
Abstract
Emotional distress is common following moderate-severe traumatic brain injury (TBI) and is associated with poorer post-injury outcomes. Previously investigated sociodemographic, psychological, and injury-related factors account for only a small proportion of variance in post-TBI emotional distress, highlighting a need to consider other factors such as genetic factors. The apolipoprotein E gene (APOE) has been commonly studied in the TBI literature, with the ɛ4 allele linked to worse neuronal repair and recovery. Few studies have investigated the potential relationship between APOE ɛ4 and emotional distress after moderate-severe TBI, and results have been varied. We examined whether APOE ɛ4 was associated with emotional distress 1 year following moderate-severe TBI, and whether this relationship was moderated by age, sex, and TBI severity (as indexed by the duration of post-traumatic amnesia [PTA]). Moderate-severe TBI survivors provided saliva samples following inpatient admission to a TBI rehabilitation hospital. They completed a self-report measure of emotional distress, the Hospital Anxiety and Depression Scale (HADS), at a follow-up interview ∼1 year post-injury. Complete genetic and follow-up data were available for 441 moderate-severe TBI survivors (mean age = 39.42 years; 75% male). We constructed a linear regression model that included APOE ɛ4 carriage status (carrier vs. non-carrier) and interactions with age, sex, and TBI severity (APOE × age, APOE × sex, APOE × age × sex, and APOE × PTA duration) to predict total score on the HADS, while covarying for the main effects of age, sex, PTA duration, and previous head injury. There was a significant main effect of APOE ɛ4, whereby ɛ4 carriers reported less emotional distress than non-carriers (p = 0.04). However, we also found a significant interaction with age such that APOE ɛ4 carriers reported increasingly greater emotional distress with older age compared with non-carriers (p = 0.01). A sensitivity analysis (n = 306) suggested that the APOE × age interaction, and main effects of age and previous head injury, were not unique to individuals with pre-injury mental health problems (n = 136). However, the main effect of APOE ɛ4 was no longer significant when individuals with pre-injury mental health problems were removed. Our findings highlight the importance of considering moderation of genetic associations, suggesting that APOE ɛ4 may be a risk factor for emotional distress specifically among older survivors of moderate-severe TBI. If these findings can be independently replicated, APOE ɛ4 carriage status, interpreted in the context of age, could be incorporated into risk prediction models of emotional distress after moderate-severe TBI, enhancing targeted early detection and intervention efforts.
Introduction
Survivors of moderate-severe traumatic brain injury (TBI) often report ongoing physical, cognitive, social, and emotional difficulties. 1,2 Emotional distress is a significant issue following TBI, with pooled prevalence estimates of post-TBI anxiety and depressive disorders reported at 36% and 43%, respectively. 3 The experience of emotional distress tends to peak in the 1st year post-injury; however, some survivors continue to experience elevated emotional distress for decades. 4 –6 Emotional difficulties after moderate-severe TBI may arise directly from injury to brain structures supporting emotional regulation, as well as in response to newfound functional limitations (e.g., changes to participation in work and leisure activities). 2,4,7,8
Previous studies have identified a range of factors associated with emotional distress following TBI. These include pre-injury mental health problems, a history of previous TBI, comorbid limb injury, earlier time post-injury, and use of avoidant and emotion-focused coping strategies. 3,6,9 –14 Some studies suggest that females experience higher levels of post-TBI depression and anxiety, but findings are mixed. 3,15 –17 Recent research also suggests a quadratic relationship for age, whereby psychiatric disturbance post-TBI peaks in middle age (at ∼30–60 years) and then declines thereafter. 6,18 –20 Findings regarding an association between TBI severity and emotional distress are also mixed, with some studies reporting a negative relationship (i.e., more distress with less severe TBI), others reporting a positive relationship, and others not detecting any association. 5,6,12,21 –23 These sociodemographic, psychological, and injury-related factors, even when examined in combination, do not account for the substantial heterogeneity in post-TBI emotional distress. 24 It is therefore important to examine other potential risk factors.
