
Abstract
We prospectively evaluated a panel of seven blood biomarkers (S100 calcium-binding protein B [S100B], neuron specific enolase [NSE], spectrin breakdown products [SBDP], ubiquitin C-terminal hydrolase L1 [UCHL1], glial fibrillary acidic protein [GFAP], neurofilament light chain [NFL], and tubulin-associated unit [Tau]) for sport-related concussion (SRC) in a large multi-centric cohort of 496 professional rugby players from 14 French elite teams. Players were sampled twice during the season (beginning and end) away from any sport practice. From these two baseline samples, we evaluated the intra-individual variability to establish the effect of rugby on blood biomarkers over a season. Only S100B and GFAP remained stable over the course of a season. During the period of the study, a total of 45 SRC cases was reported for 42 players. In 45 SRCs, the head injury assessment (HIA) process was performed and blood collection was realized 36 h after the concussion (HIA-3 stage). For each biomarker, raw concentrations measured 36 h after SRC were not significantly different between players with a non-resolutive SRC (n = 28) and those with a resolutive SRC (n = 17; p between 0.06 and 0.92). In a second step, blood concentrations measured 36 h after SRC were expressed according to the basal concentrations as an individual percentage change (PCH36[%]), calculated as follows: PCH36 = 100 × (([Biomarker]36h - [Biomarker]basal)/[Biomarker]basal). S100B and NFL concentrations expressed as PCH36[%] were significantly different between non-resolutive and resolutive SRCs (p = 0.006 and 0.01 respectively), with a positive delta found in non-resolutive SRCs. Among the two biomarkers, it is important to note that only the S100B protein was stable during the season. In the context of our study, during HIA-3 assessment, S100B seems to perform better than NSE, SBDP, UCHL1, GFAP, NFL, and Tau as biomarker for SRC. From a clinical standpoint, the S100B modification over baseline may be valuable, at 36 h after concussion to distinguish non-resolutive SRC from resolutive SRC.
Introduction
Rugby, a popular full-contact sport played worldwide, has one of the highest rates of concussions of all full-contact sports. 1 Over the past years, the incidence of reported concussions in 15-player-a-side rugby has increased from ∼4 to ∼13 concussions/1000 player-match hours. 2 Failure to manage sport-related concussion (SRC) in athletes can lead to further, potentially devastating insults to the brain; evidence shows an increased risk of neurological deficits when athletes return to play prematurely with an undetected or unresolved SRC. 3 -5
In the early 21st century, SRC has become a prominent public health concern, commonly referred to as “The Concussion Crisis.” 6 In the absence of universal agreement on an operational protocol for the evaluation of SRC, World Rugby introduced the Head Injury Assessment (HIA) protocol in 2012. The HIA protocol is a three-stage pitch-side process for the assessment of head injuries based on the 5th edition of the Sport Concussion Assessment Tool (SCAT5). 7 The HIA protocol combines cognitive, balance, and memory evaluation. It consists of three assessments: immediately post-injury (HIA-1), within 3 h of the injury (HIA-2), and a follow-up at 36-48 h post-injury (HIA-3). 8 An SRC is excluded in the absence of concussion criteria on these three steps (HIA-1, HIA-2, and HIA-3) 8 and an SRC is considered unresolved if the HIA-3 examination is positive. The HIA protocol has been implemented by World Rugby in August 2015 into its rules, “the laws of the game.” 9
In 2012, the expert committee of the 4th International Conference on Concussion in Sport put forward a panel of potential blood biomarkers that are believed to potentially improve the management of SRCs. 10 These biomarkers include S100 calcium-binding protein B (S100B), neuron specific enolase (NSE), glial fibrillary acidic protein (GFAP), and tubulin-associated unit (Tau). Since then, many studies have focused on the utility of these biomarkers in the management of SRC in sports such as hockey or football, but very few concerned rugby. The aim of this study is to evaluate a panel of seven blood biomarkers (S100B, NSE, GFAP, Tau, spectrin breakdown products [SBDP], ubiquitin C-terminal hydrolase L1 [UCHL1], and neurofilament light chain [NFL]) for early steps of SRC management.
Methods
Study protocol
This prospective multi-center observational study was performed to evaluate a panel of seven blood biomarkers as clinical tools for the management of SRCs in players of the 14 French professional rugby teams. The medical staffs of the 14 teams were trained about the study protocol prior to the start of the study. Instructions for blood tests were sent to each team. The SRCs were diagnosed by nationally certified neurological referent (established by the Medical Committee of the French National Rugby League), following the World Rugby's HIA three-stage diagnostic protocol. 8 The HIA protocol is a multi-modal assessment that contains a clinical evaluation supported by a symptom checklist, a cognitive evaluation (orientation, concentration and immediate and delayed memory) and balance test. 8 A national expert reviewed all the HIA results. SRCs were not recorded if the neuropsychological examinations were negative on three occasions: pitch-side at the time of impact (HIA-1), 3 h after impact (HIA-2), and 36-48 h after impact (HIA-3).
