
Abstract
Traumatic brain injury is a global public health problem associated with chronic neurological complications and long-term disability. Biomarkers that map onto the underlying brain pathology driving these complications are urgently needed to identify individuals at risk for poor recovery and to inform design of clinical trials of neuroprotective therapies. Neuroinflammation and neurodegeneration are two endophenotypes potentially associated with increases in brain extracellular water content, but the nature of extracellular free water abnormalities after neurotrauma and its relationship to measures typically thought to reflect traumatic axonal injury are not well characterized. The objective of this study was to describe the relationship between a neuroimaging biomarker of extracellular free water content and the clinical features of a cohort with primarily complicated mild traumatic brain injury. We analyzed a cohort of 59 adult patients requiring hospitalization for non-penetrating traumatic brain injury of all severities as well as 36 healthy controls. Patients underwent brain magnetic resonance imaging (MRI) at 2 weeks (n = 59) and 6 months (n = 29) post-injury, and controls underwent a single MRI. Of the participants with TBI, 50 underwent clinical neuropsychological assessment at 2 weeks and 28 at 6 months. For each subject, we derived a summary score representing deviations in whole brain white matter extracellular free water volume fraction (VF) and free water-corrected fractional anisotropy (fw-FA). The summary specific anomaly score (SAS) for VF was significantly higher in TBI patients at 2 weeks and 6 months post-injury relative to controls. SAS for VF exhibited moderate correlation with neuropsychological functioning, particularly on measures of executive function. These findings indicate abnormalities in whole brain white matter extracellular water fraction in patients with TBI and are an important step toward identifying and validating noninvasive biomarkers that map onto the pathology driving disability after TBI.
Introduction
Traumatic brain injury (TBI) is a global public health issue where even in its most mild form—mild TBI or concussion—there is a substantial risk for chronic post-traumatic symptoms and long-term disability. 1 Neurotrauma results in injury to multiple brain structures including neurons, glia, and cerebral blood vessels, with considerable person-to-person variability in terms of severity and anatomic location of injury. This mechanistic and spatial heterogeneity likely underlies the interindividual variability in outcomes post-injury. Abnormalities seen on clinical neuroimaging such as subarachnoid hemorrhage and contusions may improve long-term outcome prediction after TBI, 2,3 but do not explain enough of the variance to be useful tools for risk stratification. Quantitative tools, such as advanced neuroimaging, offer promise for providing more accurate risk stratification after TBI.
One such advanced neuroimaging tool used extensively in TBI studies is diffusion tensor imaging (DTI) obtained from diffusion-weighted magnetic resonance imaging (MRI). DTI models white matter microstructural integrity with variables such as fractional anisotropy (FA) and mean diffusivity (MD). 4,5 Multiple studies have demonstrated diffuse white matter abnormalities, namely decreases in FA and increases in MD, across the TBI severity spectrum. 6 Although primarily thought to reflect diffuse axonal injury, DTI models water diffusion, which could be abnormal for a multitude of reasons, including axonal injury, gliosis, atrophy, edema/inflammation, and partial volume effects at brain/CSF boundaries. 7 All of these processes result in similar effects on FA and MD and their presence reduces the specificity of DTI for detecting axonal pathology. 8 Given that all of these processes occur in TBI, novel methods for characterizing white matter microstructure are needed to improve the specificity of quantitative neuroimaging biomarkers with the goal of creating a clinical decision making tool in TBI. One such method is free water correction, 8 which models water diffusion at the extracellular (isotropic) level. Water diffusion is more isotropic in the presence of CSF and edema; and free water correction can map this at the voxel level while also providing voxel-wise estimates of traditional DTI variables (e.g., FA) corrected for extracellular free water. By eliminating the contribution of edema and partial-volume effects to the measured DTI signal, these corrected DTI variables provide more specific estimates of axonal/white matter pathology. 8
A major challenge with DTI and other quantitative neuroimaging modalities is that there are few robust measures for summarizing abnormalities occurring with variable spatial distribution across the brain. This is of particular concern for brain disorders characterized by pathologically heterogenous abnormalities such as TBI. To facilitate data reduction, voxel-wise estimates are typically averaged across neuroanatomically meaningful regions of the brain (regions of interest [ROIs]) that correspond to named anatomical structures [e.g., white matter tracts, cortical gyri and sulci, subcortical nuclei]). This approach generates hundreds of variables that provide little useful information when analyzed with univariate statistics where values are averaged across a cohort of patients with heterogenous brain pathology. One potential solution to this problem is to generate a single composite measure summarizing imaging abnormalities across the entire brain using the Mahalanobis distance, a multi-variate generalization of the z-score. 9 This approach was originally proposed as a method for describing deviation from normal structural connectivity in mild TBI. 9
Emerging evidence indicates that elevated whole brain white matter free water content is associated with cognitive performance and may represent a promising biomarker in TBI. In a study of cognitively diverse individuals (without TBI), free water volume fraction (VF) correlated with episodic memory and executive function. 10 In a recent study by our group, we validated a Mahalanobis distance-based summary score of free water VF as a measure of injury severity in moderate-to-severe TBI. 11 This measure was associated with worse long-term executive functioning and processing speed. In this study, we extend our prior work and apply the Mahalanobis distance-based summary score of free water VF to a cohort of patients with primarily complicated mild TBI to investigate the hypothesis that free VF abnormalities are present in TBI across the injury severity spectrum. The main objective of this study was to assess the utility of a summary score based on the Mahalanobis distance to describe anomalies in white matter microstructure and explore its correlation with neuropsychological functioning in an independent cohort of patients with primarily complicated mild TBI.