Genetic vulnerability is likely another contributory factor to emotional distress after TBI. In the general population, family and twin studies provide evidence that genetic factors make an important contribution to mental health, with high heritability estimates for psychiatric problems such as depression and anxiety. 25 Following TBI, there are alterations in the expression of various genes and gene-related biological systems in the brain. 26
The apolipoprotein E gene (APOE) is the most frequently studied gene in the TBI literature, reflecting its central role in neuronal maintenance and repair. 27 –30 APOE has three alleles: ɛ2, ɛ3, and ɛ4. 29,31 Whereas the APOE ɛ2 and ɛ3 alleles have been shown to promote neurite outgrowth and facilitate lipid transport, the ɛ4 variant is neurotoxic to these processes. 29,31 Therefore, individuals with TBI carrying the ɛ4 allele could be at risk of poor outcomes. Indeed, APOE ɛ4 has been significantly associated with longer loss of consciousness and prolonged hospitalization after TBI, 32 increased risk for post-traumatic seizures, 33 and poorer post-injury cognitive and functional outcomes. 34 –36
Few studies have investigated the association of APOE with emotional outcomes after TBI, and results have been varied. The APOE ɛ4 allele may contribute indirectly to elevated emotional distress in the TBI population via its associations with worse cognitive and functional outcomes (i.e., individuals carrying ɛ4 may have worse functioning and feel distressed about this). Alternatively, this genetic variant may also directly contribute to emotional outcomes by modulating neuronal repair and recovery in frontal-subcortical regions, which are often impacted post-TBI and are involved in emotional regulation. 37
Some previous studies have found the APOE ɛ4 allele to be significantly associated with greater self-reported emotional distress after TBI. In studies of mild TBI, APOE ɛ4 was significantly associated with increased emotional symptom reporting 2 months after injury in adults, 38 and with greater levels of depression and anxiety in military veterans on average 6 years after injury. 39 The APOE ɛ4 allele was also associated with greater self-reported emotional distress in young and middle-aged adults 6 months following moderate-severe TBI, 40 in older adults who sustained a moderate-severe TBI on average 9 years earlier, 41 and in young adult military veterans who had survived mild-severe TBIs. 37 In contrast, other groups have reported no significant association between APOE ɛ4 and symptoms of emotional distress 6 months 42 and 5 years following mild-moderate TBI, 43,44 or three decades after predominately moderate-severe TBI. 5,45
There are several study factors that may have contributed to these mixed findings. First, previous samples have comprised a preponderance of mild TBI survivors, whereas moderate-severe TBI is associated with more extensive neuropathology 46,47 and persistent emotional distress. 26,46 –48 Therefore, APOE ɛ4 may be a greater contributor to emotional distress following moderate-severe TBI, because of its role in neuronal repair in regions of the brain (e.g., frontal-subcortical areas), which are often impacted post-TBI and are involved in the regulation of mood and emotion. 46 Second, the sample sizes in previous studies of APOE and post-TBI distress (n = 42–134) may have been too small to detect what is likely a relatively modest effect of a single candidate gene on a polygenic trait such as emotional distress. 34 Third, previous studies have used measures of emotional distress that overlap with direct physiological consequences of TBI such as fatigue and difficulty concentrating, possibly confounding findings. 26
Further, inconsistent findings may reflect the presence of moderating variables in the relationship between APOE ɛ4 and post-TBI emotional distress. There is some evidence to suggest that the association between APOE and TBI outcomes may vary as a function of other factors such as age, sex, and injury severity. 49 Several studies have associated APOE ɛ4 with better functional and cognitive outcomes after TBI, specifically in childhood or young adulthood, whereas it appears to be a risk factor for poorer TBI outcomes among older survivors. 50 –54 According to the antagonistic pleiotropy hypothesis, the APOE ɛ4 variant may be neurotoxic in older age (because of increasing neurodegenerative burden) but may provide some advantages to younger individuals, thereby maintaining its presence in the gene pool. 55,56 Sex may also moderate the association between APOE and TBI outcomes, because the female sex hormone estrogen modulates the transcription of the APOE gene. 57 There may also be a three-way interaction among APOE, age, and sex on TBI outcomes, with one study showing that the APOE ɛ4 allele was most strongly associated with worse global functional outcome among female participants ≥55 years of age. 58 Finally, APOE ɛ4 carriers with severe TBI may experience disproportionately impaired neural recovery processes in areas underlying emotional regulation, implicating injury severity as another possible moderating factor. To our knowledge, no study has considered potential moderating influences on the relationship between APOE ɛ4 and emotional distress after TBI.
