
Abstract
Traumatic injury is linked increasingly to alterations in both stress response systems and psychological health. We investigated reactivity of salivary analytes of the hypothalamic-pituitary-adrenal axis (cortisol) and autonomic nervous system (salivary alpha amylase, sAA) during a psychosocial stress procedure in relation to psychological health outcomes. In a prospective cohort design, stress reactivity of children ages 8 to 15 years hospitalized for traumatic brain injury (TBI; n = 74) or extracranial injury (EI; n = 35) was compared with healthy controls (n = 51) 7 months after injury. Area under the curve increase (AUCinc) assessed pre-stressor to post-stressor cortisol and sAA values. Multi-variable general linear models evaluated demographic, family functioning, group, cortisol, and sAA AUCinc, and their interactions in relation to concurrent child and parent ratings of emotion regulation and internalizing and externalizing problems. Although AUCinc values were similar across groups, their relations with outcomes varied by group. Higher stress reactivity is typically associated with fewer adjustment problems. Relative to controls, greater sAA reactivity was associated with greater emotion dysregulation after TBI. In contrast, the relation of sAA reactivity with internalizing and generalized anxiety scores was flatter for both TBI and EI groups. The flattened and/or reversed direction of sAA reactivity with psychological health outcomes after TBI, and to a lesser degree EI, suggests autonomic nervous system dysregulation. Across groups, sAA reactivity interacted with sex on several psychological health outcomes with greater dysregulation in girls than in boys. Our findings highlight altered sAA, but not cortisol reactivity, as a potential mechanism of biological vulnerability associated with poorer adjustment after TBI.
Introduction
Pediatric traumatic brain injury (TBI) continues to be an immense public health burden in the United States. Nearly 50% of children with TBI are at risk for development of psychological health problems, which contribute to disability and family burden. 1 –4 Injury to the brain or body during childhood is a physical and psychological stressor linked to increases in behavior problems and emotional symptoms. 5 Although alteration in stress response systems (SRS) likely contributes to adverse changes in behavioral adjustment, 6 little is known about the relation of SRS changes to adjustment after TBI.
Behavior problems are typically categorized as internalizing problems, such as anxiety and depression that are directed inward, and externalizing problems, such as oppositionality or conduct problems directed toward the external environment. In comparison to children with bodily injuries or healthy youth, most studies report that children with TBI have elevated internalizing and/or externalizing behavior problems, including greater levels and duration of self-reported depression and anxiety symptoms. 1,3,7 –13 TBI is also associated with difficulties in emotion control and emotion regulation. 3,14
Long-term follow-up studies have shown that children with a range of TBI severity have elevated risk for internalizing and externalizing problems when assessed during adolescence or adulthood. 15 –19 Several child and family factors may predispose children to post-traumatic behavioral problems, including elevated pre-injury behavioral difficulties or executive dysfunction, limited family resources, and reduced family functioning. 3,7,14,20 –23
Few studies have examined the relation of alteration in SRS to behavioral problems after pediatric injury. SRS include the sympathetic branch of the autonomic nervous system (ANS) and the hypothalamic-pituitary-adrenal (HPA) axis. During a stressful event, such as physical injury, the sympathetic branch of the ANS activates the “flight or fight” stress response by releasing catecholamines into general circulation. The response of this system can be measured by salivary alpha amylase (sAA), a salivary enzyme released in the oral cavity during stressful events, infection, and digestion. 24,25 The HPA axis secretes cortisol, a steroid hormone, from the adrenal glands into the bloodstream. sAA and cortisol levels change in response to physical and psychosocial stressors. Stress reactivity refers to activation and engagement of resources in response to a stressor. The time course of reactivity differs across systems, with the ANS responding rapidly within minutes while the HPA axis reacts more gradually over 20-30 minutes.
Chronic exposure to stress is believed to cause wear and tear on SRS, resulting in a shift over time to hyper- or hypo-responsiveness to acute stressors that reduces the ability to generate an adaptive response to stress. 26,27 Dysregulation of SRS after an injury or stress exposure is associated with increased risk of psychological problems, such as anxiety, mood disturbance, and post-traumatic stress. 28 –31 In healthy children, behavioral outcomes are typically negatively related to reactivity such that higher analyte reactivity is associated with fewer psychological health problems. 24,29,32 –34 Findings are inconsistent across studies examining internalizing and externalizing disorders, with some reporting underactivity and others reporting overreactivity of sAA or cortisol. 35 –38
Despite the importance of SRS on adjustment, few studies have investigated how reactivity of HPA and ANS systems relate to psychological health outcomes after pediatric injury. Although cortisol and sAA have yet to show a clear relationship to psychological health outcomes after injury, post-traumatic stress symptoms that persisted after injury were preliminarily linked to TBI or EI via stress response system markers across the spectrum of injury severity. 30
The purpose of this study is to (1) investigate the independent associations of salivary analytes of HPA and ANS stress reactivity at 7 months after injury to the brain or body compared with healthy controls, and (2) to examine whether analytes are linked to concurrent child- and parent-reported psychological health outcomes in girls and boys.
