
Abstract
The demographics of acute traumatic spinal cord injury (SCI) have changed over the last few decades, with a significant increase in age at the time of injury, a higher percentage of injuries caused by falls, and incomplete tetraplegia becoming the most common type of neurological impairment. Incomplete SCI syndromes, most specifically central cord syndrome (CCS), anterior cord syndrome (ACS) and Brown-Sequard syndrome (BSS), constitute a substantial proportion of incomplete tetraplegia and SCI overall. Nevertheless, the updated incidence of these syndromes is not well known, and their estimates vary considerably, largely because of methodological inconsistencies across previous studies. A retrospective analysis of individuals with new traumatic SCI enrolled in the Spinal Cord Injury Model Systems database between January 2011 and May 2020 was performed. Using newly proposed computable definitions for ACS and BSS, as well as an existing quantitative definition of CCS, we determined the current incidence and neurological characteristics of each syndrome. Within the population of individuals with a traumatic SCI, including all levels and severity of injuries (N = 3639), CCS, ACS, and BSS accounted for 14%, 6.5%, and 2%, respectively. Of the 1649 individuals with incomplete tetraplegia in our cohort, CCS was the most common syndrome (30%), followed by ACS (10%) and BSS (3%). Using quantifiable definitions, these three syndromes now account for ∼22% and ∼44% of cases of traumatic SCI and incomplete tetraplegia, respectively, with CCS having increased over the last decade. This updated information and proposed calculable criteria for these syndromes allow for a greater understanding of the incidence and characteristics of these syndromes and enable greater study in the future.
Introduction
Demographics of acute traumatic spinal cord injury (SCI) have changed over the last few decades with a dramatic shift in the characteristics of this patient population by age, etiology, and level and severity of injury. Studies from multiple countries have shown similar patterns of change to the composition of the SCI population over time, including an older mean age at injury, a higher percentage of injuries caused by falls, and a larger prevalence of incomplete tetraplegia. 1 –5
In the United States, the national Spinal Cord Injury Model Systems (SCIMS) database has shown that from the 1970s to 2020, the average age at injury increased from 29 to 43 years, and the percentage of SCI caused by falls nearly doubled from 16.5% to 32.2%. 6 In addition, incomplete tetraplegia is now the most common type of neurological impairment, comprising 47.4% of all SCI in the United States, compared with only 29.6% in 2001. 1,7 The increased prevalence of incomplete tetraplegia has resulted in a greater need to understand the occurrence of tetraplegia-specific syndromes to more effectively design and target interventions for this large portion of persons with SCI.
There are a number of syndromes described for persons with incomplete SCI. These include central cord syndrome (CCS), Brown-Sequard syndrome (BSS), and anterior cord syndrome (ACS). 8 CCS is a clinical syndrome following a cervical SCI, resulting in disproportionately greater weakness of the upper limbs compared with the lower limbs. 9 While there have been numerous criteria used to define CCS, 9 –14 the European Multicenter Study on Human Spinal Cord Injury (EM-SCI) study group 15 classified the syndrome by using a difference of at least 10 motor points in favor of the lower extremities. This quantitative definition does not rely on clinical interpretation, which was occasionally used in earlier reports. 16 –18
BSS, in its pure form, is an incomplete syndrome consisting of ipsilateral paralysis (hemiplegia) and loss of proprioception with contralateral hemianalgesia (loss of pain and temperature sensation).
19
Only a limited number of patients, however, fulfill these criteria,
20
and its derivative, Brown-Sequard plus syndrome (BSPS), is much more common. BSPS is defined as a
ACS incorporates a loss of motor function, pain, and temperature sensation at and below the injury level with preservation of light touch and proprioception. 8 Over the years, studies have had significantly different interpretations of the motor loss element ranging from complete paralysis to minimal weakness (allowing only one muscle with less than normal strength). 10,23,24
Because of methodological inconsistencies across previous studies, the full extent of these incomplete syndromes is not well known. A comprehensive review of incomplete syndromes in SCI in 2007 reported that CCS accounted for an estimated 9% of injuries, with BSS at 4% and ACS at 1%, 17 although considerably different proportions were reported elsewhere. 2,25 Most of the studies that characterized patterns of traumatic incomplete syndromes were restricted to persons with tetraplegia, completed 20–50 years ago, and the estimated incidence of each syndrome varied substantially. 23,26,27 For instance, studies have reported that CCS accounted for anywhere from 18–70% of the cases of incomplete tetraplegia, whereas ACS, which was considered to be “relatively rare,” 8 was reported to occur in 20-60% of cases. 23,26,27
The dissimilarities in previously reported estimates are partially attributable to inconsistencies in the criteria used to define the common incomplete tetraplegia syndromes. 21,28,29 With the exception of several studies that used the EM-SCI criteria for CCS 11,30 –34 and a few additional sporadic articles, 10,22 most studies did not use quantitative definitions to classify these syndromes, instead relying on clinical interpretation.