Resolution of SRC
The resolution of SRC was determined at 36-48 h post-injury (HIA-3), with the absence of any symptoms, a normal SAC, 11 and balance examination, in addition to normal neuropsychological tests such as Trail Making Test. 8 Any abnormality on these different tests lead to consider the SRC as non-resolutive.
Participants
Between 2016 and 2017, 496 male professional rugby players from the 14 teams of the French Professional Championship (Top 14) were enrolled in this protocol. To determine the baseline serum biomarker concentrations and to assess the effect of rugby on blood biomarkers over a season (intra-individual variability), each of the 496 participants underwent venipuncture on two separate occasions: at the beginning, and at the end of the season. The blood samples were always collected away from any sport practice (48 h minimum), and when possible, were carried out during a week off. For previously concussed players, the blood samples were only drawn in the case of a fully resolutive SRC.
During the course of the study, a total of 45 SRC cases was reported for 42 players who completed HIA assessment and blood collection at 36 h after SRC.
Of the 42 players included, 39 presented one SRC, and three sustained two SRCs. Therefore, two groups were constituted: one containing all SRCs (n = 45), and another, including only the first SRC (n = 42). Matched controls were constituted for the two groups composed of 90 and 84 players, respectively. Controls were recruited from the non-concussed professional rugby players and matched to SRC players according to demographic characteristics (age, weight, size, and body mass index), player position, and skin pigmentation. Skin types were assessed using the Fitzpatrick phototyping scale. In addition, 29 of the 45 concussed players also underwent blood collection 36 h after return to play (RTP) without a new concussion.
Standard protocol approvals, registrations, and patient consents
The study was conducted in accordance with the principles of the Declaration of Helsinki for ethical medical research involving human subjects, and the project was approved by the national ethics committee for the protection of the persons involved in health research study (CCP Sud-Est 6; authorization number: AU 1277; date: July 6, 2016). All participants provided written informed consent forms prior to the enrolment in the study.
Biochemical procedures
Blood samples (through venipuncture) were collected into gel separator tubes for serum and centrifuged within 15 min (2000 xg at 4°C). The blood samples were anonymized with a unique participant identifier ensuring participant confidentiality. Serum samples were aliquoted into cryovials (with a minimum volume of 500 μL per cryovial) and stored at - 80°C until analysis. S100B and NSE concentrations were determined by electro-chemiluminescence immunoassay on a Cobas e411® instrument, using kits generously gift by Roche Diagnostics (Meylan, France). NFL, GFAP, UCHL-1, and Tau concentrations were measured using digital enzyme-linked immunosorbent assay (ELISA) technology (Quanterix Corporation, Lexington, MA). SBDP concentrations were measured using an ELISA kit (MyBioSource, San Diego, CA).
For each concussed player, blood biomarkers concentrations obtained 36 h after SRC were expressed as an individual and personalized percentage change from baseline (PCH36[%]) and were calculated as follows: PCH36 (%) = 100 × (([Biomarker]36h - [Biomarker]basal)/[Biomarker]basal). The baseline concentrations, as mentioned above, were obtained away from sport practice and concussions. Biomarker concentration obtained 36 h after RTP (without new concussion) was also expressed as a PCH36[%] according to the same calculation as above.
Statistical analysis
The sample size estimation was determined according to 1) CONSORT 2010 statement, extension to randomized pilot and feasibility trials 12 and 2) Cohen's recommendations 13 who has defined effect-size (ES) bounds as small (ES: 0.2), medium (ES: 0.5), and large (ES: 0.8, “grossly perceptible and therefore large”). For 45 concussed players and 90 control players, an effect-size of at least 0.8 can be highlighted for a two-sided type I error at 0.005 (a correction to take into account multiple comparisons) and a statistical power greater than 90%. Statistical analyses were performed using Stata software, Version 15 (StataCorp, College Station, TX). The tests were two-sided, with a Type I error set at 5%. Continuous data were expressed as median ± (interquartile range [IQR]) according to statistical distribution. The assumption of normality was assessed using the Shapiro-Wilk test. To compare the groups (such as concussed players vs. controls, and non-resolutive vs. resolutive SRCs), analysis of variance (ANOVA) or Kruskal-Wallis test (when ANOVA assumptions were not met) were used for continuous parameters. The homoscedasticity assumption was studied by Bartlett test. Chi-squared or Fisher's exact tests were used for categorical variables.
Further, for each biomarker, the intra-class correlation coefficient (ICC) was estimated using a random-effects model (more precisely linear mixed model) in order to evaluate between and within team variability (as random-effect). When appropriate, the normality of residuals from these models was studied as above mentioned, using Shapiro-Wilk's test. If necessary, a logarithmic transformation was suggested as a means to access the normality of dependent variables. As ICC values were low, the comparisons drawn using random-effects model were completed by usual statistical tests (ANOVA or Kruskal-Wallis) described above.
