
Abstract
The rationale of performing surgery for acute subdural hematoma (ASDH) to reduce mortality is often compared with the self-evident effectiveness of a parachute when skydiving. Nevertheless, it is of clinical relevance to estimate the magnitude of the effectiveness of surgery. The aim of this study is to determine whether surgery reduces mortality in traumatic ASDH compared with initial conservative treatment. A systematic search was performed in the databases IndexCAT, PubMed, Embase, Web of Science, Cochrane library, CENTRAL, Academic Search Premier, Google Scholar, ScienceDirect, and CINAHL for studies investigating ASDH treated conservatively and surgically, without restriction to publication date, describing the mortality. Cohort studies or trials with at least five patients with ASDH, clearly describing surgical, conservative treatment, or both, with the mortality at discharge, reported in English or Dutch, were eligible. The search yielded 2025 reports of which 282 were considered for full-text review. After risk of bias assessment, we included 102 studies comprising 12,287 patients. The data were synthesized using meta-analysis of absolute risks; this was conducted in random-effects models, with dramatic effect estimation in subgroups.
Overall mortality in surgically treated ASDH is 48% (95% confidence interval [CI] 44–53%). Mortality after surgery for comatose patients (Glasgow Coma Scale ≤8) is 41% (95% CI 31–51%) in contemporary series (after 2000). Mortality after surgery for non-comatose ASDH is 12% (95% CI 4–23%). Conservative treatment is associated with an overall mortality of 35% (95% CI 22–48%) and 81% (95% CI 56–98%) when restricting to comatose patients. The absolute risk reduction is 40% (95% CI 35–45%), with a number needed to treat of 2.5 (95% CI 2.2–2.9) to prevent one death in comatose ASDH. Thus, surgery is effective to reduce mortality among comatose patients with ASDH. The magnitude of the effect is large, although the effect size may not be sufficient to overcome any bias.
Introduction
Three hundred per 100,000 persons are admitted with traumatic brain injury (TBI) yearly. 1 Of those, 20% has an acute subdural hematoma (ASDH), which is one of the most important causes of the high mortality and substantial morbidity in TBI. 2 Surgical evacuation is considered the cornerstone of treatment but associated with strong practice variation. 3 The evidence level of the effect of surgical evacuation does not rise above class III (Brain Trauma Foundation [BTF] classification of evidence 4 ) and is based mainly on uncontrolled cohorts or case series. 2
A systematic review with or without meta-analysis has never been performed. The most recent review is from 1997 and was not performed systematically. 5 Neurosurgical interventions are seldom based on level I/II evidence. 6 There is a lack of comparative studies that are properly designed to estimate the effectiveness of surgery. In ASDH, neurosurgeons are reluctant to randomize surgery. 7 It is considered unethical because it potentially withholds a lifesaving treatment and common sense can be applied to deduce its effectiveness. Some make the analogy with the effect of a parachute when jumping from a plane. 8
In an effort to integrate obvious effects with evidence-based medicine (EBM), Glasziou and associates 9 coined the term “dramatic effect” and explored methods to infer causality of several interventions. 9 This approach has also been applied in neurosurgery. The effect of surgery in epidural hematoma (EDH) was determined in a meta-analysis using a historical control group. 10 The Oxford Centre for Evidence Based Medicine has proposed to upgrade observational studies with a dramatic effect to a higher evidence level. 11 Whether surgery for ASDH can be seen as a dramatic effect for which bias is unlikely to explain its apparent effect remains to be determined.
The question of this study is whether a surgical strategy (i.e., evacuation by craniotomy [CR] or decompressive craniectomy [DC]) leads to lower in-hospital mortality compared with (initial) conservative treatment in ASDH. Our hypothesis is that mortality in comatose (Glasgow Coma Scale [GCS] ≤ 8) patients with ASDH is high for conservative treatment and much lower for surgery. A large difference between mortality risks, in combination with an end-point that is not prone to misclassification, would provide robust evidence for which the common sense parachute analogy applies. 10,12 The underlying concept is that the effect will probably be very large and thereby outweighs any practically conceivable bias.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses were followed. 13 The review protocol was pre-registered on PROSPERO (registration number CRD42015025491). It was prepared as start of a living systematic review (LSR) of the CENTER-TBI project. 14 The LSR was performed separately, with the Glasgow Outcome Scale (Extended) as outcome and was started in 2016 (PROSPERO CRD42019125336).
