
Abstract
Impaired cerebrovascular reactivity has emerged as an important associate with poor long-term outcome after moderate/severe traumatic brain injury (TBI). However, our understanding of what drives or modulates the degree of impaired cerebrovascular function remains poor. Age and biological sex remain important modifiers of cerebrovascular function in health and disease, yet their impact on cerebrovascular reactivity after TBI remains unclear. The aim of this study was to explore subgroup responses based on age and biological sex on cerebral physiology. Data from 283 TBI patients from the CAnadian High Resolution TBI (CAHR-TBI) Research Collaborative were evaluated. Cerebrovascular reactivity was determined using high-frequency cerebral physiology for the derivation of three intracranial pressure (ICP)–based indices: 1) pressure reactivity index (PRx)—correlation between ICP and mean arterial pressure (MAP); 2) pulse amplitude index (PAx)—correlation between pulse amplitude of ICP (AMP) and MAP; and 3) RAC—correlation between AMP and cerebral perfusion pressure (CPP). Insult burden (% time above clinically defined thresholds) were calculated for these indices. These cerebral physiology indices were studied for their relationship with age via linear regression, age trichotomization (< 40, 40 - 60, > 60), and decades of age (< 30, 30-39, 40-49, 50-59, 60-69, > 69) schemes. Similarly, differences based on biological sex were assessed. A statistically significant positive linear correlation was found between PAx, RAC, and age. In corollary, a statistically significant relationship was found between increasing age on trichotomized and decades of age analysis with PAx and RAC measures. PRx failed to demonstrate such relationships to advancing age. There was no clear difference in cerebrovascular reactivity profiles between biological sex categories. These findings suggest that AMP-based cerebrovascular reactivity indices may be better positioned to detect impairment in TBI patients with advancing age. Further investigation into the utility of PAx and RAC is required, as they may prove useful for certain subgroups of patients.
Introduction
Impaired cerebrovascular reactivity has recently emerged as a critical associate with poor long-term outcome in moderate/severe traumatic brain injury (TBI). 1 –6 Cerebrovascular reactivity metrics are surrogate measures of cerebral autoregulation, originally defined by Lassen 7 as the innate ability of the cerebral vessels to maintain constant cerebral blood flow (CBF) over a wide range of mean arterial pressures (MAP) or cerebral perfusion pressures (CPP), ensuring a steady state of oxygen and nutrient delivery to the brain. 8 The shape of this autoregulatory curve varies depending on individual injury burden and medical co-morbidities, with varying ranges of normal, which can often be narrow in nature. TBI and any form of brain trauma causes impairment of cerebral autoregulation which can then lead to potentially unfavorable long-term outcomes. 1 –6
Three key continuously updating intracranial pressure (ICP)–based indices help clinicians monitor cerebral autoregulation at the bedside, and have been validated pre-clinically in experimental models. 9 –12 These indices are: pressure reactivity index (PRx)—the correlation between ICP and MAP; pulse amplitude index (PAx)—the correlation between pulse amplitude of ICP (AMP) and MAP; and RAC—the correlation (R) between AMP (A) and cerebral perfusion pressure (CPP). 9,13 -15 PRx is most widely published on, while PAx and RAC continue to emerge in the literature with very promising results. 9,15 –19 However, regardless of the measure utilized, our understanding of the drivers and modulators of impaired cerebrovascular reactivity after moderate/severe TBI remains largely unclear. 2,20 –24
Two important potential modifiers of cerebrovascular and secondary injury responses are chronological age and biological sex. These two factors have great bearings on cerebrovascular response seen across health and disease, and have been documented in the TBI literature as associates with long-term patient outcomes. Age is one of the major drivers of prognosis and is a crucial component of existing standard prognostic models in moderate/severe TBI. 16 Elderly persons tend to suffer poor outcomes after sustaining a TBI as arterial integrity and functions deteriorate in most cases secondary to deleterious effects of chronic illnesses, poor neuronal repair mechanisms and deposits of biological matter in the arterial walls. 25 –28 Next, biological sex impacts cerebrovascular response in TBI independently and even in relation to advancing age. In animal models, females in their reproductive years have a superior advantage over males as estrogen and progesterone promote protective cerebral vasculature vasodilation and anti-inflammatory effects secondary to the action of prostaglandin I2 (PGI2). 25,29 –32 And conversely, they suffer the vasoconstrictive effects of thromboxane A2 (TXA2) during low hormonal states (older females and males). 25,29 –32 Of note, males usually constitute the majority of TBI cohorts and seem to have the worst outcomes. 19,25,33,34
However, despite the possible impact of age and biological sex on cerebrovascular function after moderate/severe TBI, there is limited literature evaluating their role in modulation of continuously measured cerebrovascular reactivity. A scoping review by Batson and colleagues 35 showed that nine original studies documented a correlation between advanced age and worse cerebrovascular reactivity; eight on PRx, 19,21,22,25,32,34,36,37 three on PAx, 19,22,38 and one on RAC. 22 This study also showed that three articles 22,33,36 had a correlation between biological sex and PRx with females having higher PRx values, and no studies existing on PAx and RAC. Yet, all identified studies carried significant limitations, including grand averaged data over large swaths of recording periods for patients and no evaluation of insult burden metrics of impaired cerebrovascular reactivity, which have recently emerged as stronger qualifiers of cerebrovascular function in TBI. 1 –4,6 Further to this, given the relatively new nature of PAx and RAC, the literature on these metrics was essentially non-existent.