Methods
Participants
In this single-center observational study, we recruited adult (age 18 or older) patients with non-penetrating TBI who required hospitalization post-injury. Patients were enrolled at the time of hospital admission. Patients were excluded for a history of pre-existing serious neurological or psychiatric disorder, comorbid disabling condition limiting outcome assessment, current pregnancy, if they were incarcerated, had low MRI image quality, or were under the age of 18. Patients with focal intraparenchymal lesions exceeding 50 cm3 were also excluded. 11,12 Patients underwent brain MRI at 2 weeks and 6 months post-injury. We also enrolled healthy control subjects recruited from the general population via local advertisement with no history of TBI, pre-existing disabling neurological or psychiatric disorder, or current pregnancy.
Healthy controls underwent a single brain MRI. Demographic information, medical history, admission injury characteristics, and other clinical information were collected from the medical record. This study was approved by the Institutional Review Board at the University of Pennsylvania.
Neuropsychological assessment
Patients underwent neuropsychological assessment by trained research personnel, who were blind to imaging findings. Assessments were performed on the same day as the MRI at approximately 2 weeks and 6 months post-injury. Neuropsychological function was assessed across three domains: processing speed assessed with the Processing Speed Index from the Wechsler Adult Intelligence Scale IV 13 ; verbal learning by Rey Auditory Verbal Learning Test (RAVLT) 14 ; and executive functioning by the Trail Making Test-Parts A and B. 15 The assessment of neuropsychological outcome mirrored those of the Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study.
Image acquisition
Brain MRIs were performed on a 3 Tesla scanner (Siemens Prisma) using a product 32-channel head coil. Structural imaging included a sagittal T1-weighted magnetization-prepared 180 degrees radio-frequency pulses and rapid gradient-echo (repetition time [TR] = 2.3 sec, echo time [TE] = 2.94 msec, inversion time [TI] = 900 msec, FA = 9°, resolution = 1 × 1 × 1 mm). Whole brain diffusion MRI (dMRI) was performed with an echo planar sequence with FA 90° and resolution = 2.4 × 2.4 × 2.4 mm (b-value = 1000 sec/mm2, 64 diffusion directions, TR 2.9 sec, TE 94 msec). Separately, 14 images with b-value = 0 sec/mm2 with reverse phase encoding were acquired.
Image processing
Structural MRI and dMRI data were visually inspected for artifacts before preprocessing. T1-weighted images were bias corrected using the N4BiasCorrection tool from ANTs, 16 followed by brain extraction using a multi-atlas segmentation tool, MUSE. 17 Diffusion MRI data was preprocessed in three steps. First, local-PCA denoising 18 as implemented in MATLAB 2021a (MathWorks, Natick, MA); followed by motion and distortion correction using the topup and eddy tools in FSL 19 ; then, bias field correction using N4BiasCorrection from ANTs. A tensor model 4 was fit to the data in DIPY. 20 We used FERNET (Freewater EstimatoR using iNtErpolated iniTialization), 8 a recent method for free water correction in clinically acquired DTI data, to estimate the free water-volume fraction or VF and free water-corrected FA (fw-FA). FERNET has been validated using simulated data, healthy control data, and clinical data from patients with TBI and brain tumors. 8,11 Using the deformable SyN registration algorithm from ANTs, 21 the data were registered to the JHU-MNI-ss (Eve) template. 22 Two example cases are shown in Figure 1. Mean values of VF and fw-FA were calculated in 90 ROIs of the Eve white matter parcellation. Fornix and tapetum were excluded because of their small size and proximity to the ventricles. For each of the 90 ROIs, we then regressed out age from the mean value of VF and fw-FA in each ROI using the following method: Using linear regression we fit a model using only observations from controls with age as the independent variable and the mean of the respective DTI variable (e.g., VF) as the dependent variable. Age was then regressed out for both patients and controls using the residuals (Xr i) from the above regression.