Search strategy and selection criteria
To find studies on mortality risks in surgical and conservative ASDH, we searched English and Dutch publications in the databases IndexCAT, PubMed, Embase (OVID-version), Web of Science, Cochrane library, CENTRAL, Academic Search Premier, Google Scholar, ScienceDirect, and CINAHL. The search string focused on traumatic ASDH, cranial surgery, conservative management and outcome, and was devised with a trained librarian (JS).
We did not restrict the search to a publication date, because reports on the natural history of ASDH were estimated to be mostly available in very old literature. The search dates from September 19, 2019 (Supplementary Material 1). For studies describing cohorts with either treatment strategy only, we truncated the search at 2016. The LSR started in 2016 and focused on traditional meta-analysis to infer effectiveness. Therefore, from 2016 onward, we only included studies with both treatment groups.
Original studies were eligible if they met the following criteria: (1) a cohort study or a trial with at least five patients with traumatic ASDH, clearly describing surgical, conservative treatment or both with (2) description of the in-hospital mortality. Studies with patients younger than age 16 or with posterior fossa or interhemispheric ASDH were excluded. Case series were not considered because these do not allow calculation of absolute risks. 15 Studies with outcome-based sampling—for example, in studies in which ASDH is diagnosed post-mortem—will be excluded. We included studies with exposure (surgical or conservative treatment) based sampling.
The citations were downloaded into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). The initial study selection on abstract and title was independently performed by two authors (TvE, NvdG). Full texts were reviewed by three authors (TvE, LR, NvdG). Discrepancies were solved by consensus. We did not treat the absence of a stated aim, an unclear aim, or an aim discordant from our systematic review as exclusion factors.
Definitions
We used the BTF's definition of ASDH: every patient within two weeks of head injury and a diagnosis of a subdural localized hematoma (either on computed tomography [CT], by angiography, by other radiological examinations [including air ventriculography] and/or by surgery). 2 Subacute or chronic subdural hematomas were not considered.
Pragmatic definitions for a primary surgical and conservative treatment strategy were used by adhering to the definition of the study in question. A surgical strategy, however, had to include at least: (1) a CR or a DC to evacuate the hematoma and (2) initiated within 24 h of presentation or, when no time window was reported, surgery directly after the first CT that revealed the ASDH. A conservative strategy is any hospital admittance with associated medical interventions without a CR or a DC within 24 h of presentation or after the first CT with optional secondary CR or DC in case of secondary deterioration after 24 h.
Because the presentation of ASDH is clinically heterogeneous, we regarded several outcome predictors relevant: Clinical parameters: age, level of consciousness as an indicator of TBI severity (mild and moderate (GCS >8), mixed, severe (GCS ≤8)), pupillary reactivity (abnormal or non-reactive to light, normal); Radiological parameters: thickness of the ASDH, the severity of midline shift, other intracranial lesions (e.g., contusions); Process parameters: time to hospital, time to operation (either from injury or from hospital).
If two of three parameters were completely described, the article was qualified as adequately reporting relevant prognostic characteristics.
Data extraction and risk of bias assessment
Data were independently extracted by two authors (LR, TvE). Discrepancies were resolved by consensus. The following data were extracted: study design, presence of a comparison group, sample size, in-hospital mortality, inclusion and exclusion criteria, age, GCS score, anticoagulant use, concomitant intracranial hematoma/contusion, proportion surgically treated (in case of comparative studies), operation type (DC, CR, and/or burr-hole), report on relevant outcome predictors, and CT diagnose of ASDH. Further, we extracted whether the cohort of patients consisted of a subpopulation.