In an attempt to remedy this, the Winnipeg Acute TBI Laboratories performed an exploratory analysis that showed that there was a statistically significant relationship between PAx, RAC and age with linear regression and age trichotomization analysis but not with PRx and age. 16 Also, in their cohort, biological sex did not have an impact on the cerebrovascular reactivity measures. 16 This cohort had well controlled ICP and CPP values over the course of their intensive care unit (ICU) stay. Subsequently, such findings suggested that AMP-based cerebrovascular reactivity indices performed superior to the standard PRx in detecting impaired reactivity in populations with advancing age. However, this exploratory analysis suffered from power issues, leaving the results preliminary and necessitating further investigation.
The CAnadian High-Resolution TBI (CAHR-TBI) Research Collaborative was created in 2019 for the purpose of investigating cerebral physiologic relationships in acute neural injury, using high-fidelity multi-modal cerebral physiologic data sets collected in a multi-center fashion. 39 This study provides a follow-up validation analysis 16 of the impact of age and biological sex on ICP-based cerebrovascular reactivity in moderate/severe TBI using the multi-center CAHR-TBI dataset.
Methods
Study type
This is a retrospective multi-center study of a prospectively maintained database of moderate to severe TBI patients. Data from the CAHR-TBI Research Collaborative, 39 led by the Winnipeg Acute TBI Laboratories was used. This data came from the Universities of Manitoba, British Columbia, and Calgary, and contains demographic, injury, treatment, outcome information and high-frequency physiology from various multi-modal monitoring devices. Local research ethics board approval at the University of Manitoba is in place for all aspects of this database (H2017:181 and H2017:188). Similarly, we obtained ethics approval for retrospective access to the database and for data transfer with each center for this project (H2020:118, H20-03759, and REB20-0482).
Patient population
Patient data was entered into the database from January 2019 to December 2021 for the University of Manitoba, 2014 to 2019 for the University of British Columbia, and 2011 to 2021 for the University of Calgary. Inclusion criteria for this study were patients 16 years and older who suffered moderate-to-severe TBI with invasive ICP and arterial blood pressure (ABP) monitoring who were admitted to the ICUs of the Health Sciences Centre (University of Manitoba), Vancouver General Hospital (University of British Columbia), and Foothills Medical Center (University of Calgary). Patients who were younger than 16 years, those who suffered mild TBI and those without invasive ICP monitoring were excluded from this study. None of the patients were actively treated according to cerebrovascular reactivity monitoring or optimal CPP (CPPopt) guided–therapy.
Patient data collected
For the purposes of this study, we extracted general admission demographics for this patient cohort from the database. The demographic variables included: age, sex, admission pupillary response, admission Glasgow Coma Scale (GCS) total and motor sub-score, pre-hospital hypoxia, presence of traumatic subarachnoid hemorrhage index CT (CT-tSAH), presence of epidural hematoma index CT (CT-EDH), admission Marshall CT grade, 40 and admission Rotterdam CT grades 41 for the University of Manitoba cohort. The University of British Columbia cohort included all of these except presence of CT-tSAH and presence of CT-EDH. The University of Calgary cohort included all of these except best admission GCS—motor, presence of CT-tSAH, and presence of CT-EDH.
Physiologic data acquisition
Standard care at these centers for critically ill TBI patients includes ABP and ICP monitoring which is also in keeping with the brain trauma foundation (BTF) guidelines. 42 ABP was monitored via radial arterial lines (zeroed at the level of the tragus) and ICP was monitored via intraparenchymal strain gauge monitors (Codman ICP Microsensor; Codman & Shurtleff Inc., Raynham, MA), with external ventricular drains used in the minority of cases. All physiology data was recorded in digital high-frequency time series (i.e., 100 Hz) using analogue-to-digital signal converters (Data Translations, DT9804 or DT9826) where applicable. This digital data was linked and stored in time series using Intensive Care Monitoring (ICM+) software (Cambridge Enterprise Ltd, Cambridge) .