The results were expressed using Hedges' effect-sizes and 95% confidence intervals. The analyses were completed by multi-variable regression models with age, BMI, skin pigmentation and pitch position as adjustment covariates to take into account possible confounding factors. The relationship between continuous variables was explored using correlation coefficients (Pearson or Spearman, according to the statistical distribution), and applying a Sidak's type I error correction to take into account multiple comparisons. The effect of rugby on blood biomarkers over a season (intra-individual variability) was evaluated by calculating ICC estimated from random-effects model, and was interpreted according to the thresholds reported in the literature. 14 Finally, a restricted analysis was performed on the group limited to the first 42 SRCs matched to 84 controls in order to guarantee the robustness of the results. Besides, the same statistical analysis plan (as previously described) was applied. Since the two analyses (45 SRCs, 90 controls; 42 SRCs, 84 controls) behave in a similar fashion, only the results of 45 SRCs vs. 90 controls analyses are presented.
Results
Participants and blood samples
A total of 496 professional rugby players was followed from December 8, 2016, to June 4, 2017. During this study period, 79 players were suspected of having potentially been concussed. In the end, the diagnosis of SRC was confirmed for 53 players. Only 42 players (n = 45 SRCs) provided a blood sample 36 h after SRC (Fig. 1). Of these 45 SRCs, 28 were non-resolutive and 17 were resolutive. Another blood sampling 36 h after RTP (without concussion) was also taken from 29 players out of 42 players previously concussed.

Screening and enrolment of study participants. HIA, head injury assessment; SRC, sport-related concussion; RTP, return to play.
The demographic characteristics, player position, and skin pigmentation were summarized for 45 SRCs matched to 90 controls (Table 1). There was no statistically significant difference (for age, weight, size, body mass index, skin pigmentation, and player position) between concussed players and their matched controls (p = 0.78, p = 0.44, p = 0.06, p = 0.59, p = 0.93, p = 0.75, respectively), establishing retrospectively the validity of our matching criteria.
Demographic Characteristics, Pitch Position, and Skin Pigmentation of the Study Participants
A total of 45 sport-related concussions was reported for 42 players
Light: types I and II; intermediate: types III and IV; dark: types V and VI (according to the six categories of the Fitzpatrick scale).
IQR, interquartile range; BMI: body mass index.
Relationship of biomarkers with demographic characteristics, player position, and skin pigmentation in control players
There was no correlation between each tested parameter (age, weight, size, or body mass index) and serum concentrations of each biomarker (r between 0.002 and 0.336; Table 2) in control players (n = 90). Additionally, there was no significant difference in biomarker concentration (p between 0.05 and 0.93; Table 2) according to the player position (wing, fullback, center, scrum-half, fly-half, second row, back row, prop, or hooker). A significant association was found between S100B concentrations and skin pigmentation (p < 0.001; Table 2).
Relationship of Biomarkers with Demographic Characteristics, Pitch Position, and Skin Pigmentation in Control Players (n = 90)
p < 0.05.
+ = light, intermediate, or dark
++ = wing, fullback, center, scrum-half, fly-half, second row, back row, prop, or hooker.
BMI: body mass index; S100B, S100 calcium-binding protein; NSE, neuron specific enolase; SBDP, spectrin breakdown products; UCHL1, ubiquitin C-terminal hydrolase L1; GFAP, glial fibrillary acidic protein; NFL, neurofilament light chain; Tau, tubulin-associated unit.
The team-related effect on biomarker concentrations in control players
Overall, ICCs were very low (ICC = 0.01 for S100B and UCHL1) or low (ICC = 0.07 for GFAP, ICC = 0.08 for NSE and NFL, ICC = 0.14 for Tau), indicating that results of concentrations were not team-related for control players. However, ICC was high for SBDP (ICC = 0.66), meaning that results of concentrations were strongly influenced by the team factor.
The effect of rugby on blood biomarkers over a season (intra-individual variability): Evaluation on two samples
Control players (Table 3; Fig. 2)
Analysis of ICC suggested, with an excellent reliability (ICC = 0.93), that concentrations of S100B remained stable over the course of a season. The median concentrations of baseline S100B, measured twice during the season, were 0.062 ng/mL (IQR: 0.042-0.078 ng/mL) and 0.056 ng/mL (IQR: 0.038-0.072 ng/mL). For GFAP (ICC = 0.85), the reliability was good. The median concentrations of baseline GFAP were 48.22 pg/mL (IQR: 40.54-63.09 pg/mL) and 48.24 pg/mL (IQR: 38.05-64.33 pg/mL). For UCHL1, the ICC of 0.60 was indicative of moderate reliability. For the four others biomarkers (NSE, SBDP, NFL and Tau), weaker ICCs (0.01 to 0.37) were found, suggesting that concentrations were not stable over the course of a season.
