
Abstract
Early targeted heart rate (HR) aerobic exercise has been shown to reduce the duration of recovery from sport-related concussion (SRC) as well as the incidence of persistent post-concussive symptoms (PPCS). It is not known, however, if more severe oculomotor and vestibular presentations of SRC benefit from a prescription of aerobic exercise. The current study is an exploratory analysis of two published randomized controlled trials that compared aerobic exercise within 10 days of injury with a placebo-like stretching intervention. Combining the two studies yielded a larger sample size to stratify severity of concussion based on the number of abnormal physical examination signs present at the initial office evaluation, which were confirmed with self-reported symptoms and recovery outcomes. The most discriminant cut-off was between those who had ≤3 oculomotor and vestibular signs and those who had >3 signs. Aerobic exercise (hazard ratio = 0.621 [0.412, 0.936], p = 0.023) reduced recovery times even when controlling for site (hazard ratio = 0.461 [0.303, 0.701], p < 0.001), severity (hazard ratio = 0.528 [0.325, 0.858], p = 0.010) and the interaction term of intervention and severity (hazard ratio = 0.972 [0.495, 1.909], p = 0.935). Adolescents who presented with >3 signs and were assigned to the placebo-like stretching group had a PPCS incidence of 38%, which was the highest of all subgroups (aerobic exercise and ≤3 findings: 8%; stretching and ≤3 findings: 11%; aerobic exercise and >3 findings: 21%). This exploratory study provides pilot evidence that prescribed sub-symptom threshold aerobic exercise treatment early after SRC may be effective for adolescents with more oculomotor and vestibular physical examination signs and should be validated in future adequately powered trials.
Introduction
Mild traumatic brain injury, which includes sport-related concussion (SRC), is a significant public health problem, with adolescents representing the highest risk group for injury. 1,2 The signs and symptoms of concussion are diverse. Clinical phenotype profiles have been classified in a number of ways, with one system separating the profiles into autonomic/physiological, cervical, vestibulo-ocular, and cognitive/mood-related signs and symptoms. 3 The variability in presentation makes it difficult to diagnose concussion and determine severity, especially when the phenotypes overlap and can evolve over a series of days to weeks. 4 The variability in symptom presentation, once more serious injury has been ruled out, reinforces the importance of a targeted physical examination for concussion to inform individualized treatment approaches. 5
For years, the standard of care for SRC was prescribed rest until all symptoms resolved, 6 an approach that was recently found to actually delay recovery. 7 The rest-is-best approach was based on early animal research and was endorsed by initial versions of the International Consensus on Concussion in Sport Group (CISG) guidelines. 6,8 More recently, a growing number of studies has demonstrated that physical activity (including prescribed aerobic exercise) early after injury safely speeds recovery from concussion. A randomized controlled trial (RCT) by Leddy and colleagues 9 found that individualized sub-symptom threshold aerobic exercise treatment prescribed to adolescents during the first 10 days after SRC significantly reduced recovery time when compared with those prescribed a placebo-like stretching program. This study was replicated using an intent-to-treat analysis and multiple sites, including two sites with hospital affiliations that serve more symptomatic adolescents. 10 The second trial validated that early prescription of targeted heart rate (HR) aerobic exercise not only facilitated recovery from SRC, but also significantly (by 48%) reduced the likelihood of adolescents developing persisting post-concussive symptoms (PPCS).
The evidence against the efficacy of strict rest was initially demonstrated in patients seen in the emergency department (ED). 11 Concussed adolescents and young adults were randomly assigned to two groups: 1) treatment as usual: rest for two days and progressive return to activity (n = 43); and 2) strict rest and avoidance of activity for 5 days (n = 45). At 10 days post-injury, those instructed to rest and avoid activity had significantly more symptoms and ultimately had slower symptom resolution. 11 A secondary analysis 12 of the data from this study compared the outcomes of two subgroups: those who reported two or more signs of concussion at the time of injury (post-traumatic confusion/disorientation, post-traumatic amnesia, or loss of consciousness) versus those reporting less than two signs. The authors concluded that patients with two or more signs of concussion benefitted more from a prescription for strict rest than a prescription to resume moderate levels of physical activity, at least during the first 10 days post-injury. Although this study evaluated observed signs associated with time of injury as opposed to physical examination signs observed in the ED or clinic, 12 the study raised a critical question: is early subthreshold aerobic exercise beneficial for all patients, or should those with more signs of concussion avoid prescribed exercise?
The current study is an exploratory analysis of the two Leddy and colleagues 9,10 RCTs examining the effectiveness of individualized subthreshold aerobic exercise treatment across a spectrum of injury severity. The first part of our analysis was aimed at how to grade severity using five commonly assessed oculomotor and vestibular physical examination signs that are typically assessed upon initial evaluation in an out-patient setting, 13 -15 which we subsequently confirmed with self-reported symptom and comparing recovery outcomes. Combining data from both RCTs provided a larger sample to explore the effect of aerobic exercise versus a placebo-like stretching program in those different severities of presentation. We hypothesized that adolescents with more signs would take longer to recover than those with fewer signs, and that aerobic exercise would be more beneficial to participants than placebo stretching when controlling for the initial presentation severity.
Methods
This analysis presents data from two published RCTs, 9,10 and approval for the studies was obtained from Institutional Review Boards at the University at Buffalo (UB), Children's Hospital of Philadelphia (CHOP) and Boston Children's Hospital (BCH). Participants from UB were seen in community sports medicine practices (n = 131), while participants from CHOP and BCH were seen in hospital-affiliated sports medicine practices (n = 47). SRCs were diagnosed by experienced sports-medicine physicians in both trials using recent CISG guidelines, 1 including history, concussion symptoms linked to a head injury or injury to another part of the body with a force transmitted to the head, impairments on a concussion-focused physical examination, 16 and exercise intolerance on the Buffalo Concussion Treadmill Test (BCTT). 17 The oculomotor and vestibular clinical examination and BCTT are explained in further detail later in this paper.
