
Abstract
Spinal cord injury (SCI) frequently results in motor, sensory, and autonomic dysfunction for which there is currently no cure. Recent pre-clinical and clinical research has led to promising advances in treatment; however, therapeutics indicating promise in rodents have not translated successfully in human trials, likely due, in part, to gross anatomical and physiological differences between the species. Therefore, large animal models of SCI may facilitate the study of secondary injury processes that are influenced by scale, and may assist the translation of potential therapeutic interventions. The aim of this study was to characterize two severities of thoracic contusion SCI in female domestic pigs, measuring motor function and spinal cord lesion characteristics, over 2 weeks post-SCI. A custom-instrumented weight-drop injury device was used to release a 50 g impactor from 10 cm (n = 3) or 20 cm (n = 7) onto the exposed dura, to induce a contusion at the T10 thoracic spinal level. Hind limb motor function was assessed at 8 and 13 days post-SCI using a 10-point scale. Volume and extent of lesion-associated signal hyperintensity in T2-weighted magnetic resonance (MR) images were assessed at 3, 7, and 14 days post-injury. Animals were transcardially perfused at 14 days post-SCI and spinal cord tissue was harvested for histological analysis. Bowel function was retained in all animals and transient urinary retention occurred in one animal after catheter removal. All animals displayed hind limb motor deficits. Animals in the 10-cm group demonstrated some stepping and weight-bearing and scored a median 2–3 points higher on the 10-point motor function scale at 8 and 13 days post-SCI, than did the 20-cm group. Histological lesion volume was 20% greater, and 30% less white matter was spared, in the 20-cm group than in the 10-cm group. The MR signal hyperintensity in the 20-cm injury group had a median cranial-caudal extent approximately 1.5 times greater than the 10-cm injury group at all three time-points, and median volumes 1.8, 2.5, and 4.5 times greater at day 3, 7, and 14 post-injury, respectively. Regional differences in axonal injury were observed between groups, with amyloid precursor protein immunoreactivity greatest in the 20-cm group in spinal cord sections adjacent to the injury epicenter. This study demonstrated graded injuries in a domestic pig strain, with outcome measures comparable to miniature pig models of contusion SCI. The model provides a vehicle for the study of SCI and potential treatments, particularly where miniature pig strains are not available and/or where small animal models are not appropriate for the research question.
Introduction
Traumatic spinal cord injury (SCI) often results in devastating neurological impairment. Despite numerous clinical trials, 1 only limited surgical and therapeutic treatment pathways exist for SCI, 2 leaving individuals with permanent motor, sensory, and autonomic dysfunction. Pre-clinical research efforts have contributed to the understanding of the mechanisms underlying the primary and secondary tissue damage associated with SCI; however, much still remains unknown.
Pre-clinical SCI research has primarily been dominated by rodent models 3 ; however, treatments developed in these models have shown little success when trialed in humans. 2 This is likely due, in part, to the various anatomical and pathophysiological differences that exist between these species. 4,5 As such, it has been proposed that intermediary, large-animal models of SCI may help to improve clinical translation of proposed treatments. 6,7 Non-human primates, 6,8 –17 sheep, 18 –20 dogs, 21 –25 cats, 26,27 and goats 28 have all been used for SCI research, with contemporary studies mainly using pigs. 29 –44 Spinal cord and dura dimensions, 45 vertebral column size and shape, 46 and blood flow characteristics 47 of pigs are similar to those of humans, suggesting that pigs are a suitable option to study the physiological response to injury, and to explore potential treatments. The majority of pig contusion SCI studies use miniature strains 30 –32,35,39 –42 because they are of more manageable size and mass than domestic pigs at skeletal maturity. However, miniature breeds are not available universally, and can be cost prohibitive, hence domestic pig models using a variety of injury mechanisms are also being developed. 29,34,37,43,44,48,49
To date, histological lesion volume, gray and white matter changes, and motor function at various time-points up to 1 year post-injury have been described for pig SCI models. However, there are few reports of pig models incorporating in vivo magnetic resonance imaging (MRI) following SCI, 30,34,39 –42,48,50,51 despite this being a primary clinical tool. Some non-human primate studies have performed MRI in the days to weeks following injury, 6,10,11 but in pig models of contusion SCI, MR imaging has only been reported up to 2 h post-injury 34,40,50 or for ex vivo tissue evaluation. 39,41,48,50,52 The morphology and MR signal changes occurring in the subacute injury phase in pigs are not well understood, and may be useful in this large-animal model where histological analysis at multiple experimental end-points may not be feasible.
The aim of this study was to develop a thoracic contusion SCI model in domestic pigs using a custom-instrumented weight-drop injury device, and to characterize the effect of two weight-drop heights on hind limb motor function, MR signal changes, and histological lesion characteristics, over 2 weeks post-injury.
Methods
All animal protocols in this study were approved by the South Australian Health and Medical Research Institute Animal Ethics Committee (SAM243) and performed according to the requirements of the National Health and Medical Research Council Australian Code for the Care and Use of Animals for Scientific Purposes (8th edition, 2013). 53 Pigs were acclimatized to the facility and human contact for at least 1 week prior to the first procedure. Pigs were housed indoors in raised pens (except immediately after SCI; see below), with at least one companion housed in the same room throughout, and were provided enrichment toys, access to water, and twice-daily food rations (500 g, Pig Finisher; Lauke Mills, South Australia). Pigs received prophylactic antibiotics from arrival at the facility until the first surgery (TrimidineTM 0.15 g/10 kg bodyweight; sulfadimidine 430 mg/g, trimethoprim 86 mg/g).
Animal preparation and general care
Ten female domestic pigs (Large White cross Landrace, 26–34 kg at SCI; Roseworthy Piggery, South Australia) were randomly assigned to receive a graded SCI of a nominal “low” (n = 3) or “high” (n = 7) rating; group sizes were allocated a priori. For all procedures requiring anesthesia, animals were administered pre-medication of medetomidine (0.02–0.04 mg/kg), followed by induction with ketamine (11 mg/kg) and propofol (2 mg/kg). Anesthesia was maintained with continuous intravenous infusion of ketamine (7.0–8.0 mg/kg/h), propofol (3.5–4.5 mg/kg/h), midazolam (0.1–0.2 mg/kg/h), and fentanyl (6.0–8.0 μg/kg/h). Animals were intubated via endotracheal tube and ventilated at 17–19 breaths/min, with a tidal volume of 270–400 mL/min. Intra-operative heart rate, blood pressure, oxygen saturation, end tidal CO2, and body temperature were monitored. All surgical procedures were completed under sterile conditions.
Transdermal fentanyl patches (slow release, 50–75 μg/h) were administered approximately 12 h prior to the first surgical procedure because they have a delayed onset of action. The patches were replaced every 3 days (they have approximately 72 h of action) until 3 days post-injury. Antibiotics (Clavulox: 12.5–20 mg/kg of 140 mg/mL amoxicillin) were administered intra-operatively and daily post-operatively. A urinary catheter was placed for SCI surgery, and it remained in place for 3–4 days.