The objective of this study was to determine the more recent distributions of incomplete syndromes in acute traumatic SCI, most specifically with tetraplegia, utilizing clear and quantifiable definitions. This information would allow for a greater understanding of their current incidence and highlight the importance of more specific definitions for these syndromes.
Methods
Sample
This investigation is a secondary analysis of existing data obtained from persons with traumatic SCI enrolled in the SCIMS database between January 2011 and May 2020 (N = 5743). Before 2011, individual dermatome light touch and pinprick scores were not included in the database, interfering with the ability to determine specific criteria for the incomplete syndromes. The details of the SCIMS database are described elsewhere. 35
Briefly, the database is a prospective longitudinal follow-up study of the demographics, injury characteristics, and long-term health, functioning, and well-being of persons who complete acute inpatient rehabilitation for traumatic SCI at a designated SCI Model System center in the United States. All participants provided informed consent according to protocols approved by the Institutional Review Boards of the designated centers.
The analytic sample retained for this investigation (N = 3639) was based on the following criteria: (1) ≥16 years of age at time of injury; (2) a complete neurological examination between three and 30 days of injury. Further subanalysis of individuals with incomplete tetraplegia only was performed including those with a cervical SCI (neurological level of injury [NLI] C1–C8) and an American Spinal Injury Association (ASIA) Impairment Scale (AIS) grades of B, C, or D (n = 1649). A flowchart of patient inclusion and exclusion is presented in Figure 1.

Flowchart of patients in the Spinal Cord Injury Model Systems database for inclusion in the study. SCI, spinal cord injury; ISNCSCI, International Standards for Neurological Classification of Spinal Cord Injury; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Measures
Measures of demographics and injury characteristics included age, sex, etiology of injury, as well as NLI and severity (AIS) according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI).
CCS
Consistent with recent studies,
11,30
–34
CCS was defined by the following equation using lower extremity motor score (LEMS) and upper extremity motor score (UEMS):
15
BSS
In this investigation, the term BSS applies to both the pure syndrome and BSPS, as has been described previously. Because there is no consistent calculable definition available for BSS, we used the following quantifiable criteria for BSS: (1) marked asymmetry of motor scores between the sides, if almost all key myotomes below the motor level of injury were weaker on the ipsilateral side (allowing only one key myotome to have the same motor score as the contralateral side), (2) more pinprick sensory impairment on the stronger (contralateral) side, defined as at least half of the ipsilateral (weaker) side pinprick scores below the NLI being greater than their counterparts. See Figure 2 for an example.