Materials and Methods
Participants
Children ages 8 to 15 years old treated at the emergency department or Level 1 pediatric trauma center at Children's Memorial Hermann Hospital (University of Texas Health Science Center at Houston) for either a TBI or EI were screened. Children were eligible if they were injured in a vehicular collision causing acceleration-deceleration or blunt impact injuries (passenger in auto, auto and pedestrian, auto and bicycle, all terrain vehicle (ATV), or golf cart accidents).
Children with EI with no evidence of concussion were included to assess whether the observed outcomes in the TBI group could be because of pre-injury characteristics or the experience of injury and hospitalization instead of the head injury itself. The control group of healthy typically developing peers was recruited from the community. They were excluded if review of their lifetime medical history indicated a previous serious injury, involvement in a vehicle collision, or a previous head injury.
Participants met the following inclusion criteria: (1) proficiency in English or Spanish, (2) no previous history of major neuropsychiatric disorder (intellectual deficiency or low functioning autism spectrum disorder) that would impact the reporting of behavioral outcomes, (3) no metabolic disorders, (4) no previous medically attended TBI, and (5) residence within a 125-mile catchment radius. Criteria 2–4 were assessed during screening through a brief interview of the parent.
Between September 2014 and June 2016, 241 patients with TBI and 292 with EI were screened for eligibility; 144 and 76 met entry criteria, respectively. Figure 1 shows the patient flow and exclusions through the 7-month follow-up. The final analysis sample included TBI (n = 74), EI (n = 35), and healthy controls (n = 51). Informed written consent was obtained from each child's guardian according to Institutional Review Board guidelines; written assent was obtained from all participants.

Recruitment and participant inclusion at the 7-month follow-up by group and completion of the Trier Social Stress Test (TSST).
Table 1 contains the injury and demographic characteristics of the TBI, EI, and Control groups. Pre-injury psychological health disorders were based on a previous formal diagnosis provided by the parent during a structured interview. Cause of injury was classified by accidents involving ATVs, automobiles vs. pedestrians or bikes, falls from moving vehicles, motorcycles, and motor vehicle crashes.
Demographic and Injury Information for Traumatic Brain Injury, Extracranial Injury, and Control Groups
TBI, traumatic brain injury; EI, extracranial injury; SD, standard deviation; ADHD, attention-deficit hyperactivity disorder; ATV, all terrain vehicle; MVC, motor vehicle collision; ED, emergency department; PICU, pediatric intensive care unit.
The Abbreviated Injury Scale (AIS) measures injury on a scale of 0 to 6 for each area of the body. 39 Injury Severity Scores (ISS) were calculated by combining the highest AIS scores from three discrete anatomical areas on the body. The modified ISS (MISS) excludes AIS for head injuries of participants with TBI. 40 These scores were obtained from the hospital trauma registry. Severity of brain injury was measured using the lowest post-resuscitation Glasgow Coma Scale (GCS) scores, which measure acute eye, verbal, and motor function. 41
The TBI group was split into mild (n = 47), moderate (n = 6), and severe (n = 21) categories based on GCS scores of 3–8, 9–12, and 13–15, respectively. EI and control participants had no concussive symptoms or history of blunt head trauma.
Procedures
This project is part of a larger longitudinal study assessing traumatic stress outcome after pediatric injury. At the baseline visit four to seven weeks after injury, parents completed retrospective ratings to reflect the functioning of the child and family previous to the injury. Parents of children in the control group assessed functioning just previous to study enrollment.
Retrospective ratings of pre-injury status are standard procedure in studies of outcome after pediatric injury. 42 At the seven-month follow-up, stress reactivity and pubertal development were assessed in the laboratory as detailed below. Both parent- and child-reported psychological health outcomes were obtained to assess post-acute functioning in relation to salivary markers of stress reactivity.
Before stress induction, participants completed a neuropsychological test battery for 1.5 h and, apart from water, did not eat, drink, or exercise. Pre- and post-stressor time periods were spent completing questionnaires and resting in a quiet room.
Measures
Pre-injury covariates.
McMaster Family Assessment Device (FAD) 43 was used to assess family functioning in the pre-injury period. The FAD contains 12 items, scored 1–4, with a higher cumulative score representing worse family functioning.
Psychosocial adversity was assessed by trained interviewers and measured the child's pre-injury exposure to specific stressors: (1) divorce or separation of parents, (2) Hollingshead Index score = 4 or 5, (3) three or more children in the child's home, (4) history of abuse or neglect identified by child protective services, (5) criminal conviction of a parent, and (6) parental mental health problems receiving treatment 44 . Each item was scored as present or absent and summed.
Psychological health: Parent-report—Baseline and 7-month
Child Behavior Checklist (CBCL). 45
This was used to characterize externalizing and internalizing behavior using t-scores normalized for sex and age; higher scores indicate greater symptoms.
Behavior Rating Inventory of Executive Function (BRIEF). 46
Emotional Control subtest evaluated children's ability to regulate emotions and manage behavioral reactivity. Higher scores indicate more symptoms.
Psychological health: Self-report—seven-month
We selected child-reported subtests that evaluated self-perceived anxiety, depression, and emotional problems to align with parent-reported outcomes.
Screen for Child Anxiety and Related Emotional Disorders (SCARED).
General Anxiety and Social Phobia subtests were selected because they discriminate between children with other anxiety disorders. 47
Children's Depression Inventory (CDI). 48
The Negative Mood with Physical Symptoms and Emotional Problems factors were selected to provide measures of depressed mood with associated somatic symptoms and more generalized mood and self-esteem problems.