Participants
Male and female adolescents (aged 13-18 years) presenting within 10 days of head injury and diagnosed with SRC were included in both trials. 1 Participants were excluded if they had any of the following: 1) 3-point or less difference between current and pre-injury symptoms as measured by the Post-Concussion Symptom Inventory 18 or Post-Concussion Symptom Scale 19 ; 2) moderate or severe TBI as indicated by a score <13 on Glasgow Coma Scale, lesion on computed tomography/magnetic resonance imaging, and/or focal neurologic sign consistent with intracerebral lesion; 3) injury involving loss of consciousness for 30+ min or post-traumatic amnesia for 24+ h; 4) inability to exercise because of lower-extremity orthopedic injury; 5) pre-existing comorbidities that prevent participation in active testing and/or rehabilitation, such as increased cardiac risk; 6) history of more than three previously diagnosed concussions; 7) currently on medications that affect autonomic function, such as medication for ADHD or mood stabilizers; 8) active substance abuse/dependence; and 9) limited English proficiency.
Signs from the outpatient clinical examination
Before beginning enrollment, the lead study physicians at each site (JJL at UB, CLM at CHOP, RCM at BCH) agreed upon the standard protocol for oculomotor and vestibular examinations,
5,20,21
which has been demonstrated to be reliable in this population.
22
A manual of procedures
16,23
included instructions for each examination as follows: Smooth pursuits: Participants are asked to visually track a target moving slowly in the horizontal direction with the head stationary for 5-10 repetitions (depending on subject tolerance). Movements are limited to 30-40° from neutral to avoid eliciting end-gaze nystagmus. Smooth pursuits are abnormal if there are sustained beats of nystagmus, staccato (or jerking) eye motion, loss of conjugate vision, corrective (catch-up or back-up) saccades, loss of visual fixation, or symptom provocation (dizziness, nausea, or headache). Repetitive saccades: Participants are asked to shift their eyes from point to point in rapid succession in the horizontal and vertical visual planes, rapidly switching focus between two targets held at shoulder width for up to 20 repetitions (according to subject tolerance). Repetitive saccades are abnormal if there is delayed initiation of eye movement, slow velocity, inaccurate movements such as over/undershooting with greater than one re-fixation saccade, or abnormal symptom provocation of increased headache or dizziness. Vestibulo-ocular reflex (VOR): Participants are asked to focus on a stationary target and rotate their head in the horizontal and vertical planes while maintaining visual fixation for up to 10 repetitions. Any saccadic eye movements, inability to maintain visual fixation (i.e., beating back to the center), or symptom provocation, including headache, dizziness, or lightheadedness, are considered abnormal. This test was deferred if participants had significant cervical impairment. Near point of convergence (NPC): NPC is measured using an Astron ACR/21 Accommodation Rule (Gulden Ophthalmics, Elkins Park, PA) with a standard single 20/30 vertical column of letters as the visual target.
24,25
Measurements are taken by placing the ruler at the nasion and moving the target slowly toward the nose. NPC is the point at which convergence is lost, which occurs if lateral deviation of one eye is observed, or participants report splitting of the visual target in two (not blurring of the target). NPC is considered abnormal if it is ≥10 cm from the nasion.
25,26
Complex tandem gait: Participants are instructed to walk in a straight line (heal to toe) for five steps forward with eyes open and five steps forward with eyes closed, immediately followed by five steps backward with eyes open and five steps backward with eyes closed. Both sway and number of corrective steps are recorded for each phase. The test is considered to be abnormal is there are >4 total errors.
27
Additional physical examination tests, such as fundoscopy, cranial nerves, and head, neck and face examinations were also performed as part of the concussion-focused physical exam, 28 but the incidence of focal neurological abnormalities is rare and a more severe brain injury; hence, they were not included in the stratification analysis. Neck injuries are also common in patients with concussion but are not considered to be a brain injury, so they were not included in the analysis. If present, neck injuries were treated after the initial assessment using self-guided stretching, warm compresses or, in some cases, referral to a cervical physical therapist.
Assessment of exercise tolerance
The BCTT was used to assess presence and severity of exercise intolerance and to provide HR data for the individualized aerobic exercise prescription. The BCTT was performed weekly at each study visit for the first 4 weeks. The ability to exercise fully without exacerbation of concussion-like symptoms was one criterion that defined clinical recovery. The BCTT has been shown to be safe and reliable as early as the day after injury. 29 Detailed instructions on how to perform the BCTT have been published. 30 The HR at exercise cessation due to symptom exacerbation was recorded as the heart rate threshold (HRt). Exertion testing was performed by research assistants who were either exercise science or athletic training students in settings that included physician presence. The following treadmills were used at each site: Landice L8 at UB, and Precor TRM 885 at CHOP and at BCH. All treadmills allowed for incremental adjustment of speed by 0.1 mph and incline by 1° up to a minimum of 15°.
Initial symptoms and daily symptom reporting
Participants in both trials completed a concussion symptom questionnaire at the initial assessment and daily during the interventions. The first RCT 9 used a secure, password-protected website with daily text messages to remind participants to complete the symptom questionnaire while the second RCT 10 used ReCOUPS, a LifeData-based mobile application 31 that employs ecological momentary assessment with built-in daily reminders to complete the symptom questionnaire.
Intervention
No interventions were initiated prior to 48 h post-injury in both trials. During the consent process, all participants were told that they would be randomly assigned to one type of exercise, but there was no indication of the superiority of one over the other. Apart from the prescribed intervention, study personnel instructed both groups in both trials to limit activities that may exacerbate symptoms, such as excessive use of computers or phones. Participants in both groups were asked to perform their prescribed form of exercise at home with supervision, if possible. No additional motivational strategies were used. Adherence to home exercise prescriptions was self-reported in the first RCT 9 and was verified using Polar HR monitors in the second RCT. 10 If participants did not fully recover by 4 weeks from injury, they discontinued the experimental intervention and advanced to a multi-disciplinary treatment program, which may have included interventions by a physical therapist, athletic trainer, and/or neuropsychologist. All participants were instructed to refrain from participation in sports or any other form of physical exercise (aside from their prescribed exercise) during the intervention period of 4 weeks.
