
Abstract
This study aims to investigate the brain gray matter volume (GMV) alterations of pediatric complete thoracolumbar spinal cord injury (SCI) without fracture or dislocation (SCIWOFD) using voxel-based morphometry (VBM) analysis and assess the sensitive neuroimaging biomarkers that may be surrogate targets to enhance brain plasticity. A total of 52 pediatric subjects (age range, 6–12 years), including 25 pediatric SCIWOFD patients and 27 typically developing (TD) children were recruited. An independent two-sample t test was performed to assess between-group differences of brain GMV. Partial correlation analyses were performed to explore the correlations between GMV values and The International Standards for Neurological Classification of Spinal Cord Injury scores, age at the time of injury, time after initial SCI. Receiver operating characteristic analysis was performed to compute the sensitivity and specificity of the imaging biomarkers for pediatric SCIWOFD diagnosis. As for the results, pediatric SCIWOFD patients showed significantly decreased GMV of bilateral cerebellum lobule VIII, right middle occipital gyrus and putamen (PUT), left pallidum (PAL) and thalamus, and increased GMV of vermis III, right cerebellum lobule VI, and supramarginal gyrus. In addition, GMV of left PAL and right PUT were negatively correlated with the pinprick/light touch sensory scores in pediatric SCIWOFD patients. Finally, when using the GMV values of left PAL and right PUT in combination as the predictor, area under the curve reached the highest—0.93. These findings provided evidence that the brain undergoes GMV changes after pediatric SCIWOFD, which may suggest important targets for functional remodeling after SCI in children and provide valuable information for the development of novel and effective rehabilitation therapies in the future.
Introduction
Brain plasticity has been reported in patients with spinal cord injury (SCI), but most studies have focused on adult SCI. 1 –6 Because of the particularity of pediatric growth and development, there are few studies on pediatric SCI. At present, the research on pediatric SCI has focused mainly on epidemiological investigation, 7 complications, 8 rehabilitation treatment, 9,10 and spinal cord diffusion tensor imaging (DTI). 11 –13 There is no relevant report on the potential structural and functional changes of the brain in pediatric SCI. Exploring the microstructural changes of the brain after SCI, however, may help us to deeply understand the pathological mechanism and provide new perspectives for future therapeutic targets.
Because of the particularity of the biomechanics of the pediatric spine (the compliance of the spinal cord is less than that of the spine), SCIs in children are often absent radiographic evidence of fracture or dislocation (SCIWOFD), 14,15 and the type of complete thoracolumbar SCI is common.
The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) is currently used to classify the extent of motor and sensory impairment after SCI 16 ; however, recent reports indicate that ISNCSCI is of no practical value for children under 6 years of age because of the poor coordination. 17 Therefore, it is essential to develop an objective, quantitative, and reliable method for assessment, which is particularly important for younger children.
Previous studies have confirmed that spinal cord DTI can be used as a better objective evaluation method to replace ISNCSCI. 11 –13 Spinal cord DTI, however, focused mainly on the local injury lesions in the spinal cord while neglecting the potential structural and functional alterations of the brain. On the other hand, because the results of spinal DTI depend mainly on the operator's selection of the region of interest, the results are relatively subjective. We hope to find a more accurate and objective imaging evaluation index.
Voxel-based morphometry (VBM), which is an automated and unbiased method, can quantify the brain gray matter volume (GMV) changes 18 and has already been used widely in adults SCI research. 1 –3,5 To our knowledge, there have been no studies using VBM to analyze brain structural changes in children with SCI.
Therefore, the purpose of this prospective pilot study is three-fold: (1) to investigate the brain GMV alterations of pediatric SCIWOFD with complete thoracolumbar (non-cervical) SCI using VBM; (2) to evaluate the correlations between GMV values and developmental factors (including the age at the time of injury and time after initial SCI), and clinical neurological variables as measured by ISNCSCI in pediatric SCIWOFD; (3) To assess the diagnostic and predictive value of brain structural alterations in pediatric SCIWOFD.
