
Abstract
Epidural spinal cord stimulation (eSCS) of the lower thoracic spinal cord has been shown to partially restore volitional movement in patients with complete chronic spinal cord injury (cSCI). Combining eSCS with intensive locomotor training improves motor function, including standing and stepping, but many patients with cSCI suffer from long-standing muscle atrophy and loss of bone mineral density, which may prohibit safe implementation. Safe, accessible, and effective avenues for pairing neuromodulation with activity-based therapy remain unexplored. Cycling is one such option that can be utilized as an eSCS therapy given its low-risk and low–weight-bearing requirement. We investigated the feasibility and kinematics of motor-assisted and passive cycle-based therapy for cSCI patients with epidural spinal cord stimulation. Seven participants who underwent spinal cord stimulation surgery in the Epidural Stimulation After Neurologic Damage (E-STAND) trial (NCT03026816) participated in a cycling task using the motor assist MOTOmed Muvi 300. A factorial design was used such that participants were asked to cycle with and without conscious effort with and without stimulation. We used mixed effects models assessing maximum power output and time pedaling unassisted to evaluate the interaction between stimulation and conscious effort. Cycling was well-tolerated and we observed no adverse events, including in participants up to 17 years post–initial injury and up to 58 years old. All participants were found to be able to pedal without motor assist, which primarily occurred when stimulation and effort were applied together (p = 0.001). Additionally, the combination of stimulation and intention was significantly associated with higher maximum power production (p < 0.0001) and distance pedaled (p = 0.0001). No association was found between volitional movement and participant factors: age, time since injury, and spinal cord atrophy. With stimulation and conscious effort, all participants were able to achieve active cycling without motor assistance. Thus, our stationary cycling factorial study design demonstrated volitional movement restoration with eSCS in a diverse study population of cSCI participants. Further, motor-assist cycling was well-tolerated without any adverse events. Cycling has the potential to be a safe research assessment and physical therapy modality for cSCI patients utilizing eSCS who have a high risk of injury with weight bearing exercise. The cycling modality in this study was demonstrated to be a straightforward assessment of motor function and safe for all participants regardless of age or time since initial injury.
Introduction
Spinal cord injury (SCI) is associated with a broad array of long-lasting secondary health consequences that affect nearly all aspects of patients' lives—including motor, sensory, cardiovascular, urinary, bowel, and sexual function. In the past decade, many small cohort studies have demonstrated that epidural spinal cord stimulation (eSCS) can restore limited volitional motor control and improve autonomic nervous system function, even after motor and sensory-complete SCI. 1 –4 While encouraging, these small cohorts have limited representation of the larger SCI population, which is generally older and further out from their initial injury. More diverse and representative participation is needed to understand which individuals with SCI would benefit from eSCS. The variety of rehabilitation modalities is limited as well, with most studies to date focusing on adjusting stimulation parameters. Previously, the ESTAND trial reported that participants with chronic SCI (cSCI) were able to recover motor activity immediately after implantation and over time as demonstrated by electromyography (EMG). 4,5 In this study, we further explore the impact of patient demographics and the utility of alternative low weight-bearing exercise to characterize functional movement.
Previously reported outcome metrics used in eSCS studies have typically focused on functional outcomes, such as steps taken, and electrophysiology (i.e., EMG) to characterize muscle activity. Muscle contractions recorded by EMG are limited by extensive background noise and cannot characterize full limb movement, nor can they in isolation determine if the movement is functional. 4 Overground walking distance during body weight–supported treadmill (BWST) training as an outcome measure represents functional movement but may not be achievable early in eSCS therapy for cSCI patients with advanced age or atrophy, requiring significant supervision and/or facilitation limiting its generalizability. 1 With the expansion of the proportion of individuals living with chronic SCI who could benefit from functional improvement with eSCS, safety and practicality must be optimized when choosing therapy modalities in research and in clinic.
Motor-assist cycling is ubiquitous and commonly used for SCI rehabilitation and exercise-based therapy. 6 It is accessible to most patients after SCI in a variety of therapy settings. 7 The simple kinematics of cycling makes measuring movement quality manageable with limited staff and training, increasing internal validity and reproducibility. Cycling also has merit as a proven SCI rehabilitation modality. The benefits of functional electrical stimulation (FES) cycling to cardiovascular fitness and body composition are well known, 8,9 and volitional arm ergometry has shown superiority to BWST in peak oxygen uptake, a marker of cardiorespiratory fitness. 10 Further motor-assist cycling has also shown to be a generally safe rehabilitation modality. 7 Users are not required to bear full body weight in complete extension during cycling or during transfer in and out of the exercise equipment, providing a theoretically safer alternative for those at high risk of fracture due to SCI-induced osteoporosis. The risk of injury during full or partial weight bearing limits the number of people with SCI who could participate in BWST as a safe modality. 1,2,11 A seated activity such as cycling avoids a fall-from-standing fracture scenario and is theoretically safer.