Risk of bias was assessed by an adapted MINORS instrument. 16 The “low risk of bias” requirements were: (a) ascertainment of exposure by CT, (b) consecutive inclusion, (c) prospective data collection, and (d) adequate description of prognostic characteristics (see Definitions). In (comparative) studies containing both treatment groups, additional criteria for low risk of bias were: (e) contemporary groups (no historical comparison), (f) baseline equivalence of groups, and (g) adequate adjustment for confounders. At the end of this process, we allocated each study to a dichotomic qualitative score low risk of bias “yes” or “no,” instead of the original quantification of the risk of bias from MINORS, because numerical representation of the components may be misleading. 17
Statistical analysis
The pooled mortality risk (proportion) was the outcome measure. Mortality was stratified on publication date (before vs. after CT-era), age categories, and presenting consciousness level (motor score 6/GCS >8 vs. motor score <6/GCS ≤8). After assessment of risk of bias and study heterogeneity, pooled estimates of, respectively, the proportions of the surgical and conservative cohorts and of the effect measures (i.e., relative risks, odds ratios) from the comparative studies were obtained.
The pre-defined plan for meta-analyses: The first strategy assumed a dramatic effect (of surgery on death) by comparison with estimations from historical cohorts. The assumptions are (1) an objective outcome measure, not prone to misclassification, (2) a high mortality risk in untreated subjects confirmed by multiple cohorts, and (3) a much lower mortality risk in surgically treated subjects in multiple cohorts. The pooled mortality risk of the surgical cohorts was compared with that of the conservative cohorts by use of the absolute risk reduction (ARR), relative risk (RR), and the numbers-needed-to-treat (NNT) to quantify the effect of surgery on mortality. 10
We sought to provide these effect measures specifically for the comatose subgroup (GCS
The second strategy was a (conventional) meta-analysis with pooling of effect estimates. Pooled estimates were obtained when studies were termed low risk of bias.