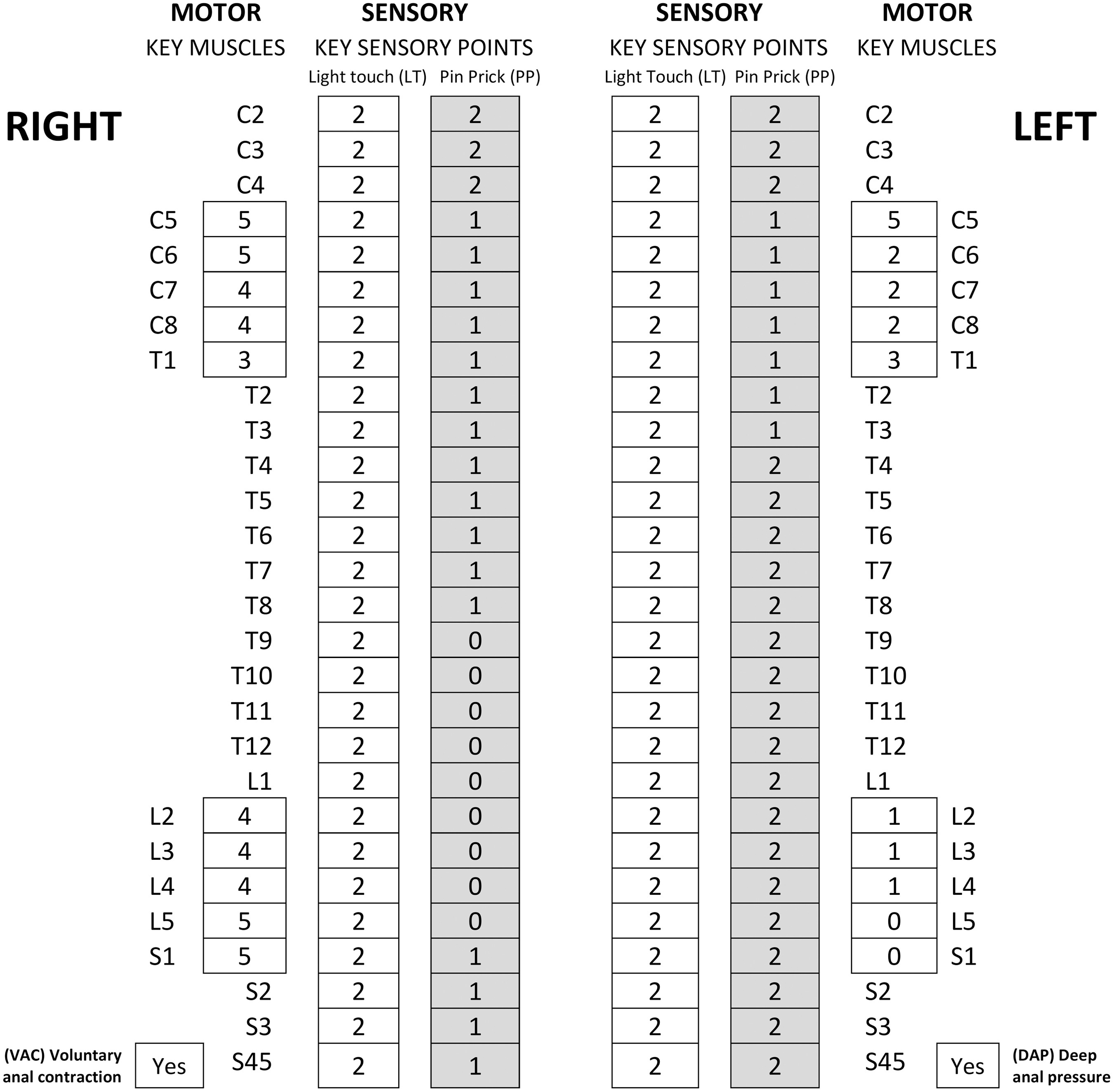
An example of our definition for an individual with Brown-Sequard syndrome (BSS).
ACS
ACS was identified as an incomplete syndrome with substantial motor weakness reflected by AIS grades of B or C and significant loss of pinprick sensation compared with light touch sensation, with at least half of the dermatomes below the NLI having a greater light touch score than their parallel pinprick score on each side. See Figure 3 for an example.