Aerobic exercise prescription
Participants in the aerobic exercise groups were instructed to exercise (i.e., walking, jogging or stationary cycling) at 80% 9 or 90% 10 of the HRt they achieved on the BCTT (the target HR) for at least 20 min a day during the intervention period. All participants in both RCTs received the same HR monitor (Polar OH1 monitor and Polar Beat application) to track HR during activity. Participants were instructed to stop and rest if they experienced an increase in concussion-like symptoms by 2 or more points on the Visual Analogue Scale (VAS, range 0-10) 32 while exercising at home and to resume exercise the following day. Participants were assessed weekly with the BCTT and received a new target HR exercise prescription until the intervention period ended at 4 weeks post-injury or sooner if they had recovered.
Stretching exercise prescription
Participants were instructed to perform a standardized combination of light stationary stretches and breathing exercises that would not significantly elevate HR. Similar to the aerobic exercise group, they received a Polar OH1 HR monitor to wear while stretching, and they performed the BCTT every week and received a new progressive stretching prescription until the intervention ended at 4 weeks post-injury or sooner if they had recovered.
Main outcome measure
The main outcome was clinical recovery from SRC during the intervention period as determined by an experienced sports medicine physician who was blinded to intervention arm. Clinical recovery was defined as resolution of symptoms to pre-injury levels, the absence of abnormal signs on the standardized physical examination, and the ability to complete the BCTT without exacerbation of concussion-like symptoms or excessive fatigue. 33 The date of recovery was identified as the date that participants with a normal examination and normal exercise tolerance had returned to pre-injury symptom levels on their daily symptom reports. Duration of clinical recovery in days was calculated as the difference between date of injury and date of recovery in both RCTs. PPCS was defined as not achieving full recovery by Day 29 since injury. 1
Statistical analysis
Sample sizes were calculated for each trial separately, but no sample size estimation was performed for the current secondary analysis. The only difference in inclusion/exclusion criteria between the two trials was that exercise intolerance was an inclusion criterion in the first RCT but not the second; thus, we excluded participants in the latter trial who were exercise tolerant on Day 1 (n = 4). Additionally, we excluded participants in both RCTs with no abnormalities on the initial physical examination (n = 14). Sample demographics and pre-intervention clinical characteristics were compared between the studies and no significant differences were observed. Continuous variables were compared using a non-parametric Mann-Whitney U test and categorical/binary variables were compared using a χ 2 -test (or Fisher's exact test for cell sizes <5).
Adolescents in each trial were grouped according to their treatment intervention: 1) aerobic exercise or 2) stretching exercise. The outcome variable, days to recovery, was not normally distributed so we used a non-parametric Mann-Whitney U test. A Kaplan-Meier survival graph up to Day 29 was made and a Cox proportional hazards (PH) test was used to compare survivorship between intervention groups. Hazard ratios with 95% confidence intervals (CIs) were calculated. Type of clinical setting (i.e., community vs. hospital-based) was a priori identified as a confounding variable for survival analysis.
To control for the different combinations of abnormal physical signs at initial presentation, a second Cox PH model was made including intervention group, clinical setting, and the five binary physical examination results (smooth pursuits, NPC, repetitive saccades, VOR, complex tandem gait) for survival up to Day 29. The number of abnormal physical signs for each participant was tabulated.
Adolescents were then grouped according to the number of abnormal signs at initial visit (range 1-5), and a Kaplan-Meier survival curve up to Day 29 was made for each cumulative number of abnormal signs (> 1, > 2, > 3 and >4). A series of Cox PH model were made to identify the optimal physical sign cut-off number that could be used to stratify participants into the mild and moderate/severe categories (henceforth referred to as severe). Correlation between the number of abnormal physical examination findings with initial symptom severity was determined using a non-parametric Spearman's rank correlation to confirm the injury severity classifications.
Finally, to test our main hypothesis, a Cox PH model was used to compare survival during the intervention period with the main effects of site, intervention and severity, and the interaction term of intervention and severity. A post hoc power analysis was performed. A p value of <0.05 was considered statistically significant and all analyses were performed on SPSS Version 28 (IBM, Armok, NY). 34
Results
The first trial recruited from 2016 to 2018 and the second trial from 2018 to 2020. Seventy-five out of 103 eligible participants (73%) in the first trial and 107 out of 118 eligible participants (91%) in the second trial were included. Figure 1 presents a Consolidated Standard of Reporting Trial (CONSORT) flow diagram summarizing included and excluded participants. After merging datasets (pooled sample), 84 participants comprised the aerobic exercise group and 98 participants the stretching group. Group-wise participant demographics and initial clinical presentation are presented in Table 1. There were no significant differences in any demographic or initial visit clinical characteristics between aerobic exercise and stretching groups. Adherence to aerobic exercise was reported to be 89% in the first trial 9 and was confirmed to be 74% in the second trial. 10 No adverse events were reported during the exercise tolerance tests or during home exercise bouts at any site in both RCTs.