Methods
Participants
The current study included 25 right-handed pediatric SCIWOFD patients with complete thoracolumbar injury (≥2 months post-injury, age range, 6–12 years; mean age, 8.36 ± 1.65; two males and 23 females) and 27 right-handed typically developing (TD) children with no evidence of spinal cord pathology (age range, 6–12 years; mean age, 8.48 ± 1.57; four males and 23 females). Subjects with SCIWOFD were excluded from the study if the following conditions were present: (1) They had sustained a traumatic brain injury; (2) they were unable to tolerate magnetic resonance imaging (MRI); (3) they have neuropsychiatric disease. The TD subjects were excluded from the study if the following conditions were present: (1) they were unable to tolerate MRI; (2) they had a history of neuropsychiatric illness.
Table 1 details the demographic information of the pediatric SCIWOFD patients (including the etiology of injury—among them, 21 pediatric patients had a traumatic history after backbend during dance practice—age at the time of injury, time after initial SCI, level and severity of injury, whether there is sensory plane shift and increased muscle tone). The extent of motor and sensory impairment was assessed by a qualified clinician using the classification scale of ISNCSCI. 16
Clinical Data of Pediatric Spinal Cord Injury Without Fracture or Dislocation Patients With Complete Thoracolumbar Injury
Pediatric patients had a clear traumatic history after backbend during dance practice. The level of lesion refers to the magnetic resonance imaging level.
AIS, American Spinal Injury Association Impairment Scale; AIS A, complete injury.
Written informed assent (child) and consent (parent) were obtained under the protocol approved by the Medical Research Ethics Committee of Xuanwu Hospital, and the Declaration of Helsinki. All subjects underwent a complete ISNCSCI examination. All the pediatric patients classified as American Spinal Injury Association Impairment Scale A (complete SCI).
MRI data acquisition
Images were obtained using a 3.0-T MRI system with a 12-channel phased-array head coil. A conventional brain axial fluid-attenuated inversion recovery sequence was scanned to exclude visible brain abnormalities. High-resolution three-dimensional (3D) structural T1-weighted images were acquired in sagittal orientation using a 3D magnetization-prepared rapid gradient-echo sequence (MP-RAGE) for 6:59 min with the following parameters: repetition time (TR) = 1800 msec; echo time (TE) = 2.13 msec; inversion time (TI) = 1100 msec; flip angle (FA) = 9 degrees; number of slices = 192; slice thickness = 1 mm; field of view (FOV) = 256 × 256 mm2; matrix = 256 × 256. The latter parameters resulted in an isotropic voxel size of 1 × 1 × 1 mm3.
Voxel-based morphometry
Post-processing of structural data was performed using Statistical Parametric Mapping (SPM) software implemented in MATLAB 2013a (Math Works, Natick, MA). The steps were as follows: First, each structural MRI (sMRI) was reoriented manually to place the anterior commissure at the origin and the anterior–posterior commissure in the horizontal plane. Next, images were segmented into GM, white matter (WM), and cerebrospinal fluid (CSF) areas, using the tissue probability templates in the Chinese pediatric (CHN-PD) atlases, which were constructed based on high-quality T1-and T2-weighted MRI from 328 cognitively normal Chinese children aged 6–12 years. 19
In addition, individual GM and WM components were normalized into the same template (from the CHN-PD atlases) using the Diffeomorphic Anatomical Registration through Exponentiated Lie algebra (DARTEL) algorithm. 20 The normalized GM component was modulated to generate the relative GMV multiplied by the non-linear part of the deformation field at the DARTEL step. The resulting GMV images were then smoothed with an 8-mm full-width at half-maximum Gaussian kernel.
Statistical analyses
To assess the between-group (pediatric SCIWOFD patients vs. TD children) differences of GMV of the whole brain, an independent two-sample t test was performed with age and gender as covariates using SPM. The significance threshold was set to Family Wise Error (FWE) correction (peak-level, p < 0.05, cluster size = 50).