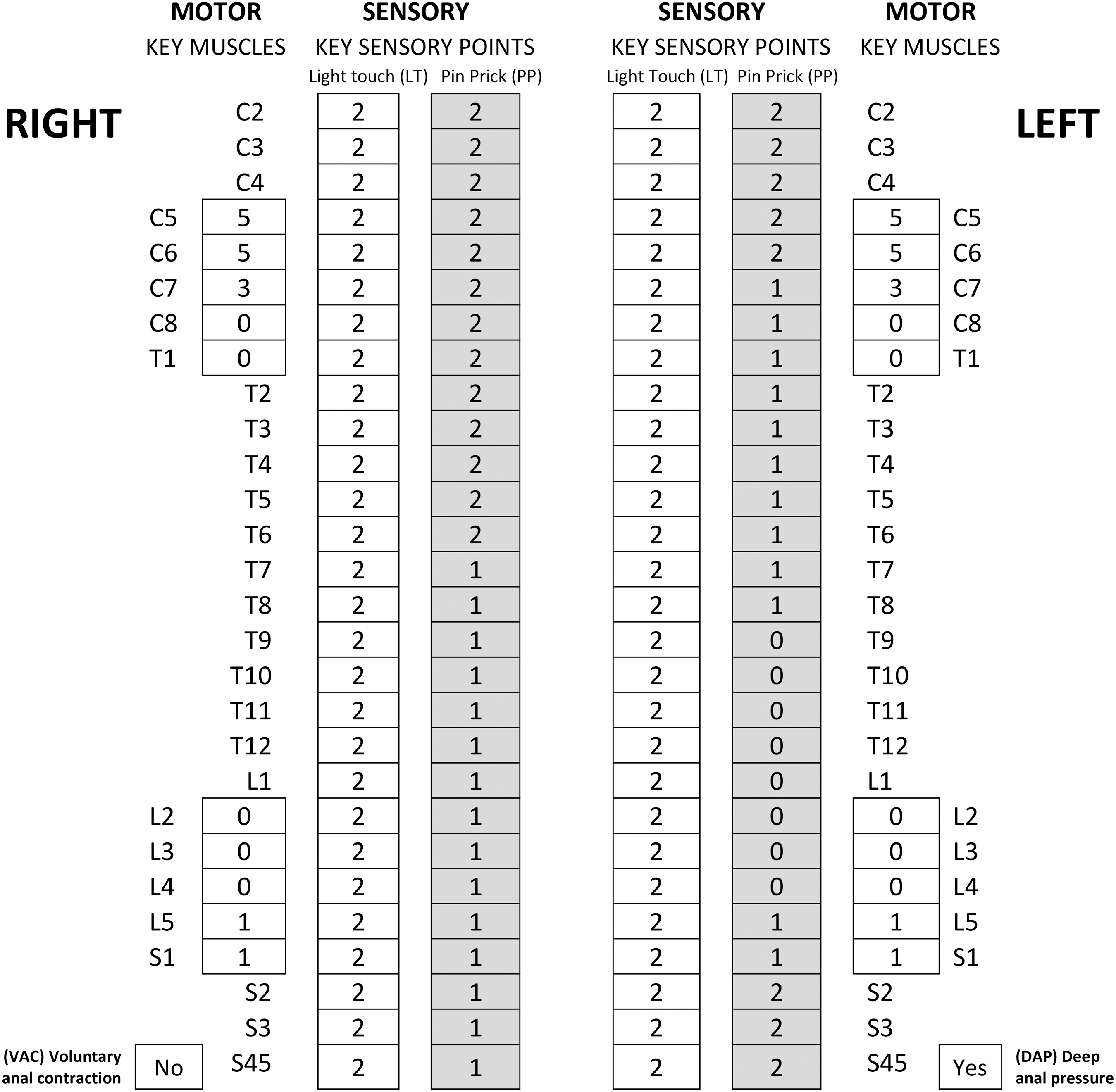
An example of our definition for an individual with anterior cord syndrome (ACS).
In the event of a case fulfilling the criteria for more than one syndrome, cases were classified according to the following priority: BSS first because it has the most distinct neurological characteristics, followed by ACS, and ultimately CCS, because it has the least specific definition, only including motor (without sensory) scores.
Statistical analysis
A descriptive analysis of patients' characteristics was completed with absolute and relative frequencies for categorical variables and means (standard deviation, SD) for continuous variables. A one-way analysis of variance (ANOVA) was used to identify differences in age between incomplete tetraplegia subgroups.
Results
Sample characteristics
The distributions of the sample characteristics are presented on Table 1. For the full sample of persons with traumatic SCI (N = 3639), CCS accounted for 14% (n = 499), ACS for 6.5% (n = 236), and BSS for 2% (n = 71). All syndromes were more common in individuals with tetraplegia compared with paraplegia; CCS is 100% tetraplegia by definition, and persons with ACS and BSS had tetraplegia in 72% (169/236) and 77% (55/71) of cases, respectively.
