
Abstract
Increasing rates of sport-related concussion (SRC) in youth impose a significant burden on public health systems and the lives of young athletes. Accurate prediction for those likely to develop persistent post-concussion symptomology (PPCS) using a fluid biomarker, reflecting both acute injury and recovery processes, would provide the opportunity for early intervention. Cortisol, a stress hormone released through the hypothalamic-pituitary-adrenal (HPA) axis following injury, may provide a missing physiological link to clinical recovery. This cohort study investigated the change in saliva cortisol following SRC and the association between cortisol and symptom burden in pediatric ice hockey players. Further, the association between cortisol levels and medical clearance to return to play was explored. In total, cortisol samples from 233 players were included; 165 athletes (23.6% female) provided pre-injury saliva and 68 athletes (19.1% female) provided post-SRC saliva samples for cortisol analysis. Quantile (median) regressions were used to compare cortisol between pre-injury and post-SRC groups, and the association between total symptoms (/22) and symptom severity scores (/132) reported on the Sport Concussion Assessment Tool (SCAT)3/SCAT5 and post-SRC cortisol (adjusting for age, sex, history of concussion, and time from injury to sample collection). Results demonstrated significantly lower saliva cortisol in post-SRC athletes compared with the pre-injury group (β = −0.62, 95% confidence interval [CI; −1.08, −0.16], p = 0.009). Post-SRC cortisol was not significantly associated with the SCAT3/SCAT5 symptom totals or symptom severity scores; however, females were found to report more symptoms (β = 6.95, 95% CI [0.35, 13.55], p = 0.040) and greater symptom severity (β = 23.87, 95% CI [9.58, 38.15], p = 0.002) compared with males. Exploratory time-to-event analysis revealed a point estimate suggesting a potential association between low cortisol levels and days to medical clearance to return to play. Although preliminary, these findings suggest that the HPA axis may be dysregulated post-SRC. Further, our exploratory analysis and case presentation of post-injury outliers highlight the need to further research cortisol as a prognostic biomarker to inform individualized sex-specific care after SRC.
Introduction
Sport-related concussion (SRC) is a mild traumatic brain injury (mTBI) that imposes significant burden on the public health system. This is especially pronounced in the pediatric population, where in Canada approximately 10% of adolescents sustain an SRC each year. 1 Pediatric hospital visits due to SRC have significantly increased over the past 2 decades. 2,3 According to the 5th International Consensus Statement on Concussion in Sport, typical clinical recovery in children and adolescents occurs before 4 weeks 4 ; however, up to 30% do not recover within 1 month, with approximately 11% suffering from persistent post-concussion symptoms (PPCS) beyond 3 months of injury. 5 –7
The clinical diagnosis and prognosis of SRC relies on self-reported symptoms using tools such as the Sport Concussion Assessment Tool–5 (SCAT5) 8 or the recent 5P Clinical Risk Score developed to assess the risk of PPCS after concussion. 9 However, these tools rely greatly on subjective assessment and self-reported measures of symptoms, highlighting the need for more objective tests in concussion management. Research examining fluid biomarkers of SRC is ongoing, but has yet to definitively determine an accurate fluid biomarker for SRC diagnosis or prognosis. 10 Many acute biomarkers of brain injury have garnered recent attention such as ubiquitin-C-terminal hydrolase 1 (UCH-L1), glial fibrillary acidic protein (GFAP), neurofilament-light (NF-L), and Tau to help diagnose SRC. 11 Thus far there has been little success in linking these markers of underlying pathophysiology to clinical measures of recovery. 12 Further, few efforts have been made to examine post-SRC biomarkers in the pediatric population.
The link to physiological recovery may lie instead with a marker of systemic stress involved in the global response to injury and recovery processes. Cortisol, a stress hormone released through activation of the hypothalamic-pituitary-adrenal (HPA) axis, is one potential biomarker for SRC. 13 In general, cortisol release results in energy mobilization and mediates anti-inflammatory actions to moderate the body's reaction to a particular stressor. 14 Cortisol serves similar purposes in the context of TBI, mediating specific anti-inflammatory actions on the blood–brain barrier (BBB) and immune cells of the central nervous system (CNS), that is, microglia. 15 However, the pituitary gland is particularly susceptible to primary and secondary injuries from TBI due to its confined location and the delicate structure of the pituitary stalk. 16 Further, the pituitary stalk is highly vascularized where damage could impair blood supply to the gland. 16,17 Injury to the pituitary gland can impair HPA-axis function resulting in a maladaptive response to SRC manifesting as decreased energy availability, increased neuroinflammation, and BBB permeability, all of which are linked to worse outcomes. 15,18,19
Pituitary deficiencies have been observed for all severities of TBI, although diagnostic criteria may vary based on study design. Whereas the prevalence is highest in severe TBI (both acute and chronic stages ranging ∼35–69%), it remains substantial, yet varied, in mTBI (∼17–38%). 20 –22 The estimated prevalence of pituitary dysfunction post-SRC is between 15% and 46.6%. 16,23 A regularly monitored pituitary hormone after more severe acute TBI is cortisol. 24 In any TBI case, regardless of severity, acute adrenal insufficiency requires urgent replacement; however, cortisol levels are not routinely screened in SRC given that the injury is not typically severe enough to warrant hospitalization or intensive care unit (ICU) monitoring. 24
Unfortunately, the literature concerning the associations between acute hormone changes and long-term outcomes lacks consensus. Findings from severe TBI studies have shown decreased cortisol post-injury to be predictive of long-term hypopituitarism and increased morbidity and mortality. 25,26 However, one study in children with TBI found that all cases with acute pituitary deficiencies recovered by 12 months (with some new deficiencies developing after 12 months), whereas another study in adult TBI demonstrated that acute pituitary dysfunction was not associated with the development of chronic hypopituitarism. 27,28 Nonetheless, in the context of SRC, the non-specific symptoms of PPCS greatly overlap with those of endocrine dysfunction. 29 There have been few studies examining cortisol changes post-SRC showing mixed results due to sampling timing and methodology. Two studies did not find changes in cortisol following SRC; however, they did show associations between acute cortisol post-SRC and symptom burden and recovery time. 30,31 Conversely, a case series recently published by our research group did see a significant drop in serum cortisol acutely post-SRC accompanied by greater symptom burden and prolonged recovery. 32 This relationship may be indicative of a maladaptive response to injury in the HPA axis contributing to protracted recovery. However, that study did not acquire enough serum samples inside the recommended 7:00–10:00 a.m. cortisol sampling time to allow for statistical inferences from the data.