Physiologic signal processing
Artifact clearing was performed on the data using ICM+ software to manually remove signal interferences, including drain opening-artifact for those small number of patients with ventricular drains. This was performed under the supervision of a qualified clinician with experience with all of the multi-modal cerebral physiologic signals both in bedside care and in the laboratory environment. All signal files were cleaned without knowledge of patient age or sex as they were completely de-identified when stored in the signals database. CPP was calculated as MAP minus ICP. Second, pulse amplitude of ICP (AMP) was derived using the fast Fourier transform decomposition of the ICP pulse waveform. 18,19 Afterward, the full waveform data for all physiology was decimated using non-overlapping moving average filter of 10-sec duration, which facilitates focusing on the slow-wave frequency range associated with cerebral autoregulation and reduce interference with ventilation induced changes. This 10-sec by 10-sec data was then used to derive continuously updating cerebrovascular reactivity and compensatory reserve measures.
As an example, PRx is computed as the moving Pearson correlation coefficient between 30 consecutive 10-sec mean paired values of ICP and MAP. The other indices are computed in a comparable manner. The following cerebrovascular indices were derived: PRx—correlation between slow waves of MAP and ICP, 1,43 pulse amplitude index (PAx)—correlation between slow waves of AMP and MAP, 18,19 and RAC—correlation (R) between slow-waves of AMP (A) and CPP (C), 17 Lastly, the continuously updating compensatory reserve index, RAP (correlation between slow-waves of AMP and ICP) 44 was also derived to facilitate surrogate evaluation of brain compliance. All signals (recorded and derived) were output in minute averages into comma-separated values datasets for further analysis.
Physiologic data post-processing
The data were sorted into two main datasheets (i.e., the first 72 h of recording and the entire recording period). The first 72 h is the critical time where most acute physiology changes and aggressive treatment would occur post-TBI.
1,23,45
This period of time is crucial and was compared with the entire recording period to see what important findings arise. Doing this will avoid the pitfalls of previous literature regarding grand averaging of large amounts of data relating to cerebrovascular reactivity, especially when withdrawal of the treatment due to refractory intracranial hypertension occurs with monitoring devices still in place. Also, insult burden metrics were derived for key physiology measures for all of the data sheets. These metrics were defined as the percent (%) time spent above literature defined thresholds for ICP, CPP, PRx, PAx, and RAC. These derived variables included: % Time with ICP above 20 and 22 mm Hg. These are BTF-based ICP treatment thresholds.
46
% Time with CPP below 60 mm Hg and above 70 mm Hg. These are BTF-based CPP thresholds.
13,42
% Time with PRx above 0, +0.25, and +0.35. These are literature-defined critical thresholds associated with outcomes in TBI.
9,13
% Time with PAx above 0 and +0.25. These are literature-defined critical thresholds associated with outcomes in TBI.
9
% Time with RAC above -0.10 and -0.05. These are literature-defined critical thresholds associated with outcomes in TBI.
9
Statistical analysis
The data was analyzed using the R statistical software (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics; mean/standard deviation (SD) and median/interquartile range (IQR) were used to summarize patient demographics and physiology variables, where appropriate. Boxplots were used as a visual aid of the data. Shapiro-Wilks tests were performed on the continuous variables from these two data sets to test for normality, with all physiologic variables demonstrating non-parametric natures. Multiple comparisons were corrected for using false discovery rate (FDR) testing.
The impact of biological sex on the continuously measured metrics (namely ICP, MAP, CPP, PRx, PAx, and RAC) was assessed by comparing values between males and females using the Mann-Whitney-U test. Age was assessed using linear regression, trichotomization and decades of age (dividing into six subgroups) categorical analyses. To begin, age was used as a continuous variable and compared with the physiology variables using Pearson correlations. Scatterplots; linear regression plotting (95% confidence interval [CI]) were used for data visualization. Then, age was divided based on age trichotomization (i.e., Age <40, Age 40-60 and Age >60) and division by decades of age (i.e., Age <30, 30-39, 40-49, 50-59, 60-69, > 69). A cutoff of 60 years was chosen as this is common for outcomes in various neuropathological and critical care states as patients older than 60 years suffer unfavorable outcomes. 42,47,48
The basis of the age trichotomization scheme was to evaluate the hypothesis of the age-related maturation of cerebrovascular function. Forty years of age was used as a cutoff as the literature shows that there are potentially more unfavorable outcomes across the age groups centered on 40 years with persons <40 years likely to experience good recovery unlike persons >40 years. 49 -51 For comparison of physiology metrics for the age trichotomization and decades of age scheme, Kruskal-Wallis testing and FDR testing were used.
Finally, we evaluated physiologic signal co-variance between age and sex groups using various exploratory clustering techniques: Agglomerative Hierarchical Clustering (AHC), K-means Clustering Analysis (KMCA), K-Medoids/Partitioning Around Medoids (PAM), and Principal Component Analysis (PCA). These four clustering techniques were conducted on male physiology, female physiology, age <40 years physiology, age 40-60 years physiology, and age >60 years physiology for the first 72 h and entire recording period. Such clustering analytics in cerebral physiologic signal analysis in TBI have been pioneered by our group, 52 -54 with detailed descriptions beyond the scope of this paper. We refer the interested reader to the referenced literature for details, and the brief primers on select clustering techniques provided in Appendices B and C of this manuscript.