Then, to explore the correlations between the GMV values and ISNCSCI scores, age at the time of injury, time after initial SCI, partial correlation analyses were performed with gender being used as nuisance covariate (p < 0.05, SPSS20.0).
Finally, we used receiver operating characteristic (ROC) analysis with SPSS20.0 to compute the sensitivity and specificity of the imaging biomarkers for pediatric SCIWOFD diagnosis. The ROC analysis essentially employed a binary classifier of pediatric SCIWOFD patients versus TD children as the discrimination threshold, which was varied from high to low. We created the ROC curve by plotting the true positive rate against the false positive rate at various thresholds.
Results
Demographic and clinical characteristics
There were 25 right-handed pediatric SCIWOFD patients with complete thoracolumbar injury (≥2 months post-injury, age range, 6–12 years; mean age, 8.36 ± 1.65; two males and 23 females; among them, 21 pediatric patients had a clear traumatic history after backbend during dance practice) and 27 right-handed TD children with no evidence of spinal cord pathology (age range, 6–12 years; mean age, 8.48 ± 1.57; four males and 23 females) who were recruited in this study. Demographic and clinical data for all the pediatric SCIWOFD patients are shown in Table 1. No statistically significant differences were found between pediatric SCIWOFD patients and TD children in age and gender.
Abnormal brain structural changes in pediatric SCIWOFD patients
Compared with the TD children, pediatric SCIWOFD patients showed significantly decreased GMV in bilateral cerebellum lobule VIII, right middle occipital gyrus (MOG) and putamen (PUT), left pallidum (PAL) and thalamus (THA), and increased GMV in vermis III, right cerebellum lobule VI and supramarginal gyrus (SMG) (peak-level FWE correction with p < 0.05, cluster size = 50, shown in Table 2 and Fig. 1).
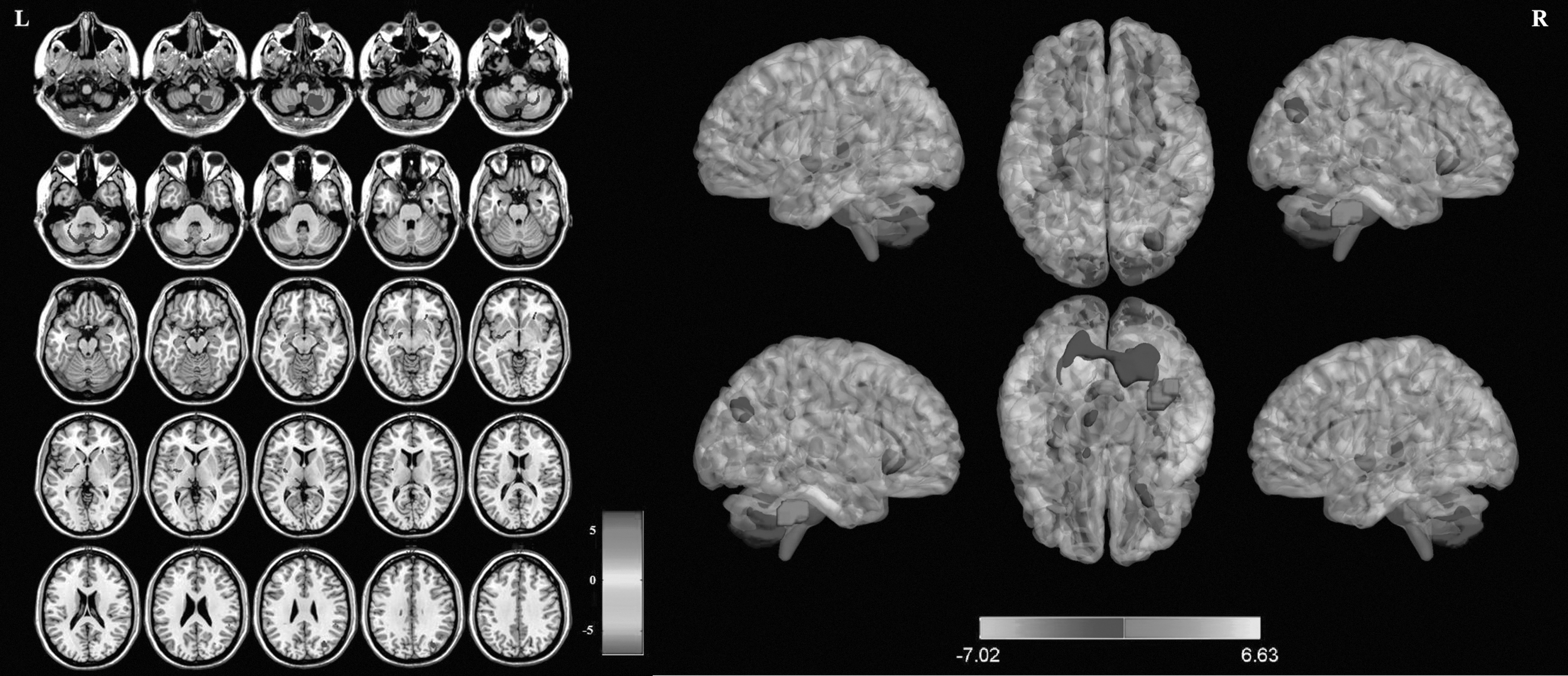
Regions showing intergroup differences in gray matter volume (GMV) between pediatric spinal cord injury without fracture or dislocation (SCIWOFD) patients and typically developing (TD) children. Compared with the TD children, the pediatric SCIWOFD subjects showed significantly decreased GMV in bilateral cerebellum lobule VIII, right middle occipital gyrus and putamen, left pallidum and thalamus, and increased GMV in vermis III, right cerebellum lobule VI, and supramarginal gyrus (peak-level FWE correction with p < 0.05, cluster size = 50).
Regions Showing Gray Matter Volume Alterations in Pediatric Spinal Cord Injury Without Fracture or Dislocation Patients With Complete Thoracolumbar Injury
GMV, gray matter volume; MNI, Montreal Neurological Institute; MOG, middle occipital gyrus; PUT, putamen; PAL, pallidum; THA, thalamus; SMG, supramarginal gyrus.