Although there has been promising research into the use of salivary measurements of morning cortisol to monitor for adrenal insufficiency in hospital settings, 33 it is not yet part of the clinical algorithms used in Canada, which rely on serum cortisol instead. Saliva collection for cortisol analysis serves as an attractive alternative to blood collection in pediatric populations given the non-invasive method of collection, ease of storage, and low cost of analysis. As a follow-up to the serum cortisol study described above, we aimed to assess changes in saliva cortisol concentrations after SRC in a larger sample of youth ice hockey players. The primary objective of this study was to investigate the difference in cortisol levels following SRC and the relationship between cortisol and symptom burden in a pediatric population. Additionally, an exploratory objective was to investigate the potential association between cortisol and recovery time post-SRC.
Methods
Participants
This was a sub-cohort that recruited youth ice hockey players enrolled in the Safe2Play prospective cohort study (S2P). S2P was a longitudinal cohort study that included clinical, psychosocial, and functional measurements to inform SRC detection, diagnosis, and prognosis in youth ice hockey players. The S2P study was conducted over 5 ice hockey seasons (2013–2018) in Calgary, Edmonton, and surrounding areas in Alberta, Canada. Data for the present study were collected during the 2014–2018 seasons. Inclusion criteria were: a) age 11–17 years, b) enrollment in a hockey team registered with Hockey Canada in Calgary or Edmonton, and c) written consent of player or player parents. Exclusion criteria included a previous medical history of neurological conditions such as stroke, moderate to severe TBI, or chronic neurological conditions; players who did not provide morning saliva samples; or players who were taking steroidal medications (oral or inhaled). Demographic information collected included age, sex, past medical history, medications, and previous concussion history. This study was approved by the University of Calgary Conjoint Research Ethics Board (Ethics ID: REB14-0348/REB14-2209).
Procedure
Pre-injury saliva samples, demographic information, and questionnaires were collected at S2P hockey camps. The Sport Concussion Assessment Tool–3 (SCAT3) was used to collect self-reported medical history (including history of concussion) and demographic information for years 2014–2017 and the SCAT5 was collected in year 2018. 4,34 Symptom and symptom severity scores were self-reported using the graded symptom checklist embedded in the SCAT3 and SCAT5 and these components were the same in both versions. Validated injury surveillance methods were implemented to follow youth ice hockey players over the 2014–2018 hockey seasons. Suspected SRCs were diagnosed by a sports medicine physician using criteria from the 4th International Consensus Statement on Concussion in Sport. 34 After SRC diagnosis (within 1 week of injury), athletes underwent a 1-h clinical assessment with study therapists where the SCAT3/SCAT5 evaluated self-reported symptom burden. Acute, post-injury morning saliva samples were obtained within 3–7 days of SRC. Players were then followed throughout their recovery until cleared to return to play (RTP) by a sport medicine physician.
Sample collection and analysis
Morning saliva samples were collected by a research assistant pre-injury and within 3–7 days post-SRC in two different athletic populations upon presentation to the clinic. Using the clean drool technique (Salimetrics, USA), saliva collection tubes were filled during a 7:00–10:00 a.m. time window to capture peak physiological cortisol concentrations occurring upon wakening. 35 Players were instructed to refrain from tobacco use, eating, drinking, and brushing their teeth 1 h prior to sample collection. In addition, players were advised to abstain from caffeine consumption for the 12-h prior to collection. Saliva samples were stored at −80°C until analysis.
Each sample was analyzed using an Agilent 1200 binary liquid chromatography (LC) system coupled to an AB SCIEX QTRAP 5500 mass spectrometer equipped with an electrospray ionization (ESI) source. LC separation was performed on an Agilent ZORBAX Eclipse plus C18 column (100 × 2.l mm, 1.8 μm particle size) at 40°C. The mobile phase A was acetonitrile (95.5, v/v, 2 mM NaF) and mobile phase B was 100% acetonitrile (2 mM NaF). The 12-min gradient was 15–70% B (0–6 min), and 70–100% B (6–7 min), 100% B (7–8.5 min), 100–15% B (8.5–9 min) and then held at 15% B for 3 min. The flow rate was 220 μL/min and the injection volume was 10 μL. Analytes were detected by positive LC-ESI/multiple-reaction monitoring (MRM). Mass resolutions in Q1 and Q3 were set as unit. Each analyte was monitored by two transitions (a quantifier and a qualifier). The lower limit of quantitation (LLOQ) for cortisol was 0.1 ng/mL.
Statistical analysis
Participant characteristics were described using means, standard deviations, medians, interquartile range (IQR), and frequency distributions for pre-injury and post-SRC groups. To examine whether there was a difference between pre- and post-SRC participant cortisol values, quantile (median) regression was used with adjustment for age, sex, and history of concussion (Yes/No) as our data did not meet assumptions of normality and for multi-variable linear regression. In addition, two quantile (median) regression models were conducted to examine whether symptom severity or number of symptoms was related to post-injury cortisol, adjusting for age, sex, history of concussion, and time between injury and sample collection, separately. An exploratory time-to-event analysis using Cox regression was performed to explore whether post-injury cortisol levels influenced the number of days to RTP, adjusting for age, sex, and history of concussion (Yes/No). Cortisol was capped at 4.0 ng/mL to ensure the proportional hazard assumptions were met. Survival curves examining time to medical clearance to RTP between low and high post-injury cortisol groups (split upon median post-injury cortisol) were compared using the log-rank test. Statistical analysis was performed using SAS 9.4 software. A p-value <0.05 was considered statistically significant and 95% confidence intervals (95% CI) were reported where appropriate.
Results
A total of 4747 ice hockey player-years were included in the S2 study (2014–2018, 4 seasons) of which 335 unique players provided saliva samples for this sub-study. Of these, 202 were pre-injury samples and 133 post-SRC samples (note: pre-injury and post-SRC samples were not from the same individuals as these groups were from a convenience sample). Excluded samples included those from participants taking medications containing steroids (n = 26), samples collected after 10 a.m. (n = 66), samples with insufficient saliva volume for analysis (n = 7), and sampling variability (saliva quality insufficient for analysis; n = 3). The final sample for analysis included 165 pre-injury (mean age: 12.7 ± 1.7 years, n = 125 male, n = 39 female) and 68 post-SRC (mean age: 13.8 ± 1.4 years, n = 55 male, n = 13 female). Additionally, participants were excluded from relevant statistical tests based on missing data on sex (n = 1 pre-injury), total number of symptoms and symptom severity score (n = 8 pre-injury, n = 20 post-injury), previous concussion history (n = 4 pre-injury, n = 13 post-injury), and days to RTP (n = 18 post-injury). See Figure 1 for a patient recruitment flowchart and Table 1 for participant characteristics and respective descriptive statistics.