Meta-analyses for effect estimates and for proportions were performed using the metan and metaprop commands 18,19 in Stata 14 (Stata Corp., College Station, TX) in random-effects models.
Results
Study characteristics
One hundred and two studies were included involving data from 12,287 patients (Fig. 1): seventy cohort studies of surgically treated ASDH, 11 cohort studies of natural history/conservatively treated ASDH, and 21 studies containing both surgically and conservatively treated patients (Tables 1, 2, 3 in Supplementary Material 2). 20 –121 Consequently, there were 91 surgical cohorts and 32 conservative cohorts of which the natural history of ASDH can be inferred. All studies considered, mortality risk was 46% (95% confidence interval [CI] 42–51%).
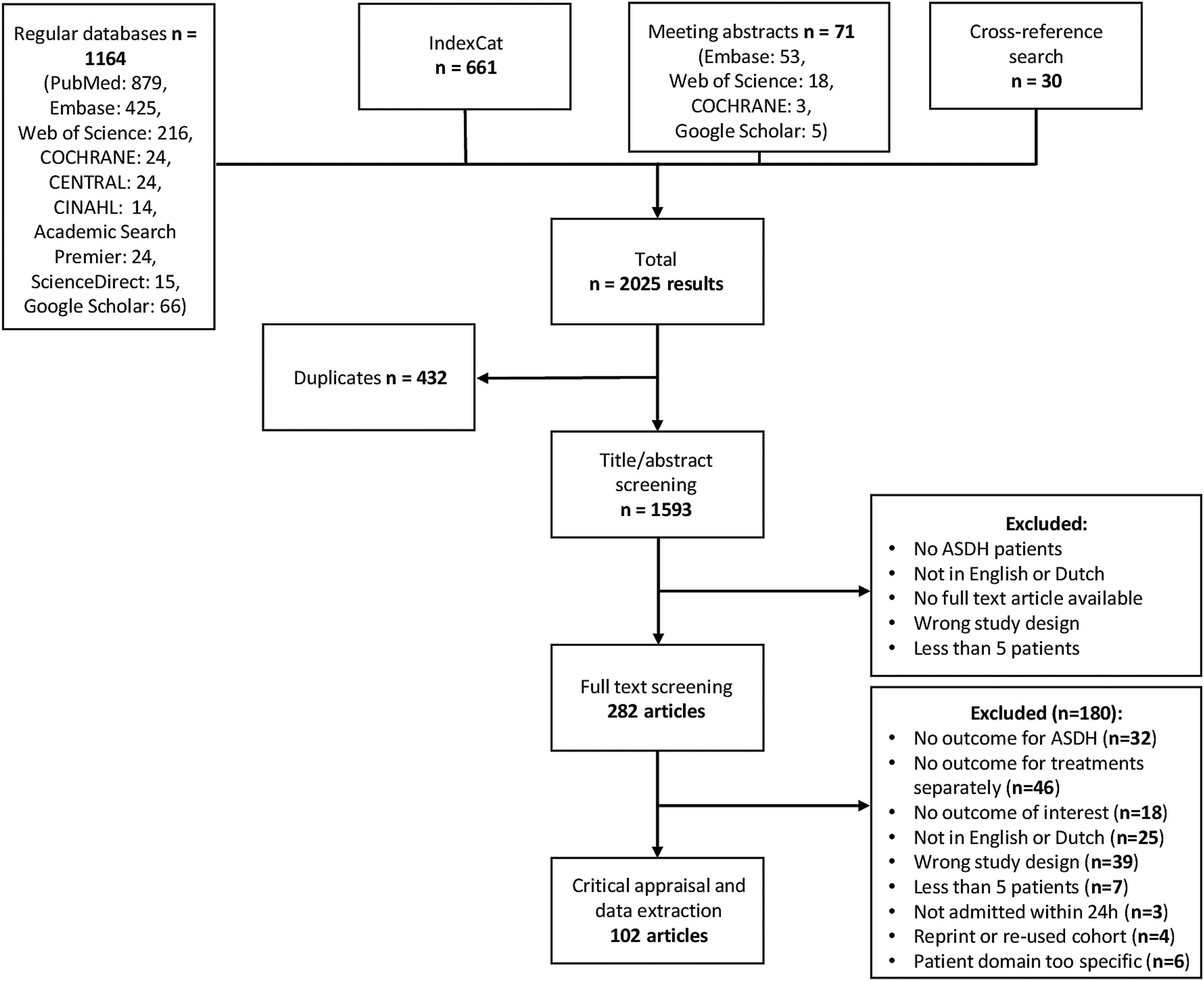
Flow diagram of screened, included, and excluded studies. ASDH, acute subdural hematoma.
Risk of bias and heterogeneity
Four of the conservative cohorts (13%) had a low risk of bias compared with eight surgical cohorts (9%) (Table 1, 2, and 4 in Supplementary Material 2). None of the studies containing both groups had a low risk of bias (Table 3 and 4 in Supplementary Material 2). Visual (qualitative) assessment of the wide variability in the reported mortality risks of the studies in the forest plots showed substantial between-study heterogeneity.
Mortality in surgically treated patients with ASDH
The overall mortality in the surgery group was 48% (95% CI 45–52%). Patients younger than age 30 and older than age 60 had a lower mortality (respectively, 19% and 31%) than patients between 30 and 60 years (44% and 54%, respectively, for 31–45 and 46–60 years, Fig. 1 in Supplementary Material 2).
There were two surgical cohorts for non-comatose ASDH. In these studies, patients had a GCS score between 11–15, and the pooled mortality was 12% (95% CI 4–23%). Thirty-one studies in comatose patients with ASDH showed a pooled mortality of 51%, 95% CI 45–58 (Fig. 2 in Supplementary Material 2). Pooled mortality for (surgical) ASDH in studies without restriction to TBI severity (i.e., GCS score 3–15) was 45% (95% CI 38–51, Fig. 3 in Supplementary Material 2).