Catheter surgeries
Prior to SCI induction, all animals underwent surgical procedures on day −5 and −3 under anesthesia, as described above. The first procedure (day −5) involved placing custom catheters (60 cm long × 2.5 mm outer diameter [OD] × 1.5 mm inner diameter [ID] polyethylene [PE] tubing) into the left carotid artery and the left external jugular vein (approximately 10 cm in length in vessel). These facilitated invasive arterial blood pressure monitoring, venous blood sampling, and intravenous drug administration, and were flushed twice daily with 5–10 mL of saline and 2–5 mL of heparinized saline (5 IU/mL) until humane killing. The second procedure (day −3) involved placing custom catheters (25 cm long × 1.9 mm OD × 1.4 mm ID PE tubing) in the intrathecal space (approximately 2 cm in length intrathecal), at spinal levels T7 and L1/2 via a <1 cm in diameter laminectomy for intrathecal pressure monitoring, the results of which are not reported here.
Spinal cord injury
Under anesthesia, the animal was placed in a prone position, and C-arm fluoroscopy (Veradius; Philips, Netherlands) was used to confirm the location of spinal level T10. After surgical preparation, a dorsal midline incision was made between T9 and T13, and the spinous processes were exposed via periosteal stripping of the paraspinal muscles, then removed. Electrocautery was used to achieve soft-tissue hemostasis as required. A laminectomy centered on T10 (3 cm × 1.2 cm) was performed using a surgical burr (Midas Rex Legend V02; Medtronic, Minneapolis, MN, USA) and Kerrison rongeurs to expose the spinal cord and dura. Hemostasis was achieved by applying bone wax (W31G; Ethicon, NJ, USA) to any exposed trabecular bone. Polyaxial pedicle screws (3.5 mm diameter × 28 mm long; Vertex System, Medtronic) and titanium rods (3 mm diameter × 40 mm long) were inserted bilaterally at T12 and T13 to secure the base of a custom-instrumented weight-drop injury device. The injury apparatus is similar in design to that described by Streijger and colleagues. 52 In brief, the device comprised a 50 g impactor (9.5 mm diameter circular tip with beveled edge) that interfaced with a linear rail aligned vertically, such that the impactor was centered over the laminectomy.
Immediately prior to injury induction, the location of the dorsal dura was recorded with a magnetic linear position sensor attached to the rail (described below) while manually suspending the impactor tip on the dura surface. To induce SCI, ventilation was paused briefly to eliminate respiratory motion and a solenoid was actuated to release the impactor onto the exposed dura, from a height of either 10 or 20 cm. Ventilation was resumed immediately and an additional 100 g weight was added for 5 min. The weight-drop apparatus and pedicle screws were then removed, a vacuum wound drain (Mini-Redon 50; Primed, Germany) was applied, the tube was tunneled subcutaneously, and the bottle was placed in a pouch sutured to the back (a drain was not placed in the first two animals, both in the 20-cm group). The wound was closed in layers (Vicryl size 0 suture; Ethicon). Local anesthetic was administered at the surgical site (Marcain 0.5% bupivacaine).
Injury apparatus data were collected at a sampling rate of 50 kHz and included: impact force via a load cell mounted between the impactor tip and body (LLB215-25LB, FSH02623; Futek, Irvine, CA, USA; range: 111 N compression, non-linearity/hysteresis 0.56 N), and impactor displacement via a magnetic linear position sensor (BTL6-G500-M0102-PF-S115, non-linearity ±200 μm, accuracy ±5 μm; Balluff, Neuhausen, Germany) attached to the rail; high-speed video (iSpeed TR; Olympus/iX Cameras, UK) was recorded simultaneously at 5000 Hz. A custom control box interfaced with a data acquisition system (cDAQ9174 chassis with NI9401 and NI9215; National Instruments, Austin, TX, USA) was used to control the injury device and acquire synchronized data. These data were post-processed to determine velocity immediately prior to contact with the dura, and the peak impact force, impulse, and peak dura/cord displacement during the impact event.
Post-injury care
For 3–4 days following SCI, pigs were individually housed in recovery beds and provided continuous 24-h care. Animals were administered meloxicam (0.4 mg/kg) daily for up to 3 days and Temgesic (0.005–0.01 mg/kg buprenorphine) as required. Water and regular food rations were offered by hand while the pigs had limited mobility. Fruit and cordial (sugary fruit-flavored concentrate diluted with water) were also offered during recovery to encourage hydration and caloric intake. Oxygen saturation was monitored via a pulse oximeter on the tail and oxygen was supplied by nose cone when saturation was not maintained above 90%. Body temperature was often elevated in the first 24 h; if >39.5°C, fans and cold towels were applied. Heart rate, urine output, and defecation were monitored. The wound drain bottle was emptied as needed and the drain was removed 3 days post-operatively.
Incision sites were regularly checked for any signs of infection. Skin was cleaned and barrier cream was applied to any pressure sores or abrasions resulting from sitting or dragging the rump and hind limbs around the pen. The urinary catheter was removed at 3–4 days post-injury when animals returned to their pre-injury pen (1.1 m × 1.6 m). Trays extending the length and width of the raised pens were placed under the pen-grating floor so urination could be monitored. If urination was not witnessed, no urine was evident overnight following catheter removal, or animals showed signs of discomfort or abdominal distension, manual bladder expression was undertaken until normal urination resumed.
Ultrasound
Intra-operative mid-sagittal and axial ultrasound videos were obtained pre- and post-injury at T10 using a handheld linear array probe (L14-5/38, Ultrasonix RP; Ultrasonix Medical Co., Richmond, BC, Canada), with the following settings: frequency 14 MHz, gain 55%, dynamic range 65 dB, depth 3 cm, field of view 100%, image resolution 0.063 mm/pixel. The pre-injury axial videos were split into individual frames using MATLAB software (R2021a; MathWorks, Massachusetts, USA). An image was selected at the point in the dura pulsation cycle with the greatest dorsal-ventral intrathecal diameter. This was measured between the centers of the hyperechoic bands of dural tissue using the line tool in FIJI (ImageJ software, version 2.1). The dorso-ventral spinal cord diameter was measured in the same way (Fig. 1A,B).

Intrathecal and spinal cord dorsal-ventral diameter measurements were taken from axial pre-injury ultrasound
Motor function assessment
Prior to surgery, animals undertook six to nine training sessions until they were able to successfully complete the Porcine Thoracic Injury Behavior Scale (PTIBS) 35 motor function assessment task. For up to 1 h daily, pigs were clicker trained to traverse a runway (1.2 m wide × 5.0 m long × 4.5 mm thick, 2-ply insertion rubber; Clark Rubber, Australia) following a target and rewarded with a small amount of their usual food ration. Baseline locomotor ability was videotaped with cameras (HERO5 Black; GoPro, California, USA) positioned such that the rump and hind limbs were visible. On days 8 and 13 post-injury, when the animals were not undergoing any procedures requiring anesthesia, they were recorded completing the task at least 5 times. The animal was placed in the “index” position, with hind limbs extended behind them, at the start of each trial (Supplementary Fig. S1). The camera views were synchronized using video editing software (ShotCut; MeltyTech, LLC) and motor function was scored 35 separately by two researchers who were blinded to the injury groups. Any differences in scoring were resolved by consensus.
