing areas. Nonetheless, Batula and colleagues have shown highly similar activation patterns between imagery and execution in lower-limb movement among healthy participants, and that is consistent with the findings reported in this study using fNIRS. 32
Task-based functional connectivity
Task-based FC revealed distinct connectivity patterns during each of the three motor conditions. The SCI group exhibited localized connectivity for all three task conditions as compared with a more widespread connectivity in the HC group. Particularly, the connectivity between right mediolateral SMN and right medial SMN during the FT task was significantly reduced in the SCI group. Somatotopic reorganization following SCI as a result of neuroplasticity has been demonstrated in human and animal studies. 48 Often the regions of M1 and S1 corresponding to the deafferented segments of the body are compensated by adjacent cortical regions encroaching the deafferented limb representation of the cortex. The reduced coactivation/connectivity during preserved function (FT) may reflect the result of M1 regions corresponding to the hand rewiring toward lost function (lower-extremity movement) as a compensatory response. Even though inferences regarding such reorganization may be beyond the scope of the study, our findings using fNIRS demonstrate a distinct spatial response within the SMN to the various task conditions. Further, as hypothesized, these task connectivity measures were negatively correlated with duration of injury, where the longer the injury duration, the smaller the activation in SMN in response to the FT task, potentially due to an overuse of upper body/finger in these patients.
Resting-state functional connectivity
As hypothesized, the overall RSFC was lower for the SCI group than the HC group, although a significant difference was only observed in the Slow-3 category, for channel pairs 10-12 and 10-22. Previous studies found decreased RSFC in various cortical and subcortical regions of SCI populations. 10,49,50 In contrast, an increase in FC has also been observed in the sensorimotor regions of some SCI populations, possibly indicative of successful sensorimotor recovery. 14,51 The inconsistencies in RSFC results across studies of SCI populations is potentially due to several factors including different rehabilitation strategies practiced, duration since injury, and level of injury. This being said, the observed decreases in RSFC of the SCI group can be explained by deafferentation of the spinal cord, which directly affects cortical networks and consequently, functional reorganization. 52
Our RSFC results for the full-frequency band, Slow-5, and Slow-4 categories showed no significant difference after Benjamini-Hochberg's FDR correction at α = 0.05. However, there were significant differences between the HC and SCI groups in the Slow-3 frequency range, in the SMN and SMA. This could suggest that RSFC differences are more pronounced between the HC and SCI groups in specific frequency bands. The frequency-dependent nature of RSFC has been shown in a previous resting-state study investigating five different frequency bands ranging from 0.01 to 0.75 Hz, in which significant variability in resting-state fluctuations across frequency bands was observed. 38 It is important to note that we defined the Slow-3 category to cover frequencies from 0.073 to 0.1 Hz, instead of the range from 0.073 to 0.198 Hz seen in previous studies, due to most resting-state activity being observed from 0.01 to 0.1 Hz. 37,38 The frequency-dependent dynamics of resting-state signals are not well studied using fNIRS; however ,the high temporal resolution of fNIRS may offer new insight into resting-state frequency dynamics. 53 Therefore, our results showing specificity in the Slow-3 frequency band warrant future investigation into different frequency band dynamics in resting-state fNIRS data.
No significant differences were observed after correlating the RSFC (Slow-3 frequency band) with the duration of injury. For the Slow-3 category, activity in the significant channel pairs (significantly different between HC and SCI) showed no significant correlation with the SCI group's duration of injury. More research is warranted because this may not fully represent the relationship between RSFC and duration of injury in individuals with SCI, because only two significant channel pairs were used. A study by Hawasli and colleagues showed increased connectivity between the cerebellar cortex and both the primary motor and sensory cortices over time, suggesting reorganization of resting-state networks over time, post-injury. 49 To further assess the association between RSFC and injury duration of the SCI population using fNIRS, longitudinal studies are suggested.