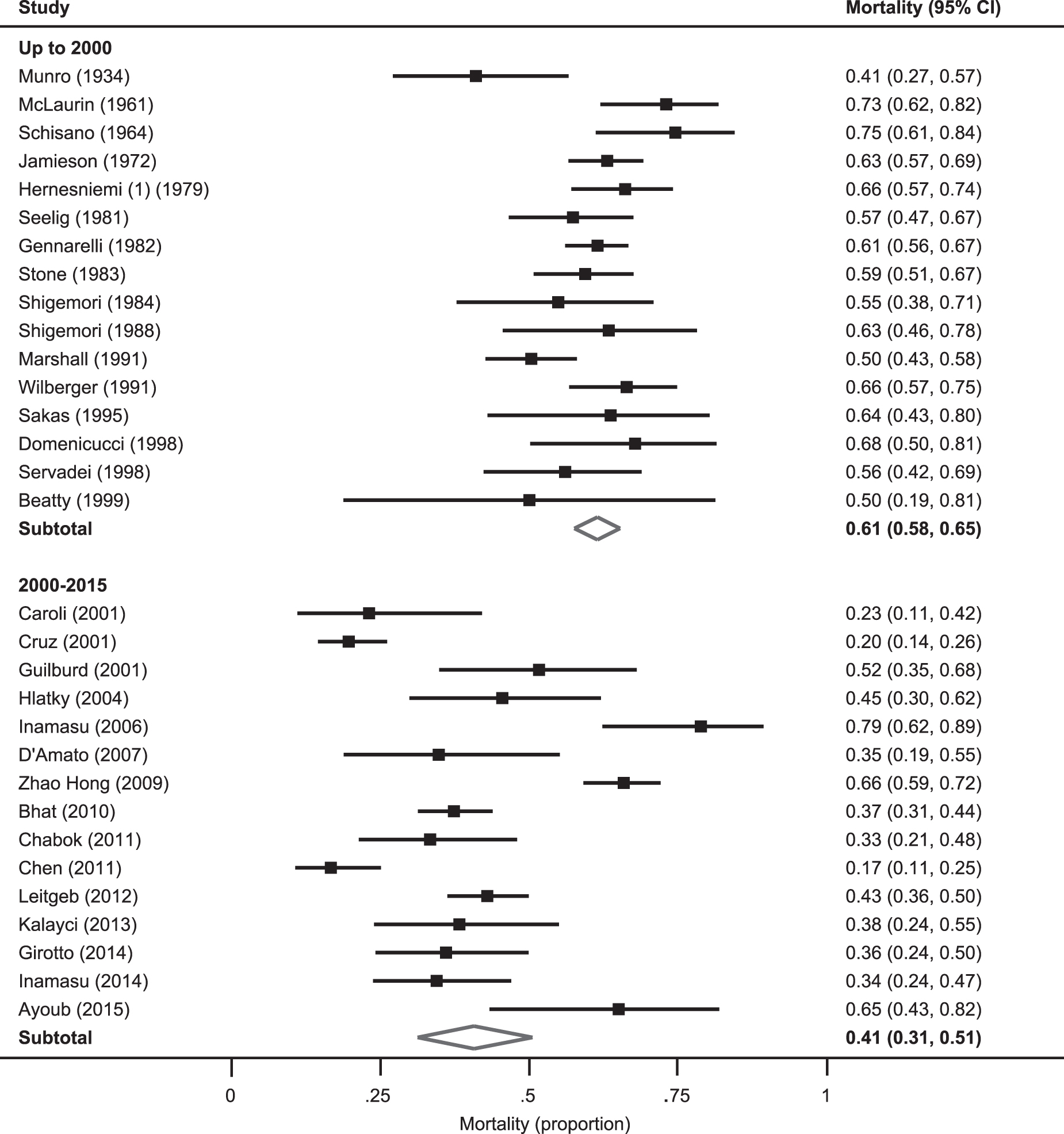
Historical and contemporary mortality risks in surgically treated comatose patients with acute subdural hematoma. The squares and horizontal lines correspond to the mortality risks with 95% confidence intervals (CIs). The diamond represents the pooled mortality risk and 95% CI of the subgroup population.