Representative cases (
Patient-specific summary anomaly score of white matter microstructure
We next derived a patient-specific summary anomaly score (SAS). SAS is an age-corrected measure of whole brain white matter microstructural anomaly referenced to a cohort of healthy controls. SAS was derived separately for VF and fw-FA for each control (from our cohort) and at each time-point for each patient using the Mahalanobis distance, a multi-variate generalization of the z-score:
where s = [Xr 1, Xr 2… Xr 90] is a 90x1 vector containing the residuals of the age-regressed DTI variable (Xr i) for each ROI for the participant; μ is a 90x1 vector of mean Xr of each ROI in the healthy controls; and C is the covariance matrix between ROIs across the control population. Thus, for each patient and control we calculated M, the Mahalanobis distance-based SAS for each dMRI measure: VF and fw-FA. This is a validated method for describing whole brain abnormalities in TBI and is described in more detail elsewhere. 9,11
Calculation of Mahalanobis distance requires that the number of reference observations (i.e., control subjects) exceed the number of variables (i.e., ROIs). Since the number of ROIs in the Eve white matter parcellation (90) is larger than the number of controls in our cohort (36), we additionally used DTI data from 77 control subjects enrolled in the TRACK-TBI study [mean age (standard deviation) of 39 (15.0); 51 men (66%)] to increase the size of the reference cohort used for calculation of SAS to 113. The TRACK-TBI controls were used only as a reference for calculation of SAS for patients and controls enrolled at our center and we did not calculate SAS for participants from TRACK-TBI nor conduct any subsequent analyses using their data. To mitigate potential confounds from use of multi-site data, dMRI data from TRACK-TBI were harmonized with our cohort using ComBat, 23 a batch effect removal technique that removes acquisition and processing differences while retaining the effects of biology (e.g., age, sex, group). To assess the effectiveness of ComBat, we fit linear mixed effects models separately using unharmonized (pre-ComBat) and harmonized (post-ComBat) DTI data. We modeled the mean DTI measurement (VF and fw-FA separately in different models) in each ROI as the dependent variable with fixed effects for study site, age, sex, and group (i.e., TBI vs. control) with a random intercept for participant. We compared this model to one without a term for site effects and assessed its significance by calculating the F-statistic. Further details on the comparison between pre- and post-ComBat harmonized DTI variables are presented in Supplementary Figure S1.
Statistical analysis
Data was assessed visually and via the Kolmogorov-Smirnov test for normality. As SAS was not normally distributed, we utilized the nonparametric Mann Whitney U test for comparisons between patients and controls and the Wilcoxon signed rank test was used for comparison of SAS from 2 weeks to 6 months post-injury. Chi-squared or Fisher's exact test were used for categorical data where appropriate. We assessed the relationship between neuropsychological functioning and SAS using Spearman's rank correlation. Our primary hypothesis was that 2-week SAS is associated with 6-month neuropsychological outcomes. Significance for these comparisons was set at p = 0.01 (0.05/5) after Bonferroni correction for five comparisons. Our secondary hypothesis was that SAS correlated with neuropsychological outcomes, cross-sectionally. These results are presented without correction for multiple comparisons (i.e., p < 0.05 is considered statistically significant). We repeated the above analyses including only patients with mild TBI (i.e., Glasgow Coma Scale [GCS] score 13-15) to ensure that findings were not driven by patients with more severe injury (i.e., those with moderate or severe TBI). To determine if results were robust to outliers, we fit robust linear models using bisquare regression. All analyses were carried out using MATLAB 2022a (MathWorks, Natick, MA).
Results
Demographic and clinical information
We enrolled 65 patients and 36 controls. Two patients were excluded due to low MRI quality or artifact. Four patients with focal intraparenchymal lesions exceeding 50 cm3 were excluded (Fig. 2). Demographic and clinical information for the cohort is presented in Table 1. Injury severity according to GCS category was predominantly mild (90%); Two patients had moderate and two had severe TBI. An acute intracranial lesion was visible on computed tomography (CT) in 71% of patients. Forty-one (71%) participants had an admission GCS of 13-15 and an acute post-traumatic lesion on CT hence the cohort primarily consisted of participants with complicated mild TBI.