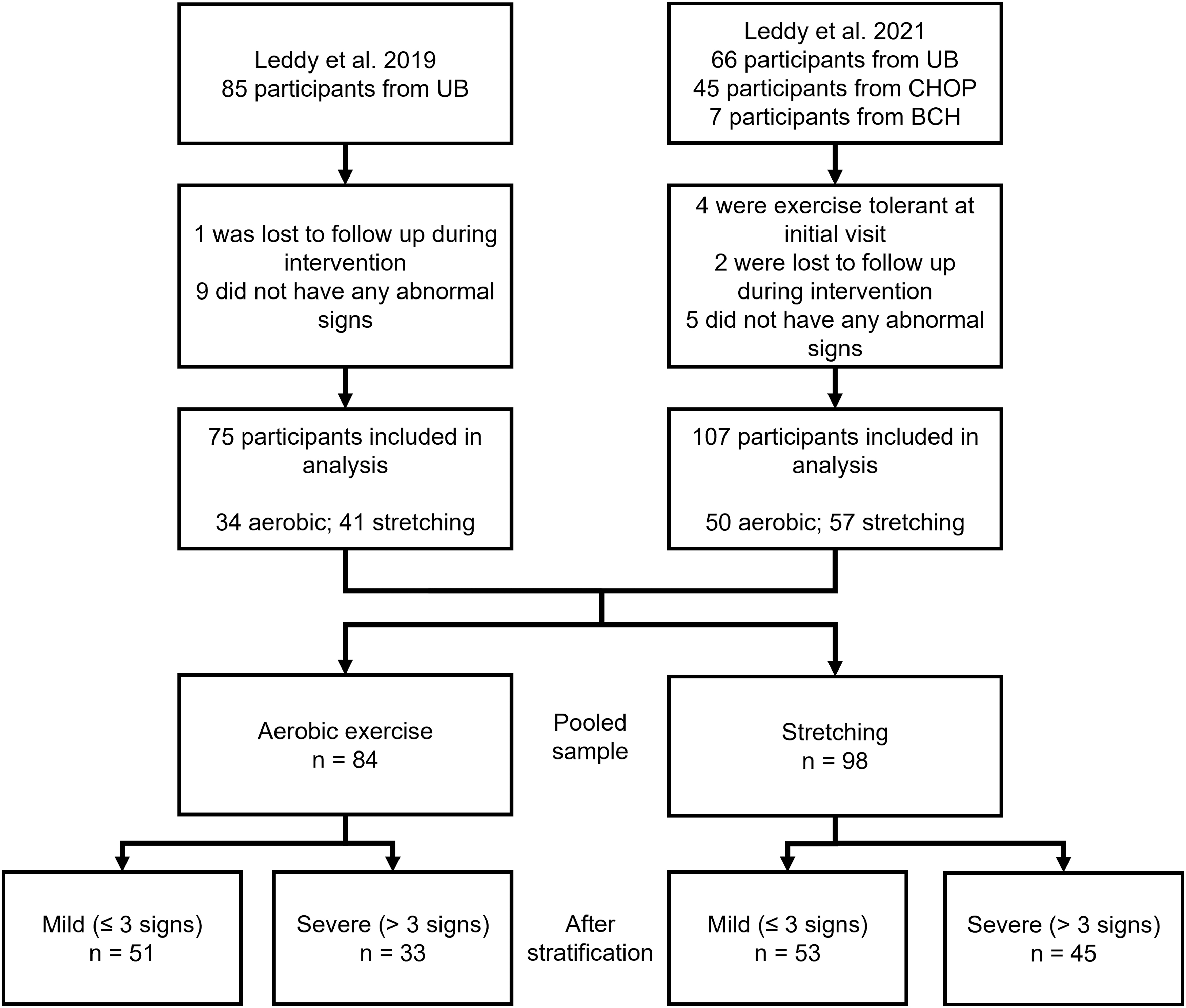
Consolidated Standard of Reporting Trials (CONSORT) flow diagram for participant inclusion.
Group-Wise Demographics of Total Sample
Bold values represent a significant comparison.
RCT, randomized controlled trial; SD, standard deviation; max, maximum; IQR, interquartile range.
A Kaplan-Meier survival curve censored at Day 29 is presented in Figure 2. In the aerobic exercise group, 13% (11/84) of participants did not recover by Day 29 compared with 25% (24/98) of participants in the stretching group. A Cox PH survival analysis comparing recovery during the intervention period between aerobic exercise and stretching was significant (Hazard ratio exercise/stretching = 0.609 [0.439, 0.845], p = 0.003), even when controlling for site (Hazard ratio community/hospital = 0.411 [0.272, 0.622], p < 0.001).
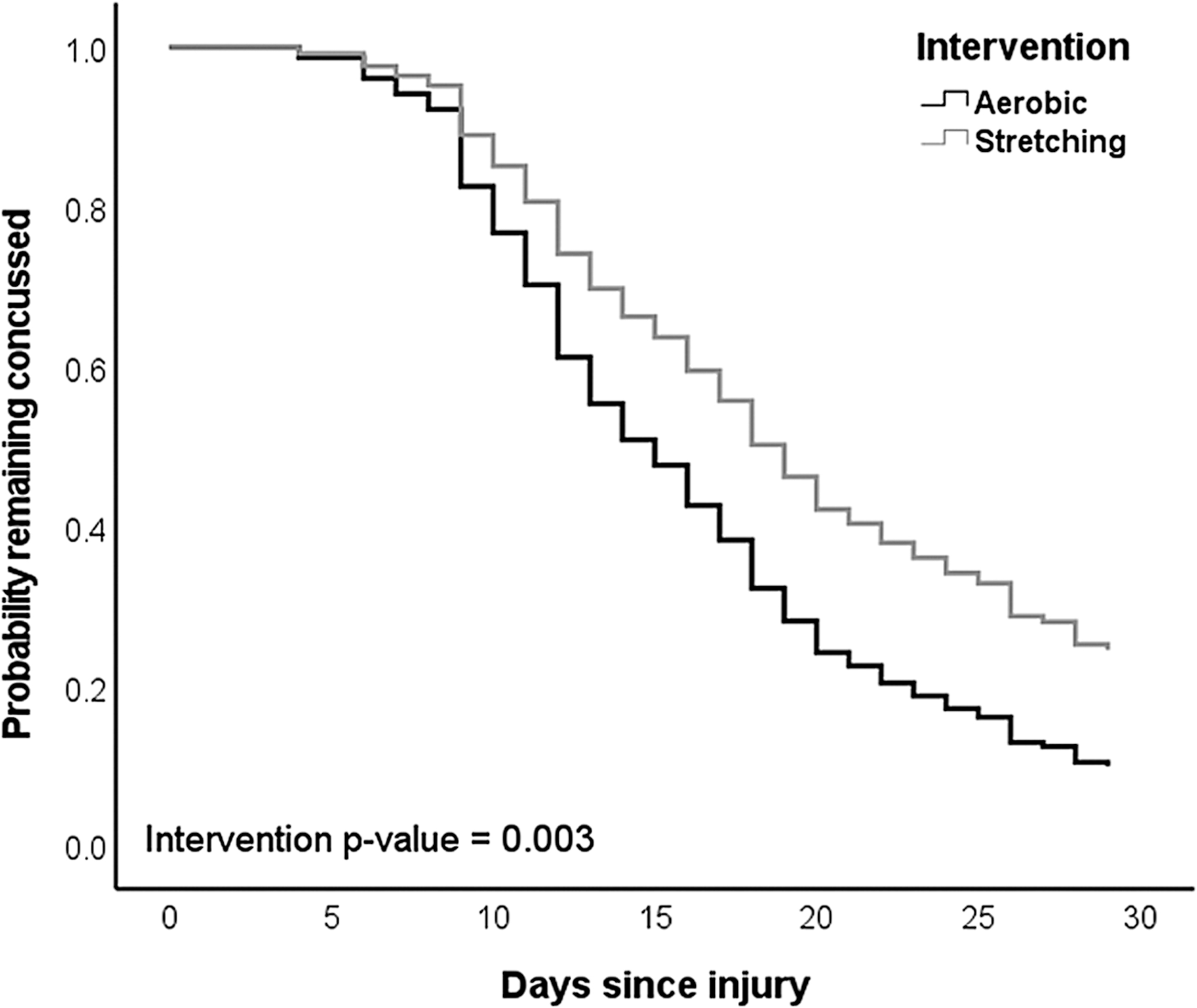
Kaplan Meier survival graph between intervention groups. Proportion of participants not recovered in aerobic and stretching groups are the following for Day 7: 81/84 and 92/98; Day 14: 38/84 and 68/98; Day 21: 24/84 and 35/98; and Day 28: 11/84 and 25/98.
In the second Cox PH model with the addition of five binary (abnormal/normal) responses for all combinations of initial visit physical examination signs, the aerobic group still recovered faster during the 4-week intervention period, corresponding to a 41.7% reduction in PPCS risk. Results of this regression are presented in Table 2.