Correlations between clinical variables and GMV values in significantly changed regions in pediatric SCIWOFD patients
Partial correlation analysis showed that the pinprick/light touch sensory scores were negatively correlated with the GMV values of left PAL (p = 0.019, r = -0.485, shown in Fig. 2A) and right PUT (p = 0 .007, r = -0.543, shown in Fig. 2B ) in pediatric SCIWOFD patients. No significant correlations were found between the age at the time of injury, time after initial SCI, and GMV values (p > 0.05).
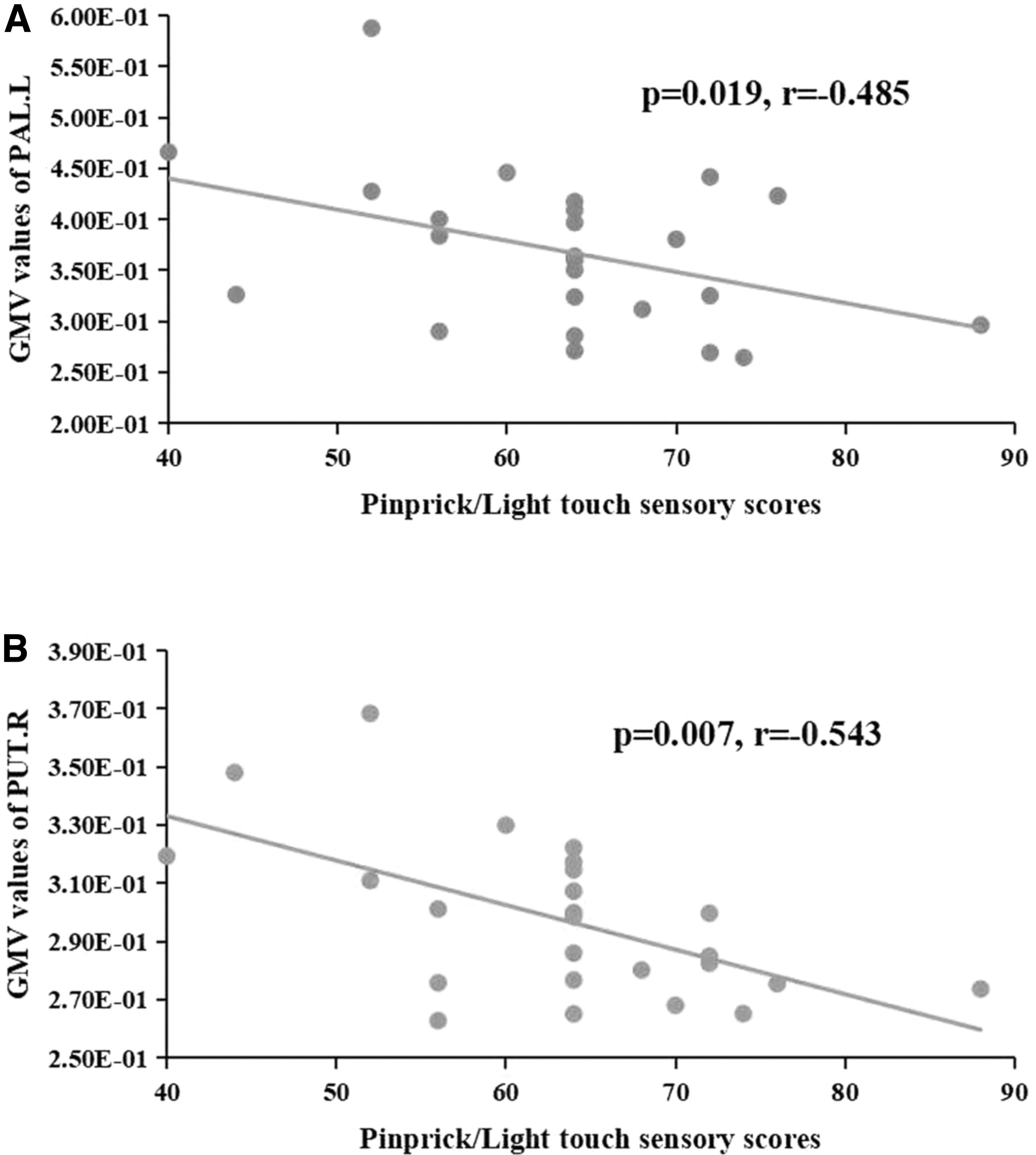
The correlation between clinical variables and gray matter volume (GMV) in pediatric patients with spinal cord injury without fracture or dislocation (SCIWOFD). Partial correlation revealed negative correlations between the pinprick/light touch sensory scores and the GMV values of left pallidum (PAL) (p = 0.019, r = -0.485, [
ROC analysis of VBM index as sensitive imaging biomarkers for pediatric SCIWOFD
Results of ROC curve analysis of the brain GMV parameters in pediatric SCIWOFD are shown in Table 3. Figure 3 shows the sensitivity and specificity of the GMV values of the left PAL and right PUT in combination, with a sensitivity of 96.3%, specificity of 80%, and area under the curve (AUC) of 0.93 (95% confidence intervals: 0.851 to 1.009).