In the current study, we investigated whether the APOE ɛ4 allele was associated with emotional distress 1 year after moderate-severe TBI. Additionally, we explored whether any association between APOE ɛ4 and emotional distress was moderated by age, sex, and TBI severity. We formed two hypotheses: Individuals with moderate-severe TBI carrying one or more copies of the APOE ɛ4 allele would report greater levels of emotional distress 1-year post-injury, as measured by the Hospital Anxiety and Depression Scale (HADS). The association between APOE ɛ4 and emotional distress would be moderated by age, sex, and injury severity. We hypothesized that the ɛ4 allele would be most strongly associated with higher levels of emotional distress among older participants, female participants, and participants with a longer duration of post-traumatic amnesia (PTA).
Methods
Participants
Participants were sampled from the Longitudinal Head Injury Outcome Study (LHS) conducted at the Monash-Epworth Rehabilitation Research Centre (MERRC). Ethics approval was previously received from the Monash University Human Research Ethics Committee for the LHS at MERRC. Written informed consent was provided by all participants or their next of kin during their inpatient stay, including consent for their de-identified personal and genetic data to be used by MERRC in future research projects.
Data were collected from consecutive inpatient TBI admissions to Epworth HealthCare (Melbourne, Australia) between 1999 and 2020. Persons over the age of 16 (n = 441; mean = 39.42 years; 75% male) who had sustained a moderate-severe TBI and completed the 1-year LHS follow-up were included in the current project. Participants with any pre- or post-injury neurological condition other than moderate-severe TBI (e.g., mild TBI, stroke; n = 5) or who had missing responses on the HADS at the 1-year follow-up (n = 5) were excluded from the current project. Completion of Little's Test of Missing Completely at Random (MCAR) demonstrated that the missing data was MCAR (p = 0.10, see Supplementary Text regarding missing data, and Table S1).
Measures
Demographic and injury variables
Participant demographic and injury information were obtained from medical records. Injury variables included the injury mechanism, date of injury, and indices of injury severity including the Westmead PTA scale
58
and worst 24-h Glasgow Coma Scale (GCS) score.
59,60
The Westmead PTA scale includes 12 items that assess orientation to person, place, and time, as well as the ability to consolidate new memories. Patients are required to answer all items correctly consecutively across 3 days (unless a perfect score is obtained on day 1) to be deemed to have emerged from PTA. All participants in this study had obtained a moderate or severe TBI based on the Mayo classification system (i.e., PTA duration
Emotional distress
The HADS was used to assess symptoms of anxiety and depression during the previous week. 65 The HADS is a self-report measure containing 14 items that are rated on a four-point Likert scale. The HADS excludes many symptoms of anxiety and depression that may overlap with the direct physiological consequences of TBI, such as cognitive problems and sleep disturbance. We used the total score on the HADS as a measure of general distress, as the subscales are strongly positively correlated in moderate-severe TBI samples, and a one-factor model of the HADS yielded good fit in a similar sample to the current project. 12,66 Some items are reverse-scored. We summed all items to generate the total score (range = 0–42), with higher overall scores indicating greater emotional distress.
Procedure
Saliva samples were collected for genetic analysis during participants' inpatient stay at Epworth HealthCare. Approximately 1 year after their TBI, participants completed the HADS and other questionnaires with a psychologist-researcher over the phone or in person, or on hard copy via mail.
Genetic analysis
Genomic data (gDNA) were extracted from participant saliva samples using the ReliaPrep gDNA Tissue Miniprep system (Promega). Each gDNA sample was genotyped for the APOE ɛ2/ɛ3/ɛ4 polymorphisms using one-step amplified refractory mutation system polymerase chain reaction (ARMS-PCR) 67 to amplify each allele at each locus. ARMS-PCR products were then run on 2% agarose gels and visualized using SYBR Safe (Thermo Fisher Scientific) staining.
Statistical analysis
Data analysis was conducted using R Studio version 3.6. The total sample comprised 447 participants. Assumption checks for statistical analysis were completed, and no data transformations were necessary. Because of the low number of ɛ4 homozygotes (nine participants with ɛ4/ɛ4), we coded participants as carriers (i.e., having at least one copy of the APOE ɛ4 allele) or non-carriers (i.e., having no APOE ɛ4 allele).