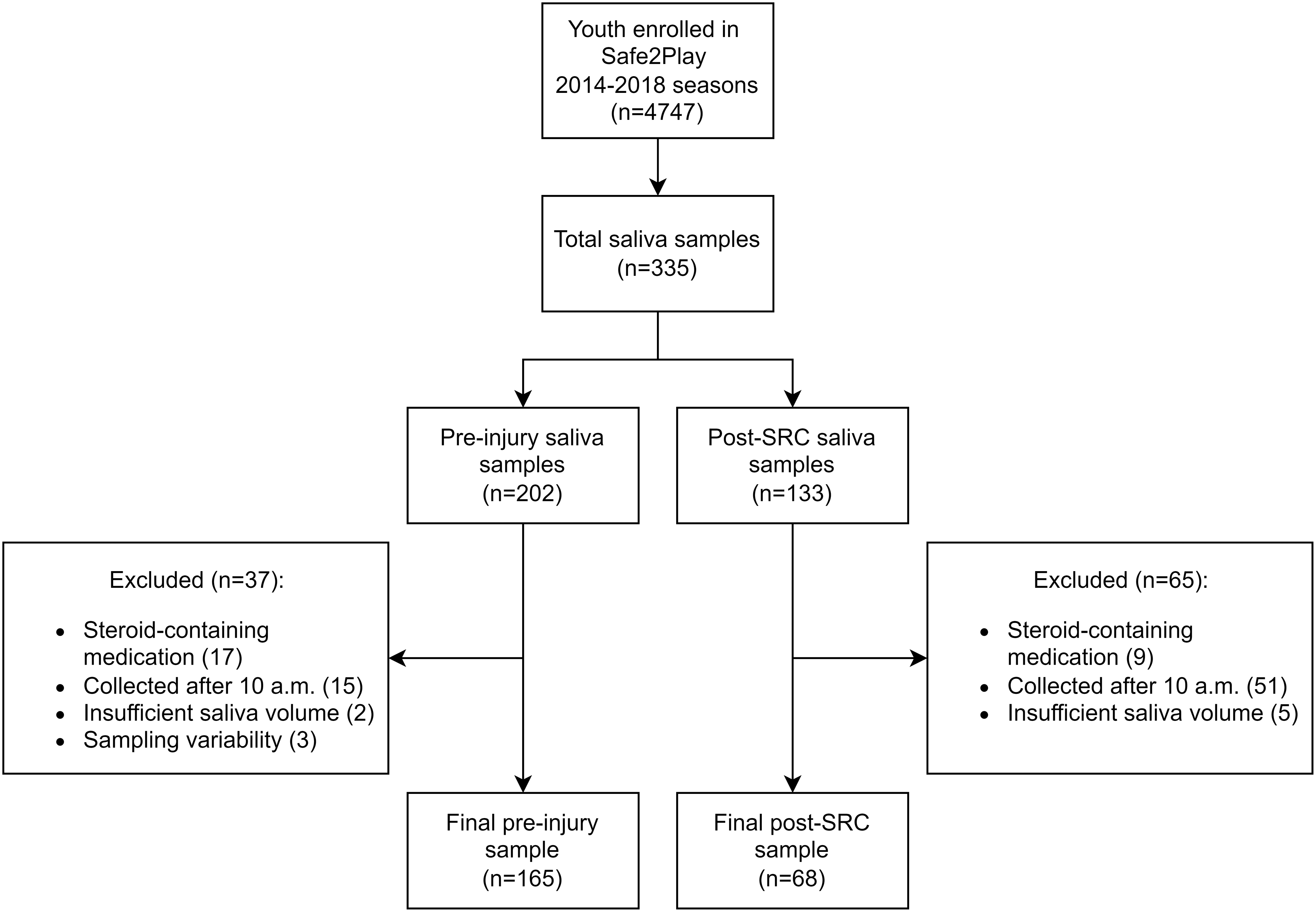
Participant recruitment flowchart. SRC, sports-related concussion.
Participant Characteristics
Age is at time of sample collection.
Q1, first quartile; Q3, third quartile; SD, standard deviation.
Influence of sport-related concussion on cortisol levels
Lower morning saliva cortisol levels were found after adjusting for age, sex, and history of concussion in the post-SRC group compared with the pre-injury group. Median quantile regression analysis revealed that the median cortisol levels were 0.6 ng/mL lower in the post-SRC sample than the expected median cortisol level of the pre-injury group (β = −0.62, 95% CI [–1.08, −0.16], p = 0.009; Fig. 2). Analysis also showed a significant association between age and cortisol, whereby a 0.24-ng/mL increase in median saliva cortisol was found with a 1-year increase in age, adjusting for injury group, sex, and history of concussion (β = 0.24, 95% CI [0.12, 0.36], p < 0.001; Fig. 3). Additionally, no significant associations were found between sex (β = 0.36, 95% CI [–0.10, 0.81], p = 0.128) or history of concussion (β = 0.21, 95% CI [–0.38, 0.43], p = 0.907) on median cortisol levels after adjusting for all other variables in the model.

Scatterplot of saliva cortisol levels (ng/mL) of total, male, and female samples in pre-injury (squares) and post-SRC (circles) groups. Pre-injury and post-injury groups consist of separate athletes. Error bars represent median and interquartile range of each group. Findings from median quantile regression modeling indicated a significant influence of SRC on median saliva cortisol levels whereby the post-SRC group had lower cortisol levels than the pre-injury group (β = −0.62, 95% CI [–1.08, −0.16], p = 0.009) when controlling for age, sex, and history of concussion. No significant associations were found between sex and median saliva cortisol levels after adjusting for all other variables (β = 0.36, 95% CI [–0.10, 0.81], p = 0.128). CI, confidence interval; SRC, sports-related concussion.