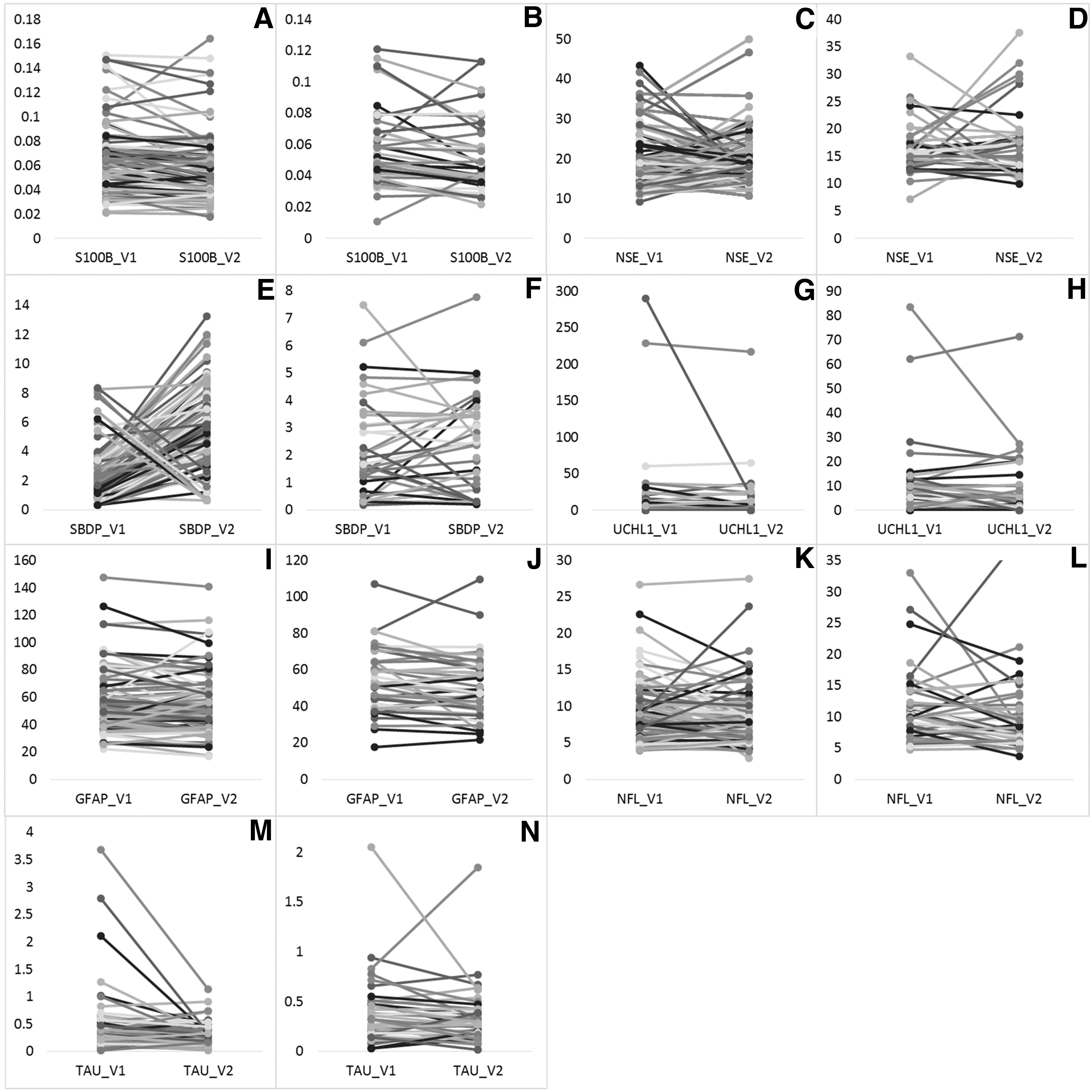
Levels of biomarkers measured, at the beginning (V1) and at the end (V2) of the season, for each rugby player.
Effect of Rugby on Blood Biomarkers over a Season in Control Players (n = 90) and Concussed Players (n = 45 SRCs)
Biomarker stability evaluated during the season on two basal samples.
SRC, sports-related concussion; IQR, interquartile range; ICC, intra-class correlation coefficient; S100B, S100 calcium-binding protein; NSE, neuron specific enolase; SBDP, spectrin breakdown products; UCHL1, ubiquitin C-terminal hydrolase L1; GFAP, glial fibrillary acidic protein; NFL, neurofilament light chain; Tau, tubulin-associated unit.