Magnetic resonance imaging
MR images were obtained 5 days pre-injury, and 3, 7, and 14 days post-injury using a Magnetom Skyra (3T; Siemens, Germany). The anaesthetized animal was placed in the left lateral decubitus position with two Body 18 coils (Siemens) wrapped around the dorsal torso and neck. A three-dimensional (3D) T2-weighted fast spin-echo (FSE) Sampling Perfection with Application optimized Contrasts using different flip-angle Evolution (SPACE) scan was obtained (repetition time 1500 msec, echo time 136 msec, 2 averages, 110-degree flip angle, 384 × 384 acquisition matrix, voxel resolution 0.8125 mm isotropic, 9-min scan duration).
On the pre-injury images, intrathecal and spinal cord dorso-ventral diameters were measured on a single axial slice near the center of spinal level T10 using medical image processing software (MIMICS, version 22.0.0.524; Materialise NV, Belgium; Fig. 1C,D) for comparison with the equivalent ultrasound measurements. The volume of the region of hyperintense signal at the SCI site was calculated from 3D models, which were created by manual segmentation and smoothing, using the MIMICS software (version 22.0.0.524; Materialise NV). The lesion rostro-caudal extent was measured between the most cranial and caudal margins of the model at the mid-sagittal slice exhibiting the greatest lesion length (Fig. 2).
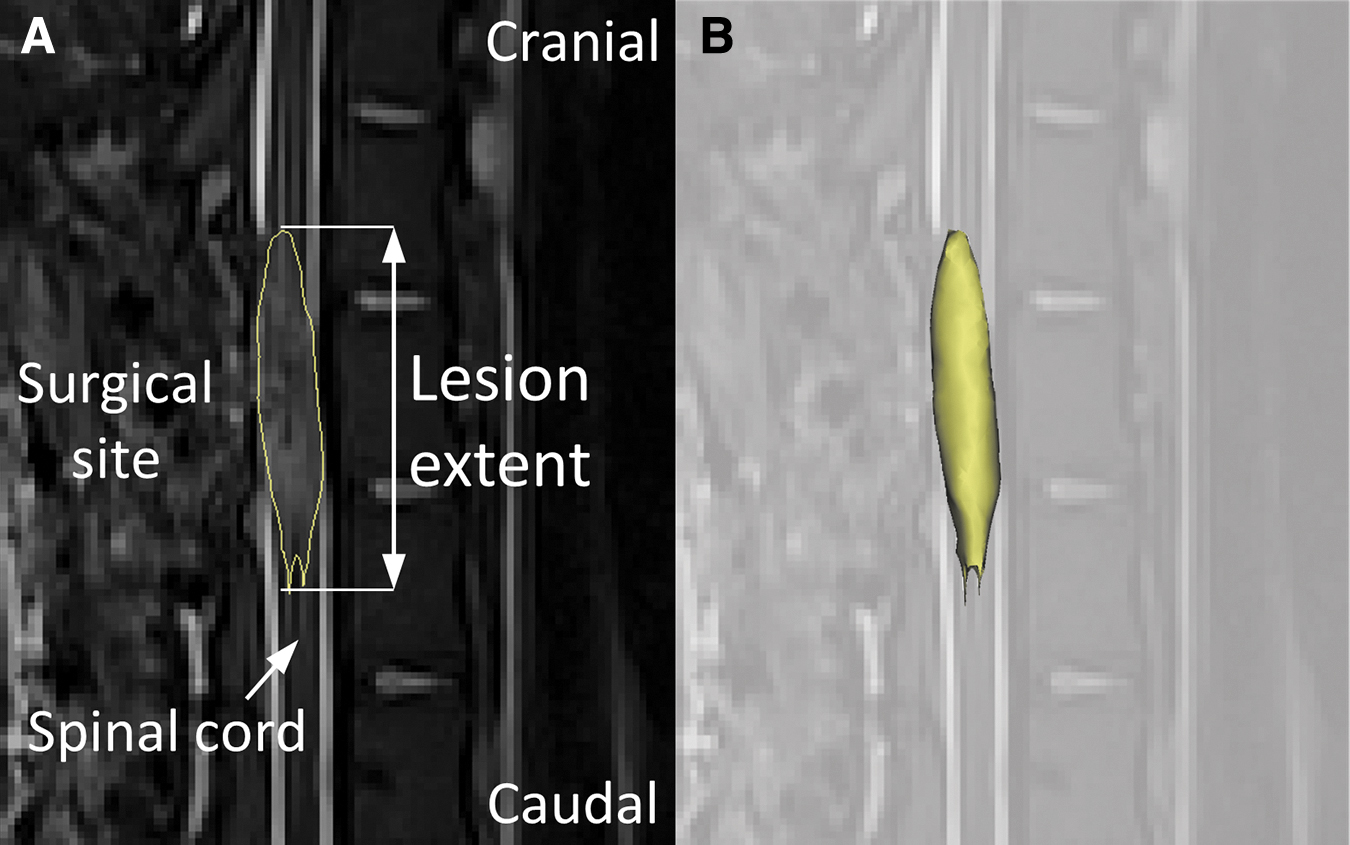
A mid-sagittal MRI slice with the hyperintense signal model overlaid (yellow). Lesion extent was measured between the most cranial and caudal points
Histological analysis
Pigs were humanely killed at 14 days post-injury via intracardiac perfusion with 1 L heparinized saline, then 2.5 L 10% neutral buffered formalin (ACE Chemical Company, Australia). In a purpose-specific room, on a post-mortem table with drainage into waste containers and a local air extraction unit, the pig was placed in a supine position and the thoracic cavity opened. Saline and formalin were introduced into the cardiovascular system using a custom container attached to room compressed air regulated to 80–120 kPa, via tubing and a 14G catheter needle inserted into the left ventricle. Researchers wore half-face respirator masks (6200 with ABE1 class filters; 3M, Minnesota, USA) throughout the procedure. Spinal cord tissue was harvested and post-fixed in 10% neutral buffered formalin. Segments 1 cm in length, centered about the injury site, were processed and embedded in paraffin, then serially sectioned in the transverse plane at 5 μm thickness.
Total lesion volume was assessed with Luxol fast blue, hematoxylin and eosin (LFB/H&E) staining of serial tissue sections 500 μm apart taken from the injury site (approximately 3–5 cm total).
Immunohistochemistry was performed to evaluate axonal injury (amyloid precursor protein [APP]) 54 in spinal cord sections at the injury epicenter, 1 and 3 cm cranial and caudal, and spared white matter (Eriochrome cyanine/neurofilament [EC/NF]) was assessed throughout the injury site on tissue sections 500 μm apart. Heat-induced antigen retrieval was performed in a citrate buffer (pH = 6) for 10 min at boiling, then sections were blocked in normal horse serum (NHS; S-2000-20, Vector Laboratories). The primary antibody (APP: MBS766745, 1:2000, MyBioSource; NF: ab215903, 1:4000, Abcam) was incubated overnight, the secondary antibody (horse anti-mouse IGG, BA-2000-1.5, 1:250; Vector Laboratories) was applied for 30 min before the tertiary antibody (streptavidin peroxidase conjugate, SA-5004-1, 1:1000; Vector Laboratories) for 1 h with phosphate-buffered saline (PBS) washes in between. The immunocomplex was visualized with 3,3’-diaminobenzidine (DAB; SK-4100, Vector Laboratories) and counterstained (hematoxylin for APP, and Eriochrome cyanine for NF).