Cox PH Model Comparing Effect of Intervention While Controlling for Each Abnormal Physical Examination Sign at Initial Visit
Bold values represent a significant comparison.
PH, proportional hazards; CI, confidence interval.
Recovery trajectories categorized according to the number of initial visit abnormal physical signs are presented in Figure 3. The results of the Cox PH model for each of the physical sign cut-off points are the following: 1) > 1: hazard ratio = 0.613 (0.411, 0.913), p = 0.016; 2) > 2: hazard ratio = 0.502 (0.357, 0.705), p < 0.001; 3) > 3: hazard ratio = 0.463 (0.329, 0.651), p < 0.001; and 4) > 4: hazard ratio = 0.635 (0.403, 1.000), p = 0.05. The most discriminant cut-off point was for those who had ≤3 versus those with >3 abnormal physical examination signs. A Spearman's correlation between number of initial visit abnormal signs and duration of recovery was significant (ρ = 0.326, p < 0.001). Additionally, the correlation between number of abnormal physical signs and symptom severity was also significant (ρ = 0.349, p < 0.001). This supports stratifying the sample by number of abnormal oculomotor and vestibular physical examination findings, with ≤3 abnormal signs classified as a mild concussion, while >3 abnormal signs can be classified as a more severe concussion.
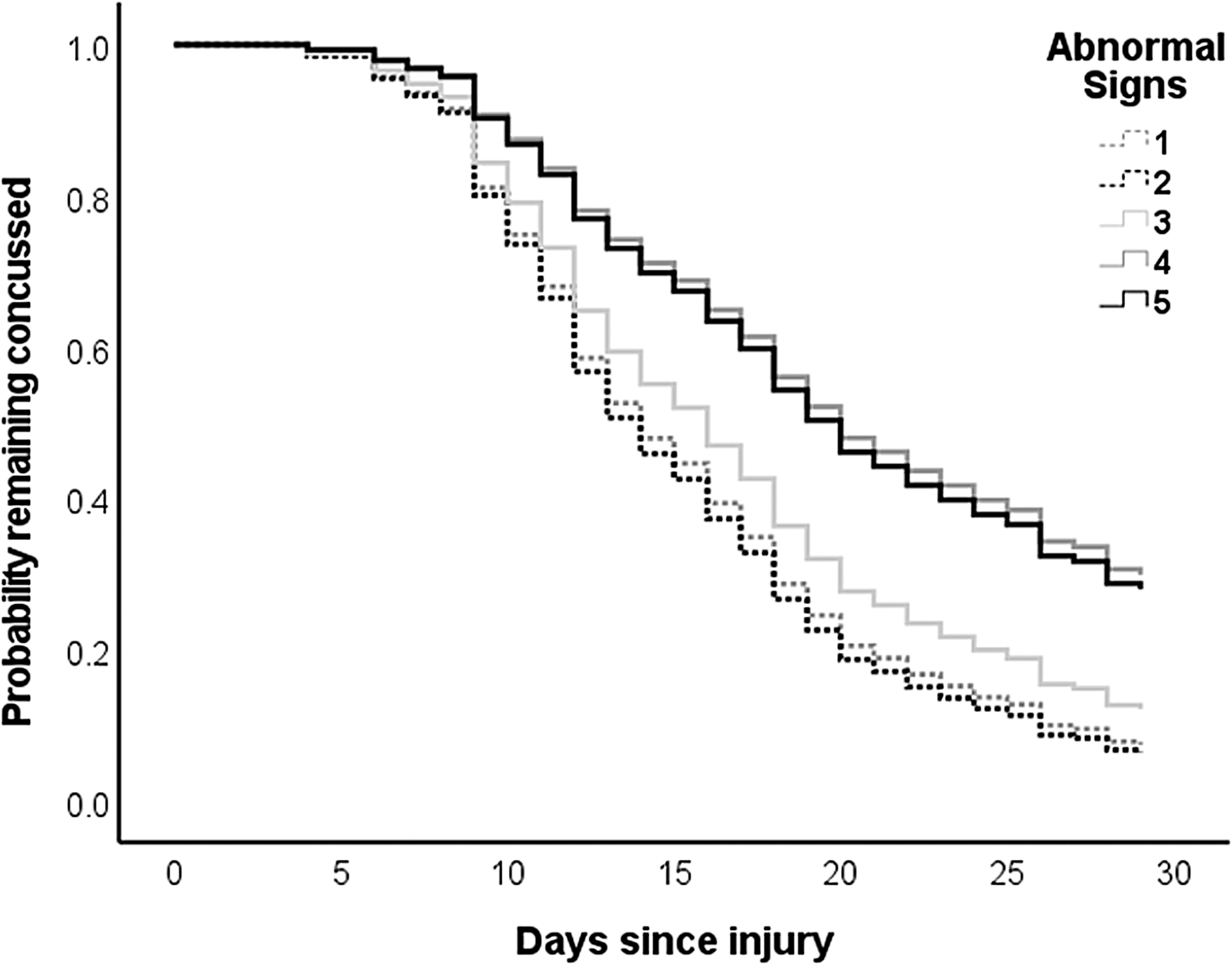
Kaplan-Meier survival graph by number of abnormal signs at initial visit and recovery.