Concussed players (Table 3; Fig. 2)
Analysis of ICC suggested, with a moderate reliability (ICC = 0.73), that concentrations of S100B remained stable over the course of a season. The median concentrations of baseline S100B, measured twice during the season, were 0.052 ng/mL (IQR: 0.043-0.069 ng/mL) and 0.045 ng/mL (IQR: 0.038-0.068 ng/mL). For GFAP (ICC = 0.83), the reliability remained good. The median concentrations of baseline GFAP were 51.93 pg/mL (IQR: 39.61-64.71 pg/mL) and 47.23 pg/mL (IQR: 38.95-60.40 pg/mL). For UCHL1, the ICC of 0.76 was indicative of good reliability. For Tau and SBDP, the ICCs were respectively 0.54 and 0.61, suggesting moderate reliability. For NSE and NFL, ICCs (0.07 and 0.42, respectively) remained weaker, suggesting that concentrations were not stable over the course of a season.
Biomarker concentrations at 36 h of SRC
Raw concentrations
Raw concentrations of the seven biomarkers measured 36 h after SRC were not significantly different between non-resolutive (n = 28) and resolutive (n = 17) SRCs (p between 0.06 and 0.92; Table 4). These results were consistent with the effect size showing small to medium values (Table 4).
Ability of Blood Biomarkers to Identify Non-Resolutive SRCs from Resolutive SRCs
Calculated with Hedges' formula.
PCH36 % = 100 x (([Biomarker]36h - [Biomarker]baseline)/[Biomarker]baseline).
p < 0.05.
SRC, sport-related concussion; Q1, first quartile; Q3, third quartile; CI, confidence interval, AUC, area under the curve; S100B, S100 calcium-binding protein; R, resolutive SRC; NR, non-resolutive SRC; NSE, neuron specific enolase; SBDP, spectrin breakdown products; UCHL1, ubiquitin C-terminal hydrolase L1; GFAP, glial fibrillary acidic protein; NFL, neurofilament light chain; Tau, tubulin-associated unit.
Concentrations expressed from baseline
The PCH36[%] of S100B and NFL were significantly different between non-resolutive (n = 28) and resolutive (n = 17) SRCs (p = 0.006 and 0.01 respectively; Table 4), with a large effect-size (S100B: -0.877 [95% confidence interval [CI]: -1.492 to -0.252]; NFL: -1.012 [95% CI: -1.771 to -0.237]; Table 4). Both these biomarkers were able to distinguish non-resolutive SRCs from resolutive SRCs with an area under the curve of 0.77 (Table 4; Supplementary Data)
Figure 3 showed S100B levels measured at baseline and 36 h following SRC for each rugby player. The median PCH36[%] of the S100B was -14.3% in case of resolutive SRC, while the median value was 6.7% for players with a non-resolutive SRC (p = 0.006).
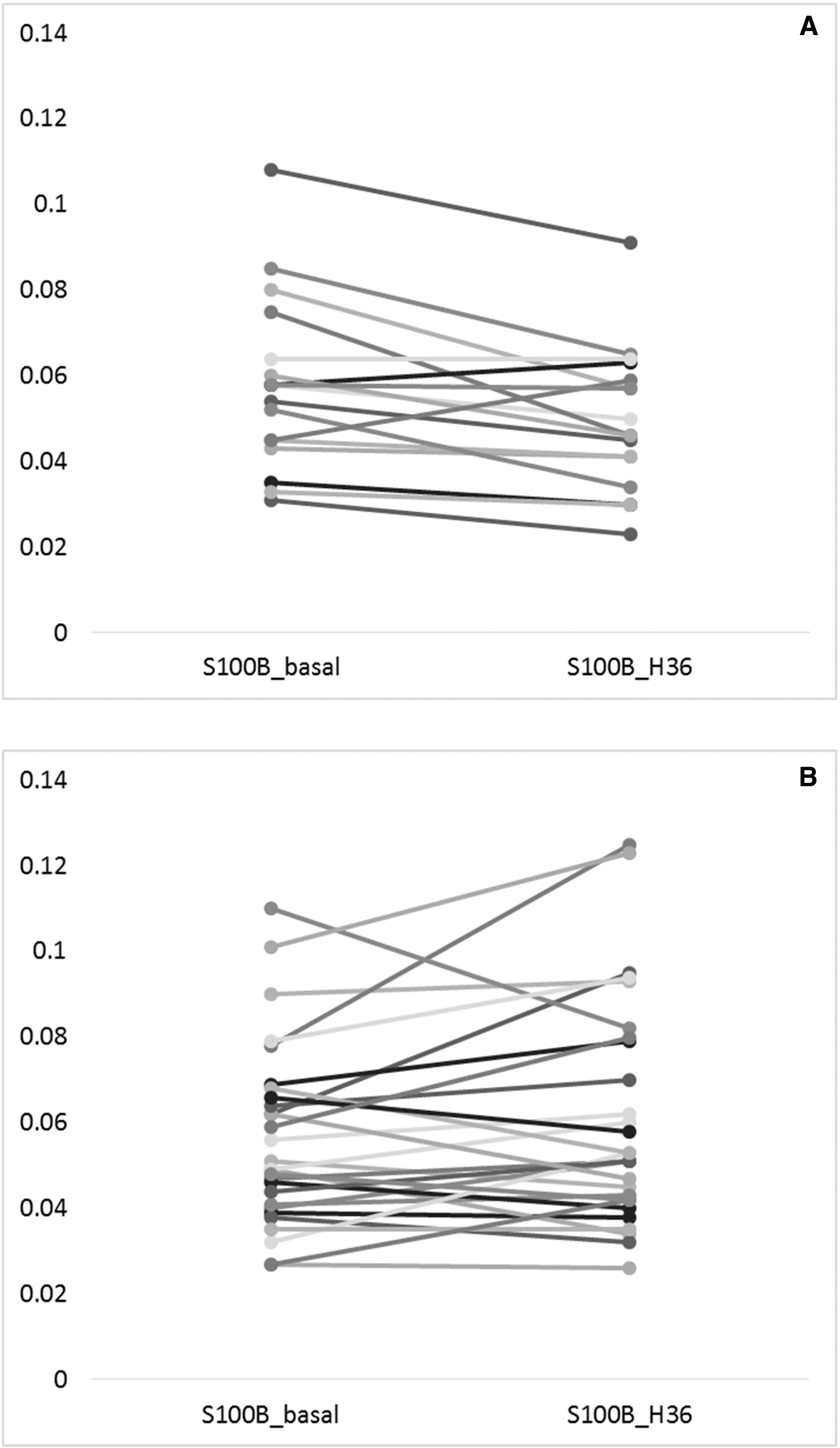
S100 calcium-binding protein B (S100B) levels measured at baseline and 36 h following sport-related concussion (SRC) for each rugby player.
S100B concentrations in previously concussed players at 36 h of RTP without concussion
Raw concentrations
S100B raw concentrations measured 36 h after RTP (without concussion) were not significantly different between the previous non-resolutive (n = 15) and resolutive (n = 14) SRCs (p = 0.19). These results were consistent with a medium effect-size [0.48 (95%CI: -0.24 to 1.20)].
Concentrations expressed from baseline
While concentrations measured 36 h after the RTP were expressed as a percentage change (PCH36[%]) in comparison with the baseline concentrations of each player, results were still not significantly different (p = 0.74). These results were consistent with a small effect-size [0.16 (95%CI: -0.55 to 0.86)].
Discussion