Implications for spinal cord injury research
Compact and non-ionizing nature, relatively lower cost, and ease of use by both clinical and research personnel in clinical and real-world settings make fNIRS a unique neuroinvestigative tool for patients with SCI, paralysis, stroke, and other human motor disorders. Firstly, fNIRS may be used to understand the neuropathology of the injury and secondary complications such as neuropathic pain, autonomic dysfunction, phantom limb syndrome, cognitive dysfunction, and so forth. Unlike fMRI, patients may stay sitting, standing, or supine during scans. This is important in populations such as SCI, where autonomic dysfunction and improper blood pressure regulation are common. Further, current advances in wearable fNIRS technology enable its use in challenging and constrained settings such as during physical therapy. NIR SPORT 2 (NIRx Inc., Germany), Brite MkII (CORTECH solutions), and the NIRSIT system (Soterix Medical) are examples of wearable wireless NIRS systems. fNIRS may be used in conjunction with conventional physical therapy such as gait training, treadmill training, etc., as well as robotic-based approaches such as gait training with exoskeletons to evaluate therapy efficacy and mechanisms of recovery to maximize benefit. The same may be feasible for modulation techniques such as functional electrical stimulation, transpinal stimulation, epidural stimulation, and other avenues of treatment development in these patients.
However, we recommend future studies to consider the potential confounds in designing an fNIRS study for an SCI population, namely: 1) the variation in pulmonary and cardiovascular physiology in sitting versus standing position that could be mitigated by concurrent physiological measures such as heart rate variability, blood pressure, oxygen saturation, etc.; 2) autonomic dysfunction contributing to systemic cerebrovascular changes that could be measured using vasoactive tasks; 3) between-subject differences introduced due to variability in task performance and the use of passive tasks and non-sensorimotor tasks as control in complete injury; 4) inter-subject differences in injury characteristics, particularly the injury duration, injury level, and completeness; and 5) spatial differences in activation by use of a distributed probe layout.
Limitations
It is important to note a few limitations of this study. Only three patients had an incomplete SCI; differences based on the completeness of injury were not evaluated in the current study. The socioeconomic status (SES) of the participants recruited was not collected. It is thus impossible to determine the impact of SES on study results. SES is an important factor to consider in future research as it contributes to health disparities among racial/ethnic minorities, women, and the elderly. 54 Although no SES scores were recorded from participants, the HC and SCI groups were recruited from the same center and were age- and sex-matched to reduce possible confounding variables.
Another limitation of this study is the imbalance between the number of males and females recruited. Due to the higher incidence rates of SCI among males—approximately 80% occurring in males between 25 and 45 years of age 55 —our recruitment efforts were limited by population demographics. To further study sex differences after SCI, it is critical to include both males and females in pre-clinical SCI research in particular, in which there is better control over biological variables. 56 Additionally, the differences in task performance were not recorded or accounted for in the task analyses, limiting the interpretability of task-induced outcomes. Finally, this study is limited by the relatively low number of fNIRS channels covering the cortex, which limits spatial inference. As fNIRS devices experience advances in hardware, such as the development of high-density fNIRS, 57,58 spatial inference of neurovascular activity can be improved.
Conclusions
The current results suggests that cortical functional differences between individuals with SCI and age-matched HCs in the performance of different motor tasks involving physically executed movements and imagined/attempted movements can be detected using fNIRS. No significant differences were found in the full-frequency resting-state FC between the SCI and HC groups, although overall connectivity was decreased in the SCI group. These findings provide valuable insight into the supraspinal pathology of SCI. Importantly, findings indicate that fNIRS, currently popular in traumatic brain injury and stroke research, may be an effective neuroimaging modality to evaluate individuals with SCI as well. Considering the applicability and translatability of fNIRS is tremendous due to the portability and robust performance, validating the technique would benefit not just SCI but other motor disorders requiring rehabilitation, neonatal research, space research, and so forth.
Footnotes
Data Availability
Data will be made available upon request to the corresponding author.
Acknowledgments
Portions of this article are published as part of the doctoral dissertation of KDK.
Authors' Contributions
The authors contributed as follows. Keerthana Deepti Karunakaran: conceptualization, methodology, software, formal analysis, investigation, writing–original draft, funding acquisition; Donna Y. Chen: software, formal analysis, writing–original draft; Katherine Ji: methodology, formal analysis, writing–review and editing; Nancy D. Chiaravalloti: resources, writing–review and editing, supervision; Bharat B. Biswal: conceptualization, writing–original draft, funding acquisition, resources, supervision, project administration.
Funding Information
This study was funded by a fellowship from the New Jersey Commission on Spinal Cord Research (NJCSCR; CSCR15FEL002) to KDK and BBB.
Author Disclosure Statement
No conflicting financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.