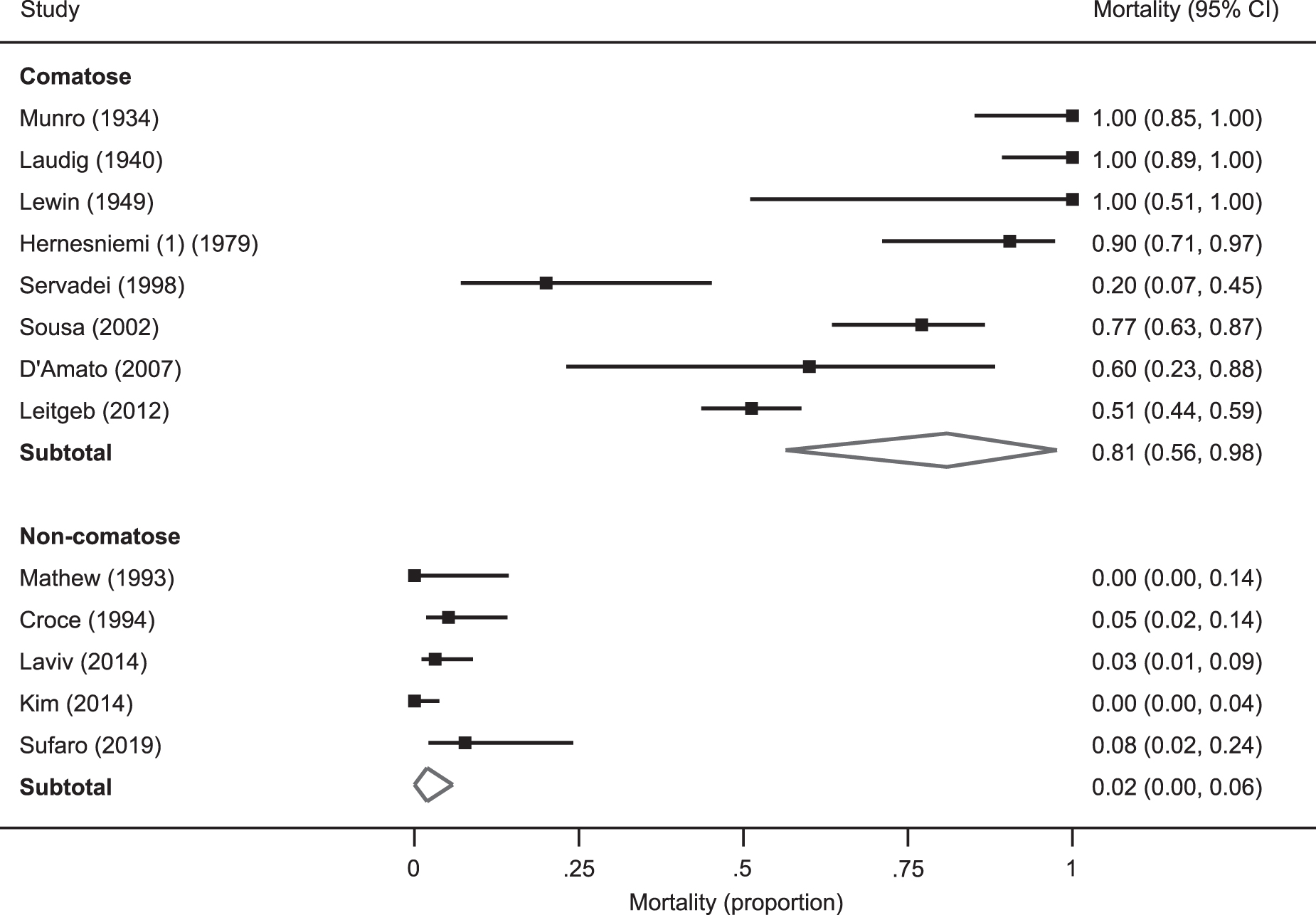
Mortality risks of the natural history or conservative treatment of comatose and non-comatose acute subdural hematoma patients. The squares and horizontal lines correspond to the mortality risks with 95% confidence intervals (CIs). The diamond represents the pooled mortality risk and 95% CI of the subgroup population.
Mortality before the CT era was 59%, and in studies with a CT diagnosis of ASDH, mortality risk was 45% (Fig. 4 in Supplementary Material 2). Surgery for comatose patients with ASDH in more recent studies (after 2000) is associated with a pooled mortality of 41%, while mortality risk was 61% in studies before 2000 (Fig. 2).