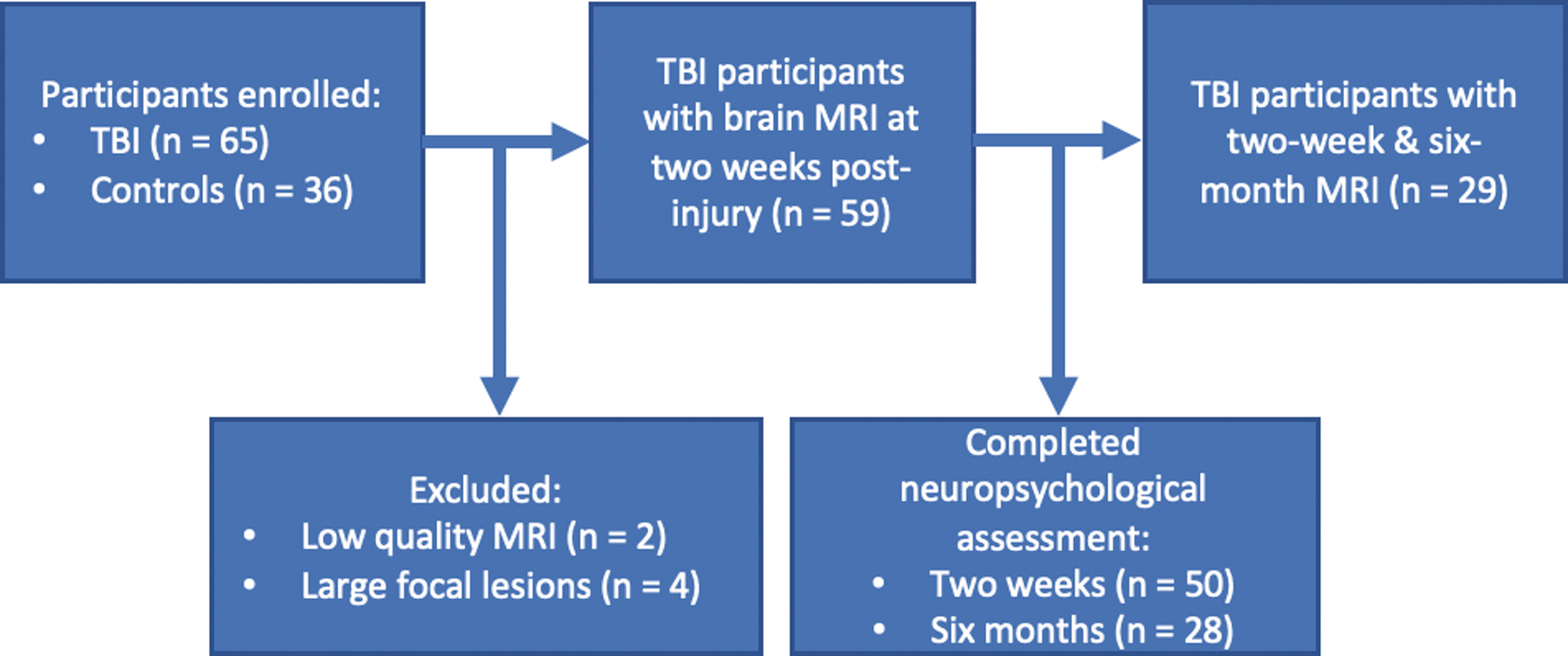
Consort diagram showing participant enrollment and follow-up.
Participant Characteristics
TBI, traumatic brain injury; IQR, interquartile range; GED, General Educational Development; GCS, Glasgow Coma Scales; CT, computed tomography.
Summary specific anomaly score at 2 weeks and 6 months post-injury
Fifty-nine patients underwent brain MRI 2 weeks post-injury (median 17 days post-injury; interquartile range [IQR] 8-27 days), of which 29 had a follow up scan at 6 months post-injury (median 195 days post-injury; IQR 170-220 days). Participants with 2-week only imaging were overall similar in terms of demographics and outcomes to those with imaging at both 2-weeks and 6 months (Supplementary Table S1). Figure 3 shows the summary specific anomaly score (SAS) for controls and patients at 2 weeks and 6 months post-injury for VF and fw-FA, respectively. SAS was significantly higher in TBI patients at 2 weeks relative to controls for VF (p < 0.001), but not fw-FA (p = 0.09). Similarly, SAS was significantly higher in TBI patients at 6 months post-injury period relative to controls for VF (p < 0.001), but not fw-FA (p = 0.5). We then fit a linear regression model to assess for effects of time from injury to scan acquisition on SAS. Time to scan acquisition was not associated with VF or fw-FA SAS (Supplementary Table S2). Among TBI patients, SAS remained stable at a group level from 2 weeks to 6 months for both VF and fw-FA. Sensitivity analyses performed among patients with GCS from 13-15 showed similar results (excluding four patients with moderate or severe TBI).