SRC is currently diagnosed in professional rugby players by a specific HIA protocol incorporating an assessment on the pitch, an assessment within 3 h of the injury, and a follow-up assessment at 36-48 h post-injury. In a previous study, the Pitch Side Concussion Assessment tool demonstrated a sensitivity of 84.6% and a specificity of 74% in the identification of SRC. 15 This lack of sensitivity and specificity was confirmed in a more recent study. 16 Thus, the implementation of a blood biomarker in the diagnostic process may enhance the diagnostic performances and improve the overall management of concussed players. In this context, our study is the first to evaluate a panel of seven blood biomarkers for SRC (S100B, NSE, SBDP, UCHL1, GFAP, NFL, and Tau) in a large multi-centric cohort of professional rugby players including concussed and control players matched by age, weight, size, body mass index, pitch position, and skin pigmentation. Among these detailed matching criteria used for our study, only a significant association between S100B concentration and skin pigmentation (p < 0.001) was reported. This association has already been discussed in well-known literature and is explained by the fact that melanocytes are non-brain cells that synthesize small amounts of S100B protein under physiological conditions. 17,18
In the present study, two data are essential to validate the robustness of biomarkers: the team-effect factor and especially the intra-individual variability over the course of a season. Indeed, we consider that it is essential to study the effect of rugby on blood biomarkers over a season in order to validate a biomarker in the routine management of SRC. This study is the first to publish such data of brain injury blood biomarkers during a rugby season. Concerning our results, no team-effect was described for the tested biomarkers except for SBDP concentrations influenced by the team factor. Moreover, only two biomarkers remained stable in control players over the course of a season. The reliability was excellent for S100B and remained good for GFAP. In concussed players, S100B concentrations remained stable over the course of a season, although SRCs impacted the ICC score (moderate reliability). Protein S100B is a biomarker of the acute phase of mild traumatic brain injury; its concentration increases rapidly within the first hours of the trauma, then decline quickly with a short half-life. 19 -21 Yet, the moderate decrease in stability over the season observed in our study for concussed players could reflect a change in the kinetics of the biomarker, which can be explained by the long-term impact of SRC on brain function.
After taking into account the above results, we evaluated the biomarkers' concentrations at 36 h after SRC in concussed players. On the one hand, no biomarker raw concentrations measured 36 h after SRC were significantly different between resolutive and non-resolutive SRCs, with small to medium effect-size. On the other hand, there was a large effect-size for S100B and NFL when concentrations were expressed as a percentage change (PCH36[%]) in comparison with the individual baseline concentrations of each player. The effect size was larger than 0.8, indicating an optimal interpretation according to our statistical methodology. S100B and NFL concentrations expressed as PCH36[%] were also significantly different between non-resolutive and resolutive SRCs. As expected, this difference was no longer found for S100B at the “return to play” step (without concussion).