All slides were digitized with a whole slide scanner (NanoZoomer 2.0HT; Hamamatsu Photonics, Japan). Manual segmentation of lesion area, indicated by a decrease in LFB/H&E staining intensity, and spared white matter, indicated by dense blue EC staining, was performed using
Statistical analysis
Due to the small sample sizes, statistical analyses were not performed; however, complete results have been made available to guide future study design (Supplementary Table S1). Values are represented as median [range].
Results
Prior to SCI, no spinal cord abnormalities were observed on MRI and animals demonstrated no motor function deficits. The pre-injury dorso-ventral median diameter of the intrathecal space was 7.43 mm [7.09–8.06 mm] and of the spinal cord was 5.40 mm [4.95–5.81 mm] (Table 1), on ultrasound. When measured on MRI, the intrathecal space diameter was similar (7.55 mm [7.03–7.7 mm]); however, the spinal cord diameter was smaller (4.44 mm [4.21–4.82 mm]). The velocity of the impactor immediately prior to dura contact, and the impulse of the injury event varied by less than 10% of the median, and the peak impact force varied by less than 20% of the median, across each injury group (Table 1).
Table 1: Pre-Injury Body Mass, Intrathecal, and Spinal Cord Dorso-Ventral Diameters from Intra-Operative Axial Ultrasound Images and Pre-Injury MR Images and Biomechanical Parameters of Injury
Force resulting from impactor contact with bone rather than spinal cord.
MRI, magnetic resonance imaging.
All animals survived the procedures, and all received 3–4 days of 24-h care following SCI. High heart rate and body temperature were observed immediately after SCI surgery in 8 animals, and were resolved within 12–24 h. Pain relief was not required beyond 3 days. The wound drain failed to operate in one animal. Urinary catheters were removed by 4 days post-injury, at which point 8/10 animals were capable of spontaneously urinating. Two animals in the 20-cm group (pigs P06 and P07) required manual bladder expression until day 6 or 7. External anal sphincter response to insertion of a rectal thermometer suggested that animals maintained anal tone, and the frequency and consistency of defecation was consistent with fecal continence, in all animals. No surgical wound infections were observed. Some animals developed skin abrasions or minor pressure sores on the rump, which were treated with barrier creams.
Technical difficulties with the injury apparatus resulted in milder injuries than intended for two animals in the 20-cm group. For the first, the impact velocity was insufficient due to an equipment fault (pig P01), and for the second, the impactor contacted bone before the spinal cord, as evidenced by a double-peak in the impactor force data (pig P02; Table 1). These pigs were maintained in the study to observe graded injury severities produced by altering the force or velocity of impact, and to show how milder injuries presented in each of the outcome measures.
Motor function
Prior to injury, no gait anomalies were detected in any animal. On days 8 and 13, both the 10- and 20-cm groups exhibited substantial hind limb motor dysfunction. The 10-cm group demonstrated some weight-bearing ability, whereas the 20-cm group was generally only capable of transiently lifting the knees off the ground. Median PTIBS scores were 6 [5–7] and 4 [3–6] for the 10-cm and 20-cm groups, respectively, on day 8. On day 13, median scores were 7 [6–7] and 4 [2−5] (Fig. 3). At both time-points, pig P01 had mild difficulty balancing during otherwise normal locomotion, and pig P02 demonstrated grossly normal locomotion.
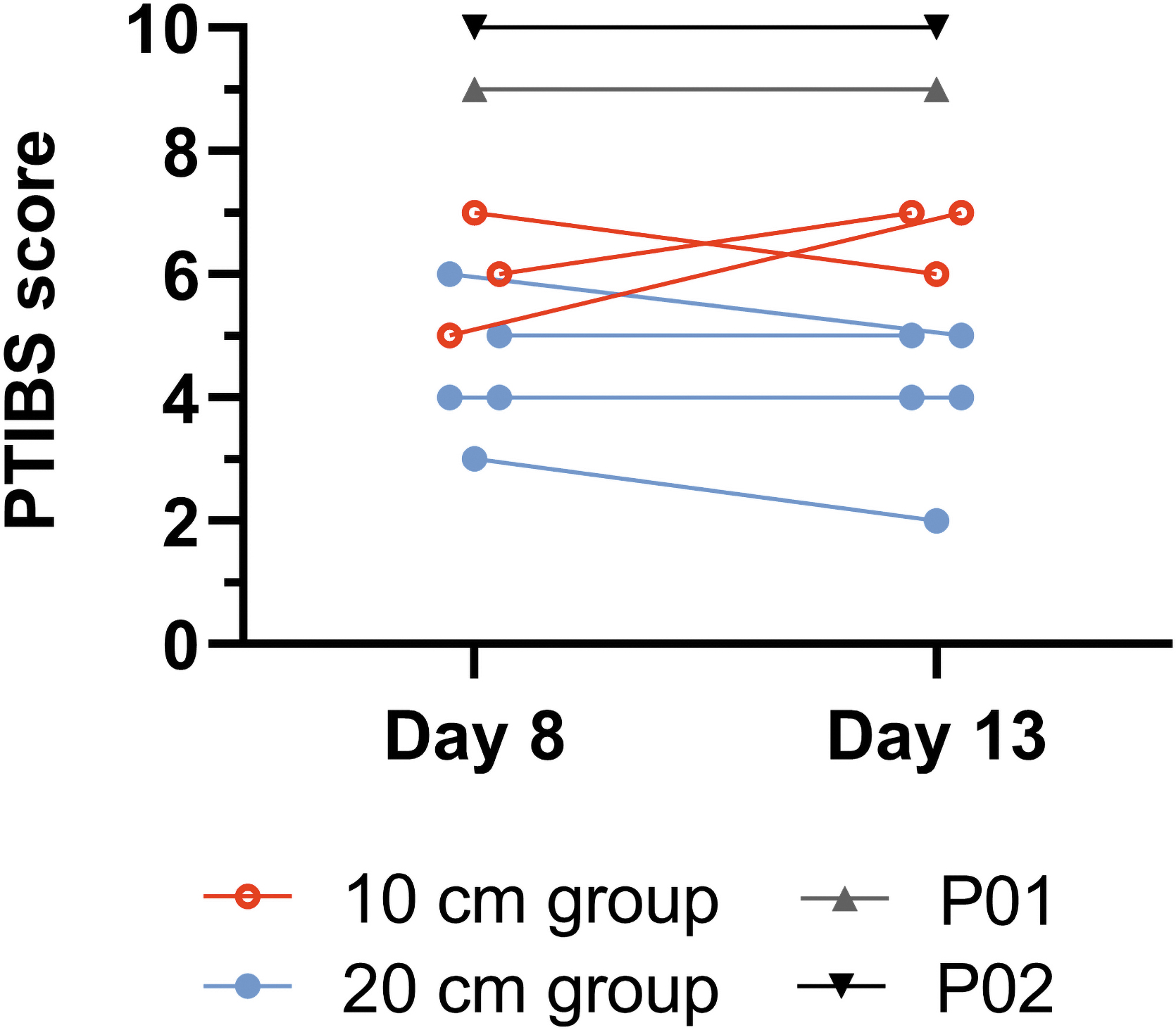
Hind limb motor function was scored on the PTIBS 8 and 13 days post-SCI. A score of 0 indicates no voluntary motor control and a score of 10 indicates normal walking ability. PTIBS, Porcine Thoracic Injury Behavior Scale; SCI, spinal cord injury.