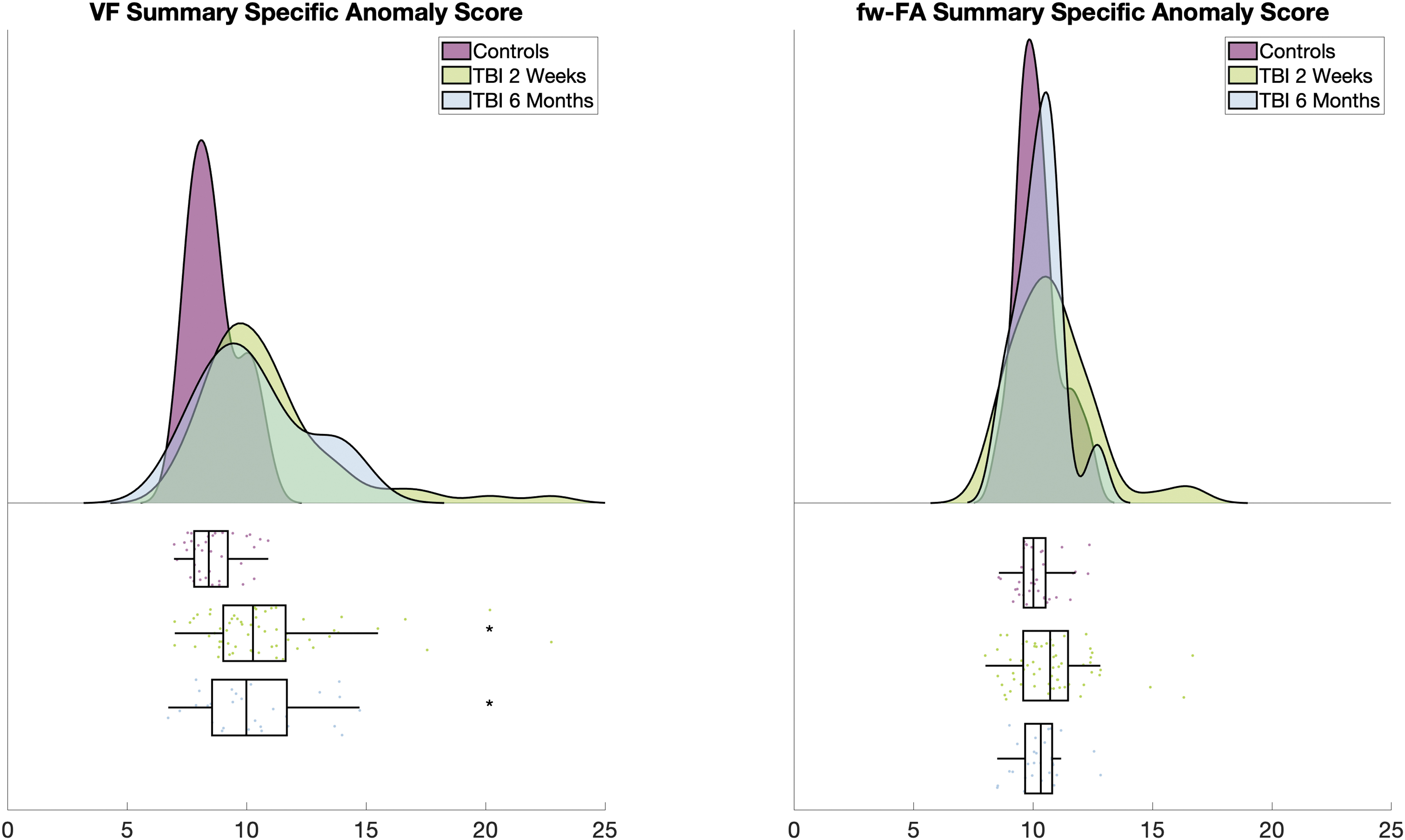
Raincloud plot showing summary specific anomaly score (SAS) for volume fraction (VF) and free water-corrected fractional anisotropy (fw-FA) for TBI patients and controls. Higher SAS indicates more white matter abnormalities. *p < 0.001 for comparison between SAS VF 2 weeks post-injury period relative to controls; p < 0.001 for comparison between SAS VF in the chronic post-injury period relative to controls.