Further, to confirm the association between PRx, PAx, and RAC metrics on dichotomized outcomes (based on Glasgow Outcome Scale [GOS] score at 6 to 12 months post-injury: Dead = GOS of 1, Alive = GOS of 2 to 5, Unfavorable = GOS of 1 to 3, and Favorable = GOS of 4 or 5), when adjusting for standard variables known to predict outcome in moderate/severe TBI (i.e., age, Marshall CT grade, GCS Total [used instead of motor score due to more complete data for total score), pupil response (i.e., IMPACT Core + CT type variables), we performed multi-variable logistic regression analysis, comparing the IMPACT Core model (and Core + Marshall CT), evaluating area under the receiver operating curve and accounted variance in outcome prediction (Nagalkerke's Pseudo-R 2 ). Finally, to evaluate the impact of outcome status on the relationships between age and sex and cerebrovascular reactivity, we performed sub-group analysis for the following groups-based outcome dichotomization at 6 to 12 months post-injury: alive only, dead only, favorable only, and unfavorable only. All of these results are reported in Appendices D through ZE.
Results
Patient demographics
Two hundred and eighty-three patients (122 from the University of Calgary, 86 from the University of Manitoba, and 75 from the University of British Columbia) were identified as eligible for the study; 224 males and 59 females with a median age of 38 (IQR: 24.0-53.3) years. All patients suffered moderate (GCS score 9-12) to severe TBI (GCS score <9) requiring ICU admission, with a median GCS score of 6 (IQR: 3.0-7.0). The median time to ICP monitor placement from presentation was noted to be 12 h and 15 h at two of the three centers which actively collect this data, with the third site having monitors placed within 24 h in the vast majority of patients. Table 1 shows a summary of general patient demographics in means/medians. Also, a summary of medians and IQRs of recorded cerebral physiology during the acute phase (i.e., first 72 h) and the entire recording period can be found in Table 2.
Patients Demographic Information
CT, computed tomography; EDH, epidural hematoma; GCS, Glasgow Coma Scale; IQR, interquartile range; SD, standard deviation; tSAH, traumatic subarachnoid hemorrhage.
Cerebral Physiology for the 1st 72 h and Entire Recording Period
a.u., arbitrary units; CPP, cerebral perfusion pressure; ICP, intracranial pressure; IQR, interquartile range; MAP, mean arterial pressure; PAx, pulse amplitude index; PRx, pressure reactivity index; RAC, correlation (R) between slow-waves of AMP (A) and CPP (C); RAP, compensatory reserve index; %, percentage.
Daily physiologic insult burden
To gain a better understanding of the degree of impaired cerebrovascular reactivity seen in this cohort of patients, we analyzed the % time of index impairment daily over the first week of their ICU stay. Generally, it can be seen that over the first week, ICP and CPP were well controlled with limited time spent above thresholds and within the guideline suggested ranges (ICP 7-20 mm Hg and CPP 60-70 mm Hg). 42,46 Most patients spent the first week of their ICU stay with a daily PRx value above 0 and +0.25 for the majority of each day. Figure 1 shows boxplots for the first 7 days, highlighting % time with ICP >22 mm Hg (Fig. 1A), mean CPP (Fig. 1B), % time with PRx >0 (Fig. 1C), and % time with PRx > +0.25 (Fig. 1D).