Magnetic resonance imaging
The T2-weighted FSE SPACE MR images revealed a hyperintense region at the injury site for all animals in the 10-cm (Fig. 4A) and 20-cm groups (Fig. 4B) post-SCI. Pig P01 had a notable hyperintense region on day 3 (320 mm3, 33 mm in length), which reduced considerably by day 7 (1.5 mm3, 10 mm in length) and was no longer visible at day 14 (Supplementary Fig. 2A–D). There was no hyperintense region visible on pig P02 post-injury MR images (Supplementary Fig. 2E–H).

Example sagittal T2 SPACE MR images of the lesion site (outlined) taken pre-injury, and at 3, 7, and 14 days post SCI from a 10-cm animal
Animals in the 20-cm group had greater lesion volume (median: 884 mm3 [range: 601–2021 mm3]; 496 mm3 [353–904 mm3]; 441 mm3 [205–1585 mm3]) at day 3, 7, and 14, respectively, than the 10-cm group (504 mm3 [274–574 mm3]; 210 mm3 [126–215 mm3]; 98 mm3 [93–108 mm3]). Lesion volume in the 10-cm group peaked at day 3 and followed a downward trend toward day 14, whereas more variation occurred in the 20-cm group, with increased lesion volume from day 7 to day 14 in two animals (Fig. 4C).
The rostro-caudal extent of the lesion decreased with time in all 10-cm animals (day 3: 28.5 mm [18.0–30.5 mm], day 7: 17.1 mm [16.2–19.0 mm], day 14: 14.3 mm [13.3–14.7 mm]), whereas there was more variation in the 20-cm group (day 3: 42.6 mm [27.7–115.6 mm], day 7: 28.4 mm [26.0–42.3 mm], day 14: 22 mm [13.0–73.3 mm]; Fig. 4D).
Histology
For both injury groups, LFB/H&E staining demonstrated marked tissue damage including regions of tissue death, vacuolization, and loss of structure throughout the injury site. At the center of the injury, tissue damage was evident in both gray and white matter regions; however, this damage typically extended more distally in the gray matter than the white matter (Fig. 5A). The total percentage lesion volume for the 10-mm length of spinal cord centered at the injury epicenter was greater in the 20-cm animals (79% [69–96%]) compared with the 10-cm animals (56% [48–57%]) and rostro-caudal lesion extent was 22.5 mm [14.5–27.5 mm] for the 20-cm group, compared with 12.0 mm [10.5–13.5 mm] for the 10-cm group (Fig. 5B). The tissue damage in both pig P01 and pig P02 involved a smaller percent of each spinal cord section and demonstrated limited extension beyond the epicenter, producing lesion volumes of 8% and 1%, respectively, and lesion extents of 9 mm and 5 mm, respectively (Supplementary Fig. S3).
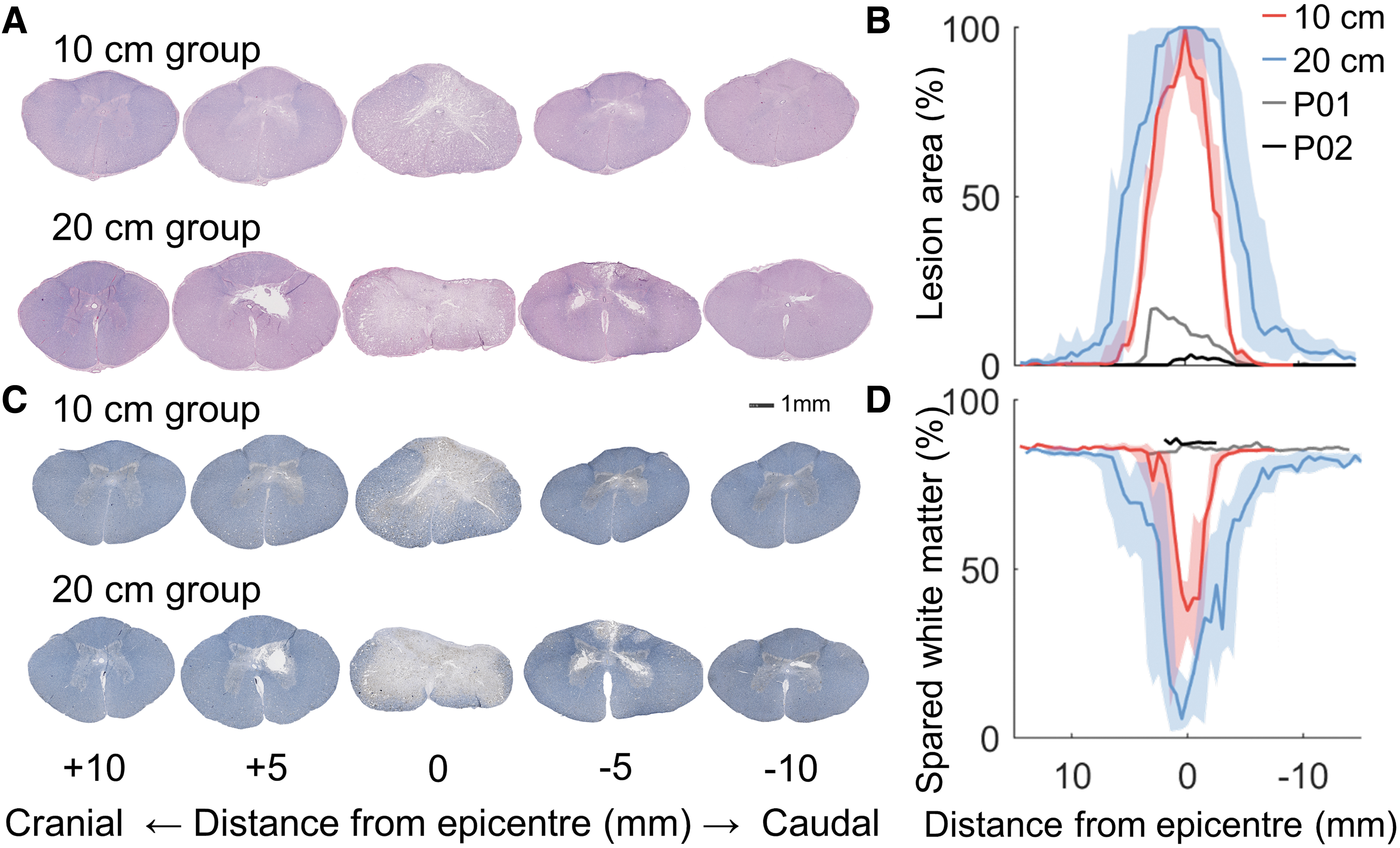
Representative images of LFB/H&E stained spinal cord sections from the 10-cm and 20-cm groups
Myelin loss was observed in the EC/NF stained tissue from all animals except pigs P01 and P02, predominantly occurring in the dorsal columns and central white matter areas of each tissue section, whereas lateral and ventral borders were usually spared at the injury epicenter (Fig. 5C). The percent volume of spared white matter was lower in the 20-cm animals (44% [28–58%]) compared with the 10-cm animals (73% [58–75%]; Fig. 5D).