Relationship between summary specific anomaly score and neuropsychological functioning
Fifty and 28 participants had neuropsychological assessment available for analysis at 2 weeks and 6 months, respectively (Fig. 2). Results of the correlation between 2-week SAS and 6-month neuropsychological function are presented in Figure 4. Two-week VF SAS correlated moderately with 6-month Trail Making Test-Part B (TMT-B; rho = 0.3; p = 0.048) and immediate memory (rho = 0.3; p = 0.036), but these results were not considered statistically significant after Bonferroni correction. Two-week fw-FA SAS correlated weakly with neuropsychological status at 6 months (results not significant). Results of the cross-sectional correlation between SAS and neuropsychological function are presented in Supplementary Figures S2 and S3. Two-week VF SAS correlated significantly with 2-week processing speed index (rho = 0.35; p = 0.006), TMT-A (rho = 0.26; p = 0.04), and TMT-B (rho = 0.41; p = 0.001). Six-month VF SAS correlated with 6-month TMT-B (rho = 0.3; p = 0.4) and immediate memory (rho = 0.4; p = 0.02). Two-week fw-FA SAS correlated with TMT-B at 2 weeks post-injury (rho = 0.4, p = 0.003). Sensitivity analyses including only patients with GCS from 13-15 showed similar results.
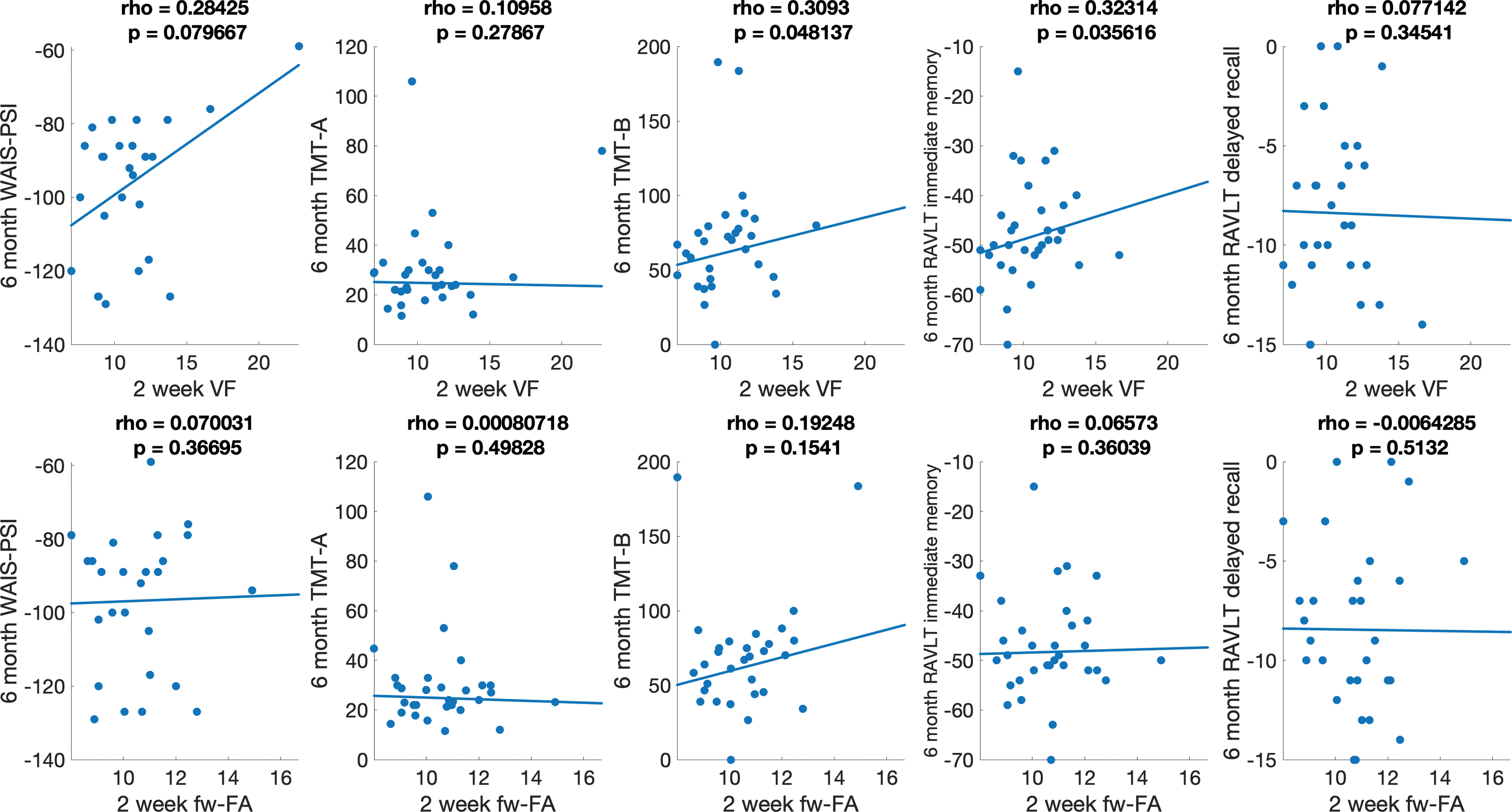
Association between 2-week summary specific anomaly scores (SAS) for diffusion tensor imaging (DTI) and 6-month neuropsychological function. Positive values for rho indicate a positive correlation between burden of DTI abnormalities and worse neuropsychological function. WAIS-PSI and RAVLT scores were multiplied by -1 so the direction of associations would be consistent across each of the five neuropsychological assessments. p < 0.01 is considered statistically significant after Bonferroni correction for five comparisons per DTI measure. Line of best fit was estimated using bisquare regression robust to outliers. WAIS-PSI, Processing Speed Index from the Wechsler Adult Intelligence Scale IV; RAVLT, verbal learning by Rey Auditory Verbal Learning Test (sub-scores for immediate memory and delayed recall); TMT-A, Trail Making Test-Part A; TMT-B, Trail Making Test-Part B.
Discussion
The main findings of this study are that a multi-variate summary score describing abnormalities in VF distinguishes patients with primarily complicated mild TBI from healthy controls both at 2 weeks and 6 months post-injury and that VF exhibits moderate correlation with neuropsychological functioning. Group differences and correlation with neuropsychological functioning are more robust than those for fw-FA, a measure thought to reflect traumatic axonal injury.