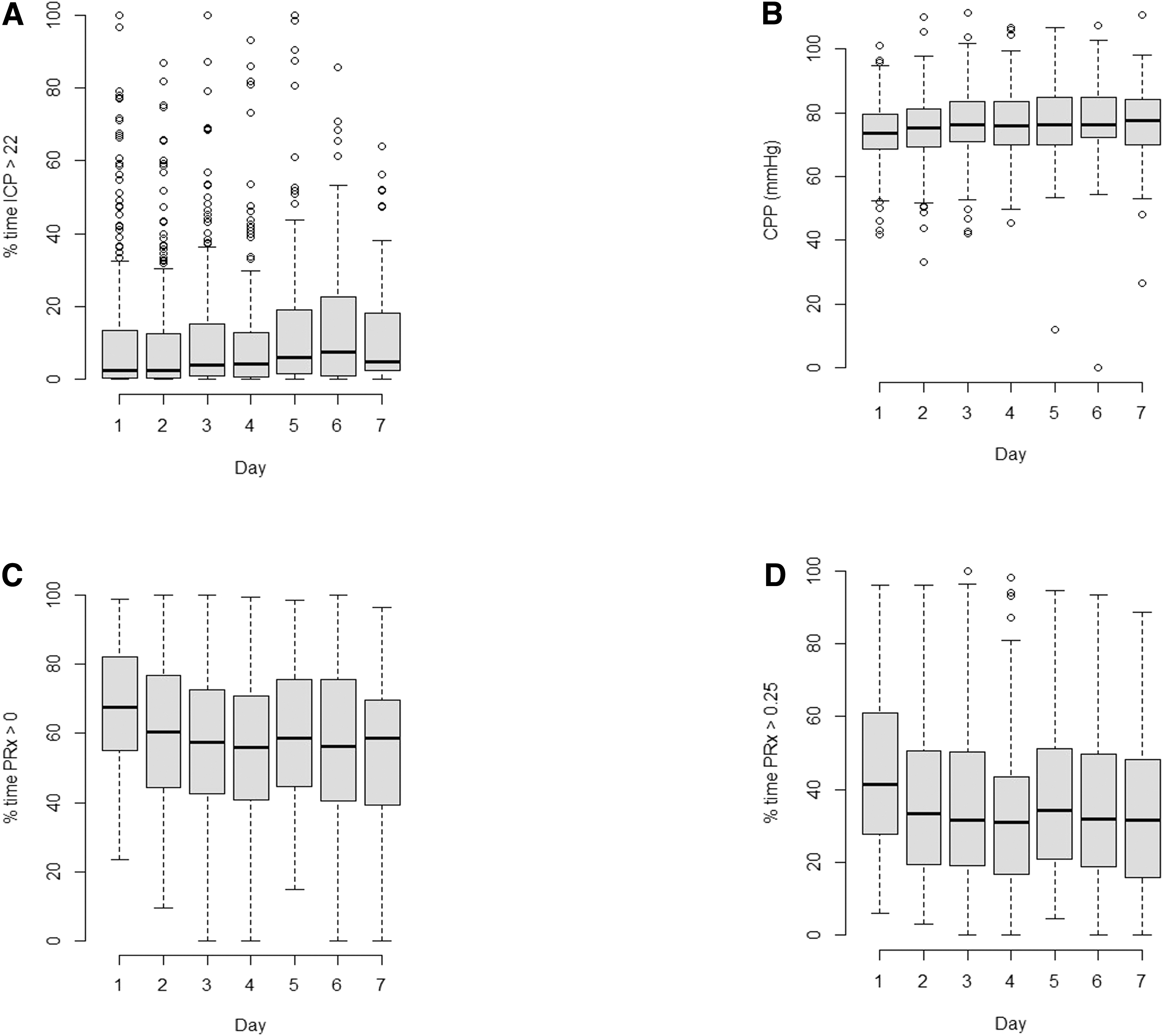
Boxplots of daily recordings of the first 7 days: % Time ICP >22 mm Hg, Mean CPP, % Time PRx >0 and % Time PRx > +0.25.
Cerebrovascular reactivity—impact of biological sex
Male and female patients were compared to evaluate the differences in physiological responses based on biological sex. Table 3 shows medians/IQRs, Mann-Whitney U and FDR p values, comparing the median physiological variables between males and females for the first 72 h of recorded data. In Appendix A, a comparable table is shown with similar results for the entire recording period. There was no statistically significant difference in cerebrovascular reactivity between the sex groups on Mann-Whitney U testing, regardless of recording period evaluated. Also, there were no differences in markers of TBI severity (age, GCS, GCS-M, Rotterdam Grade, Marshall Grade) between males and females.
Cerebral Physiology Based on Biological Sex: Medians/IQRs and Mann-Whitney U Testing: 1st 72 h of Recording
a.u., arbitrary units; CPP, cerebral perfusion pressure; FDR, false discovery rate; ICP, intracranial pressure; IQR, interquartile range; MAP, mean arterial pressure; PAx, pulse amplitude index; PRx, pressure reactivity index; RAC, correlation (R) between slow-waves of AMP (A) and CPP (C); RAP, compensatory reserve index; %, percentage.
Cerebrovascular reactivity—impact of age—linear regression
Linear regression was used to evaluate the relationship between cerebrovascular reactivity and age. ICP, CPP, and PRx failed to demonstrate a significant linear relationship with age (non-significant after correction for multiple comparisons). However, the AMP-derived metrics (PAx and RAC) yielded a statistically significant relationship with age. An example is shown in Figure 2 of scatterplots and linear regressions presented with 95% CI for the first 72 h of recording, with similar findings for the entire recording period (see Appendix A).

Scatterplots and linear regression (first 72 h of recording): % Time ICP >22 mm Hg vs. Age, Mean CPP vs. Age, % Time PRx > +0.25 vs. Age, and % Time PAx > +0.25 vs. Age.