Distributions of Sample Characteristics of Individuals with a Traumatic Spinal Cord Injury for the Full Sample and Subsample of Incomplete Tetraplegia Only
AIS, American Spinal Injury Association (ASIA) Impairment Scale; NLI, neurological level of injury; CCS, central cord syndrome; BSS, Brown-Sequard syndrome; ACS, anterior cord syndrome; SD, standard deviation.
For the subsample of cases with incomplete tetraplegia (n = 1649), 30% (n = 499) met the criteria for CCS, followed by 10% (n = 169) with ACS and 3% (n = 55) with BSS. Of note, 27 individuals fulfilled criteria for both ACS and CCS, representing 5% (27/499) of CCS cases and 16% (27/169) of ACS cases. Fourteen individuals met the criteria for BSS and CCS, accounting for 3% (14/499) of CCS and 25% (14/55) of BSS cases. One case met the criteria for all syndromes.
The distributions within incomplete tetraplegia of the syndrome categories (CCS, ACS, BSS, and unclassified cases of incomplete tetraplegia) with age, sex, injury severity and level, as well as etiology are presented in Table 2. Those in the CCS subgroup were older compared with the other subgroups and were more likely to have sustained a SCI from falls. AIS D was far more common among individuals with CCS and BSS, whereas not as common for the unclassified group. C4 was the most common level of injury across all groups.
A Comparison of Patient Characteristics between Central Cord Syndrome, Anterior Cord Syndrome, Brown-Sequard Syndrome, and Unclassified Incomplete Tetraplegia (N = 1649)
CCS, central cord syndrome; ACS, anterior cord syndrome; BSS, Brown-Sequard syndrome; SD, standard deviation; AIS, American Spinal Injury Association (ASIA) Impairment Scale; NLI, neurological level of injury.
Studies of Incomplete Syndromes in Spinal Cord Injury
SCI, spinal cord injury; CCS, central cord syndrome; BSS, Brown-Sequard syndrome; ACS, anterior cord syndrome; LEMS, lower extremity motor score; UEMS, upper extremity motor score.
CCS defined as LEMS - UEMS ≥10.
Including individuals with non-traumatic etiologies.
5% of individuals with CCS had a complete injury.
ACS defined as quadriparesis or quadriplegia and hypalgesia below the level of the lesion in the presence of varying degrees of preservation of touch, position, motion, and vibration sense. The motor paralysis is more severe in the lower than it is in the upper extremities.
Any difference between left and right total motor or total sensory scores was considered an asymmetrical left–right neurological deficit.
Only including individuals with motor incomplete SCI.
The difference in the distribution of age by syndrome was significant (F(3,1645) = 17.179, p < 0.0001). Bivariate comparisons were not tested for the other characteristics because of the occurrence of null and low frequency counts in certain variables in Table 2. A similar analysis was not performed in the whole cohort given the majority of individuals with SCI syndromes have tetraplegia.
Discussion
Given the steady increase in the incidence of new traumatic incomplete cervical SCI over the last few decades, this study presents updated epidemiological results focused on SCI incomplete syndromes, most specifically in tetraplegia, using computable definitions for syndromes that did not previously have one—i.e., ACS and BSS. Our results indicate that CCS is the most common syndrome in persons with SCI (14%), followed by ACS (6.5%) and BSS (2%), as well as in patients with incomplete tetraplegia with 30%, 10%, and 3%, respectively.
In previous reports, there was a significant variation in the occurrence of these syndromes, mainly because of a combination of factors: (1) demographics of SCI have changed, (2) a lack of clear definitions for these syndromes, often using a clinical interpretation and not a unified quantifiable definition, and (3) different populations being studied.
While some studies included individuals with all types of traumatic SCI (complete or incomplete injuries, with paraplegia or tetraplegia), 2,17,25,30,36 –40 others incorporated only individuals with tetraplegia, neurologically complete and incomplete, 41 –43 while others only included individuals with incomplete tetraplegia. 21,23,26,27,36,44 Even within studies that described a specific population, there were often variations in the inclusion criteria—e.g., including individuals with non-traumatic SCI etiology. 17 See Table 3, with our findings listed for comparison.