Pubertal Development Scale. 49
Completed by children and parents to assess pubertal status at seven months to rate changes in height, body hair, and skin. Each item scale was converted into a five-point scale like Tanner staging. 50 These converted items were then averaged to obtain a consensus score for pubertal status ranging from pre-pubertal (1) to post-pubertal (5).
Psychosocial stress reactivity and salivary analytes
Trier Social Stress Test for Children (TSST-C). 51,52
The TSST-C is a well- established measure of reactivity to psychosocial evaluative stress in children and was administered using standard procedures (see description in 30 ).
Children performed oral speaking and serial subtraction tasks while being videotaped in front of an expert panel wearing white coats. They were given no feedback on oral speaking and were instructed to try to perform better than other children. If they made an error on serial subtraction, they were corrected and asked to begin again.
Saliva samples were collected at four time intervals after established procedures.
53
Saliva was collected with 1
Because of differing kinetic response profiles of the analytes, post-stressor samples were collected directly after the task (sAA only), 20 min after (both analytes), and 40 min after (cortisol only). The samples were then frozen at -20°C and then transported to the Institute for Interdisciplinary Salivary Bioscience.
The samples were assayed in duplicate for cortisol using an enzyme immunoassay (Salimetrics, LLC, Carlsbad, CA), without modification to the manufacturer's protocol. The test volume was 25 μL, range of calibrators from 0.01 to 3.0 μg/dL, and lower limit of sensitivity was 0.007 μg/dL. Samples were assayed for sAA using a commercially available assay enzyme kit (Salimetrics LLC, Carlsbad, CA). Cortisol was expressed in units of μg/dL, and sAA was expressed in units of U/mL. The intraassay coefficient of variation was on average 10%, and the inter-assay coefficient of variation was on average 15%.
Cortisol and sAA raw value distribution were examined at each time interval. Extreme values that were 2.5 standard deviations (SDs) above the mean were winsorized, and reassigned at 2.5 SD. From each of the four collection times, area under the curve (AUC) values were calculated in relation to ground (AUCg) to measure the total secretion and in relation to increase (AUCinc) to assess change associated with the stressor. 54
Statistical approach
Analyses included participants with pre-injury parent ratings and seven-month follow-up salivary samples and parent-reported and child self-reported outcomes. After inspection of distributions, demographic characteristics, candidate predictor variables, and psychosocial outcomes were examined by group using parametric or nonparametric tests with Bonferroni post hoc comparisons across the TBI, EI, and control groups.
Post hoc chi square analyses were completed for the difference of seven month—baseline scores of CBCL and BRIEF measures to assess changes in distribution of t-scores. Difference scores were categorized as decreased (± .5 SD), no change (-.5 to .5 SD), and increased (> 3 SD). The cut point of .5 SD was selected to reflect a small to moderate effect size.
Pre-injury and follow-up behavioral and executive functioning outcomes, and cortisol and sAA AUCinc values, were compared across groups using either general linear models or nonparametric tests depending on normality and unequal variances.
Because of extreme outliers, the following data points were winsorized at 2.5 standard deviations: salivary raw data (cortisol; 9 points/8 patients; sAA 11 points/5 patients). Spearman correlation analysis examined the relation of demographic, family functioning, and salivary AUCinc values with seven-month outcomes.
Multi-variable general linear models were used to evaluate main effects of age at injury, pubertal status, sex, pre-injury family functioning, group (TBI, EI, control), and salivary AUCinc values for cortisol and sAA on parent- and child-reported outcomes.
Potential two-way and three-way interactions of group, sex, and pubertal status with AUCinc values were examined and non-significant interaction terms were trimmed from each model. Main effects were retained irrespective of significance. Models testing parent-reported outcomes controlled for pre-injury parent ratings.
All tests were two-tailed with significance of alpha = 0.05. Significant interaction effects including group were followed by planned comparisons using the Benjamini-Hochberg procedure with α = .005/3. For analyses yielding significant group
Results
Cohort description
There was no significant difference between groups in age, pubertal status, sex, ethnicity, and family functioning. There was a significantly lower proportion of white participants in the control group relative to the TBI and EI groups. Pre-injury diagnosis of anxiety, depression, or ADHD was reported in 17.6%, 17.1%, and 3.9% of subjects in the TBI, EI, and control groups, respectively. Regarding injury variables, external cause of injury did not differ between groups, with auto pedestrian and vehicle collisions being the most common. The TBI group had significantly higher ISS scores compared with the EI group. The EI group, however, had significantly higher MISS scores than the TBI group when scores were adjusted to exclude head symptoms.
More children in the TBI group required admission to the Pediaric Intensive Care Unit (PICU) than the EI group; however, the EI group underwent surgery more often. GCS scores were only reported for the TBI group, where 63.5% of the 74 patients had mild TBI.
Univariate group comparisons
Table 2 provides descriptive statistics and group comparisons of pre-injury parent ratings, as well as seven-month salivary AUCinc values and parent and child ratings. Pre-injury CBCL Internalizing scores were not significantly different between groups; however, pre-injury CBCL Externalizing scores were significantly higher in the EI group compared with the control group. Pre-injury adverse event exposure also was not significantly different between groups.