External validity of eSCS research increases by utilizing a safe modality for movement assessment allowing for inclusion of individuals who cannot undergo BWST training due to significant risk factors for poor bone health. Inclusion of a diverse set of participants also allows for exploration of the impact of non-modifiable patient demographic factors on potential clinical utility of eSCS and functional movement recovery, which has not been explored extensively. The well-known safety profile of cycling allows more comprehensive assessment of the functional movement capacity in a diverse participant pool with decreased risk of injury.
Beyond a research tool, motor-assist cycling also has potential as an intermediary training modality between eSCS implantation surgery and weight-bearing stand and step training for those with cSCI and severe musculoskeletal atrophy. Despite these potential benefits, there is limited information regarding cycling following eSCS implantation. A single study has assessed cycling in eSCS on a few individuals using a hand-leg motor-assist cycle, showing EMG activity in the legs with the epidural stimulator on. 2 No study has assessed cycling ergometry with a leg-powered cycle. We conducted a pilot study to assess safety and feasibility of motor-assist cycling in individuals with cSCI receiving continuous eSCS therapy. We hypothesized that active, continuous eSCS therapy would allow participants with motor complete paraplegia to perform volitational cycling.
Methods
Study population
We studied a consecutive, convenience sample of participants enrolled in the ESTAND study who completed one or more motor-assisted cycle assessments. Details of the ESTAND study, including details of surgical implantation and assessment of cord atrophy by magnetic resonance imaging, have been previously reported. 4 Briefly, individuals with chronic traumatic SCI (greater than 1 year since injury) were recruited for the ESTAND study if they met the following criteria: greater than 22 years of age, motor complete ASIA Impairment Scale classification A or B with a neurological level of injury between C6 and T10, full arm and hand strength, and intact segmental reflexes below the level of injury. Participants were excluded if they had medical or psychological comorbidities that would significantly increase the risk of operation, severe dysautonomia with large (> 20 mm Hg) inappropriate variations in systolic blood pressure during the tilt table procedure, severe contractures, unhealed pressure injuries, recurrent urinary tract infection, unhealed spinal fracture, recent botulinum toxin use, or pregnancy. Nine participants were enrolled in ESTAND between August, 25, 2017, and May 7, 2019. Of this group, seven participants underwent one or more stationary motor-assist cycling assessments over a 6-month data collection stage between January 10, 2019, and July 9, 2019. The two ESTAND participants not included in this sub-study had already completed all 12 follow ups and were no longer actively participating in the ESTAND study. The study was performed in accordance with local Institutional Review Board approval and U.S. Food and Drug Administration Investigational Device Exemption approval. The study protocol is registered with clinicaltrials.gov (NCT03026816).
Cycling protocol
This sub-study is a single arm, unblinded, factorial study. The original ESTAND protocol did not include a stationary motor-assist cycling assessment. This modality was added after a subset of initial participants demonstrated enough movement to allow for more robust functional assessments during follow-up sessions. The cycle was set-up to collect ergometric data and to record the energy produced by the participant over the assessment trial. Due to the later addition of this assessment, the data capture window relative to time of enrollment for each participant differs based on their relative ESTAND study follow up schedule and what session number they were at when they consented to the cycling assessment. ESTAND participants enrolled after the cycling assessment was implemented were tested at each subsequent ESTAND follow-up after surgery. In total, each participant underwent a cycling functional assessment between one and seven times over a 6-month data collection window. Participants began the cycling protocol at a variable time after initial enrollment in ESTAND and were tested a different number of total times at each visit and throughout the study (see Supplementary Table S1). Randomization of the factorial arms was not performed due to washout effects of stimulation.
The cycling assessment required participants to use their custom-fitted wheelchair, which was brought into close proximity with the MOTOmed pedals. Wheelchair brakes were applied, and participants' feet were lifted from their wheelchair footrest and strapped with Velcro support onto the pedals. Velcro straps were applied around the calves to a fixed support bar similar to an ankle foot orthotic. No other changes in the axle or other aspects of the cycle were made between participants.
All participants were assessed on a MOTOmed Muvi 300 seated cycling ergometer. Every assessment was done in the cycle's motor-assist setting which comprises two possible sub-modes: assisted mode and unassisted mode. In the assisted mode, a motor helps the rider maintain a minimum pedaling speed if they cannot generate sufficient force to pedal on their own; while the motor is engaged, it dynamically varies its speed (rpm) and resistance to allow the rider to do as much of the work as possible. In this manner, the MOTOmed cycle provides the participant visual and motion cues to follow. In the unassisted mode, the motor shuts off and the work of pedaling is provided entirely by the rider. Only during unassisted mode (sufficient power applied) does the MOTOmed record ergometry such as power. The bike automatically switches from assisted mode to unassisted mode when it senses the rider generating at least 20 Newtons (N) of force input. If the rider's force input falls back below that 20 N for any reason, the bike automatically switches back to assisted mode with motor on. The threshold of 20 N was empirically derived by the research team using a calibrated force plate and healthy volunteers.