We constructed a linear regression model to assess the association between APOE ɛ4 and emotional distress (HADS total score) following TBI. The predictor variables included in the model were: APOE ɛ4 carriage status (carrier vs. non-carrier), age, sex, PTA duration (days), history of another previous head injury prior to the index TBI (yes/no), and four interaction terms: genotype × age, genotype × sex, genotype × age × sex, and genotype × PTA duration (days). We considered whether it would be appropriate to include age squared in the regression model, as previous research has suggested that emotional distress after TBI is highest in middle adulthood (i.e., that there is a quadratic relationship). 6 However, correlation analysis revealed no significant association between age squared and emotional distress (p = 0.46); therefore, only the linear effect of age was included as a covariate.
Previous literature suggests that pre-injury mental health problems are a strong predictor of post-injury depression and anxiety. 24,68 Considering this, we sought to assess whether the association between APOE ɛ4 and emotional distress in our regression model was unique to participants with pre-injury mental health problems. We completed a sensitivity analysis by rerunning our regression after removing individuals with pre-injury mental health problems (n = 136). Information about pre-injury mental health was obtained from two sources: (1) documented pre-injury mental health treatment in participant medical records; and (2) a psychiatric study in which a subset of our participants (n = 114) completed the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) Axis I Disorders (SCID). 69 The SCID was completed early post-injury (on average 2 months) and used to assess the pre-injury presence of DSM-IV Axis I psychiatric disorders. Individuals were coded as having a pre-injury mental health problem (n = 136) or not (n = 306) according to their medical records or SCID interview if completed. Because of pre-injury mental health data being collected differently for participants who participated in the psychiatric study, there was some disagreement between the two sources. Of the participants with both medical record and SCID assessment data (n = 114), there were 34 participants (29%) who reported a pre-injury mental health problem during their SCID assessment but had no pre-injury treatment for mental health problems in their medical records. The most commonly reported pre-injury mental health problems in this group were substance abuse and addiction (n = 21), depression disorders (n = 10), anxiety disorders (n = 12), and post-traumatic stress disorder (n = 3). There were 12 participants in this group who reported multiple pre-injury mental health problems on the SCID. These individuals were all coded as having a pre-injury mental health problem and were included in the sensitivity analysis. Additionally, there was one participant with no pre-injury mental health problems reported in their SCID assessment, but treatment was recorded in their medical record. This participant was also coded as having a pre-injury mental health problem. Two participants had missing data on their SCID assessment, but had treatment documented in their medical record; therefore, they were coded as having a pre-injury mental health problem. One participant had missing data on both the SCID and their medical records and was not included in the sensitivity analysis.
We also considered the possibility that advancements in post-TBI treatment and non-treatment-related factors may influence participants' levels of emotional distress. We completed an additional regression including year of injury as a covariate in our regression model to check whether this changed the results.
Results
Sample characteristics
The total sample comprised 447 participants, who completed the HADS and provided genetic data. There were 440 participants who had complete data across all covariates, and therefore were included in the regression analysis (n = 7 excluded because of missing data on one or more variable other than genotype and HADS). All participants sustained a moderate-severe TBI, the majority from a vehicular accident (n = 390, 87.1%). Our sample was predominantly from Oceanian (n = 390, 87.1%) and European (n = 12, 2.6%) regions. For descriptive statistics of the sample (age, sex, country of origin, injury cause, pre-injury treatment mental health [yes/no], and previous TBI [yes/no]), refer to Tables 1 and 2.
Sample Frequencies of Categorical, Injury, and Demographic Variables
TBI, traumatic brain injury.
Mean (M), Standard Deviations (SD), and Correlations between Continuous Variables
p < 0.05; HADS, Hospital Anxiety and Depression Scale; PTA, post-traumatic amnesia.
APOE genotypes
A total of 124 participants carried at least one copy of the APOE ɛ4 allele (27.9% ; see Table 3). The APOE genotype frequencies in this sample were consistent with the Hardy–Weinberg equilibrium; they did not significantly differ from broader frequencies observed in Caucasian populations (χ 2 = 0.62, p = 0.40). Genotype frequencies were also consistent with previous studies in Caucasian TBI samples. 35,36,70,71 APOE ɛ4 carriers did not differ significantly from non-carriers across any covariates (see Tables S2 and Table S3).