TBI is heterogenous with respect to injury location as well as pathophysiology with contributions from axonal injury, vascular injury, and inflammation. Together, free water VF and fw-FA may be used for multi-variate biophysical modeling of these dynamic processes. Free water VF abnormalities may represent edema/inflammation or brain atrophy in this context whereas fw-FA may model the alterations in axonal coherence reflective of axonal injury. Understanding the burden of these abnormalities across the entire brain is important given the anatomic heterogeneity of TBI. Our results build upon prior studies of free water correction in patients with mild TBI. Palacios and colleagues 24 found increases in free water in a cohort of mild TBI using another biophysical model of water diffusion known as neurite orientation dispersion and density imaging. However, in this study free water decreased from the subacute to chronic post-injury period. Conversely, Pasternak and colleagues 25 found decreased free water from pre- to post-season in a cohort of subjects with sports-related concussion. Such differences may be explained by use of different biophysical models, different levels of injury severity, and different form of analysis (both studies used voxel-wise analyses). The results of this study are consistent with a prior study from our group on a cohort of patients with moderate-to-severe TBI. In our prior study, we found larger group differences (participants with TBI vs. controls) for VF compared with fw-FA and FA from a standard single tensor model. This is in line with results of the current study where the cohort consisted of patients with primarily complicated mild TBI. Thus, we demonstrate that across the TBI severity spectrum, abnormalities in VF are more prominent than (fw-)FA, which is traditionally considered a manifestation of traumatic axonal injury. Outside of TBI, free water imaging has been used to probe abnormal increase in free water in schizophrenia, 26 Parkinson's disease, 27,28 and dementia. 10,29
We found larger group differences for VF than for fw-FA (Fig. 3). Given that VF models extracellular water diffusion and fw-FA models diffusion along the main axis after free water correction, 8 this suggests that the burden of axonal injury (as modeled by fw-FA) in this cohort is less severe (and statistically similar to controls) than the burden of extracellular VF abnormalities. These findings are in agreement with our previous study of free water VF in moderate-to-severe TBI. 11 It should be noted that the underlying biological perturbations driving these changes cannot be resolved with this neuroimaging modality. Based on pathologic data in TBI indicating chronic white matter degeneration and inflammation after TBI 30 we hypothesize that increases in free water in TBI may represent either inflammation/edema or atrophy. Ex vivo correlation with histopathology or concurrent acquisition of molecular imaging using positron emission tomography tracers that quantify microglial activation 31 are needed to confirm this hypothesis.