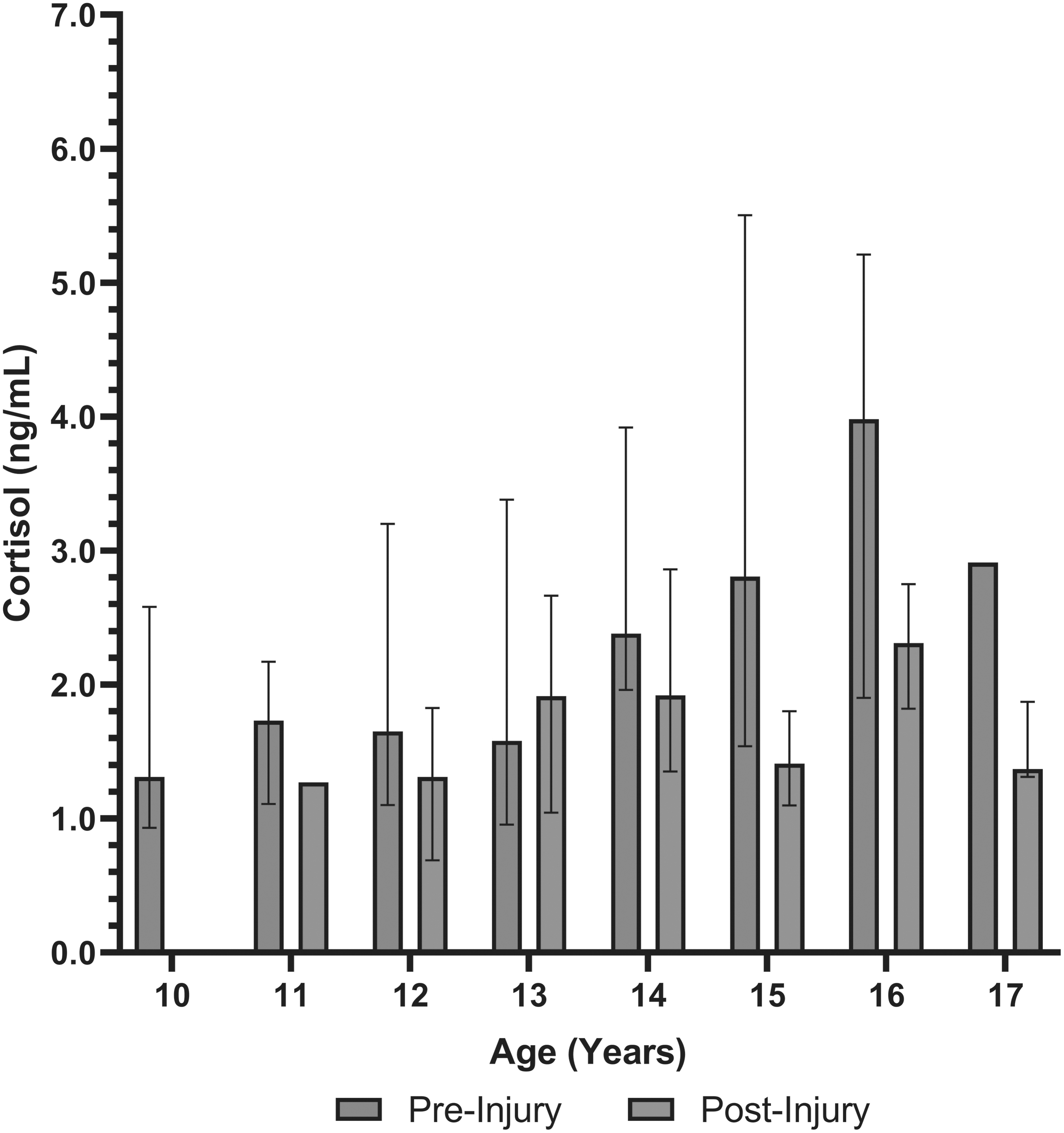
Comparison of median saliva cortisol levels across all ages included in the study in pre-injury and post-injury groups. Error bars represent median and interquartile range. Median quantile regression found a significant association between age and cortisol, whereby a 1-year increase in age was associated with a 0.24-ng/mL increase in cortisol after adjusting for injury group, sex, and history of concussion (β = 0.24, 95% CI [0.12, 0.36], p < 0.001). CI, confidence interval.
Cortisol and total number of symptoms post-SRC
After adjusting for age, sex, history of concussion, and time between injury and saliva collection, there was no significant association between post-injury median cortisol levels and total number of symptoms reported on the SCAT3/SCAT5 (β = −1.49, 95% CI [–3.95, 0.98], p = 0.288). However, there was a significant relationship between sex and total symptoms (β = 6.95, 95% CI [0.35, 13.55], p = 0.040), whereby the expected total in females post-SRC was approximately 7 symptoms higher than post-SRC males after adjusting for cortisol, age, previous history of concussion, and time between injury and saliva collection (Fig. 4). A significant relationship between age and total number of symptoms was also found where the total number of symptoms increased by approximately 2 with each 1-year increase in age (β = 2.25, 95% CI [0.19, 4.31], p = 0.033) controlling for all other variables in the model. No significant association was found between a previous history of concussion and total number of symptoms reported post-SRC (β = 1.15, 95% CI [–4.48, 6.78], p = 0.680) after adjusting for cortisol, sex, age, and time between injury and saliva collection. Lastly, time from injury to sample collection (hours) was not significantly associated with total number of symptoms (β = −0.01, 95% CI [–0.03, 0.02], p = 0.593) after adjusting for all other variables.
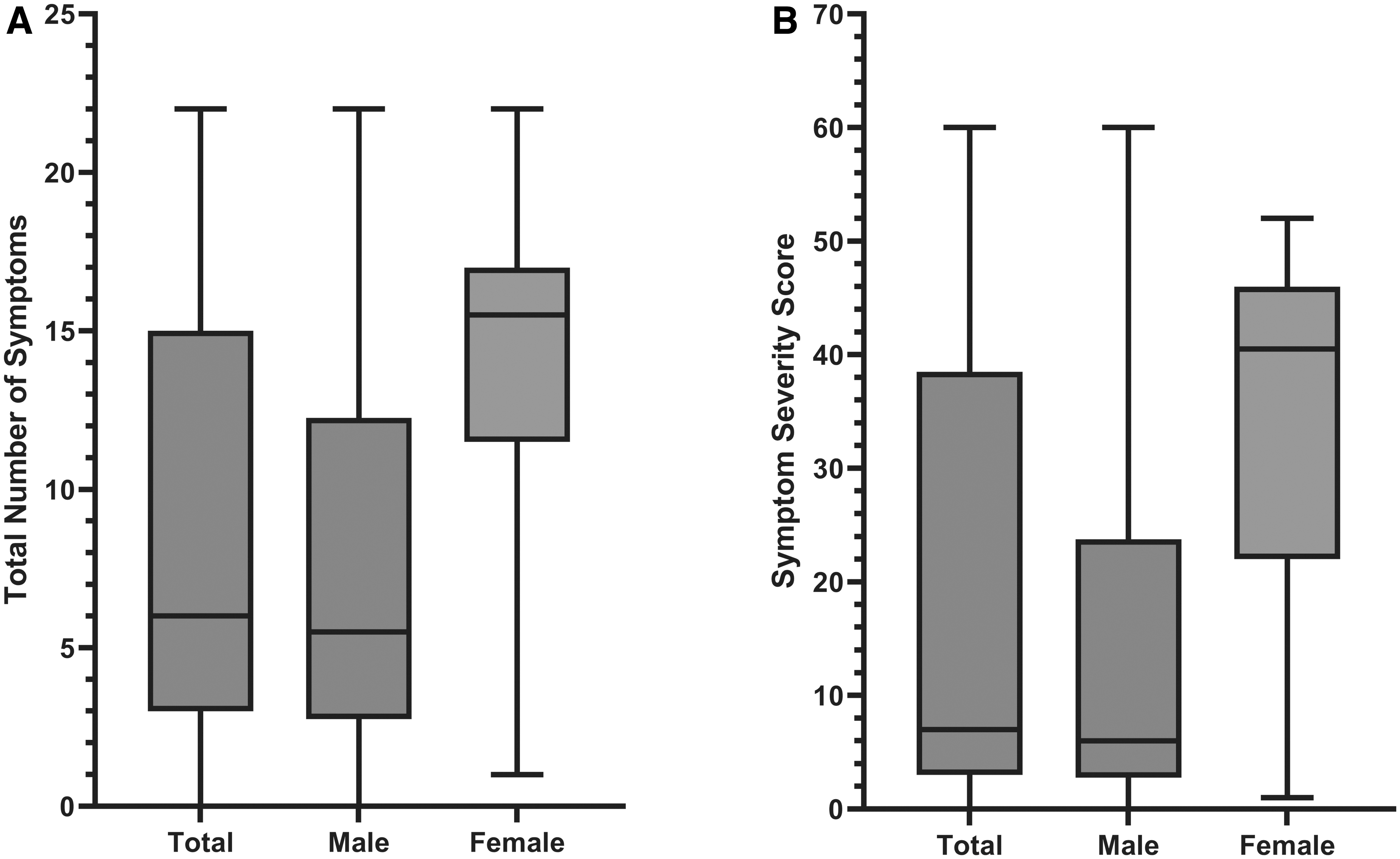
Box and whisker plots of SCAT3 total number of symptoms
Cortisol and symptom severity score post-SRC
Median saliva cortisol levels post-SRC were not significantly associated with SCAT3/SCAT5 symptom severity scores (β = −3.36, 95% CI [–8.69, 1.97], p = 0.209) after adjusting for age, sex, or previous history of concussion. Similar to the total number of symptoms, we found a significant association between sex and symptom severity score (β = 23.87, 95% CI [9.58, 38.15], p = 0.002) whereby females reported a symptom severity score approximately 24 points higher than males post-SRC, controlling for all other variables in the