Participant Genotypes Across the APOE ɛ4 Polymorphism
APOE and emotional distress
Full regression output is provided in Table 4. There was a significant main effect of APOE ɛ4 on emotional distress (p = 0.04), with ɛ4 carriers (mean = 12.21, standard deviation [SD] = 8.76) reporting significantly lower distress than non-carriers (mean = 12.80, SD = 9.03; see Fig. 1). The effect size was small, with ɛ4 carriage status uniquely accounting for only 1% of the variance in reported emotional distress.

Box plot comparison of Hospital Anxiety and Depression Scale (HADS) scores between APOE ɛ4 carriers (n = 124) and non-carriers (n = 323). In multiple regression, there was a significant main effect of APOE ɛ4, with carriers reporting significantly lower emotional distress 1 year following moderate-severe traumatic brain injury (TBI) than carriers (p = 0.04).
Multiple Linear Regression Results, Predicting Emotional Distress (n = 440)
β represents the regression standardized beta coefficient.
PTA, post-traumatic amnesia; TBI, traumatic brain injury.
However, we also found a significant, nuanced interaction between APOE ɛ4 and age on emotional distress (p = 0.01), which uniquely accounted for an another 2% of the variance in outcome (Fig. 2). APOE ɛ4 carriers reported greater levels of emotional distress with increasing age (r = 0.25, p = 0.006). For APOE ɛ4 non-carriers, HADS scores did not change across the adult lifespan (r = -0.01, p = 0.81).
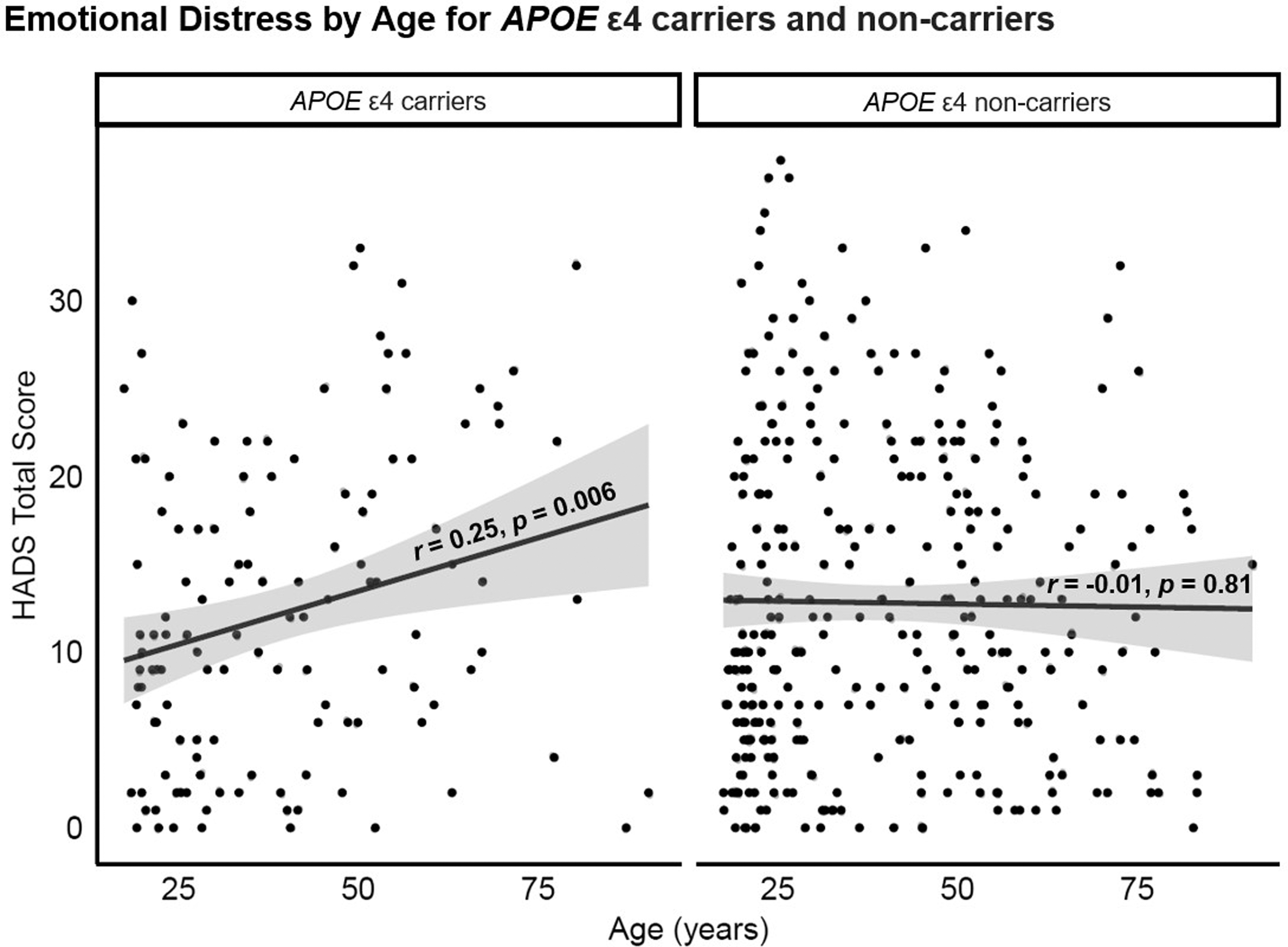
The correlation between age and Hospital Anxiety and Depression Scale (HADS) total score for APOE ɛ4 carriers and non-carriers. Multiple regression suggested that APOE ɛ4 carriers reported greater levels of emotional distress with increasing age, whereas HADS scores did not change across the adult lifespan in APOE ɛ4 non-carriers.
There were no significant interactions between APOE ɛ4 and sex (p = 0.10), APOE ɛ4, age, and sex (p = 0.20), or APOE ɛ4 and PTA duration (p = 0.10).
Regarding other variables, there were also significant main effects of age (2% of variance uniquely explained; p = 0.003) and previous head injury (2% of variance uniquely explained; p = 0.003), with older age and multiple TBIs each predicting higher levels of emotional distress. There were no significant main effects of sex (p = 0.20) or PTA duration (p = 0.10).
Influence of pre-injury mental health and year of injury
Complete data from 306 participants who had not reported previous mental health problems were included in the sensitivity analyses (n = 5 excluded because of missing data). Participants who reported previous mental health problems did not differ significantly from participants who did not report previous mental problems across all covariates (see Tables S4 and S5).