Predictor and Outcome Variables by Group
TBI, traumatic brain injury; EI, extracranial injury; SD, standard deviation; CBCL, Child Behavior Checklist; BRIEF, Behavior Rating Inventory of Executive Function; AUC, area under the curve; CDI, Children's Depression Inventory.
EI>Control, 2TBI>Control.
Parent-reported post-injury levels of CBCL internalizing and BRIEF Emotional Control were higher in the TBI group compared with the control group. Post-hoc analysis of the distribution of difference scores by group from pre-injury to seven months revealed significant differences for Internalizing, Χ 2 (4, N = 160) = 10.01, p = 0.040, Externalizing, Χ 2 = 9.74, p = 0.045, and Emotional Control scores, Χ 2 = 14.83, p = 0.005. Bonferroni corrected group comparisons indicated that the proportion of children with increased or worse Internalizing or Externalizing scores did not vary.
More children in Control and EI groups showed improved Internalizing scores than TBI whereas the proportion of children with decreased Externalizing scores did not vary by group. The TBI and EI groups had fewer decreased and more increased Emotional Control scores than controls (see Supplementary Table S1).
There were no significant group differences for child-reported SCARED Social Phobia or General Anxiety, or for CDI Emotional Problems, or Negative Mood measures. Seven-month AUCinc values for cortisol and alpha amylase were not significantly different between groups.
We examined interrelations of key dependent variables with demographic and family variables (Table 3). Significant negative correlations were found between age with CBCL internalizing scores. Parent-reported outcomes were all significantly positively correlated with family functioning. Significant negative correlations existed between cortisol AUCinc with SCARED Social Phobia and CDI Emotional Problems. sAA was not significantly related to any outcome variables.
Zero-Order Correlations of Child Demographics and Salivary Analytes With Psychological Outcomes
AUC, area under the curve; CBCL, Child Behavior Checklist; BRIEF, Behavior Rating Inventory of Executive Function; SCARED, Screen for Child Anxiety and Related Emotional Disorders; CDI, Children's Depression Inventory.
p < 0.05
Multi-variable models
Table 4 provides statistical results for multi-variable models examining the relation of salivary AA and cortisol reactivity to parent-reported psychological health outcomes at the seven-month follow-up after adjusting for pre-injury behavior ratings. Table 5 shows final multi-variable models reporting relations of salivary AUCinc and self-reported anxiety and depression symptoms assessed at the seven-month follow-up.
Final Multi-Variable Models of Parent-Reported Psychosocial Outcomes and Salivary Reactivity
BRIEF, Behavior Rating Inventory of Executive Function; TBI, traumatic brain injury; FAD, Family Assessment Device; AUC, area under the curve.
Final Multi-Variable Models of Child-Reported Psychosocial Outcomes and Salivary Reactivity
SCARED, Screen for Child Anxiety and Related Emotional Disorders; CDI, Children's Depression Inventory; TBI, traumatic brain injury; FAD, Family Assessment Device; AUC, area under the curve.
EI < Control; 2 Female > Male; 3Higher score associated with higher rating; 4TBI, EI > controls with higher reactivity associated with higher score; 5TBI > control with higher reactivity associated with higher score. See Figures 4a and 4b for depiction of group interactions.
Parent-reported outcomes: sAA.
For Internalizing problems, the three-way interaction of sAA reactivity, sex, and group was significant (Fig. 2a,2b). The relation of sAA and Internalizing scores was significantly different from 0 and negative only for control girls (B 1 = -0.00262, t = -2.27, p = 0.024), with higher Internalizing scores at lower levels of sAA reactivity. Planned group comparisons examined the relation of TBI and EI groups relative to controls for girls and boys separately using the Benjamini-Hochberg correction.

Child Behavior Checklist (CBCL) Internalizing scores varied by sex, group, and salivary alpha amylase (sAA) reactivity (p = 0.009). The relation between sAA and Internalizing ratings was statistically significant only for female controls who showed the expected higher Internalizing scores at lower sAA values and lower scores at higher sAA values. Follow-up corrected group comparisons completed for each sex found that the relation of sAA reactivity with Internalizing scores differed for girls with traumatic brain injury (TBI) and extracranial injury (EI) compared with control girls (Fig. 2a) whereas the relation did not differ by group for boys (Fig. 2b). The flattened relation in girls with TBI and EI suggests dysregulation of the ANS stress response system.
Compared with control girls, the relation of Internalizing Problems with sAA reactivity differed significantly for girls with TBI (ΔB = 0.00355, t = 2.62, p = 0.010) and EI (ΔB = 0.00403, t = 2.75, p = 0.007), indicating altered reactivity in injured girls. Values for girls in the TBI and EI groups did not differ from each other (ΔB = -0.00048, t = -0.41, p = 0.679). In contrast, sAA reactivity did not vary from control boys for boys with either TBI (ΔB = -0.00086, t = -1.12, p = 0.266) or EI (ΔB = -0.0007, t = -0.82, p = 0.412) or across the two injury groups (ΔB = -0.0002, t = -0.19, p = 0.847).
The final model for Externalizing Problem scores indicated that only the main effect of sAA reactivity was significant; higher problems were associated with higher sAA.