model (Fig. 4). Additionally, our analysis demonstrated an estimated 5-point increase in symptom severity score with each 1-year increase in age after adjusting for cortisol, sex, and previous concussion history (β = 5.03, 95% CI [0.57, 9.49], p = 0.028). The model failed to demonstrate a significant association between previous concussion history and symptom severity score after adjusting for all other variables (β = 2.95, 95% CI [–9.24, 15.14], p = 0.625). Finally, the time between injury and saliva collection (median 114.5 h, IQR [85.9, 229.9]) was not significantly associated with symptom severity score (β = −0.01, 95% CI [–0.06, 0.05], p = 0.680).
Cortisol and days to return to play
Sixty-eight players provided post-injury saliva samples; however, 18 had missing data on days to RTP leaving 50 players for tests concerning recovery time (medical clearance to RTP). Of these 50 post-SRC players, 36 (72%) were cleared to RTP within 28 days of injury (Fig. 5). The median days for clearance to RTP was 19.5 days (IQR: 11–31, 95% CI [13, 26]). Time-to-event analysis was conducted to investigate the influence of post-injury cortisol on length of recovery (days to RTP) adjusting for age, sex, and previous concussion. The point estimate suggests that post-SRC cortisol levels may be associated with length of recovery (hazard ratio [HR] = 1.35, 95% CI [0.90, 2.04], p = 0.148) with 1-unit increase in cortisol potentially associated with a 35% higher hazard of returning to play (i.e., lower saliva cortisol levels post-SRC may be associated with a longer recovery time; Fig. 6).
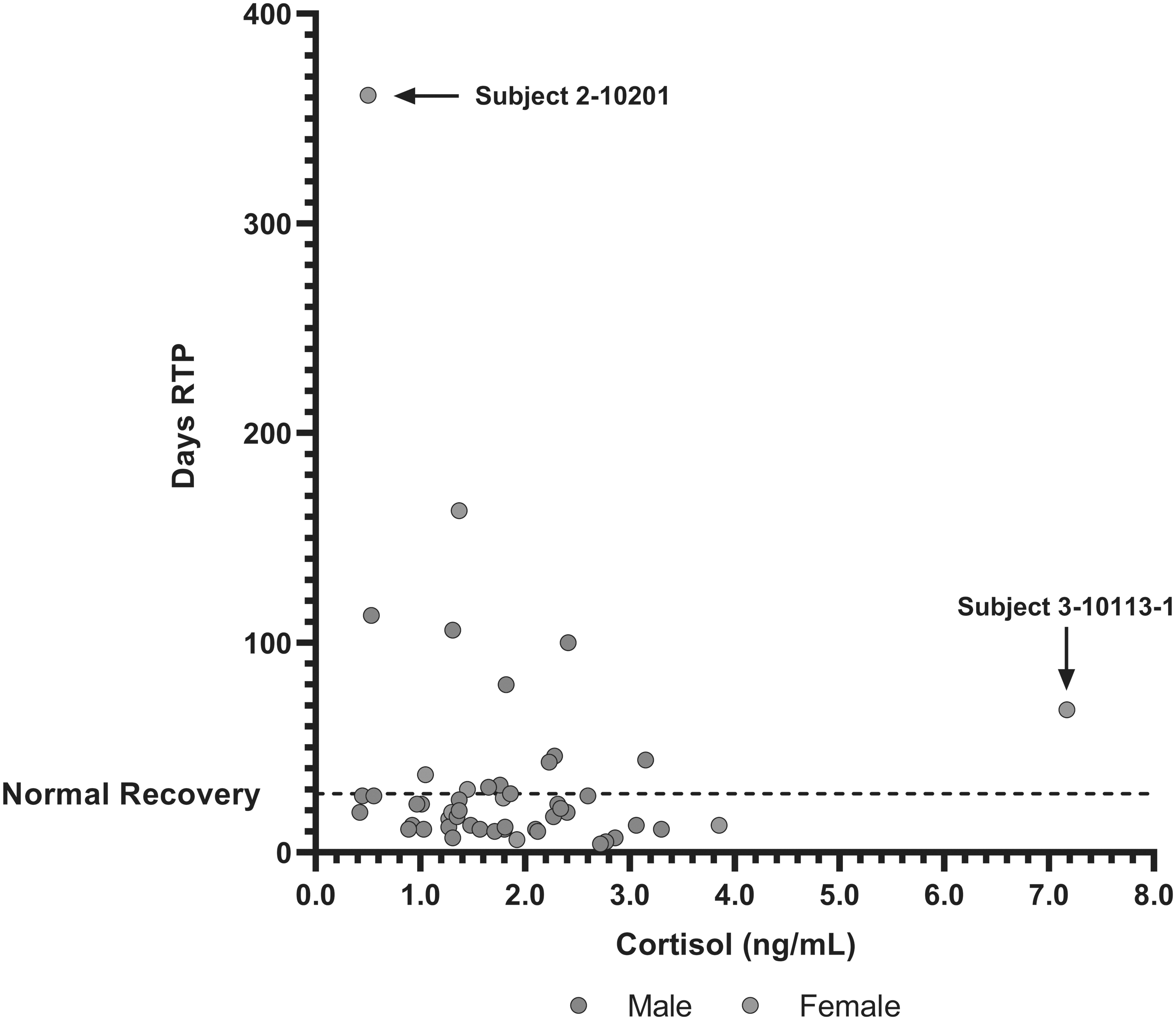
Scatterplot of saliva cortisol (ng/mL) and recovery time (days to RTP) in males and females post-SRC. Dashed line represents upper limit for normal clinical recovery time from SRC in a pediatric population (28 days) and points above this line are considered prolonged recoveries. Two outliers of interest are included in this figure: 1) 16-year-old female (subject ID: 2-10201) with abnormally low post-SRC cortisol levels (0.5 ng/mL; collected 648 h post-SRC, no previous concussions) with the highest days of RTP (361 days) of the post-SRC group, indicative of blunted HPA-axis activity; and 2) 14-year-old female (subject ID: 3-10113-1) with the highest post-SRC cortisol level (7.17 ng/mL; collected 87 h post-SRC, two previous concussions) with a prolonged recovery (68 days to RTP), potentially indicative of HPA-axis hyper-reactivity or neuroinflammatory priming to injury. HPA, hypothalamic-pituitary-adrenal; RTP, return to play; SRC, sports-related concussion.