The pattern of significant and non-significant associations remained the same, with the exception of the main effect for APOE ɛ4, which was no longer significantly associated with emotional distress (p = 0.13; see Table S6).
In our final regression model, which included the year of injury as a covariate, the pattern of significant and non-significant associations remained the same as our primary regression, with the exception of the main effect for APOE ɛ4, which was no longer significantly associated with emotional distress (p = 0.07; see Table S7)
Discussion
We investigated whether the APOE ɛ4 allele was associated with emotional distress 1 year following moderate-severe TBI. We also considered whether the association between APOE ɛ4 and emotional distress was moderated by age, sex, and injury severity. Contrary to our hypothesis, we observed an advantageous main effect of APOE ɛ4, whereby ɛ4 carriers reported significantly lower emotional distress than non-carriers. However, our exploration of potential moderating influences suggested a more nuanced gene–outcome association. Our second hypothesis was partially supported. Among APOE ɛ4 carriers, we observed a positive relationship between age and distress, reporting higher levels of emotional distress with increasing age. In contrast, APOE ɛ4 non-carriers demonstrated no change in levels of self-reported emotional distress across the adult lifespan. Other interactions (APOE ɛ4 and sex, APOE ɛ4, age, and sex, and APOE ɛ4 and PTA duration) were non-significant. Our analysis also found significant main effects of age and having sustained multiple TBIs, with older participants and those with a previous head injury reporting higher levels of distress, whereas sex and PTA duration were not significant predictors. Additional analyses found that the interaction between APOE ɛ4 and age and the main effects of age and previous head injury were still significant only among individuals with no documented pre-injury mental health problems and when covarying for time of injury (to account for advancements in post-TBI treatment). However, the main effect of APOE ɛ4 was no longer significant in either of these additional analyses.
Interaction between APOE and age on emotional distress after moderate-severe TBI
A unique contribution of this study is its consideration of potential moderating influences on gene–outcome associations after TBI. The main effect of APOE ɛ4 proved non-robust, as it was no longer significant after accounting for potential influences of pre-injury mental health problems and advancements in post-TBI treatment. In contrast, the APOE ɛ4 and age interaction remained significant. This may indicate that the role of APOE ɛ4 in emotional distress following TBI is dependent on an individual's age.