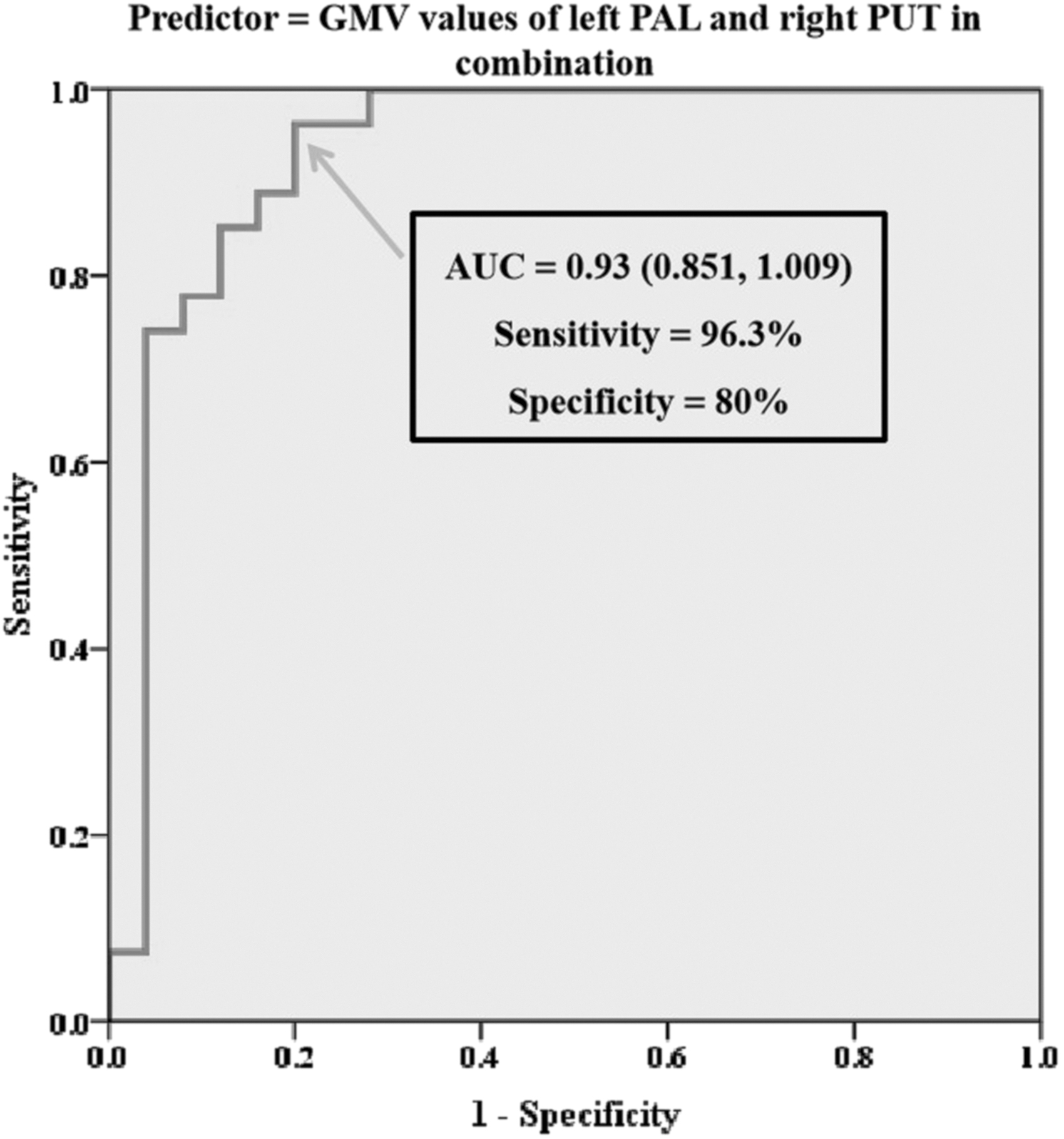
Receiver operating characteristic (ROC) curve between pediatric spinal cord injury without fracture or dislocation patients and typically developing children, when using the gray matter volume (GMV) values of left pallidum (PAL) and right putamen (PUT) in combination as the predictor. The area under the curve (AUC) for the ROC was 0.93 (95% confidence intervals: 0.851 to 1.009), with the sensitivity of 96.3%, specificity of 80%.
Results of Receiver Operator Characteristic Curve Analysis of the Brain Gray Matter Volume Parameters in Pediatric Spinal Cord Injury Without Fracture or Dislocation
Under the non-parametric assumption.
Null hypothesis: true area = 0.5.
AUC, area under the curve; MOG, middle occipital gyrus; PUT, putamen; PAL, pallidum; THA, thalamus; SMG, supramarginal gyrus.