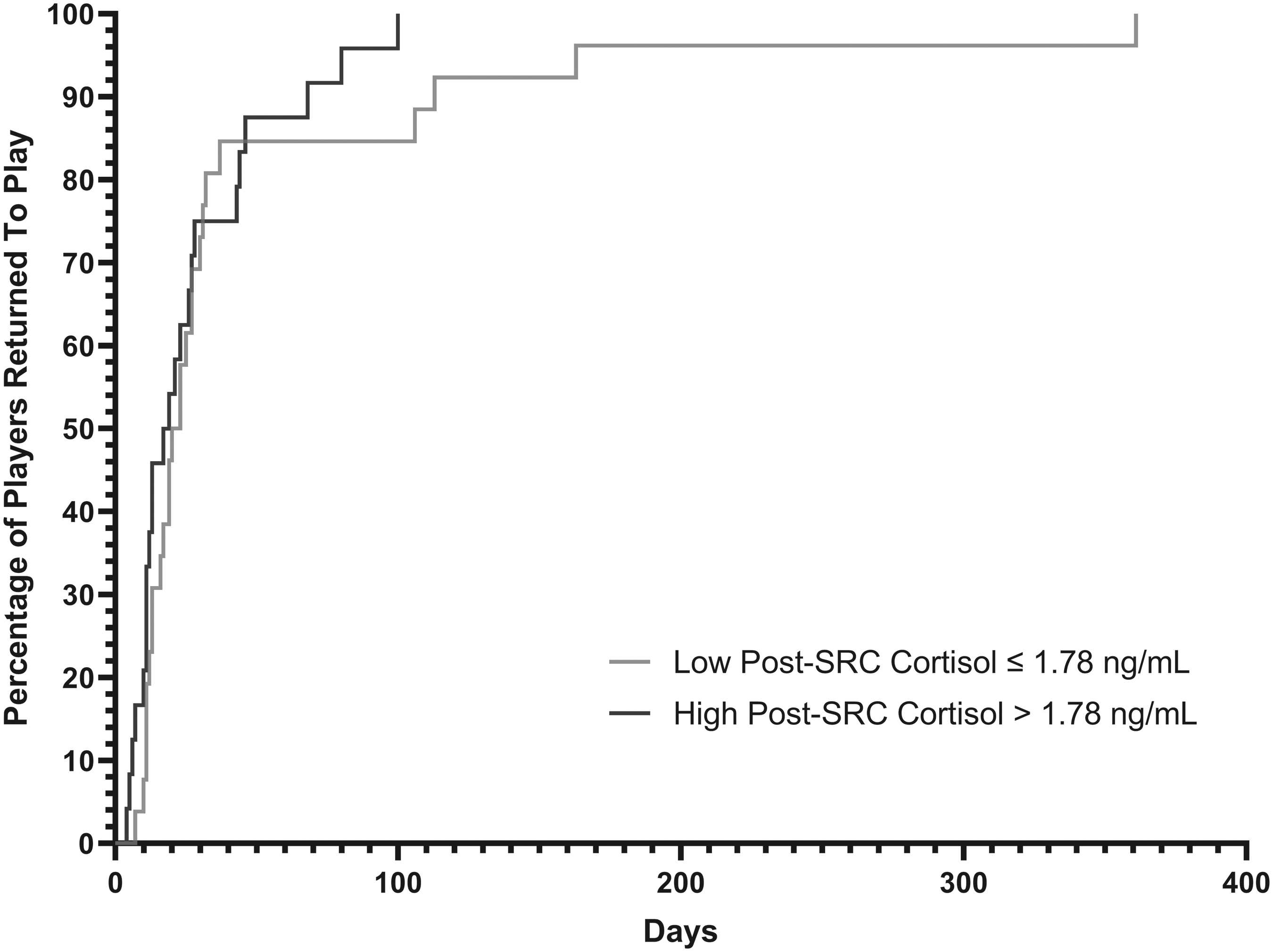
Cumulative incidence of SRC clearance to RTP by cortisol level in players with SRC. Using the median of post-SRC saliva cortisol levels (1.78 ng/mL) athletes were split into high or low groups to visually display the potential association between low post-injury cortisol and longer time to RTP. However, time-to-event analysis found this association was not statistically significant (HR = 1.35, 95% CI [0.90, 2.04], p = 0.148) and the survival curves above were not significantly different (log-rank test p = 0.281). CI, confidence interval; HR, hazard ratio; RTP, return to play; SRC, sports-related concussion.
Discussion
This study investigated saliva cortisol levels in youth ice hockey players as a possible biomarker of SRC. Between-group analyses found lower levels of saliva cortisol in ice hockey players acutely (within 1 week) post-SRC when controlling for age, sex, and history of previous concussion compared with players pre-SRC. Further, our results show an association between cortisol and age throughout puberty, regardless of injury status. Our study also demonstrates age and sex differences in post-SRC SCAT3/SCAT5 symptom reporting in this adolescent population. Lastly, our results suggest a potential association between low saliva cortisol levels and delayed recovery time (medical clearance to RTP) in young ice hockey players who sustained an SRC.