APP staining indicated axonal injury throughout the white matter at the injury epicenter and 10 mm cranial and caudal, whereas minimal axonal injury was evident at 30 mm. Profuse staining was observed in the lateral and ventral columns but less in the dorsal column where the most tissue damage and loss of axons occurred. There were a greater number of APP positive axons at the epicenter than at 10 mm cranial and caudal, for both injury groups (Fig. 6). At the epicenter, the 10-cm animals demonstrated greater APP immunoreactivity (1605 axons [620–1737 axons]) than the 20-cm group (353 axons [251–1096 axons]); however, at 10 mm caudal and cranial, the 20-cm group had higher APP immunopositive axon counts (rostral: 136 axons [61–158 axons], caudal: 177 axons [74–696 axons]; 10 cm rostral: 35 axons [28–50 axons], caudal: 77 axons [45–85 axons]. Minimal axonal injury was observed for pigs P01 and P02 at all locations (Fig. 6C).

Representative images of APP stained spinal cord sections from the 10-cm group
Discussion
In this domestic pig contusion SCI model, motor function, MRI hyperintensity, lesion volume, and white matter sparing all varied in a manner consistent with the input injury severity (Supplementary Table S1 and Supplementary Fig. S4). Post-SCI, pigs in the 20-cm injury group had median motor function scores that were 2–3 points lower, histological lesion volume that was 20% greater, and almost 30% less white matter sparing, than the 10-cm injury group at 2 weeks post-injury. These findings are consistent with previous pig SCI studies that reported severity-dependent changes in tissue sparing 31,35,55,56 and motor function. 35,39 In addition, association between histological and functional outcomes has also been observed. 35,41 In T2-weighted MR images, the median rostro-caudal extent of hyperintensity in the 20-cm injury group was 50% greater than in the 10-cm injury group up to 2 weeks post-injury, and median hyperintensity volumes were 1.8, 2.5, and 4.5 times greater at day 3, 7, and 14, respectively. Although the current study is one of few to report in vivo MRI outcomes for several SCI severities in pigs, others have shown that T1-weighted hypointensity corresponds with severity-dependent histological lesion volume, 34 and that T2-weighted signal change is related to locomotor deficit. 40
Motor deficit resulting from this weight-drop apparatus has not previously been reported for a domestic strain of pig. The injury apparatus impactor release heights and static compression duration used in the current study were based on a miniature pig SCI model for which a release height of 20 cm (with the same weight and compression), produced injury sufficient to detect effects of an intervention. 35 In the current study, the 10- and 20-cm release heights produced similar impact velocities but greater peak force than equivalent models, 35,57 with low variability. Animals in the current study scored 1 point higher on the PTIBS at 8 and 13 days post-SCI, compared with Yucatan miniature pigs of similar body mass receiving a 20-cm, 50 g weight-drop injury, assessed at 7 and 14 days post-injury. 35,56 However, those animals improved function by 1 point by 6–8 weeks, and remained at that score up to 12 weeks post-injury. 35,56 This suggests similarity in functional response in the domestic strain.
The 10-cm group (assessed at 8 and 13 days post-SCI) scored 2 points higher on the PTIBS than Yucatan miniature pigs injured with equivalent impact mass and height, assessed at 1 and 2 weeks post-SCI. 35,56 The domestic pigs were able to maintain their knees off the ground for additional steps and progressed to extension of the knee. This may suggest that domestic pigs have a higher tolerance than miniature pigs, although the sample size is low and follow-up was limited to 2 weeks post-injury, in the current study. In a study with 4 weeks post-injury follow-up, motor function reached a plateau 2 weeks after incomplete contusion SCI, 34 whereas other models have demonstrated improvement over 6–11 weeks post SCI, 35,39,57 or no improvement at all post- injury. 32,34,51 This inconsistency may be due to different injury severities, variation in functional scoring systems, differing injury mechanics due to spinal cord and dural sac dimensions, and/or the influence of animal age and breed on injury response.
Animal personality and scoring practices may have contributed to motor function scores within this study. In three animals, the PTIBS scores reduced by 1 point from day 8 to day 13. This change is likely not reflecting actual functional deterioration, but rather is a consequence of strict adherence to the scoring protocol, which grades only the video-recorded functional tasks. Animal personality, motivation, and adaptation to post-SCI ability appeared to affect performance, particularly at early time-points, which may explain the higher variability of motor function scores at day 3. In future studies, a score of animal demeanor may complement the PTIBS protocol.
In the current study, T2-weighted MR images for both injury groups displayed hyperintensity in the spinal cord at the injury site, indicative of edema 58,59 and corresponding to lesion volume (from histology) and motor function deficit. The hyperintense region decreased in volume for 8/10 animals, and in extent for 7/10 animals, from day 3 to day 14 post-injury. Reduced volume of hyperintensity beyond 1 day post-injury has been reported for rat contusion SCI models, 60,61 and a reduction in the extent of T2 hyperintensity after the first 2 days has been observed in patients with cervical SCI. 62 However, rabbit 63 and rat 61 contusion SCI models have demonstrated that edema and MRI hyperintensity, respectively, peak at 7 days post-SCI. The results of the current study support this, as diffuse tissue loss was typically observed in both gray and white matter of LFB/H&E and EC/NF stained tissue. The pigs in which hyperintensity volume or rostro-caudal extent increased from day 7 to 14 were all in the 20-cm group, had the greatest hind limb motor deficit, and had a larger lesion volume in histological sections, supporting a relationship between hyperintensity, histological lesion volume, and functional deficit 34,64 ; however, the reason for the fluctuation in signal hyperintensity post-SCI for these animals is not known.
Although day 14 post-injury lesion extent appeared to be similar when measured with histology and MRI, lesion volume was less consistent between the methods. Lesion volume from in vivo MRI was greater than from histology in the 20-cm group, but was similar for the 10-cm group (Supplementary Table S1). Lesion extent was similar between MRI and histology for both groups, except for two animals in the 20-cm group (pigs P05 and P06). They both had particularly large MRI lesion volume and extent compared with histology and with other animals in that group at day 14 (Supplementary Fig. S5A, B), and a notable increase from day 7 to 14 for both MRI measures (Fig. 4C, D). Although there are no reported quantitative comparisons of histology and MRI in large-animal contusion SCI models, comparison of lesion volume from various histology methods and MR sequences (usually ex vivo) have been reported for small-animal models.
In hemisection models in mice at 6 weeks, 65 and non-human primates at 3 months, 6 lesion volume from histology was similar to that measured on ex vivo 9.4T MRI, but less than that measured on equivalent in vivo MRI. In a clip-compression rat model at 6 weeks, the difference in lesion volume measured on ex vivo MRI versus histology was variable and dependent on tissue preparation consistency, 66 whereas in fixed spinal cords from mice 6 weeks post-contusion, histology- and MRI-derived lesion volume was similar. 67 Although the current study did not aim to determine correspondence between measurement modalities, the observed differences may be partly due to the effect of fluid distribution in vivo due to edema versus a lack of free fluid in post-mortem fixed tissue, tissue shrinkage during histology processing, and differences in spatial resolution and “signal” contrast between the two modalities.