Mortality risk after conservative treatment of ASDH
The overall mortality risk after conservative treatment was 35% (95% CI 22–48%), inferred from studies describing the natural history of ASDH and studies of conservatively treated comatose ASDH. Pooling comatose patients with ASDH with conservative treatment resulted in a mortality risk of 81% (95% CI 56–98%, Fig. 3), while in studies after 2000, conservative treatment is associated with a pooled mortality of 64% (95% CI 41–81%). Pooled mortality in conservatively treated non-comatose patients with ASDH was 2% (95% CI 0–6%, Fig. 3). Pooled mortality of ASDH conservative management in mixed GCS cohorts was 26% (95% CI 13–40%, Fig. 5 in Supplementary Material 2).
Treatment effect
The absence of studies with a low risk of bias as well as the considerable between-study heterogeneity, as can be inferred from the widely varying mortality risks, do not allow meta-analysis of effect estimates. Moreover, among the studies with both cohorts, there were no comparative studies that presented effect measures.
The mortality risk associated with the conservative treatment of comatose ASDH patients was 81% (Fig. 3). Compared with the mortality of modern surgery in comatose patients with ASDH of 41%, this translates to an ARR 40% and a NNT of 2.5 (Table 1).
Summary Statistics of the Effect Measures of Surgery for Acute Subdural Hematoma
ASDH, acute subdural hematoma; CI, confidence interval; ARR, absolute risk reduction; RRR, relative risk reduction; NNT, number needed to treat.
Restricting the historical control group to after 2000 as well leads to an ARR of 23% (95% CI 13–32%) and a NNT of 4.3 (3.1–7.7). Finally, without restricting to time period leads to 81 versus 51% with an ARR of 30% (95% CI 24–36%) and a NNT of 3.3 (2.8–4.2).
Discussion
Despite surgery, ASDH is associated with poor outcome.
We assumed a strong effect of surgery to determine the relation of surgery and mortality in ASDH. The validity of our conclusion relies on whether our effect is dramatic enough that confounding and immortal time bias can be sufficiently ruled out. The magnitude of the effect is large, although not as large as surgery for EDH (ARR 74%) or as for a parachute when skydiving (ARR 86%, Table 2).
Summary Statistics of the Effect Measures of Surgery for Epidural Hematoma and Parachute in Free Fall
EDH, epidural hematoma; ARR, absolute risk reduction; RRR, relative risk reduction; NNT, number needed to treat.
Adapted from. 10
Acute subdural hematoma is more debilitating than EDH because of underlying primary brain damage, and even after (modern-day) surgery, the mortality risk is high. Glasziou and associates 9 and Nelson and colleagues 10 propose a risk ratio (RR) of at least 10 and an ARR of 50%, respectively, to qualify as a convincing difference to claim a treatment effect. Even when the mortality risk of the natural history of ASDH would be 100%, these dramatic effect thresholds would not be reached with a RR of 2.4 and an ARR of 59%. According to these conventions, surgery for ASDH would qualify but with low confidence.
The type of control group influences the effect size. When restricting the conservative treatment estimate to after 2000, the ARR was 23%. This difference is not considered a dramatic effect beyond doubt and can be explained by bias. The clinical decision for conservative treatment in these three studies, however, was (well) reasoned—i.e., strong confounding by indication—resulting in a selected subgroup (not neurologically deteriorating patients with small ASDH and normal increased intracranial pressure [ICP]). This control group is therefore less appropriate.
The type of control group requires balancing between an accurate reflection of curative ability of conservative management against highly selected populations of comatose patients amenable to conservative management. By including studies performed before the widespread use of CT, we are exploiting the pre-CT era's inability to fully appreciate the strong curative potential of surgical evacuation. By combining those with modern conservative cohorts, we aimed to obtain an accurate reflection of conservative treatment mortality risk of comatose ASDH.