The summary specific anomaly score for VF showed moderate correlations with neurocognitive function, particularly for measures of executive function. This is in line with previous studies. In our prior study in patients with moderate and severe TBI, multi-variate abnormalities in VF correlated with measures of executive function and processing speed, but not verbal learning. 11 In a large cohort of cognitively diverse elderly participants (without TBI), a whole brain white matter measure of free water VF was associated with low baseline episodic memory and executive function. Further, higher VF was associated accelerating decline in executive function and memory. 10 Although 2-week VF correlated with executive function and immediate memory at 6 months, the significance of these findings did not survive multiple comparisons correction. Neuropsychological outcomes after TBI are strongly correlated with pre-injury factors such as education, socioeconomic status, and psychological health, which are not directly related to the biology of the injury. 32 -34 Therefore, the lack of substantial correlation between SAS and neuropsychological function is an expected finding. Future studies in larger cohorts, such as TRACK-TBI, will evaluate the utility of VF SAS measured in the acute or subacute post-injury period as a predictive biomarker of long-term cognitive outcomes.
This study has several limitations. First, the size of the cohort is relatively small, particularly at the chronic post-injury time-point. Given the heterogeneity of brain pathology and recovery trajectory in TBI these findings require validation in larger cohorts such as TRACK-TBI. Second, we did not consider the effect of lesions on the SAS. Consistent with prior studies, 11,12 we excluded patients with large focal intraparenchymal lesions, but cannot resolve the effects that smaller lesions may have on SAS. We plan to address this issue in a future study using a lesion segmentation algorithm. Third, as mentioned above, free water is a biophysical model of voxel-wise water diffusion and is not specific to the underlying brain pathology.
Conclusion
In this cohort of patients with primarily complicated mild TBI, we extend our prior work to show that abnormalities in white matter extracellular free water VF are present in patients with TBI across the injury severity spectrum. Abnormalities in free water VF are more severe than those thought to reflect traumatic axonal injury (i.e., fw-FA) and VF exhibits stronger correlation with neuropsychological functioning than fw-FA. These findings are an important step towards identifying quantitative neuroimaging biomarkers that can be used in precision medicine clinical trials for risk-stratification in TBI.
Transparency, Rigor, and Reproducibility
This study and its analytic plan were not formally pre-registered in a repository. Due to the exploratory nature of the study, a priori power analysis was not performed. The number of participants enrolled, results of image quality assessment, and number of participants with clinical outcome data is presented in the article. Participants were told the results of their imaging, when applicable, after completion of clinical outcome assessment. Details of imaging data acquisition are presented in the article. Imaging data for the analytic cohort was acquired on a single scanner. Details of pre-processing and quality control evaluation are provided in the article. The key inclusion criteria for enrollment in the study and the primary clinical outcome measures are established standards in the field. Statistical tests did not assume a normal distribution. Effects sizes are not reported in the article given the non-Gaussian distribution of the independent variable. We addressed the issue of multiple comparisons using techniques for dimensionality reduction (i.e., Mahalanobis distance) and for the primary outcome, Bonferroni correction. Efforts at external validation in a large cohort are ongoing. The primary data for this study will be available upon request to the corresponding author. The analytic code is available at GitHub.
Acknowledgments
The authors would like to thank Katya Rascovsky, PhD, for her advice on analysis of neuropsychological measures. An earlier draft of this article was originally posted as a preprint at arXiv.org.
Footnotes
Authors' Contributions
Dr. Gugger: Formal analysis, methodology, writing original draft, writing—review and editing
Dr. Walter: Data curation, project administration, writing—review and editing
Mr. Parker: Data curation, project administration, software
Dr. Sinha: Formal analysis, writing—review and editing
Mr. Morrison: Data curation, writing—review and editing
Dr. Petrov: Resources, writing—review and editing
Dr. Ware: Writing—review and editing, data curation
Dr. Schneider: Writing—review and editing, project administration
Dr. Sandsmark: Writing—review and editing, project administration
Dr. Verma: Conceptualization, methodology, supervision, writing—review and editing
Dr. Diaz-Arrastia: Conceptualization, funding acquisition, project administration, supervision, writing—review and editing
Funding Information
Work in the authors' laboratory was supported by the Pennsylvania Department of Health. This work was also funded by NINDS T32NS091006, U01NS086090, U01NS114140, DoD W81XWH-12-2-0139, W81XWH-14-2-0176, W81XWH-19-2-0002 and the American Epilepsy Society/Citizens United for Research in Epilepsy (Research and Training Fellowship for Clinicians).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.