Based on our results, the following is a summary of current information regarding incomplete syndromes in SCI.
CCS
Of persons with traumatic SCI, 14% met the criteria for CCS. This represents an increase in incidence of CCS over time, as two previous studies conducted a decade ago using the same criteria reported a lower proportion of CCS with 8–11% of cases. 30,36 The rise in incidence was also displayed in a study that used an unquantifiable definition for CCS and demonstrated an increase in CCS cases from 25% in 2000 to 37% in 2010. 2 This is not surprising, given the increase in falls over the last few decades as an etiology for SCI. 45,46 Our report also represents an increase from an oft referenced article stating that CCS accounted for 9% of total SCI, although unquantifiable criteria were used and SCI of non-traumatic etiology was also included. 17
In the subanalysis of individuals with incomplete tetraplegia, our report of 30% with CCS is similar to other relatively recent rates of 23% as recently reported in a doctoral thesis, 44 and 39%, 36 utilizing the same criteria, although the latter was obtained in a cohort of motor incomplete tetraplegia whereas our sample included all patients with motor complete and incomplete injuries. Our study was consistent with previous reports on individuals with CCS with falls being responsible for half of the CCS cases, being more prevalent in older individuals, and having an initial AIS D classification. 2,36
Only 2% of individuals with CCS had an NLI of C6 or below in our report, compared with 7% in a study by Pouw and associates 36 using the same criteria, both of which are lower than 20% of individuals reported by McKinley and colleagues. 17 The likely explanation is that the definition used for CCS based on the EM-SCI definition more often excludes cases of lower cervical injury.
BSS
The proportion of BSS (in this study we included pure BSS and BSPS) of the whole traumatic population was 2%, compared with 3–4% reported in other earlier studies. 17,25,38 Within our cohort of individuals with BSS, 77% had tetraplegia. This is consistent with McKinley and colleagues 17 reporting that 87% (n = 26) of individuals with BSS had tetraplegia.
The finding of only 3% of individuals with incomplete tetraplegia meeting criteria for BSS in our study is lower than previous reports for BSS in this population, ranging between 8–23%. 21,23,26,27,47 Most of these previous studies, however, did not specify or quantify the criteria that were used for BSS. 23,26,27 Pouw and coworkers 21 used liberal criteria, with “Differences of >0 between left and right ASIA total motor and total sensory scores were considered asymmetric left–right neurological deficits,” and subsequently, the proportion of BSS was highest in this study (23%). We used a quantifiable definition that enforced more marked motor and sensory differences between the sides, because these syndromes should have distinct neurological features.
Similar to CCS, almost 75% of individuals with BSS and incomplete tetraplegia had an AIS D injury, comparable to previous reports. 17,21 Only 4% of individuals had a lower cervical NLI (i.e., C6–C8), while other studies demonstrated a higher percentage ranging from 10–35%. 17,19,21 Because BSS is relatively rare, however, all studies included a limited number of participants—between 30 and 38 in other studies 17,19,21 and 55 in this study, a possible explanation for the inconsistencies.
An earlier study by Merriam and coworkers 41 discussed the co-occurrence of BSS and CCS cases. Of those classified with CCS, marked BSS was observed in 14%, and an additional 18% had a mild BSS (no definition was provided for marked or mild BSS). Similar numbers were described by Dvorak and associates 48 reporting 16% (11/70) of individuals with CCS also had BSS. In our study, only 3% of individuals with CCS had a concurrent BSS, probably because these syndromes were classified using differentiated quantifiable definitions, hence creating less overlap.
ACS
Within the broad population of individuals with SCI, 6.5% qualified as ACS, compared with 1% in a study by McKinley and colleagues 17 and 11% in another report, 25 each using different inclusion criteria for the syndrome. ACS remains fairly prevalent despite the ISNCSCI description of it being “relatively rare.” 8 In this investigation, most individuals with ACS had tetraplegia rather than paraplegia, with a ratio of 2.5:1. McKinley and colleagues 17 displayed opposite characteristics, as only one individual with ACS had tetraplegia, compared with seven with paraplegia.