Cerebrovascular reactivity—impact of age—categorical analysis
The relationship between age and cerebrovascular reactivity was further interrogated through categorical organization of age, using age trichotomization and analysis by decades of age. Table 4 provides the trichotomization of age subgroup analysis and Table 5 provides the decades of age subgroup analysis for the first 72 h of recording, highlighting medians/IQRs across each age group, Kruskal-Wallis and FDR p values. Data for the trichotomization and decades of age analyses for the entire recording period are shown in Appendix A, with similar findings for both recording periods.
Cerebral Physiology Association With Trichotomized Age (Age <40, Age 40 -60, Age >60): Medians/IQRs, Kruskal-Wallis and FDR Testing for 1st 72 h of Recording
Bolded p values indicate those reaching statistical significance on Kruskal-Wallis and FDR testing.
a.u., arbitrary units; CPP, cerebral perfusion pressure; FDR, false discovery rate; ICP, intracranial pressure; IQR, interquartile range; MAP, mean arterial pressure; PAx, pulse amplitude index; PRx, pressure reactivity index; RAC, correlation (R) between slow-waves of AMP (A) and CPP (C); RAP, compensatory reserve index; %, percentage.
Cerebral Physiology Association With Decades of Age Subgroups (Age <30, Age 30-39, Age 40-49, Age 50-59, Age 60-69, Age >69): Medians/IQRs, Kruskal-Wallis and FDR Testing for 1st 72 h of Recording
Bolded p values indicate those reaching statistical significance on Kruskal-Wallis and FDR Testing.
a.u., arbitrary units; CPP, cerebral perfusion pressure; FDR, false discovery rate; ICP, intracranial pressure; IQR, interquartile range; MAP, mean arterial pressure; PAx, pulse amplitude index; PRx, pressure reactivity index; RAC, correlation (R) between slow-waves of AMP (A) and CPP (C); RAP, compensatory reserve index; %, percentage.
Age trichotomization and decades of age analyses revealed in both data sheets, a statistically significant worsening of cerebrovascular reactivity, as assessed by PAx and RAC, with increasing age category, as assessed through Kruskal-Wallis testing. This was the case with age trichotomization for mean PAx (p = 0.0002), % Time PAx > 0 (p = 0.00005), % Time PAx > 0.25 (p = 0.000007), mean RAC (p = 0.0002), % Time RAC > −0.10 (p = 0.0001), % Time RAC > −0.05 (p = 0.0001) and admission Marshall CT Grade (p = 0.008) in the 1st 72 hours recording sheet. Also, similar findings were noted with the decades of age analysis where mean PAx (p = 0.0002), % Time PAx > 0 (p = 0.00004), % Time PAx > 0.25 (p = 0.000006), mean RAC (p = 0.0003), % Time RAC > −0.10 (p = 0.0002) and % Time RAC > −0.05 (p = 0.0002) in the 1st 72 hours recording sheet. These all remained significant after FDR testing. It was noted that PRx failed to document such difference. Importantly, this relationship was displayed in the absence of significant differences in injury severity assessed by admission CT grading.
Cerebrovascular reactivity—clustering physiology by age and sex categories
Males, females and trichotomized age subgroups were clustered based on their physiology for both data sheets using AHC, KMCA, PAM, and PCA. Results from these analyses were inconclusive regarding identifying clear subgroup physiology patterns based on age or biological sex. We refer interested readers to Appendices B and C for a few samples of these clustering diagrams from the AHC and PCA analyses.
Outcome association analysis
All details of this extended analysis can be found within Appendices D through ZE of the Supplementary Material. Multi-variable logistic regression demonstrated statistically significant associations between PAx and RAC with both alive/dead and favorable/unfavorable dichotomized outcomes at 6 to 12 months post-injury. Further, we demonstrated an improvement in accounted variance in outcome prediction by up to 8-9% for models with PAx, and 3 to 4% for models with RAC, when adjusting for age, admission GCS, pupillary response and Marshall CT grades. Similarly, when splitting patients into outcome sub-groups (alive only, dead only, favorable only, and unfavorable only), the findings aligned with the above-analysis in that there was no difference in PRx, PAx or RAC between males or females, but trends towards increasing values of PAx and RAC with increasing age. Of note, with progressive sub-group analysis, the number of patients in each category decreased, dropping the statistical power.