Sport-related concussion and saliva cortisol
The HPA axis is responsible for regulating the systemic response to stress and injury through cortisol-mediated mechanisms. In a normal stress response, cortisol helps regulate post-injury inflammation, tissue repair processes, and the restoration of homeostasis. 13,14 However, in some cases TBI may damage the pituitary, resulting in a dysregulated HPA response to injury. 17 This may present as hypopituitarism post-TBI, which has been previously demonstrated in all severities of TBI, 20 where cortisol deficiency may require urgent intervention. 24 In studies of moderate to severe TBI, acute hypocortisolemia has been associated with poor long-term outcomes and increased mortality. 25 Permanent and transient HPA deficiencies are prevalent following severe TBI; however, few studies have explored HPA-axis dysfunction following SRC. Altered hormonal release following SRC may be related to direct injury to the HPA axis, alterations in the modulation of the axis, or may represent functional adaptations. Recent literature has begun to show variations in HPA-axis function after mTBI, with some studies showing mixed findings after SRC. 30 –32
Results from the current study suggest that following SRC there is an acute decrease in saliva cortisol within the first week post-injury (see Fig. 2). Salivary measurements in this study suggest alterations in cortisol secondary to disruption of the HPA axis can occur following SRC. These findings are in line with a previous S2P sub-cohort case series that examined serum cortisol post-injury, where 4/15 players were described as having abnormally low cortisol. 32 Although these were preliminary findings, the prevalence is consistent with the previously reported prevalence of HPA-axis dysfunction seen in SRC and mTBI (15–46.6%). 16,20,23 A strength of the current study lies in the feasibility of collecting saliva post-SRC rather than serum in a pediatric population, resulting in a large enough sample size to demonstrate a statistical association between SRC and cortisol levels. However, this result conflicts with those in a study by Hutchinson and colleagues that did not find any differences in saliva cortisol post-SRC. 31
Divergent findings may be explained by differences in collection protocols concerning time of day. The study described above collected saliva in the afternoon to avoid the diurnal influence on cortisol, whereas our current study chose to sample between 7:00 and 10:00 a.m. to capture peak physiological levels, 36 which arguably would reflect larger effect sizes in cortisol if a blunted HPA-axis response occurred. It should be noted that a 0.6-ng/mL difference in salivary cortisol between study groups may reflect impairment to the HPA axis, specifically concerning its involvement with circadian rhythm. For instance, a recent study using saliva cortisol found blunted cortisol awakening responses and lower diurnal cortisol amplitudes in subjects with recently sustained mTBIs at both initial and 1-week follow-up time-points. Further, these decreases in cortisol (at similarly low concentrations as the current study) were associated with greater symptom severity. 37 Given the complex interactions between circadian rhythms, the HPA axis, and commonly reported sleep dysfunction post-concussion, future research would benefit from serially collecting saliva cortisol throughout the day and over time to further interrogate the interaction between diurnal cortisol, the cortisol awakening response, and SRC outcomes.
Modeling also revealed an association between cortisol and age after adjusting for injury group, sex, and previous history of concussion. As seen in Figure 3, cortisol increased with age, regardless of injury group. This finding highlights the importance of developing age-specific reference ranges when examining cortisol as a biomarker for brain injury given that basal HPA-axis activity increases throughout puberty. 38 Morning cortisol levels have also been positively related to body weight increases throughout healthy growth across adolescence. 39 Although, it is difficult to attribute these increases in cortisol exclusively to development given the increased HPA-axis activity related to social and emotional experiences throughout puberty. 40 Lastly, we did not see an association between sex and cortisol levels across both pre-injury and post-SRC groups, perhaps due to the small sample of females in the post-SRC group (n = 13). Future studies with larger cohorts may find significant cortisol changes in females given the intimate relationship between cortisol and sex hormone axes in addition to consistent reports of greater symptom burden in females. 41 –43
The influence of sex and age on symptom burden post-SRC
As mentioned above, we did not observe any associations between saliva cortisol and sex; however, when examining the post-SRC group we found that females on average reported more symptoms and greater symptom severity than males. These results support a growing body of literature around females reporting higher symptom burdens post-SRC. 42,43 These differences may be attributed to discrepancies in concussion reporting between sexes, 44 yet there may be a biological basis for this association. Emerging research is beginning to show that female menstrual cycles may be influenced by SRC, where damage to the pituitary may interfere with regulation of sex hormones. 45 A disrupted menstrual cycle may influence recovery after brain injury given the neuroprotective, anti-inflammatory, and cerebrovascular effects of estrogen and progesterone. 46,47 Unfortunately, our study did not collect data on sex hormones and menstrual cycle function, but the growing literature surrounding female athletes suggests these variables should be investigated in future SRC studies.
Results also showed an increase in symptoms and severity scores in older players, which could reflect developmental differences in symptom reporting. Older players may have a greater ability to accurately conceptualize and report symptoms they experience. 48 The variability of puberty onset likely played a role in this association too as hormone function and brain development changes drastically across the age range selected for our study. Further, SRC outcomes in adolescents are confounded by social and psychological effects influencing symptom reporting and recovery. 48,49 These findings reinforce the complexity involved in the symptomology and the associated pathophysiology in this vulnerable population. Future studies may benefit from collecting information on pubertal status when investigating any developmental influences on the clinical presentation of SRC in pediatric athletes.
HPA-axis dysfunction and time to return to play
A pitfall in the current SRC biomarker literature lies in the limited associations found between pathophysiology and clinical recovery. 12 Whereas the median days to RTP was approximately 19.5 days, a substantial portion of our sample took longer than the typical 28 days for adolescents to recover (see Fig. 5). 4 Our exploratory analysis found a potential link between low cortisol levels and days to RTP after SRC, although this association was not statistically significant (likely a function of our small post-SRC sample size; see Fig. 6). The typical response to brain injury involves activation of the HPA axis, resulting in increased cortisol to both mobilize energy stores and dampen neuroinflammation to mediate a normal recovery. 13,15,50 However, as seen in a previous study by our lab group and the current study here, the pituitary may be impaired in a small proportion of athletes leading to a dysfunctional HPA axis, potentially prolonging recovery. 32
Cortisol has potential as a prognostic biomarker after SRC, but many variables are impeding its clinical validation. First, our results here and those in previous studies suggest that pituitary impairment only occurs in a small percentage of SRC due to the heterogeneous nature of concussions. 23,32 Given the estimated prevalence of individuals with acute pituitary dysfunction following SRC is unknown, larger samples of athletes will be needed to adequately study any biomarker associations with clinical measures of recovery. It should be noted that clinically relevant pituitary impairment is typically assessed months post-TBI, well beyond the time window assessed in this study. 24 Further, this study did not perform the diagnostic tests for true adrenal insufficiency, which would require urgent glucocorticoid replacement regardless of cause. Low cortisol levels post-SRC may reflect transiently impaired HPA-axis function rather than overt pituitary damage, which is most accurately diagnosed by dynamic hormone stimulation testing 24 (currently not recommended in this outpatient injury population).
Second, many biomarker studies take a group-level approach to analysis, but fully understanding cortisol pathophysiology may require close examination of outliers in the data. We have singled out two outliers in our study (seen in Fig. 5) that we believe illustrate this point. Subject ID: 2-10201 was a female who presented with the lowest post-SRC morning cortisol (0.5 ng/mL) at 27 days post-SRC, who also had the longest recovery time in our sample (361 days RTP) raising the question of potential impairment to the HPA axis. Conversely, subject ID: 3-10113-1 was a female with the highest post-SRC cortisol levels (7.16 ng/mL) who also had a prolonged recovery beyond the typical 28 days (68 days RTP). This participant also had a history of two previous concussions, which may have resulted in an exaggerated HPA response due to neuroinflammatory priming from previous neurological insults and the associated psychological stress. 15,51 –54 These cases point toward a potential “healthy” range of cortisol in response to brain injury that warrants future investigation. Interestingly, these two case subjects were female, revealing the complexity of their SRC pathology as athletic energy demands, HPA function, and menstrual cycle activity are intimately connected. 55 Ultimately, these outliers demonstrate the need to collect in-depth medical histories and menstrual cycle function in SRC studies involving female athletes.