In the management of concussed rugby players, our results highlight how valuable S100B is in the identification of non-resolutive SRCs. Unlike NFL, S100B remained stable over the season, and the biomarker's concentrations were not affected by the team-effect. This could partially be explained by the measurement method used in our study. S100B concentrations were measured using an automated immunoassay (Cobas e411) providing excellent analytical results regarding the precision, linearity, accuracy, along with a low coefficient of variation (CV%; intra-assay CV: 1.1 to 2%; inter-assay CV: 1.8 to 2.1%), 18 recommended for clinical use. 18,22 In addition, S100B protein presents a pre-analytical advantage due to its relative stability, at least 8 h at room temperature or 48 h at 2-8°C. 23 NFL shows a similar robustness in terms of pre-analytical characteristics, 24 -26 but differs analytically with a higher CV% (intra-assay CV: 6.6%; inter-assay CV: 17%). 27 Moreover, a significant intra-individual variability of NFL was described in collegiate American football players, with a long-term elevation of NFL concentrations subsequent to the accumulation of axonal injuries during the season. 28 This cumulative elevation of NFL could be explained by the long half-life of the biomarker of 3 weeks. 28
Our results strongly suggest that an optimal interpretation of S100B levels is achieved through a personalized medical approach, with a comparison of post-SRC S100B concentration to the individual baseline level for each player. This approach reduces the influence of inter-individual variability explained by concussion history. In addition to the HIA-3 assessment, a 36-48 h S100B increase over the baseline constitutes an additional argument for the non-resolution of SRC. S100B measurement may improve the management of SRC by compensating the HIA protocol's lack of sensitivity, and by allowing the identification and the reclassification of false negatives. The use of S100B in this setting is consistent with the 2016 Berlin meeting recommendations. 29 Considering the potential medical complications of unreported concussions, blood biomarkers may constitute an objective mean to determine return-to-play decisions. Indeed, in many contact sports, the under-reporting of concussion symptoms compromises the SRC diagnosis. 29,30 A recent research identified 17.2% of elite rugby league players in Australia chose not to report likely concussive episodes and concussion-related symptoms during the 2018 and 2019 seasons. 30 The clinical application of biomarkers could also be useful in settings where the HIA is not done, i.e. in lower leagues, 31 but in this case their utility would be limited by the need for venipuncture and the high cost of biomarker testing.
In case of resolutive SRC, there was a decrease in the concentration of S100B compared to the baseline value. This decrease in concentration has already been observed in a few studies but never in rugby. 32 -34 Recently, Meier and colleagues showed an elevated serum level of S100B at 6 h following SRC relative to pre-season value. Interestingly, S100B levels were significantly decreased at 24-48 h post-injury relative to pre-season levels. According to the authors, the 24-48 h S100B decrease is linked to the fact that injured athletes were not active at this time, as recommended in return-to-play guidelines. 32 Our additional hypothesis is a physiological response to concussion in which S100B is downregulated for neuronal protection. Indeed, the release of S100B by astrocytes following SRC (micromolar levels) may contribute to neuroinflammation by activating the receptor for advanced glycation end products (RAGE). 35 Micromolar concentrations are harmful for the neuronal environment whereas nanomolar concentrations of S100B exert neurotrophic effects by stimulating neurite outgrowth and regulating survival of neurons. 36 To preserve brain functions, blood concentration of S100B could be regulated by its scavenger, soluble receptor for advanced glycation end products (sRAGE). Indeed, sRAGE is hypothesized to counteract the detrimental action of RAGE as a competitive inhibitor of the signaling pathway and as ligand scavenger. 35,37 The glymphatic system could also be involved by altering the clearance of the biomarker. 38 We therefore hypothesize that a physiological change in the body, to down-regulate S100B levels, could participate in the resolution of SRC at 36 h post-injury.
Previous studies have established the usefulness of blood S100B measurement in concussed players of contact sports such as hockey, football, and soccer. 32,33,39 Indeed, the use of a blood biomarker is particularly relevant in clinical scenarios where players might be motivated to not report or otherwise minimize SRC-related symptoms. It may also be useful for concussed players with fewer acute symptoms. In addition, in contrast to self-reported symptoms or neurocognitive tests, biomarkers provide a measure of the pathophysiological effects of SRC.