Discussion
This CAHR-TBI multi-center study has shown some novel findings and at the same time validated some earlier results from a small exploratory analysis done on the topic. 16 This TBI cohort involves 224 males and 59 females, making it one of the largest multi-center high-resolution cerebral physiologic data sets in moderate/severe TBI. Relationships between cerebrovascular reactivity and both age and biological sex were similar regardless of whether the first 72 h or entire recording period were utilized. Analysis of the first 7 days using boxplots (Fig. 1) of the daily summaries of the patients' ICU stay showed that acute management indices of ICP and CPP were well controlled according to the BTF normal ranges. 42 With regard to the burden of impaired cerebrovascular reactivity, it can be seen from these boxplots that over the first 7 days of the ICU stay, patients spent most of each day in a state of impaired cerebrovascular reactivity despite adequate control of acute management parameters. Relatively similar findings were demonstrated by Batson and colleagues 16 and Zeiler and colleagues. 10,55
With regard to the association between cerebrovascular reactivity and biological sex, our current study failed to document a significant difference. With reference to Table 3, biological sex comparison between males and females for the first 72 h of recording showed no statistically significant difference between the physiology. These findings are in keeping with previous work from the Winnipeg Acute TBI Laboratories. 16 Nevertheless, these results are in contrast to two studies by Czosnyka and colleagues, where PRx was found to be worse in females compared with males, p = 0.02236 and PRx was found to be worse in females compared with males <50 years old, p < 0.05. 33
However, sex-related findings throughout the literature has been limited and largely inconclusive, 22,33,56,57 requiring future research involving serum hormone/cerebrospinal fluid analysis (CSF). 39,58 We understand the vasodilatory benefits of the sex hormones in pre-menopausal women and the vasoconstrictive effects suffered by post-menopausal women and men due to PGI2 and TXA2 cerebral effects, respectively. 30,31 From animal models it is seen that these hormones provide added benefits of reduced neural loss, improved neurophysiologic and functional outcomes in the case of progesterone. 59,60 Also, estrogen plays an anti-inflammatory role in protecting the vasculature by decreasing leukocyte adhesion, attenuating angiotensin II/reactive oxygen species (ROS) response and decreasing inducible nitric oxide synthase in response to inflammatory processes. 31,61 Future multi-center prospective analyses must continue in this area involving hormonal, serum/CSF, inflammatory profiles and pre- vs. post-menopausal sub-analyses in order to benefit neurotrauma care.
The relationship between age and cerebrovascular reactivity validated and highlighted some important findings. Age is a very important prognostic marker in TBI. 25,51,62 A study by Xing and colleagues, the first of its kind, showed that in the aging brain pre-TBI, findings point towards the presence of age-related reductions in ABP, heart rate (HR) and CBF variability in the low frequency ranges and deranged cardiac baroreflex sensitivity (BRS) and dynamic cerebral autoregulation. 63 Additionally, augmented ABP and CBF variability during sit–stand maneuvers in the elderly show reduced cardiovascular regulatory capacity and amplified hemodynamic strain on the cerebral circulation with aging which can leave one prone to cardio- and cerebrovascular diseases. 63 These occur as the aging process causes loss of elasticity and gradual stiffening of the vessel walls from inflammation, calcification, etc. 64
Aging contributes to diminished cerebral capillary density, distortion of the microvascular wall, smooth muscle degeneration in the vessel walls, endothelial dysfunction, elevated cerebral blood flow velocity (CBFV) pulsatility, elevated microvascular resistance, etc. 63,65 –69 Aging also causes cardiovascular changes where diastolic CBFV is reduced more than systolic causing augmented pulsatility which in turn can cause increase in cerebral vascular resistance and remodeling of the vessels leading to eventual microcirculatory damage and small vessel disease. 63,65 –69 All of the above highlighted aging processes in a pre-TBI brain pertain in one way or another to sustained vascular constriction, increases in cerebrovascular resistance and can contribute to increased AMP and reduced ability to generate critical ICPs. In theory, it would make sense that it would impact AMP and thus PAx and RAC; however, how much of this contributed to the superior performance over PRx, remains unquantifiable and unclear at the moment.
Through linear regression and categorical analysis (i.e., age trichotomization and decades of age), we were able to demonstrate worse cerebrovascular reactivity with advancing age. However, contrary to prior literature, 25 PRx failed to document this association. Only AMP-based cerebrovascular reactivity metrics, PAx and RAC, were able to detect this relationship. Such findings validate previous work on the topic 16,35 and are in keeping with the general sentiment that cerebrovascular function deteriorates with advancing age in moderate/severe TBI populations. 18,19,21,25,70,71 Superior performance of PAx and RAC could be explained by the fact that ICP was low and well-controlled in our cohort. 19 Thus, in elderly patients with progressive cortical atrophy and well-controlled ICP, AMP-based cerebrovascular reactivity metrics appear better positioned to monitor/detect impaired reactivity. This is an important finding that has yet to be documented in the literature, and highlights the potential importance of these alternative ICP-based cerebrovascular reactivity measures. 17 -19 To shed further light on the true relationships between cerebral physiology and cellular/biological aging, future work should involve the use of the frailty index, epigenetic applications, etc., to quantify true biological age as opposed to using chronological age. 28,72 –76
Limitations
While this work has validated some important findings, it does not come without limitations. First, the heterogeneous nature of TBI populations must be noted as patients differ in their demographics, treatment regimens, mechanism of injury (based on age group), injury patterns, comorbidities, etc. Common age-related comorbidities knowingly associated with altered cerebral hemodynamics are hypertension, diabetes mellitus, lipid disorders, etc. Their treatment impacts on cerebral hemodynamics data were not collected but it should be a focus for future work. All these and other factors can possibly affect results and outcomes regarding age and sex effects on cerebrovascular reactivity in moderate/severe TBI. TBI is a disease composed of distinct and overlapping phenotypes—diffuse axonal injury (DAI), contusional injury, SDH, EDH, etc. These phenotypes have unique pathophysiologic sequelae, injury patterns and anatomical distribution. As such, the biggest confounder here is the underlying heterogeneous disease patterns. There may be sex or age differences if we were to focus on a homogeneous injury pattern.