According to the evolutionary concept of antagonistic pleiotropy, APOE ɛ4 may remain a variant in the gene pool despite its deleterious effects in old age if it confers advantages earlier in life. 55,56 APOE ɛ4 may provide advantages in adolescence and early adulthood through overactivation of task-related brain regions. 72,73 Indeed, APOE ɛ4 has been associated with improved attention and episodic memory in healthy young adults. 72,74 In middle-aged adults carrying APOE ɛ4, this overactivation could delay or mask cognitive decline that is associated with some neurodegenerative disorders (e.g., Alzheimer's disease) by offsetting neurodegenerative burden on the brain. 73 Lending support to this notion, middle-aged adults carrying APOE ɛ4 have performed similarly, or better, than non-carriers on measures of cognitive functioning. 75 –77 However, these compensatory resources may be depleted with old age, which could leave APOE ɛ4 carriers at an increased risk of accelerated aging and dementia. 78 The APOE ɛ4 is related to poor memory and cognitive decline in older adults, 73,79,80 and is the strongest known genetic risk factor for late-onset Alzheimer's disease. 81 –83 Some studies in the TBI literature have also supported the antagonistic pleiotropy hypothesis, with APOE ɛ4 previously being associated with better cognitive and functional outcomes after TBI if sustained during childhood or young adulthood. 50 –54 Our observations also support this phenomenon, and provide the first evidence that APOE ɛ4 could differentially influence emotional distress across the lifespan for TBI survivors. This phenomenon could also explain the conflicting results observed in previous studies, which used samples varied in age, and did not account for the potential moderating influence of age on the association between APOE ɛ4 and post-TBI emotional distress.
Study strengths and limitations
There are a number of limitations of the current study that should be considered. First, although our sample was larger than those in previous studies, reliably detecting the effect of a single candidate gene on a complex polygenic trait such as emotional distress is difficult. Replication of this finding in independent samples is required to strengthen conclusions. Second, as TBI outcomes are likely influenced by hundreds of genes, future research should consider integrating a broader range of genetic factors; for example, by creating polygenic risk scores. 49,84 Third, although the HADS is a validated measure of emotional distress in TBI samples, the sum-score approach lumps together different symptoms of anxiety and depression that may have different genetic risk factors. 85,86 Future research could consider mapping genetic factors onto more homogenous dimensions of symptom expression 87 or investigating individual symptoms of psychiatric disorders. Fourth, participants in this study had all received rehabilitation following their injury in the context of a no fault accident compensation system, which may have played a role in their levels of emotional distress at the time of assessment. Fifth, our sample was predominately from Oceanian or European regions, and gene–outcome associations may vary as a function of race, potentially limiting the generalizability of our findings. 49,88 –90 Similarly to this, racial or ethnic data were not collected for participants in this study, and therefore, our estimate of the number of participants who were considered “Caucasian” was inferred by their reported geographical region of birth. There is a possibility that our estimate was therefore inaccurate. Lastly, using two sources of data to ascertain participant pre-injury mental health issues (i.e., medical records and SCID data) was a limitation of this study. It is possible that medical records alone may not have captured pre-injury mental health data fully for participants who did not complete the SCID. Future studies would therefore benefit from utilizing a single, comprehensive measure of pre-injury mental health.
Notwithstanding these limitations, our study does have a number of key strengths. This study is the largest to date investigating the potential role of APOE ɛ4 in emotional distress after TBI, and the first to examine potential moderating influences on this association. Examination of moderators allows us to refine our understanding of the contribution of APOE to TBI recovery and to fine-tune our models of genetic risk. Finally, inclusion of pre-injury mental health data enabled us to demonstrate that the interaction between APOE ɛ4 and age on post-TBI emotional distress was not unique to participants who reported pre-injury mental health problems in this study.