Discussion
Major findings
The present study characterized significantly changed brain GMV of pediatric complete SCIWOFD, among which the left PAL and right PUT showed significant correlation with the ISNCSCI scores. These new imaging biomarkers may suggest important targets for functional remodeling after SCI in children.
Abnormal brain GMV changes in pediatric SCIWOFD patients
The PUT and PAL, as the key hubs of basal ganglia, have the function of controlling muscle movement, and combine with the hypothalamus to become the regulatory center of instinctive turning over and complete the instinctive reflex activities such as walking.
In this study, we found that pediatric SCIWOFD can lead to GMV atrophy in subcortical areas such as the thalamus and basal ganglia (PUT and PAL), regions that have direct connectivity with the sensorimotor cortex and are important for sensorimotor functioning. 21 A previous study had reported abnormalities in the corticothalamic pathway during wrist extension in patients with SCI. 22 Our findings may be because of axonal degeneration in the lesions, leading to changes in the corticothalamic pathways that reach cortical areas via the basal ganglia and thalamus. 23,24
In this study, we also found the GMV atrophy in cerebellum lobule VIII, which was associated with cognitive performance. 25 A recent study in children and adolescents (aged 8–17 years) reported that increased GMV in cerebellum lobule VII and VIII was associated with better cognitive scores. 26 It has also been documented that SCI can lead to cognitive and memory impairment in adult patients. 27
Our result seems to suggest that SCI can also lead to cognitive and memory impairment in pediatric patients. But here's an interesting finding: in children, the direction of the relationship between the GMV of cerebellum lobule VIII and cognitive scores may depend on the developmental stage, 26,28 with negative relationship in younger children; later in adolescence the relationship was positive, as was typical in adult cohorts. The age of children with SCI in our study was 6–12 years old; most of the children had not yet reached adolescence.
It is unclear whether the GMV atrophy in cerebellum lobule VIII indicated a decline or compensatory enhancement of cognitive memory; unfortunately, there were no relevant cognitive scales in our sample. We will add relevant scales in the future studies and conduct an in-depth study. In addition, we found GMV atrophy in MOG, which has a principal role in visual processing. 29 Previous studies also revealed that SCI can result in visual-related brain GM atrophy in adult patients. 30
In addition to the GMV atrophy in the above regions, we also found increased GMV in the right cerebellum lobule VI and SMG, vermis III. Palesi and associates 31 showed strong correspondence between the anterior cerebellum (I–V) and lobule VI and sensorimotor circuits. 28,32,33 The increased GMV in cerebellum lobule VI may be because of the increased muscle tone after SCI in pediatric patients.
To test our hypothesis, we tracked the current sensorimotor status of the pediatric patients with SCI through telephone follow-up and found that more than half of the pediatric patients showed a downward shift in the sensory plane and high muscle tone (52%). The SMG (secondary somatosensory cortices) is responsible for integrating tactile or painful stimuli with higher-level functions. 34 The anterior vermis, especially vermis III and the deep nuclear masses, is involved in sensing pain caused by thermal stimulation. 35 Increased GMV in SMG and vermis III may be a compensation for the motor dysfunction in SCI or may indicate a potential risk for paresthesia in pediatric patients with SCI.
The risk of neuropathic pain (NP) after chronic SCI in adults is up to 50–80%, 36,37 but the incidence in pediatric patients is unclear. We will continue to follow up these pediatric patients to find whether there will be paresthesia or even NP in the future.
Correlations between clinical variables and GMV values in pediatric SCIWOFD patients
In subsequent correlation analysis, GMV values of the left PAL and right PUT revealed significantly negative correlations with the pinprick/light touch sensory scores in pediatric SCIWOFD patients. The PUT and PAL, as the key hubs of basal ganglia, have the function of controlling muscle movement; the negative correlations between GMV of PUT/PAL and sensory scores may suggest a sensory compensation for the motor dysfunction in pediatric SCI or may suggest a potential risk for paresthesia, which need to be verified for further follow-up studies.