We stratified participants based on those that had ≤3 versus >3 abnormal signs and by intervention to create four subgroups: 1) those with ≤3 abnormal signs who received subthreshold aerobic exercise; 2) those with >3 signs who received subthreshold aerobic exercise; 3) those with ≤3 abnormal signs who received stretching; and 4) those with >3 signs who received stretching. Demographics of participants in the subgroups are presented in Table 3. Participants with >3 abnormal signs had higher symptom severity than those with ≤3 abnormal signs in both intervention groups.
Participant Demographics by Intervention and Severity Subgroups
Bold values represent a significant comparison.
p value of comparison between aerobic exercise ≤3 signs versus aerobic exercise >3 signs.
p value of comparison between stretching ≤3 signs versus stretching >3 signs.
p value of comparison between aerobic exercise >3 signs versus stretching >3 signs.
SD, standard deviation; IQR, interquartile range;
A final Kaplan-Meier survival curve stratified by intervention group and severity is presented in Figure 4. The estimated median recovery times (in days) with 95% CI for the four subgroups are: 1) aerobic exercise/≤ 3 signs: 13 (11.48, 14.52); 2) aerobic exercise/>3 signs: 20 (13.44, 26.57); 3) stretching/≤ 3 signs: 16 (13.33, 18.67); and 4) stretching/> 3 signs: 22 (15.43, 28.57). The best recovery trajectory was for the aerobic exercise/≤ 3 signs sub-group while the worst was the stretching/> 3 signs sub-group. There was no significant difference in the incidence of PPCS for the aerobic exercise groups (≤ 3 signs = 8% [n = 4], > 3 signs = 21% [n = 7], p = 0.101); however, there was a significant difference in PPCS incidence for the two stretching groups (≤ 3 signs = 11% [n = 6], > 3 signs = 38% [n = 17], p = 0.001). There was a trend toward higher PPCS incidence in the stretching group with >3 signs versus aerobic exercise with >3 signs, but this did not reach statistical significance (p = 0.079).
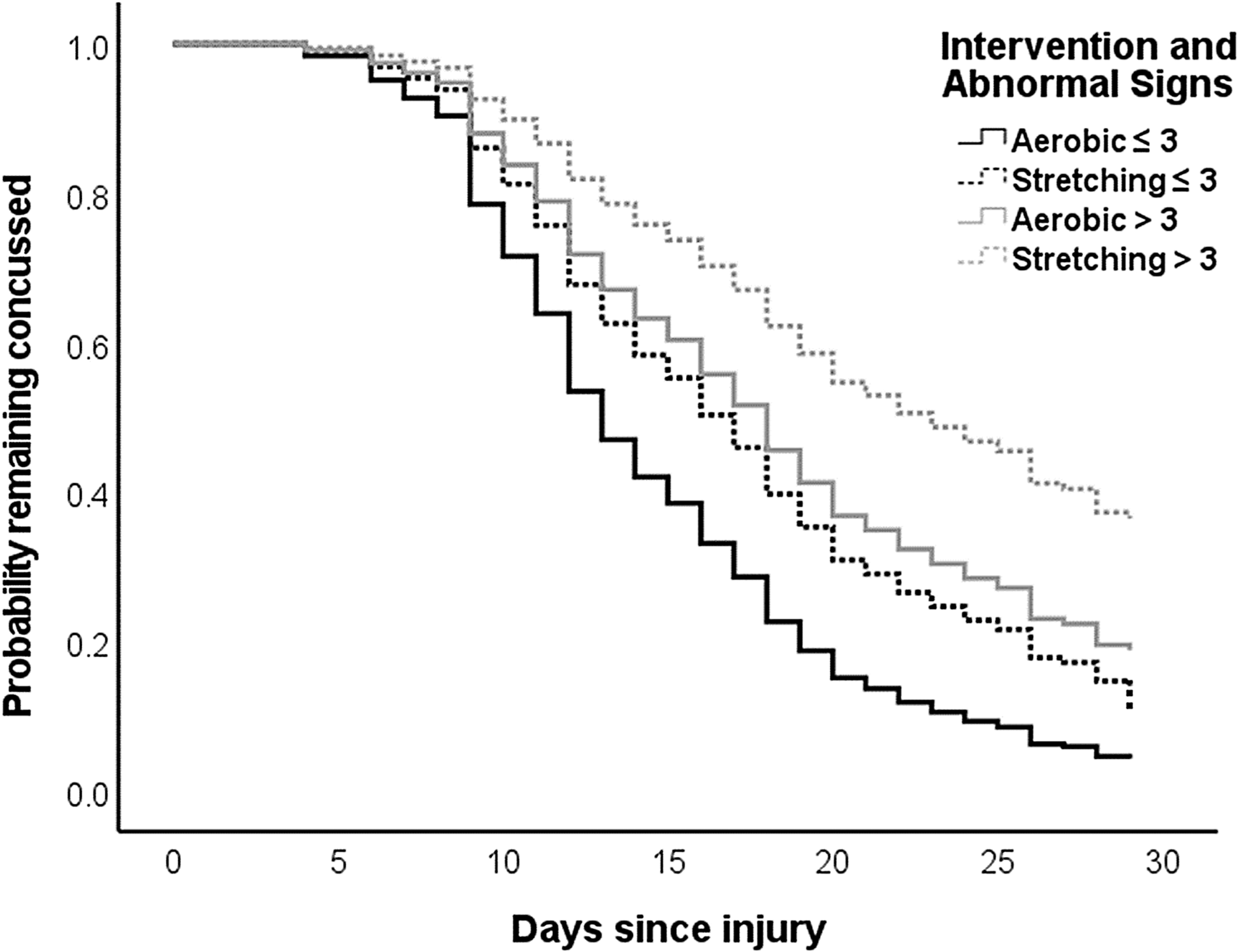
Recovery stratified by intervention group and severity. Proportion of participants not recovered in aerobic/≤ 3, stretching/≤ 3, aerobic/> 3 and stretching/> 3 groups are the following for Day 7: 48/51, 47/53, 33/33 and 45/45; Day 14: 17/51, 30/53, 21/33 and 38/45; Day 21: 8/51, 12/53, 16/33 and 23/45; and Day 28: 4/51, 7/53, 7/33 and 18/45.