Conclusion
This study found that in moderate-severe TBI survivors there was a significant interaction between APOE ɛ4 and age on emotional distress, whereby APOE ɛ4 carriers reported greater emotional distress with increasing age. The remaining interaction terms (APOE × sex, APOE × age × sex, and APOE × PTA duration) were not significantly associated with emotional distress. These results suggest that older ɛ4 carriers may be at greater risk of poor emotional outcomes following moderate-severe TBI. APOE ɛ4 carriage status, interpreted in the context of age, could be used to enhance prediction of poor emotional outcomes following moderate-severe TBI.
Transparency, Rigor, and Reproducibility Summary
This project was completed by the authors at MERRC. The data included in this study were part of the 1-year follow-up of the Longitudinal Head Injury Outcomes Study being conducted at MERRC. Participants were recruited into this longitudinal study from consecutive inpatient TBI admissions to Epworth HealthCare, a rehabilitation hospital in Melbourne, Australia. The authors of this project received ethics approval from the Monash University Human Ethics Research Committee and Epworth HealthCare. Genetic subtyping of the APOE ɛ4 single nucleotide polymorphism for each participant was completed by Richard Burke of Monash University (School of Biological Sciences).
All participant data, including genetic and injury-related data, were kept de-identified to maintain confidentiality and privacy. Data organization and statistical analyses were conducted using R Studio version 3.6. Data analysis was completed for 448 participants and included reviewing medical files in an online database for participant information including emotional distress scores, demographic data, and injury-related variables.
Emotional distress was measured as the total score on the HADS, a previously validated measure of distress after TBI. Because of the low number of ɛ4 homozygotes in the sample, APOE genotype was dichotomized as ɛ4 carriers (having at least one copy of the ɛ4 allele) versus non-carriers (having no copy of the ɛ4 allele). Multiple linear regression analyses were conducted to investigate the association between APOE ɛ4 and emotional distress. Other variables included in the analyses were time since injury (days), age, sex, PTA duration (days), previous head injury (yes/no), and four interactions terms (APOE ɛ4 × age, APOE ɛ4 × sex, APOE ɛ4 × age × sex , and APOE ɛ4 × PTA duration). Our selection of variables to include in the model and hypotheses was guided by the previous literature. A sensitivity analysis was completed, whereby the multiple linear regression was rerun using only participant data from individuals who were not indicated to have had pre-injury mental health problems. The threshold for statistical significance was set at p ˂ 0.05.
Inspection of density and Q-Q plots suggested that the distribution of HADS total scores was positively skewed. Both multiple linear regression and negative binomial regression were performed to examine the effect of this positive skew. The pattern of findings did not differ between the two types of regression, suggesting that the positive skew of the HADS data did not impact the results. Therefore, we report the output from the multiple linear regression in this article. There were no instances of multicollinearity between continuous predictors (i.e., all Spearman's r < 0.50 and variance inflation factors <10) or categorical predictors (i.e., non-significant χ 2 tests of independence; see Table 2 and Table S8).
The residual versus predicted scatterplots indicated that most scores centered around zero, with quantile regression lines appropriately parallel to the Locally Weighted Scatterplot Smoothing (LOWESS) smooth line, satisfying the assumption of homogeneity of variance. Each model also met the assumption of independence of errors (i.e., all Durbin–Watson values were ∼2.0; see Supplementary Text).
Footnotes
Acknowledgments
We thank the team at Epworth HealthCare Melbourne and the Monash-Epworth Rehabilitation Research Centre for their continued support throughout this project. We would also like to thank all participants involved in the Longitudinal Head Injury Outcomes Study for so kindly giving their time.
Authors' Contributions
C.A. was responsible for conceptualization (equal), data curation (equal), methodology (equal), formal analysis (lead), writing – original draft (lead), visualization (lead), validation (equal), review, and editing (equal). J.C. was responsible for supervision (equal), conceptualization (equal), data curation (equal), methodology (equal), validation (equal), review, and editing (equal). A.H was responsible for supervision (equal), conceptualization (equal), data curation (equal), methodology (equal), validation (equal), review, and editing (equal). R.B. was responsible for data curation (equal), formal analysis (supporting), validation (equal), review, and editing (equal). J.P. was responsible for supervision (equal), funding acquisition (lead), conceptualization (equal), validation (equal), review, and editing (equal).
Funding Statement
This study was supported by a grant funded by the Transport Accident Commission (TAC), through the Institute for Safety, Compensation and Recovery Research. J.C. was supported by an Australian Government Research Training Program (RTP) Scholarship.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Text
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.