For BRIEF Emotional Control scores, the sAA reactivity
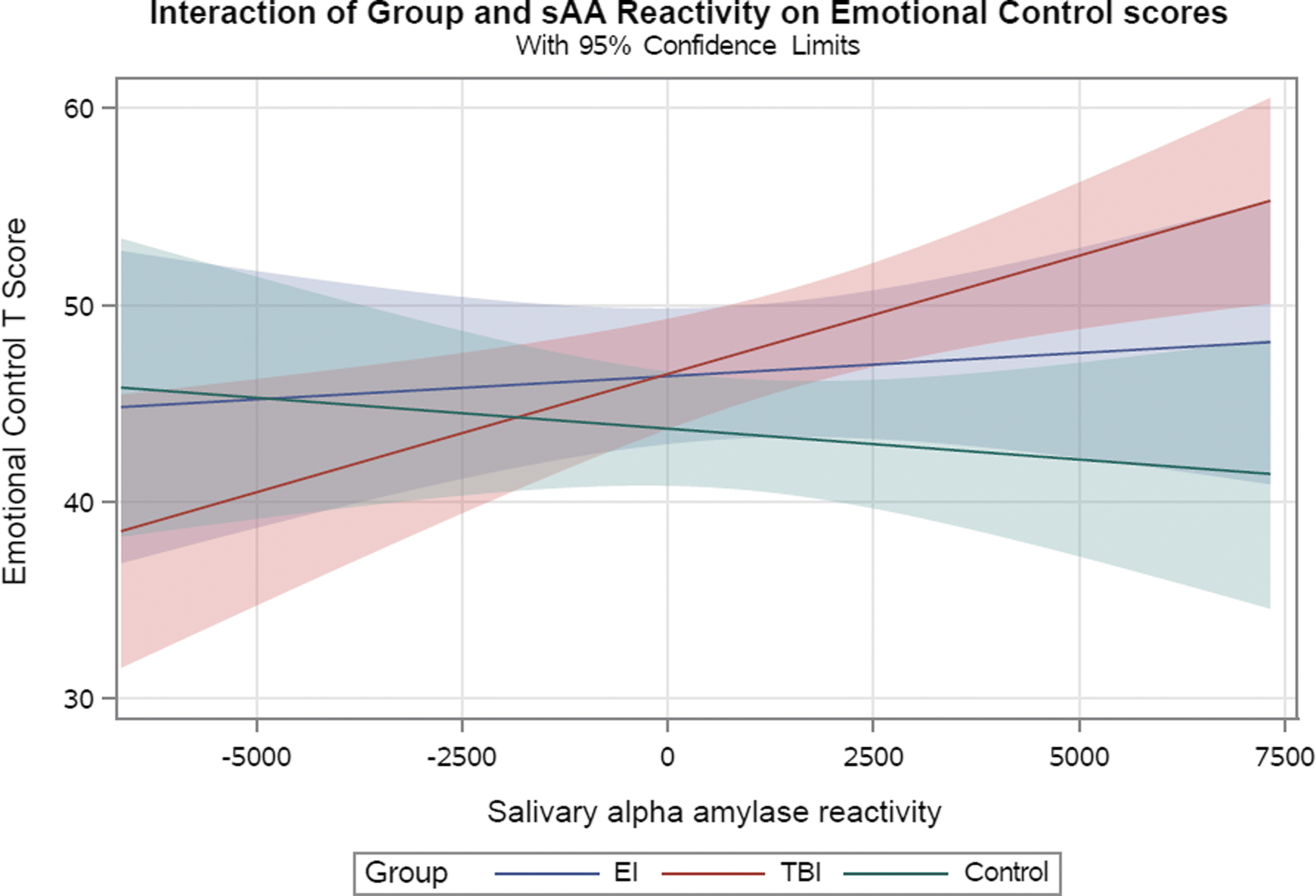
The group
Parent-reported outcomes: Cortisol.
Cortisol reactivity was not related to either Internalizing or Externalizing Problem scores and did not vary by group or demographic factors. In contrast, BRIEF Emotional Control scores had significant main effects of group, sex, and McMaster FAD. Relative to the control group, the TBI group had significantly higher scores (B = 4.5399, t = 2.86, p = 0.005), whereas the EI group did not differ (B = 3.1451, t = 1.71, p = 0.089). Emotional Control scores were lower in girls than boys and higher in families with more pre-injury dysfunction.
Self-reported outcomes: sAA.