We also report 10% of individuals with incomplete tetraplegia fulfilling our proposed criteria for ACS, which is lower than previously described for this population, of 20–60%. 23,26,27 These studies, however, were completed several decades ago and did not use quantifiable criteria, perhaps contributing to the differences and inconsistencies in the reporting of proportions. In the proposed definition, marked weakness including only individuals with AIS B and C injuries and impairment of pain sensation with significantly lower pinprick than light touch scores were required.
Summary of incomplete syndromes
The three syndromes described in this study accounted for 22% of the traumatic SCI population, while previously accounting for 14–47% in earlier studies. 17,25 Within the cohort of persons with incomplete tetraplegia, these syndromes accounted for 44% in our study, significantly less than the 86–98% described in previous studies. 23,26,27 Of note, the explanation for these high proportions is that in these earlier studies (performed 20–50 years ago), incomplete tetraplegia was almost synonymous with the definitions of incomplete syndromes, and each patient with incomplete tetraplegia was further classified with a syndrome.
This explains the unprecedented high percentage of CCS (70%) 23 or ACS (46–60%) 26,27 observed in these studies, and further highlights the need for this study to describe the incidence of these syndromes using the current classification schema (AIS scale). 8 Further investigation of the characteristics of 56% of individuals with unclassified incomplete tetraplegia is warranted.
Limitations
Although our overall cohort was the largest to date studying incomplete syndromes, some limitations remain. First, despite the relatively large sample size for the full and subsample analyses, small cell sizes for the low prevalence syndromes limit statistical power of the analyses. This study proposed new and quantifiable criteria for BSS and ACS, and these would benefit from validation. Because all of the criteria rely on the ISNCSCI examination, we do not have access to proprioception data, and therefore this component of the examination could not be incorporated into the definitions of ACS and posterior cord syndrome (PCS) (rather light touch was used for posterior column determination). PCS, a lesion that produces loss of proprioceptive sense while preserving muscle strength and pain sensation, 17 was removed from recent ISNCSCI versions 8 because of its rare occurrence and was not investigated in this study. In addition, this study did not discuss cauda equina and conus medullaris syndromes.
For the definition of CCS in this study, we used the EM-SCI definition, which has some inherent limitations, including the exclusion of individuals with a low cervical injury, as well as the inclusion of cases with only unilateral upper extremity weakness. While it has not achieved universal acceptance, it has been used by numerous recent studies 11,30 –34 and therefore was used here. Further work to best define CCS is needed.
Several subjects qualified for the definition of more than one syndrome and were prioritized by BSS, ACS, and CCS. This had little impact on the overall distribution of the syndromes. Last, this analysis did not study these incomplete syndromes as predictors of neurological recovery. Because the majority of subjects with CCS and BSS had an initial AIS D level, there would be a ceiling effect of recovery. Future work however, will focus on functional change.
Conclusions
The SCI syndromes of CCS, ACS, and BSS together constitute ∼22% of traumatic SCI and ∼44% of traumatic incomplete cervical injuries, with CCS presenting most commonly, followed by ACS and BSS. This study proposed a clear computable definition for each syndrome, to allow for a greater understanding of incidence and characteristics as well as enable comparison of the attributes of these syndromes. Further research is required to compare neurological and functional outcomes of these syndromes and to discuss the correlation between these syndromes (using the new quantifiable definitions) and prognosis.
Transparency, Rigor, and Reproducibility Summary
In this retrospective study, 5743 individuals were screened, 3639 retained for the analysis, and 1649 included in the subanalysis. Assumption of normality was not needed because of the large sample size. Individuals with missing data were excluded from the study. Statistical analysis was performed by the corresponding author with expertise in rehabilitation medicine and quantitative data analysis. A limited analysis was conducted because of the occurrence of null and low frequency counts in certain variables. The data are archived in
Footnotes
Acknowledgments
This study was performed in collaboration with the Spinal Cord Injury Model System (US) database.
Authors' Contributions
EEH: Conceptualization; writing–original draft; writing–review and editing; formal analysis. AB: reviewing and editing, formal analysis. BS: reviewing and editing. SK: Conceptualization; writing–original draft; writing–review and editing; supervision.
Funding Information
The contents of this publication were developed under a grant from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR grant number 90SIMS0012).
Author Disclosure Statement
No competing financial interests exist.