Lastly, the results of the survival analysis comparing recovery during the intervention period with the main effects of site, intervention and severity, and the interaction term of intervention and severity, is presented in Table 4. Aerobic exercise was associated with shorter recovery times during the intervention period (p = 0.023), even controlling for site (p < 0.001) and severity of initial presentation (p = 0.010), and there was no indication that the effect of aerobic exercise was different for adolescents with mild or more severe presentations (p = 0.935).
Results of Survival Analysis While Controlling for Concussion Severity
Bolded represent a significant comparison.
CI, confidence interval.
Post hoc power analysis
An accurate post hoc power analysis cannot be performed for a Cox PH model with more than two variables due to correlation between covariates. If we consider only the correlation between the two covariates of interest (intervention group and severity, ρ = 0.067, p = 0.370) with a sample size of 182, a postulated hazard ratio of 0.621, and proportion of participants with the outcome of interest at 0.192, our post hoc power estimate is only 28.8%. 35 A future validation study would require at least 753 participants after attrition to achieve a power of 80%. If we remove site and the interaction term from the survival model, we still get similar results for our main survival analysis but the hazard ratio for intervention is slightly higher (0.677 [0.489, 0.936]), which decreases our power further. A future study which only includes “severely” injured participants, assuming equal sample sizes of intervention, a hazard ratio of 0.601 [0.349, 1.034] (the hazard ratio from our study if we only analyze severely injured adolescents), a median survival time for stretching being 22 days, censorship rate of 10% and follow-up time of 29 days, we would only need 49 in each group (total 98). 36 Additionally, if base a sample size estimation to compare the binary incidence of PPCS in adolescents with severe concussions, we would only need 112 participants in each group (total 224).
Discussion
This study pooled data from two published RCTs that showed early (within 10 days of injury in still symptomatic adolescents) individualized sub-symptom threshold aerobic exercise treatment safely facilitated recovery from SRC and reduced the incidence of PPCS. The rationale for pooling data was to have a sample size large enough to explore benefits of aerobic exercise in subgroups with more severe presentations. We found that adolescents who presented to a concussion clinic within 10 days of SRC and who had evidence of a more severe concussion (which we defined as >3 abnormal oculomotor and vestibular physical examination signs) took longer to recover than those with a milder presentation (≤ 3 signs). Early aerobic exercise treatment, which is just one component of a multidisciplinary concussion intervention, 37,38 facilitated recovery regardless of initial presentation severity. Our findings, however, are exploratory and should be interpreted cautiously until they have been validated in adequately powered trials.
Our exploratory results differ from those of Sufrinko and colleagues, 12 who observed that patients with signs relating to level of mental status at the time of concussive injury had no difference in symptoms at 10 days post-injury from their own baseline if they performed early physical activity. They concluded that strict rest was best for those with more of these signs. The different results between our studies likely reflect the definition of a concussion sign. Sufrinko and colleagues 12 defined concussion signs as those the patient reported at the time of injury (post-traumatic confusion/disorientation, post-traumatic amnesia, or loss of consciousness), whereas we define concussion “signs” as abnormal findings observed by a physician during the initial clinic evaluation, 39 which typically occurs days after injury. Another reason for the different results could be based on the intervention we provided. We prescribed early sub-threshold aerobic exercise as a treatment, while the Sufrinko and colleagues study examined prescribed strict rest for 2 days versus 5 days. Our results align with those of a much larger prospective cohort study 40 that evaluated the effect of early physical activity in children after concussion and found those with a higher symptom burden benefited more from early physical activity. A similar study 41 from the same group also found that early prescribed physical activity was safe in symptomatic children who were more severely concussed according to the Predicting and Preventing Post-concussive Problems in Pediatrics (5P) score. 42
The mechanism for the beneficial effect of aerobic exercise on SRC remains to be determined. Possible candidates include: 1) enhanced neuroplasticity and neuron repair through the effects of aerobic exercise to increase brain-derived neurotrophic factor levels 43 ; and 2) restoration of balance and/or control of the autonomic nervous system (ANS), which is impaired after SRC. 44 -46 The physical signs of concussion in our study were all oculomotor and vestibular. 47 These neurologic systems are inter-connected and both are under some degree of ANS control. 48,49 It is plausible that adolescents with more abnormal signs of concussion had the greatest degree of autonomic impairment and therefore responded best to sub-symptom threshold aerobic exercise initiated early after their injury. These hypotheses, however, are speculative and future studies should attempt to investigate the ANS response to exercise after concussion using in-depth physiological assessments.