Is this study a mere exercise in epidemiological theory and unnecessary complex rendition of common sense? In other words, what are the implications of our results? First, our results demonstrate that surgical evacuation of ASDH is an effective intervention. The TBI guidelines should reflect the consensus that observational studies with a dramatic effect should be regarded as level-2 evidence, similar to randomized trials. 11
It may be argued that there is no need for additional study into the effect of surgery in comatose patients in terms of
Although ASDH is seen as a progressive condition with a certain death, it probably should be seen as spontaneous remitting. In contrast to EDH, ASDH is often of venous origin instead of arterial, perhaps making a good clinical outcome possible after expectant management. After all, chronic subdural hematomas arise from liquefication of an ASDH—albeit without or little symptoms mostly. Some of the included studies confirm this satisfactory prognosis of conservative treatment of comatose patients with ASDH patients. Thus, at least in certain comatose ASDH subgroups, randomized trials are defendable.
Second, this study does not support the notion that older patients have a worse outcome. A possible explanation, though, could be selection bias where older patients are deceased before hospital admission and therefore not included in any study. The current results, however, are in line with clinical experience that older patients often have an isolated ASDH without contusion as a result of a low energetic head trauma that may respond well to an early evacuation with a small craniotomy or conservative treatment with watchful waiting and eventually a delayed burr hole drainage.
Third, this study highlights the improved care for patients with ASDH over the past century. The targeted and efficient craniotomy and DC to manage severe TBI and ASDH have coincided with the evolution of trauma care systems. Advances in neurocritical care and the widespread introduction of CT scanners and ICP monitors have decreased mortality rates for patients with severe TBI dramatically in modern well-resourced hospitals.
Fourth and final, the effect of surgery in moderate TBI could not be estimated because cohorts restricting to moderate TBI were not available. The probable positive effect, however, exerts its influence mostly in terms of functional outcome because the in-hospital mortality risk of conservatively treated non-comatose ASDH already is relatively low with 2%.
This is the first systematic review of ASDH surgery. A strength is that it profits from an exhaustive search of ASDH studies with an overview spanning 120 years of ASDH care. Limitations are the restriction to death as outcome and the broad eligibility criteria, leading to strong between-study heterogeneity. Further, the study may have suffered from (positively skewed) publication bias; ASDH is associated with poor outcome, which can lead to underpublication of cohorts with a less favorable outcome.
This report provides a reference for studies into the effectiveness of surgery for ASDH. Apart from surgery for comatose ASDH in terms of mortality, surgery in ASDH is of unclear benefit. Wide practice variation confirms this statement. 7,122 Subgroups such as patients with moderate TBI and the elderly warrant high-quality comparative studies. In addition, the effect of surgery on functional outcome and quality of life requires further investigation.
Conclusion
By comparing contemporary surgical treatment with the natural history of ASDH in a systematic review of the mortality risk, surgery seems to reduce death among comatose patients with ASDH almost twofold. This finding integrates common sense—i.e., obvious effects—with EBM standards, although the effect size may not be sufficient to overcome any bias.
Footnotes
Acknowledgments
We would like to thank Kyle S. Nelson, Ann M. Brearley and Stephen J. Haines for their study “Evidence-based assessment of well-established interventions: the parachute and the epidural hematoma” (Neurosurgery 2014;75:552–559) that served as an inspiration for the current study. Portions of this work were presented orally as a plenary lecture at the European Association of Neurosurgical Societies (EANS) Congress, Dublin, Ireland, in 2019.
Authors' Contributions
Authors TvE and NG conceived and designed the review. The literature search was devised by TvE and JS. TvE and LR performed study screening for inclusion, data extraction, assessment of risk of bias, and selection of studies for inclusion in meta-analyses. Full texts were reviewed by three authors (TvE, LR, NvdG), and any disagreements were settled by these same authors. Analysis of the data was performed by TvE and LR. All authors contributed to the review protocol, methodological decisions, and manuscript.
Transparency,Rigor,and Reproducibility Summary
The data, which include individual study data, a database with a data dictionary defining each field and the Stata syntax, are available on reasonable request. The pre-defined study protocol has been published (PROSPERO [registration number CRD42015025491])
Funding Information
The authors' work on this study is funded by the Hersenstichting Nederland (the Dutch Brain Foundation, grant number ps2014.06) for the Dutch Neurotraumatology Quality Registry (Net-QuRe) and the European Union seventh Framework Program (grant 602150) for CENTER-TBI.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Material 1
Supplementary Material 2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.