The sAA reactivity
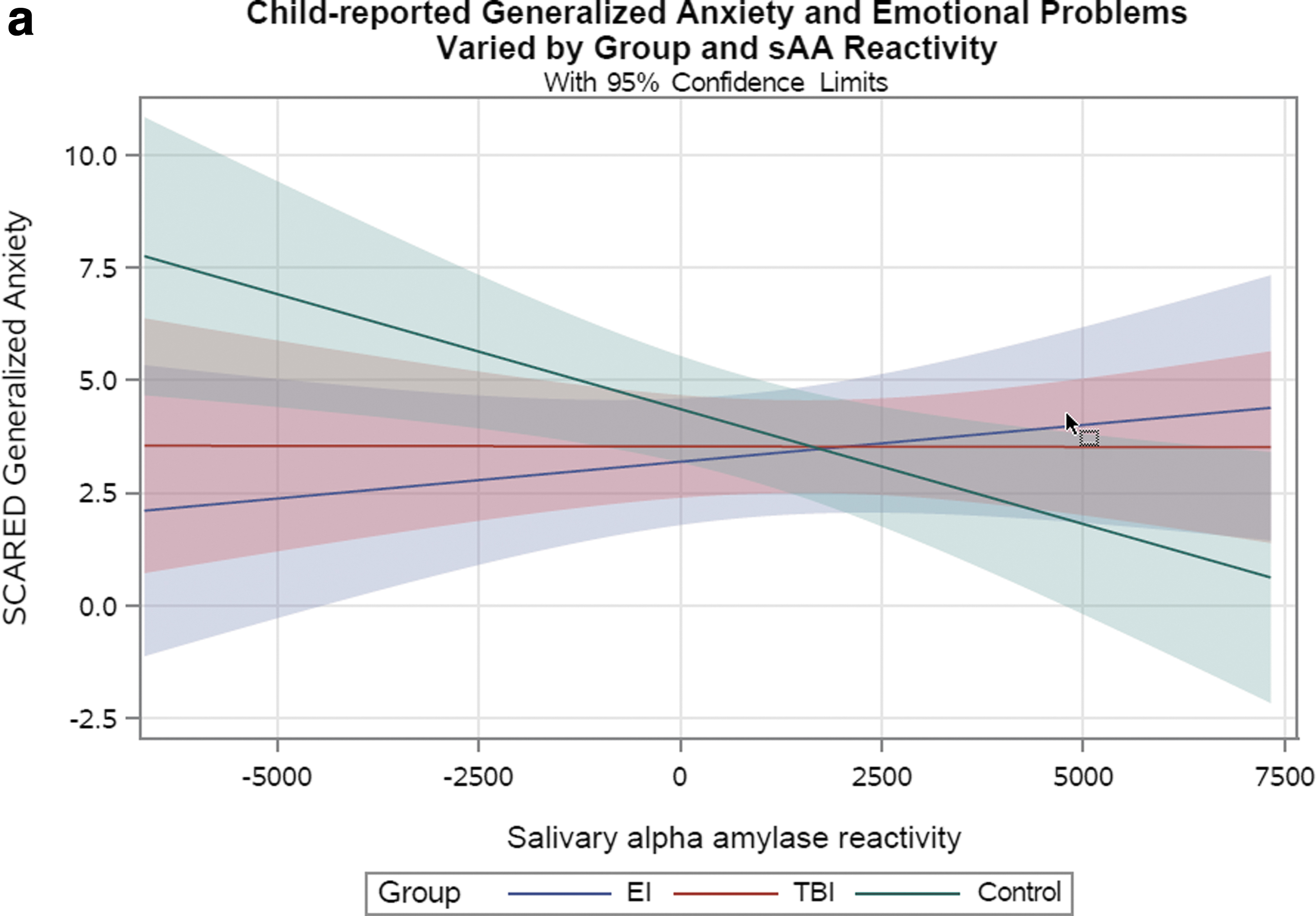
The group

The group
The sAA reactivity
Self-reported outcomes: Cortisol.
Similar to parent-reported findings, cortisol reactivity did not interact with sex or group. Higher cortisol reactivity was associated with lower Social Phobia (t = -2.67, p = 0.009) and General Anxiety (t = -2.37, p = 0.019) scores. Mood ratings were not significantly associated with cortisol reactivity.
Discussion
Little is known about how changes in stress reactivity influence adjustment after pediatric injury. We found significant dysregulation of the ANS in relation to psychological health outcomes after TBI. In the present study, reactivity of salivary sAA and cortisol were assessed seven months after injury during a psychosocial stress task. Neither sAAinc nor cortisol AUCinc differed significantly across TBI, EI, and control groups. The relation of sAA reactivity with several parent- and self-reported internalizing psychological health outcomes, however, varied by group and/or sex.
In healthy children, stress reactivity is typically negatively related to adjustment, with higher reactivity and recovery to baseline associated with fewer behavior problems. 28 –30 Relative to controls, higher sAA reactivity was associated with higher Emotional Control and Emotional Problems scores for children with TBI. In contrast, both TBI and EI groups showed flatter relations of sAA reactivity with Internalizing and General Anxiety scores. The relation of cortisol reactivity with outcomes did not differ by group.
Overall, the flattened and/or positive direction of sAA reactivity with psychological health outcomes after TBI, and to a lesser degree after EI, suggests stress system dysregulation. Our findings highlight altered sAA, but not cortisol reactivity, as a potential mechanism of biological vulnerability associated with poorer adjustment after TBI relative to healthy children.
Injury and sex effects influencing psychological health and stress reactivity
In univariate analyses, we found that TBI was associated with significant differences in Internalizing and Emotional Control problems relative to healthy children and approached traditional levels of significance for Externalizing scores. Overall, the TBI group showed significantly less improvement in Internalizing problems and significantly increased emotional dyscontrol than both comparison groups. Child-reported depression and anxiety were similar across groups.