Sensitive imaging biomarkers for the diagnosis of pediatric SCIWOFD
Previous studies have confirmed that spinal cord DTI can be used for the diagnosis of pediatric SCI with good to strong predictive accuracy (AUC = 0.88 ∼ 0.93). 12 In our current study, when using the GMV values of the left PAL and right PUT in combination, which were significantly correlated with the ISNCSCI scores in pediatric SCIWOFD patients, the AUC reached to 0.93 (95% confidence intervals: 0.851 to 1.009), with the sensitivity of 96.3%, specificity of 80%. The result suggested the potential value of brain GMV changes as sensitive imaging biomarkers for pediatric SCIWOFD and provided valuable information for the development of novel and effective rehabilitation therapies in the future.
Future considerations
Some limitations of our study should be noted. First, the sample size was relatively small, and all of the participants underwent complete thoracolumbar SCI; future studies with a larger sample size and with different injury severity and levels will be included for an in-depth mechanism discussion. Second, our study is a cross-sectional study. Longitudinal studies are needed to reveal the brain reorganization with disease progression and intervention of rehabilitation training, aiming to search for sensitive imaging biomarkers that predict future outcome of pediatric patients with SCI and develop targeted rehabilitation plan over time to improve maximize recovery.
Finally, pediatric participants in this study did not receive the evaluation of cognitive scale (e.g., mini-mental state examiniation, Montreal Cognitive Assessment, auditory verbal learning test, etc.), Visual Analogue Scale/Score, and visual function, which will be applied to our follow-up study in the future.
Conclusions
The present findings suggest significant brain GMV alterations of pediatric SCIWOFD, among which the left PAL and right PUT showed significant correlations with the ISNCSCI scores, raising the possibility that GMV changes of these two regions may serve as neuroimaging biomarkers. The ROC analysis that revealed the high AUC of the GMV values with left PAL and right PUT in combination (AUC = 0.93) further confirmed this. These new imaging biomarkers may suggest important targets for functional remodeling after SCI in children.
Transparency, Rigor, and Reproducibility Summary
The study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University (Ethics No: [2020] 003) and was registered as a clinical trial (Registration No: ChiCTR2000032793). 1. The analysis plan was registered prior to beginning data collection. 2. A sample size of 52 subjects was planned to yield 80% power to detect a statistically significant correlation (Spearman r > 0.35) with (primary clinical outcome) with a p-value <0.05. 3. 60 potential participants were screened, imaging data were obtained from 60, and successfully analyzed in 52. 4. Participants were told the results of the imaging assessments after the final clinical observations had been made. Imaging acquisition and analyses were performed by team members blinded to relevant characteristics of the participants, and clinical outcomes were assessed by team members blinded to imaging results. 5. All equipment and software used to perform imaging and preprocessing are widely available from commercial sources. 7. The key inclusion criteria and outcome evaluations are established standards. 8. Replication by the study group is ongoing, preregistered at clinical trial (Registration No: ChiCTR2000032793). 11. This article will be published under a Creative Commons Open Access license, and upon publication will be freely available at
Footnotes
Acknowledgment
The authors thank the patients and healthy volunteers who participated in this study.
Authors' Contributions
Weimin Zheng: writing–original draft (lead); formal analysis (lead). Weimin Zheng, Nan Chen: conceptualization (equal). Nan Chen: writing–review and editing (lead). Ling Wang/Beining Yang/Qian Chen/Wen Qin: software (supporting). Yongsheng Hu/Jubao Du/Xuejing Li/Xin Chen/Baowei Li/Tengfei Liang: methodology (supporting). Kuncheng Li/Jie Lu: conceptualization (supporting).
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Funding Information
This study was supported by the National Natural Science Foundation of China (No. 81871339 and 81271556), the Beijing Municipal Natural Science Foundation (No. 7113155), and the Science Foundation of Beijing Municipal Commission of Education (No. KM201210025013).
Author Disclosure Statement
No competing financial interests exist.