Second, although important findings are emerging regarding PAx and RAC, they are not widely described in the literature. These indices are rather new and require more robust work and expertise in highly analytic techniques to achieve future validation and use in neurotrauma care. 35 Our results suggest utility of PAx and RAC in specific subgroups of TBI patients for cerebrovascular reactivity monitoring. Such findings need independent validation and need to be expanded to assess how PAx and RAC may be used for derivation of personalized physiologic targets in TBI (such as optimal CPP).
Third, chronological age may be inadequate in providing the best assessment of true cellular/biological age and its impact on cerebrovascular reactivity. 28,72 –76 Biological age may be a better measure to use via epigenetic techniques based on DNA methylation and histone modification profiles. 28,72 –76 In addition, assessment and incorporation of high frequency pediatric TBI physiological data will help with seeing the full picture of the cerebral vasculature in its immature form and it's responses in TBI and compare/contrast it with findings in the mature and degenerative (elderly) phases. 77 -79
Additionally, cerebrovascular reactivity or CBF control is affected by myogenic mechanism, autonomic nervous system, neurovascular coupling, carbon dioxide/oxygen (CO2/O2) control, cardiac index and medication amongst others. This study's outcomes focusing on the myogenic mechanism of cerebral autoregulation may be altered by the aforementioned CBF control mechanisms not accounted for in this database.
Finally, our analysis of the relationship between cerebrovascular reactivity and biological sex was limited by simple binary male versus female categorization. We did not have access to the hormonal status of the female cohort or designation of pre- versus post-menopausal status. The impact of female sex hormones on cerebrovascular function have been well documented in both health and disease. 30,31,47,59,80,81 Future studies on the impact of biological sex on cerebrovascular reactivity would benefit from quantification of sex hormones and pro-inflammatory cytokine profiles, serially sampled throughout the acute ICU stay and linked with high-fidelity cerebral physiologic data. Future work also requires accurate and complete documentation of time from injury to monitoring placement and recording start. With such information more precision comments on the timeline to cerebral physiologic derangement can occur, and the impact of age/sex on this dysfunction, can be more accurately provided.
Conclusion
Using the CAHR-TBI multi-center data set, we have provided confirmatory findings that advancing age is related to worse cerebrovascular reactivity in moderate/severe TBI. AMP-based indices—PAx and RAC were better at detecting autoregulatory impairment in the elderly and in low ICP states compared with PRx. No clear difference between male and females were detected. Such findings suggest that new emerging alternative ICP-based indices of cerebrovascular reactivity monitoring may play an important role in secondary brain injury detection in certain subpopulations of TBI patients. Further work is required to better understand the relationship between biological age and sex with advanced multi-modal characterization of cerebrovascular reactivity.
Footnotes
Acknowledgments
FAZ receives research support from NSERC, CIHR, the MPI Neuroscience Research Operating Fund, the Health Sciences Centre Foundation Winnipeg, the Canada Foundation for Innovation (CFI; Project #: 38583), Research Manitoba (Grant #: 3906), the University of Manitoba VPRI Research Investment Fund, and the University of Manitoba MPI Professorship in Neuroscience.
AG is supported through the University of Manitoba Clinician Investigator Program, the University of Manitoba Dean's Fellowship, the Manitoba Medical Services Foundation Research and Education Fellowship, the R. Samuel McLaughlin Research Fellowship, and a Canadian Institutes of Health Research (CIHR) Fellowship (Grant #: 472286).
LF is supported through the University of Manitoba - Department of Surgery GFT Research Grant, the University of Manitoba - University Research Grant Program (URGP), and the Biomedical Engineering (BME) Fellowship Grant at the University of Manitoba.
EPT acknowledges funding support from Strategic Research Area Neuroscience (StratNeuro, Karolinska Institutet), The Erling-Persson Family Foundation and Region Stockholm Clinical Research Appointment (ALF Klinisk Forskare, FoUI-955376).
Funding Information
This work was directly supported through the Natural Sciences and Engineering Research Council of Canada (NSERC) (DGECR-2022-00260 and RGPIN-2022-03621) and the Manitoba Public Insurance (MPI) Neuroscience Research Operating Fund.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Appendices A to ZE
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.