APP staining provided an indication of injured and susceptible axons not detected by the lesion volume and tissue sparing analysis. As expected, the greatest amount of axonal injury was observed within the injury epicenter for both groups. Although the 20-cm group demonstrated lower APP-positive counts within the injury epicenter than the 10-cm group, this is predominantly due to the significant tissue loss observed in the 20-cm group as demonstrated in the lesion volume and tissue sparing analyses. The 20-cm group demonstrated greater axonal injury than the 10-cm group in the adjacent segments, demonstrating that greater weight-drop height is associated with greater tissue damage beyond the injury epicenter.
Greater immunoreactivity and more swollen axons are associated with greater injury severity in rat compression SCI models. 68,69 This occurred at both the epicenter and at more distal regions in one of these studies 68 ; however, in the other, results were only reported for regions beyond the epicenter, 69 so it is unclear whether APP immunoreactivity at the epicenter followed the same severity-dependent pattern observed distally, or whether the milder injury group had greater counts as observed in the current study. In rats and mice, the number of APP-positive axons peaked between 3 and 7 days post-SCI. 70,71 This suggests that in the current study, APP accumulation may have been greater at the epicenter for the 20-cm animals prior to the 2-week study end-point and before axonal death occurred.
Previous pre-clinical SCI models have identified that spinal cord and intrathecal dimensions may influence injury outcomes, as larger pre-injury ultrasound measurements of both have been associated with better motor outcomes and less tissue damage. 40,57 In the current study, median pre-injury ultrasound measurements of spinal cord and intrathecal diameters were 5.40 mm [range: 4.95–5.81 mm] and 7.43 mm [7.09–8.06 mm], respectively (Table 1). Intrathecal diameters measured on MR images were similar; however, spinal cord diameter was slightly smaller and this can likely be attributed to the lower image resolution and the partial volume effect present in the MR images.
Ultrasound measurements in the current study were similar to spinal cord (mean 5.34 ± standard deviation 0.28 mm) and intrathecal (7.79 ± 0.72 mm) diameters reported for ultrasound images of Yucatan miniature pigs weighing 19.5–34 kg. 57 In that study, animals with a 20-cm weight-drop SCI at spinal level T10 had PTIBS scores 2–3 points lower at 14 days post-SCI than animals with the equivalent injury in the current study, despite lower peak force, impulse, and cord/dura displacement. Although Kim and colleagues 57 found that dorso-ventral spinal cord diameter less than 5.33 mm was associated with poorer functional outcomes, the difference in PTIBS between that study and the current study does not appear to be related to spinal cord or intrathecal diameter as these were similar. In the current study, the worst functional outcome occurred in a 20-cm animal (pig P05) with a spinal cord diameter of 4.95 mm, the smallest of all animals across both groups. However, there were insufficient animal numbers in each group to observe a similar relationship as seen by Kim and colleagues, 57 indicating that this domestic pig strain may exhibit a similar relationship between spinal dimensions and injury outcome.
Epidural hematoma was observed at the surgical site on MR images, and appeared to compress the spinal cord in some animals (n = 3), although it reduced in size from day 3 to day 14 (Supplementary Fig. S6). Spinal cord compression due to hematoma may affect functional and histological outcomes, but an association could not be evaluated in this study due to low sample size. Pig P01 presented with a large hematoma and scored 9 on the PTIBS; however, it is unclear whether the functional deficit was caused by ongoing compression due to the hematoma or the dynamic weight-drop contusion. Symptomatic post-operative epidural hematomas are a rare but potentially serious complication, occurring in up to 1% of spinal surgeries 72 and often requiring surgical evacuation. 73 Asymptomatic post-operative hematomas may occur in more than 50% of spinal surgeries, 74,75 but are not detected without routine post-surgical imaging. Epidural hematoma has not been reported in other pig models of SCI; however, few models have included in vivo MRI at post-surgical time-point(s) (Table 2).
Porcine Thoracic Contusion SCI Characterization Studies Including In Vivo MRI, Locomotion, or Similar Histological Stains to the Present Study
Articles by the same group but characterizing SCI in different breeds.
Articles by the same group but with different injury parameters and pig age/weight.
Animals were euthanized an estimated 30 min to 1 h post-SCI after neurophysiological monitoring.
Animals were euthanized following the MRI that took place after SCI.
Some non-characterization studies have been included where a characterization article for that group was not found.
EC, Eriochrome cyanine; H&E, haematoxylin and eosin; LFB, Luxol fast blue; MRI, magnetic resonance imaging; NF, neurofilament; PTIBS, Porcine Thoracic Injury Behavior Scale; RARE, rapid acquisition with relaxation enhancement; SCI, spinal cord injury.
Surgical drains are commonly used after spinal surgery, but their ability to reduce surgical-site infection and hematoma is questioned. 76 Surgical drain use was reported for one pig SCI model, 50 but only immediate post-operative MR imaging was undertaken. In the current study, when a surgical drain wasn't placed (n = 2) or the drain was compromised (n = 1), at least 50% occlusion of the sagittal canal was observed at day 3 despite effective hemostasis via the use of bone wax, cautery, and the paraspinal muscle periosteal-stripping surgical approach. Following the introduction of wound drains into the protocol, hematoma size reduced. Extradural compression appeared to be further reduced in later animals by closing the surgical wound with a single, looser, muscle layer. This suggests that wound drains, careful attention to hemostasis and wound closure, and assessment of hematoma by MRI, may be beneficial in pig models of SCI that require surgical exposure of the spinal cord via laminectomy.
The length of the laminectomy performed to expose the spinal cord and dura is variable across pig contusion SCI models. In the current study, a 3-cm laminectomy was selected to match the length of spinal cord edema observed in a pilot study, and to facilitate localized surgical interventions and/or probe insertion at the injury site in future studies. Other survival models have used laminectomies ranging from one vertebral level to allow passage of the impactor, 38 to four vertebral levels to accommodate probes or other procedures. 57,77,78 It is not known if laminectomy length contributes to functional, histological, or MRI outcomes, for example via decompression of the epidural space or increased propensity for hematoma formation.
Although it was not a primary aim of the study, analysis of animal care requirements was an important part of developing this model and as such, details are provided for others seeking to develop similar models. Animal care was demanding in the 24 h following SCI, and required close monitoring of heart rate, core temperature, and food and water consumption. Heart rate reached 140 bpm in all animals immediately after surgery, and in three animals exceeded 170 bpm before returning to pre-injury levels (90–130 bpm), usually within 12 h. Anesthetic recovery and the SCI may have contributed to this response. 79 Eight animals recorded core temperatures reaching 40°C in a similar time period, exceeding the normal range of 37.5–39.5°C. Elevated temperatures have been reported post-SCI in a miniature pig model, 42 and have increased during SCI surgery, 50 despite other literature suggesting that pigs are prone to hypothermia while anesthetized. 80,81 In the current study, pigs were maintained on elevated canvas dog beds for 3–4 days post-injury because these appeared to enable greater ventilation and cooling than mattress and crate bedding. During this time, pigs were fed and watered by a caregiver, but on returning to the pen, feed bowls were modified to accommodate limited mobility. Reduced appetite post-SCI returned to normal within 24–36 h, and animals tolerated the procedures and functional deficit well throughout the 2 weeks.