Further, they demonstrate the potential of cortisol as a prognostic biomarker of SRC in the context of precision medicine as the identification of outliers in research may help develop clinical tools and technologies for cases that deviate from the expected norms. Regular pre-injury saliva screening could also be implemented to establish individual baseline cortisol levels to detect post-SRC abnormalities, further improving SRC management.
Limitations
The results presented herein must be interpreted with caution considering the limitations of the study. First, we recognize that our analysis involved two separate groups of participants given data were collected from a convenience sample (pre-injury vs. post-SRC). Future studies should attempt to acquire pre-injury samples on all players allowing for within-group analyses to better interrogate changes in cortisol due to SRC. Second, this study had a wide range of time between injury and saliva acquisition, likely introducing variation into our investigation. Some samples may have been collected outside the window of time needed to detect the strongest changes in cortisol post-SRC. A problem intrinsic to any study evaluating cortisol includes the necessity to sample peak physiological cortisol levels upon wakening due to diurnal variation. 35,56 This resulted in extended times between injury to sample collection, in addition to the exclusion of a large portion of saliva samples acquired in both study groups.
Last, there was an uneven ratio of male to female players in each study group, which decreased our abilities to capture and comment on potential associations between cortisol levels and sex. We also did not collect information on menstrual cycle function, which in future studies will help investigate the relationship between SRC, HPA axis, and female sex hormones in a very understudied population in the SRC biomarker literature. However, to our knowledge this is only the second study in the literature investigating acute hormone changes post-SRC in a pediatric population. A major strength of this study lies in the demonstrated feasibility of saliva collection from youth athletes as a medium for cortisol analysis. However, until saliva cortisol becomes a recommendation for assessment of HPA-axis dysfunction, it may prove useful to collect serum samples in conjunction. Future research would also benefit from cortisol sampling at a ≥3-month follow-up in those who displayed acutely low cortisol to assess clinically relevant long-term outcomes. Further, our findings do not rule out the possibility that lower cortisol may play a functional or adaptive role after SRC, warranting continued research into the HPA axis and brain injury.
Transparency, rigor, and reproducibility
This study was not formally registered as it was a longitudinal cohort study. The analysis plan was not formally pre-registered. The S2P longitudinal cohort study planned for approximately 5000 pre-injury and 425 concussion subjects (with actual sample size being 4747 pre-injury and 300 concussion subjects). The sub-cohort that provided samples for this study included 202 pre-injury samples and 133 post-SRC samples (note: pre-injury and post-SRC samples were not from the same individuals as these groups were from a convenience sample). Saliva samples were excluded (37 pre-injury, 65 post-injury) resulting in a final sample size of 165 pre-injury samples and 68 post-SRC samples included for data analysis. Figure 1 shows a summary diagram of participant recruitment and sample exclusions.
Human participants were blinded to results of the saliva cortisol measurements. Saliva cortisol measurements and quality control decisions and analyses were performed by investigators blinded to relevant characteristics of the participants. Saliva samples were labeled using codes linked to subject identification information. Saliva samples were acquired between the 2014 and 2018 ice hockey seasons between 7:00 a.m. and 6:00 p.m. (however, only samples collected between 7:00 and 10:00 a.m. were included). Post-SRC samples were acquired between 6 and 72 h post-injury at the University of Calgary Sports Medicine Centre using the clean drool technique in saliva collection tubes and were stored at −80°C for 4–6 months until analysis. Saliva samples underwent one freeze-thaw cycle for LC/mass spectrometry (MS) analysis (see Methods section) in two separate batches, with samples assigned to batches in the order they were acquired. No technical failures requiring replication occurred in samples or batches. The LC/MS analyses were validated for research use only, with only one replicate per sample, and cortisol LLOQ being 0.1 ng/mL. Analytical reagents and equipment used for cortisol analysis are available from commercial sources.
The key inclusion criteria and primary clinical outcomes (SRC diagnosis and SCAT3/5 symptom reporting) are established standards in the field, assessed by investigators with professional qualifications (sports medicine physicians and study therapists performing clinical assessment). Quantile median regression was used as data did not meet assumptions of normality for multi-variable linear regression. Proportional hazard assumptions were met for Cox regression analysis. Estimates and 95% CIs have been reported in the abstract for primary outcomes and in the main text for all outcomes. Replication and external validation studies by the study group are ongoing. Data from this study are not available in a public archive. There is no analytic code associated with this study. All saliva samples used to conduct the study were obtained from youth athletes in the Calgary, AB area and no future use is possible as all samples were used for the current analysis. The authors agree to provide the full content of the manuscript on request by contacting Jason Tabor.
Conclusions
Saliva cortisol may serve as a useful non-invasive prognostic biomarker of pediatric SRC in those who may have impairment in the HPA axis. The current study found lower levels of cortisol in youth ice hockey players who recently sustained a SRC compared with healthy controls. We also found female players to report higher symptom burden on average compared with males post-SRC. Exploratory time-to-event analysis revealed a potential association between lower cortisol levels and longer recovery times post-SRC. Interestingly, when examining outliers in post-SRC cortisol data, we found participants with the highest and lowest levels to be females who suffered prolonged recoveries. Although preliminary, these cases potentially hint toward a dynamic interplay of female sex hormones and the HPA axis in relation to clinical recovery. Overall, our findings show that cortisol may be a key target when investigating fluid biomarkers of pediatric SRC recovery and its value may lie in the individualized sex-specific treatment for those suffering prolonged recovery times.
Footnotes
Acknowledgments
The authors thank Hockey Canada, Hockey Calgary, Hockey Edmonton, and all the players, coaches, and parents involved in this study. We greatly thank all the students and research staff involved in the data collection for this study. Special thanks to Stacy Sick for coordination of clinics and sample collection. The Sport Injury Prevention Research Centre is one of 11 International Olympic Committee Research Centres for the Prevention of Injury and Protection of Athlete Health.
Authors' Contributions
All authors contributed to the writing and development of this article. Authors CE and CD were involved in study conceptualization and design. Authors PL, MM, and KWE had major roles in acquisition of data. Authors JT, PL, GK, MW, SB, KWE, CE, and CD were involved in analysis and interpretation of the data. Authors JT, PL, GK, MW, KWE, CE, and CD were involved in writing, revision, and finalizing the manuscript.
Funding Information
This study was funded by Canadian Institutes of Health Research (grant #293332). Author JT is funded by the Canadian Institutes of Health Research (CIHR).
Author Disclosure Statement
No competing financial interests exist.