There is also evidence that clinical recovery, which traditionally has been defined as resolution of symptoms and being cleared to begin the return-to-play process, does not coincide with physiological recovery. 50 Sub-clinical autonomic physiological deficits have been identified in asymptomatic athletes who had recovered clinically from a concussion over a year prior. 46 There is also a significantly increased rate of musculoskeletal injuries in athletes who return to sport after recovering from a concussion hypothesized to be attributed to these sub-clinical deficits. 51,52 Athletes in these studies, 52 however, were not treated with prescribed aerobic exercise. Given the limited post-recovery follow-up in our published RCTs, 9,10 we are unable to comment if there is altered risk of musculoskeletal injury for athletes who have been treated with early prescribed aerobic exercise.
There is emerging research on categorizing concussion into clinical phenotypes 53 to help direct treatments to specific symptom generators. Our study adds to this research by classifying concussion severity based on the number of abnormal oculomotor and vestibular physical examination signs observed at the time of initial assessment rather than relying solely on subjective symptom reports. In the authors' opinion, this approach is relatively easy to interpret for out-patient clinicians because it is restricted to five commonly assessed objective physical examination findings that are typically present in concussed patients and which are included in concussion-focused physical assessments such as the Vestibular Ocular Motor Screen 13 and the Sport Concussion Assessment Tool. 15
A strength of this study is that we were able to categorize concussed adolescents into clinically relevant groups based on the presence of signs and were then able to compare the effects of interventions by combining data from two relatively large RCTs that included multiple clinical settings. We also benefited from using a standardized oculomotor and vestibular physical examination that is valid and reliable 20 for identifying concussion-relevant signs as opposed to self- or informant-reported signs. There are validated decision rules that classify concussion severity and risk of PPCS early after injury, including the 5P Score 42 and the Risk of Delayed Recovery Score. 54 These instruments have some physical examination components but rely also on self-reported symptoms or details surrounding the injury mechanism to generate risk scores. The aim of our study was to focus solely on the response to aerobic exercise treatment in those with a spectrum of physical examination abnormalities that are pertinent to the out-patient evaluation of SRC. Future trials could stratify their samples according to these clinical decision rules and assess the effectiveness of early prescribed aerobic exercise for those defined with more severe concussions.
Limitations
The major limitation of our study is that it is exploratory. We did not have an a priori definition of severity and the first half of our analysis focused on identifying how to stratify severity. Another limitation is that the signs were rated as present or absent; therefore, we may not have captured some nuances of individual clinical variability. We assessed five physical examination signs of the oculomotor and vestibular systems, and while these are highly relevant to the clinical assessment of the concussed adolescent, other physical examination signs may also have value in classifying these patients. In addition, we did not have information on concussion-like signs that may have been present prior to injury. The Buffalo Concussion Physical Examination assess abnormalities that are not typically present in healthy adolescent athletes (i.e., <5%) 20,55 ; however, due to individual differences in neurologic maturation among adolescents, it is possible that one or more signs were present before injury.
The degree of exercise intolerance at the initial office visit has also been identified as an objective sign and a predictor of delayed recovery, 29 but the BCTT is not performed routinely in many outpatient practices. Thus, to improve generalizability, we did not include the degree of initial exercise intolerance as an indicator of injury severity. Finally, our research focused on adolescent athletes with SRC seen at out-patient sports medicine centers and therefore the results cannot be generalized to younger children, adults, or to patients with concussions sustained by other means, such as falls or automobile accidents, or to those seen in the emergency setting.
Conclusion
This study categorized adolescents with SRC into mild and more severe presentations based upon the number of abnormal oculomotor and vestibular physical examination findings identified by a physician at the initial assessment, within days of injury. The number of abnormal findings positively correlated with self-reported symptoms and there was a greater incidence of PPCS in those with >3 abnormal physical signs, which provided further support for our severity classification. We found that early, targeted HR exercise was beneficial for the recovery of adolescents after SRC, even when controlling for the severity of the initial presentation. This information is important since it is likely that some adolescents with more abnormal oculomotor and vestibular signs will eventually need specific interventions (i.e., vision and/or vestibular therapy) to help them recover. The authors recommend that early aerobic exercise be prescribed to those adolescents with more oculomotor and vestibular abnormalities because it does not adversely affect recovery, may limit deconditioning, and is a type of general intervention that athletes are likely to adhere to. 56
Footnotes
Acknowledgments
Clinical trial registration numbers: NCT02959216 and NCT02710123.
Transparency,Rigor,and Reproducibility Summary
The primary investigator (JJL), as well as the research coordinator/statistician (MNH), were the same for both trials and had access to the complete datasets. The decision to perform the present study after merging datasets was influenced by the knowledge that adolescents with more physical examination findings did poorly with a prescription for stretching exercise, which may be a source of positive results bias. Since we wanted to determine whether a prescription of aerobic exercise was beneficial for adolescents with more severe physical examination presentations, the main goal of the first half of the analysis was to identify a group of adolescents who could be considered more “severe” based on physical examination signs alone, which we subsequently confirmed with symptom severity reports and the incidence of PPCS. This stratification technique, based on the number of abnormal physical examination findings, has not been validated. Neurocognitive and mood deficits are common after concussion and may be present without identified abnormal physical examination findings. Our study was focused only on whether aerobic exercise treatment was effective (or at least not harmful) for athletes who presented with more severe physical examination presentation, but a true categorization of concussion severity should include self-reported symptoms and neurocognitive measures.
Authors' Contributions
CC, BSW, CLM, RCM, JJL and MNH made substantial contribution to the concept of the article. CC, BSW, JJL and MNH drafted the initial draft of the manuscript. EPS and MNH made substantial contributions to the acquisition and management of data collection. DJW, RCM and MNH performed the statistical analysis and CC, BSW, JIM, SAS, CLM, MFG, WPM, JJL and MNH made substantial contributions to interpreting the data and editing the final manuscript. All authors approved the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Information
This study was supported by the American Medical Society for Sports Medicine.
Author Disclosure Statement
No competing financial interests exist.