Although there is limited scope to determine relationships between injury groups and outcome measures due to sample size, some observations are offered. The animal (pig P05) with the smallest spinal cord diameter received a weight-drop with the greatest impact velocity and generated the second greatest peak force. This produced the worst PTIBS score, the largest histological lesion volume, and the largest MRI lesion volume and extent at days 3 and 14 (Supplementary Table S1 and Supplementary Fig. S4), indicating that this animal consistently demonstrated a severe injury across various measures. Spinal cord dimensions, impact velocity, and peak force alone do not explain the outcomes for the other animals. Although statistics are not presented, a heat map (Supplementary Fig. S4) suggests some relationships across multiple domains, including worse PTIBS scores occurring with greater lesion volume.
There were a number of limitations in this study. The high costs and resources associated with large-animal studies limited the sample sizes and follow-up time possible. Typically, no more than 10 animals are used per group in non-survival SCI studies using domestic pigs, 36,37,43,48,50 and 5–15 domestic pigs across 1–2 groups have been used in survival models, 29,41,44 similar to the current study. In miniature pigs, up to 52 animals across 5 experimental groups have been used in a single study 40 (Table 2). Due to their rapid growth rate, and the mass of mature animals, domestic pigs are best suited to studies in which an age of around 3 months at injury, and shorter-term follow-up, is acceptable. Miniature pig SCI models have shown improvements in motor function up to 6 weeks post-SCI, 35 and this is likely the upper limit of post-injury follow-up possible in domestic animals entering a study at 25–30 kg. Studies using domestic animals of this weight and a starting age of 3 months have included follow-up for 5 weeks, 41 whereas a 3-month follow-up was possible in 2-month-old domestic pigs weighing only 10–15 kg. 29
Although histological analysis was only completed at 2 weeks post-SCI, because it was not feasible to include groups with earlier experimental end-points in this study, MR imaging was undertaken three times post-injury, providing qualitative observation of morphological changes at the injury site during that period. This is of interest given the dynamic nature of the spinal cord lesion and secondary injury processes occurring within the first few days. 58 More frequent MR imaging was not undertaken so that animals had adequate recovery between each anesthetic exposure, and could undertake periodic functional assessment. 3T MRI does not provide detailed insight into the microscopic cellular and extracellular changes possible with histological analysis, and earlier imaging and histology analysis may be useful for a more complete characterization of the model.
Another limitation of the study was having two animals with considerably milder injuries than planned. In both pig P01 and pig P02, histological analysis demonstrated minimal spinal cord lesion and axonal injury, and no loss of white matter. In pig P01, MR hyperintensity resolved by day 14, and motor impairment was similar to that reported for 5-cm impactor height in an equivalent weight-drop model in Yucatan miniature pigs, despite the peak force of injury being greater. 35 Pig P02 had an overall milder injury than pig P01, showing a consistent lack of demonstrable injury across MRI and motor function outcomes. Although these low injury severities were unintentional, the data demonstrate relationships between the outcome measures that may occur for weight-drop release heights less than 10 cm, for which little data are currently available in pigs. 35
Conclusions
In this study, a domestic pig model of graded contusion SCI was characterized with 2 weeks survival. Biomechanical injury parameters, motor function, and histological outcomes were comparable to other SCI models using both miniature and domestic pigs. It is one of few studies to investigate in vivo MRI hyperintensity at multiple time-points post-SCI. This domestic pig model is an alternative large-animal model for investigating the acute natural history of SCI, and for assessing acute therapeutic and surgical interventions, where miniature pig breeds are not available or are cost-prohibitive, and where a large-animal model is most appropriate for addressing the aims of the study.
Footnotes
Transparency,Rigor,and Reproducibility Summary
This study, and the corresponding analysis plan, were not formally registered due to the developmental nature of the project. The study design, experimental conditions, and outcomes are detailed above. A sample size of 10 animals was planned based on scheduling, logistics, and cost. Technical difficulties occurred in 2 animals and they were subsequently removed from their severity groups. However, the data from these animals were included in the study independent of the two planned severity groups to demonstrate how a milder injury would present. Subsequently, there were 5 animals within the high-severity group and 3 animals in the low-severity group. Statistical analysis was intended; however, the reduced sample size prohibited the performance of meaningful statistical analysis.
The motor function assessment scale (PTIBS) is established within the field, and frequently used for this injury model. Investigators completing the analysis of motor function were blinded to the severity group and results were cross-checked. MR and histological images were labeled with the animal number but not the severity. In one animal, MR imaging occurred on day 8 instead of day 7 due to a public holiday and MRI unavailability. Antibody concentrations for immunohistochemistry (IHC) procedures were optimized prior to staining the complete data set. APP staining was completed in a single batch. EC/NF and LFB staining was completed in two batches with control slides included for comparison between the batches. Materials and software required to complete this study are publicly available as per company names listed above, except the injury device, which was custom made. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. A limited number of histological samples from each of the experimental groups are available for future analyses on request. The authors agree to provide the full content of the manuscript on request by contacting the corresponding author.
Acknowledgments
The authors acknowledge the technical assistance of Dr. Chris Christou and the staff of the South Australian Health and Medical Research Institute Preclinical, Imaging and Research Laboratories. The authors acknowledge the facilities and scientific and technical assistance of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability, at the South Australian Health and Medical Research Institute Preclinical, Imaging and Research Laboratories. The authors thank Kitty So, Neda Manouchehri, Brian Kwon, and staff of the Centre for Comparative Medicine, University of British Columbia, for technical advice. The authors thank Professors Nigel Jones and Markus Stoodley for helpful discussions.
Authors' Contributions
The authors contributed as follows: conceptualization, AVL and CFJ; methodology, CDG, MAB, AM, AVL, and CFJ; validation, CDG, AVL, and CFJ; formal analysis, CDG, MAB, and CFJ; investigation, CDG, MAB, RMD, RDQ, AM, RLOD, AVL, and CFJ; resources, AM, AVL, and CFJ; data curation, CDG and CFJ; writing—original draft, CDG, AVL, and CFJ; writing—review and editing, CDG, MAB, RMD, RDQ, AM, RLOD, BJCF, AVL, and CFJ; visualization, CDG, MAB, AVL, and CFJ; supervision, BJCF, AVL, and CFJ; project administration, CDG and CFJ; funding acquisition, BJCF, AVL, and CFJ.
Funding Information
This work was supported, in part, by grants from Conquer Paralysis Now (Collaboration Award) Depuy Synthes (Investigator-Initiated Study Grant), and the North American Spine Society. Spinal instrumentation was provided in-kind by Medtronic LLC. CDG received a PhD scholarship from The Hospital Research Foundation. CFJ was partially supported by a National Health and Medical Research Council (Australia) Early Career Fellowship during this study (APP1072387).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.