Our findings regarding post-traumatic changes in behavior problems are consistent with previous literature showing parent ratings of increased internalizing, externalizing, and/or emotional control problems during the first year after TBI relative to healthy controls or children with EI. 3,4,7 –9,55 –58 Similar to Kirkwood et al., 8 self-reported mood problems did not differ by group in our sample. Clearly, TBI places school-aged children and adolescents at elevated risk for both internalizing and externalizing problem behaviors. 2,19 There is little evidence that significant recovery of psychological health occurs one or more years after TBI. 7,59 As a significant minority of youth experiencing TBI continue to show persistent difficulties into adulthood, 16,19 it is essential to identify biopsychosocial factors that may inform interventions to improve long-term adjustment and quality of life.
sAA.
Our findings are unique in characterizing the relation of psychological health outcomes with stress reactivity values for sAA and cortisol across injury groups and sex. In children with TBI or EI, the pattern of sAA reactivity to both Internalizing Problems and General Anxiety was flatter than in healthy comparison children.
Previous studies of sAA reactivity and psychosocial stress across different populations have identified inconsistent relations with psychological health. In relation to internalizing problems, the most common pattern involves elevated and a reduced response to the stressor. This pattern has been linked to elevated anxiety, depression, interpersonal problems, and/or childhood adverse event exposure. 54,60 –64 A similar pattern of sAA reactivity was found in plasma in children with generalized anxiety, suggesting that this pattern extends beyond salivary analytes. 65 Other studies reported no differences in either pre-stressor or reactivity sAA values in children with elevated internalizing problems. 29,66
Similar to other populations, our findings suggested attenuated reactivity was associated with higher internalizing problems. These findings are consistent with stress system dysregulation characterized by altered responsiveness to psychosocial stressors that is associated with psychological health problems. 26
In relation to Externalizing scores, neither parent ratings nor salivary analytes varied by group. For the total sample, sAA, but not cortisol reactivity, was related to Externalizing scores. Higher levels of Externalizing problems were significantly associated with higher levels of sAA reactivity. This pattern is an inversion of the usual relationship of higher levels of externalizing problems associated with lower levels of sAA reactivity. In previous work, externalizing problems have been linked to attenuated sAA reactivity in boys with disruptive behavior disorders 32 whereas other investigators found no relation between externalizing behaviors and sAA reactivity. 29
TBI was uniquely linked with greater Emotional Control and Emotional Problems in the context of higher sAA. These scales evaluate emotional regulation, situational reactivity, negative mood, and anger. Elevated symptoms may reflect personality change disorder related specifically to TBI. The most common personality change subtypes after pediatric TBI are affective instability, aggression, and disinhibition. 67 It is possible that changes in autonomic reactivity, as indicated by sAA, are additional correlates of emotion dysregulation and/or personality change specific to TBI.
Cortisol.
Surprisingly, the relation of cortisol reactivity to psychological health did not vary in injured versus healthy children. In the total sample, cortisol reactivity was unrelated to parent ratings of either Internalizing or Externalizing symptoms. In contrast, cortisol reactivity was significantly related to self-reported Social Phobia and General Anxiety. For both outcomes, the relation was negative, such that higher reactivity was associated with fewer self-reported symptoms. The multi-variable models for depression scores from the CDI approached traditional levels of statistical significance; this relation was also negative. Together, these findings indicate that sustaining a physical injury did not change the expected negative relation of cortisol reactivity with self-reported internalizing health outcomes.
Influence of sex.
Despite the importance of considering sex as a biological variable, few studies have examined sex as a main effect or as a moderator of the relation of TBI to behavioral or stress system outcomes. We found that sex moderated sAA reactivity on several internalizing outcomes. In relation to group effects, girls with TBI and EI had a more positive relation of sAA to Internalizing Problems scores than Control girls, again suggesting greater adjustment problems associated with higher stress reactivity.
Our finding of elevated risk for Internalizing Problems in girls with TBI who show higher sAA reactivity is consistent with girls being more likely than boys to develop depressive symptoms after a stressful event. 38 Moreover, female sex is a predictor of internalizing problems persisting into adulthood after childhood TBI, 16 highlighting the vulnerability of girls to some long-term adverse psychological health outcomes after TBI.
Our remaining findings regarding sex differences were consistent across both injured and control groups. For girls, greater sAA dysregulation was associated with elevated Social Phobia ratings, and greater cortisol dysregulation was associated with higher Negative Mood ratings. This pattern of findings of elevation in selected internalizing symptoms at higher levels of either sAA or cortisol reactivity represents an inversion of the usual relationship of higher levels of reactivity associated with fewer psychological health symptoms. 50,51
Our findings are in line with previous work showing that girls with high sAA reactivity had elevated depression scores relative to boys. 68 For boys in our sample, Emotional Control ratings were elevated relative to girls, but did not vary by either sAA or cortisol reactivity. This varies from studies reporting that externalizing problems may be associated with low cortisol activity in boys, especially those with callous-unemotional traits. 33,69,70 Clearly, additional work is needed to unravel the relations of sex, SRS analytes, and outcomes in youth with a range of injury types and psychological health profiles.
Developmental and family influences
Psychological health outcomes after injury are shaped by a variety of demographic and family factors. Because the ages of our sample spanned the pubertal transition, we assessed potential influences of age and pubertal status, as well as family functioning, in multi-variable models. Surprisingly, neither age nor pubertal status was significantly related to parent-reported outcomes. For child-reported variables, pubertal development was significantly related only to General Anxiety and was significant in models accounting for sAA or cortisol reactivity. In both cases, more advanced pubertal development was associated with endorsement of more generalized anxiety symptoms.