Finally, according to Meier and colleagues, a biomarker should not be interpreted in an isolated way but always associated with a clinical examination. 33 So far, only a few studies have been published on professional rugby players to evaluate a biomarker of brain damage in SRC. In our previous study, 40 a change in S100B concentration, 36 h after the match, in relation to the basal concentration was found to identify SRC with a sensitivity of 100 %. 40 Nonetheless, only five SRCs were included and the ability of S100B to differentiate a non-resolutive SRC was not tested. 40 Shortly after a rugby match (< 8 h), the ability of S100B to identify SRC was very low because of a significant increase in S100B (due to an extracerebral release) in the absence of concussion, 40,41 compared with other sports as described previously. 32,33,39 Further, Bouvier and colleagues 40 showed that this increase was correlated with the number of body collisions the rugby player suffered. Another study was also published on rugby players but no concussed players were included and S100B concentrations were measured using a manual assay (ELISA kit). 42
With regard to sports other than rugby, several studies showed the usefulness of Tau, NFL, and GFAP in the identification of SRC and the prediction of RTP after a concussion. 43 –46 However, the variation pattern of each biomarker may differ according to the nature of the sport, leading to a distinct kinetic profile observed for rugby players. Although, in a recent prospective study, Laverse and colleagues 47 suggested that plasma NFL and GFAP, unlike Tau, have a potential for the identification of SRC in rugby players. Our results are not in line with these observations. However, in our study the number of pre-season samples is higher. Moreover, we evaluated the intra-individual variability to establish the effect of rugby on blood biomarkers over a season and incorporated the biomarkers results into the HIA protocol. A study with a similar design to ours is being conducted in another rugby country. 48
There are some limitations to our study. The effect of rugby on blood biomarkers over a season was only evaluated on two blood baseline samples. Although, only two basal values may seem insufficient, our data are robust as the concentrations were measured at the beginning and end of the season, and away from any sport practice. Moreover, 11 concussed players among the initial 53 SRCs did not wish be part of the study, which may be explained by its multi-centric nature. Another limitation of the study was the lack of repeated blood sampling post-SRC. The post-SRC sample was collected strategically at 36 h of the SRC (during HIA-3 assessment). A complementary study could also complete the kinetics of biomarkers at other times after SRC, for example at 3, 6, 12, 24, and 36 h after SRC, to give a kinetic aspect compared to our one-point strategy. This scenario based on such repeated sampling could be supported by the development of point-of care solution for capillary S100B measurement. Other blood samples were considered too complicated in our population of professional rugby players, and not allowed by our experimental design validity ethical committee. Lastly, the biomarkers have been validated against the HIA, which has both sensitivity and specificity limitations. Inaccuracies in the HIA process could have affected our results. However, there is no gold standard to date for diagnosing concussion and, the HIA protocol introduced by World Rugby is the best tool available for monitoring professional rugby players.
Conclusions
To conclude, we found out that individual increase in S100B blood concentration (related to baseline) within 36 h of an SRC is predictive of non-resolutive SRC. Finally, integrating personalized measurement of serum S100B in the HIA-3 clinical assessment may help in declaring a non-resolutive SRC objectively and in introducing for such players a better protection after SRC, following the recommendations determined at the 2016 Berlin meeting.
Transparency, Rigor, and Reproducibility Statement
The study was pre-registered at
Samples were analyzed in four separate batches, with samples assigned to batches randomly and all reagents used were from the same lots. All equipment and analytical reagents used to perform measurements on the blood biomarkers are available from commercial sources. The key inclusion criteria and outcome evaluations are established standards. All blood samples used to conduct the study were obtained by the investigators and 100% of the participants have provided permission for samples to be used for future research without requirement for specific additional informed consent.” option under appropriate license.
Footnotes
Acknowledgments
The authors would like to thank all the medical physicians and biologists in charge of the 14 rugby teams for their involvement in the research project, Dr. David Latour for proofreading this manuscript and Dr. Céline Lambert for her help in statistical analysis. This research project was supported by the medical committee of the French National Rugby League (Ligue Nationale de Rugby/LNR) and of the French Federation of Rugby (Fédération Française de Rugby/FFR).
Authors' Contributions
Dr. Oris wrote the manuscript. Ms. Durif contributed to the data analysis. Ms. Rouzaire contributed to the data collection. Dr. Abbot critically reviewed the manuscript. Dr. Pereira performed statistical analysis. Dr. Brailova critically reviewed the manuscript. Dr. Bouvier critically reviewed the manuscript and finalized the manuscript. Dr. Kahouadji critically reviewed the manuscript and finalized the manuscript. Pr. Lehmann critically contributed to the validation of biological data and critically reviewed the manuscript. Dr. Hirtz critically contributed to the validation of biological data. Pr. Decq critically contributed to the validation of clinicial (SRC) data and critically reviewed the manuscript. Dr. Dusfour critically reviewed the manuscript. Dr. Marchi was implied in the finalization of the study’ design and critically reviewed the manuscript. Pr. Sapin conceptualized and designed the study as well as co-drafted and finalized the manuscript.
Funding Information
World Rugby (Scientific Program grant number 16003) funded the global organization of the project and the “S100B” part of this study and “NSE, NFL, GFAP, UCHL-1, Tau and SBDP measurements” part was completed by an internal grant of the University Hospital of Clermont-Ferrand.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.