Our findings are consistent with recent findings that typically developing girls are particularly vulnerable to internalizing problems, particularly beginning at the pubertal transition. 71 –73
Given the importance of family factors in shaping children's psychological health, we examined whether pre-injury estimates of family functioning were related to parent- and self-reported outcomes. More problems in family functioning assessed before injury were specifically linked to parent ratings of higher Emotional Control scores in models including either analyte.
Stress reactivity is likely related to context, such that elevated biological activation of SRS may be associated with poor outcomes when associated with adversity but with positive outcomes when associated with support. 34,74 This is consistent with previous findings that adolescents with the combination of high cortisol reactivity and a high level of family stress had elevated internalizing and externalizing problems. 75 Family functioning may be a promising target of intervention to reduce emotional dyscontrol and moderate SRS activation after TBI.
Limitations and future directions
To our knowledge, this is the first study to characterize alterations in the reactivity of salivary stress markers in boys and girls sustaining injuries in relation to a range of psychological health outcomes. Our findings highlight alteration in sAA, but not cortisol reactivity, as a potential mechanism of biological vulnerability associated with poorer adjustment after TBI. This study, however, is not without limitations.
The sample targeted children treated in the ED, 23 h observation unit, or hospitalized at a tertiary care center after vehicle-related injuries. The findings should be extended to children with other external causes of injury and those treated in the community. Although we adjusted for pre-injury estimates of behavior problems and family functioning, it is possible that other pre-injury factors may have influenced our findings. We did not obtain pre-injury child self-ratings, which precluded analysis of change. The study was adequately powered; however, there may be reduced power to detect differences related to interactions of sex, injury type, and injury severity. We did not evaluate how participants perceived the social evaluative threat of the TSST-C challenge; this may influence their salivary analyte responses to the TSST and relations with self- and parent-ratings of adjustment.
Strengths of the study include the prospective cohort design that assessed pre-injury child and family factors and allowed examination of stress system reactivity across ANS and HPA systems. Reactivity was examined in relation to both self- and parent-reported psychological health outcomes in children experiencing physical trauma and TBI. Future studies should examine coordination across ANS and HPA systems to identify general effects and stresses associated with injury and isolate relations that are specific to TBI to inform psychological health interventions.
The high incidence of pediatric injury and persistence of psychological health concerns results in a substantial public health burden. It is essential to understand links between neurobiological changes after TBl and long-term psychological health outcomes. Additional work is urgently needed to develop targeted strategies that guide behavioral and/or pharmacological therapies to normalize stress system reactivity and improve long-term adjustment.
Transparency, Rigor, and Reproducibility Summary
The study was not formally registered because it was completed in 2016 before the development of independent repositories. The analysis plan was not formally pre-registered. The planned sample size was 180, and we used 160 cases in power analyses to account for likely attrition from the targeted sample. We used regression to estimate power using ordinary least squares instead of maximum likelihood.
In considering such models, effect sizes are determined by the amount of variance attributable to a specific predictor relative to the error variance. Cohen's f2 varied from about .05 to about .15. We estimated a model with 10 predictors and considered power for the test of the overall model and for the effect of a single variable within the model using an alpha of .05 and a sample of 160. Power for testing the overall model exceeded .80 when the R2 was at least .10 (f 2 = .111) and the power to detect a single variable as a significant contributor to prediction was .80 even if the R2 change was only .05 and the overall R2 was .05. The study was amply powered.
Figure 1 contains the consort diagram. The key inclusion criteria and behavioral outcomes are Common Data Elements for pediatric TBI. All salivary assessments were handled using standard protocols, and analyses were completed by Salimetrics LLC as described in Methods. Persons performing the analyses and patients were blinded to results of biomarker measurements. Outliers for salivary data were defined as >2.5 SD above the mean and were winsorized. Correction for multiple comparisons used the Bonferroni or Benjamini-Hochberg procedure. No replication or external validation studies have been performed or are planned at this time to our knowledge.
De-identified data and analytic code are not available in a public archive but will be made available according to institutional IRB standards by emailing the corresponding author as of 12-31-2023. No future use of biofluid samples is possible because insufficient quantities remain.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the granting institute. We gratefully acknowledge the contributions of Dr. Paul Swank to the analytic plan prior to his death.
Authors' Contributions
Dr. Ewing-Cobbs: conceptualization (co-lead), writing of the original draft (co-lead), review, and editing (equal). Dr. Danna: conceptualization (co-lead), writing of the original draft (co-lead), data analysis (equal), review, and editing (equal). Dr. Tolar: data analysis (lead), writing and reviewing (equal). Dr. Granger: methodology (lead), review, and editing (equal). Dr. Cox: review and editing (equal).Dr. Prasad: conceptualization (co-lead), review, and editing (equal).
Funding Information
This work was funded in part by National Institutes of Health R01 NS046308.
Author Disclosure Statement
DAG is founder and Chief Scientific and Strategy Advisor at Salimetrics LLC and Salivabio LLC. These relationships are managed by the policies of the committees on conflict of interest at the Johns Hopkins University School of Medicine and the University of California at Irvine. For Drs. Ewing-Cobbs, Cox, Tolar, Prasad and Danna, no conflicts of interest exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.