Participants were assessed once monthly at their ESTAND follow up visits at the research facility. During these cycling assessments, participants completed a minimum of four individual two-minute cycling trials. The 2-minute cycling trials followed a 2 × 2 factorial design (see below) of stimulation off (stim -) compared with stimulation on (stim +), each with and without conscious effort to pedal (active or passive).
The four trial types completed at every monthly assessment were: [Stim -, Passive], [Stim -, Active], [Stim +, Passive], [Stim +, Active]. For the passive (effort -) trials, participants were asked to relax and contribute no effort to the motor assisted cycling program. For the active (effort +) trials, the participants were asked to consciously attempt to pedal.
Stim/Stim +: The implanted stimulator is turned on
No Stim/Stim -: Implanted stimulator is turned off
Active/Effort +: Participant makes a conscious effort to pedal
Passive/Effort -: Participant makes no conscious effort to pedal
Assisted/Assisted Mode: Participant does not generate an active pedaling force of 20N or more and the cycle uses a motor to move their legs through the range of motion. Pedaling is driven by the bike with the participant contributing less than 20N force input.
Unassisted/Unassisted Mode: Participant does generate an active pedaling force of 20N or more and the cycle motor is inactive. Pedaling is entirely driven by the participant.
Effort provided by the participant was an important variable to allow assessment of volitional movement vs spastic (involuntary) movement. The passive trials provided a baseline level of participant spasticity to compare to trials where the participant was asked to intentionally move. If there were any technical and/or procedural issues during a trial the participant would be given time to rest and then asked to repeat that individual trial. For some participants, additional trials were also added at a single visit, outside the typical four, to assess the effect of varying unassisted cycling motor speeds or stimulator settings. The stimulation parameters (frequency, pulse width, amplitude, and paddle pattern) for each discrete follow-up session are determined from preference optimization as reported for the previous month, as dictated by the larger ESTAND study protocol. 4
Statistical analysis
During every assessment the stationary cycle collects a variety of quantitative data, including trial duration (seconds [sec]), assisted and unassisted mode duration (s), assisted and unassisted distance traveled (meters [m]), assisted and unassisted mode average speed (rotations per minute [rpm]), work done in unassisted mode (kilojoules [Kj]), and average and maximum power while in unassisted mode (watts [W]). In each assessment, the test proctor also documented the stimulation parameters used, assisted phase motor speed, and pedal resistance used. The primary outcome measures for this study are the proportion of trial total time (2-min trial) spent in unassisted mode and the maximum power generated during unassisted mode. Metrics chosen to characterize the sustainability and the strength of the movements documented in unassisted mode across all trials.
Due to the heterogeneous sampling in this cross-sectional study and lack of independence of the pooled trial data between follow-ups and participants, we used a mixed effects linear model. The random intercepts were follow-up number nested into each participant identification number. Further information regarding random effects is detailed in the Supplementary Files and Supplementary Figures S1 and S2. The fixed effects were stimulation, effort, and their interaction, as well as additional variables of interest including age, years post-injury, spinal cord atrophy above and below the injury, and the number of days post-surgery. The dependent variables included the portion of the test in unassisted mode (unassisted duration/total trial duration) and maximum power in unassisted mode. An alpha of 0.05 was used as the threshold for statistical significance. No imputation method was used for missing data, and incomplete factorial elements were included in the mixed models.
Data analysis was performed in R version 4.2.0. Packages lme4 (version 1.2.29) and sjPlot (version 2.8.10) were used to generate and visualize the mixed models and figures, respectively.
Results
Participant demographics
Six participants had complete paraplegia (AIS classification A) and one participant had motor-complete paraplegia (AIS classification B), with injury sites ranging from T4 to T8 (Table 1). At the time of enrollment, the participants were 26- to 58-years-old (average: 38.3, standard deviation [SD]: 9.96) and 3 to 17 years post-SCI (average: 7.10, SD: 4.88). Six participants were male and one was female. Of 36 follow-up sessions across the six participants, six sessions had incomplete factorial data due to technical limitations with data collection.
Decade, Gender, Years Post-Injury, and Injury Level at Time of Surgery for Study Participants
The neurological level of injury is derived from the International Standards for Neurological Classification of Spinal Cord Injury revision 2019.
F, female; M, male.
Threshold assessment of volitional movement
All participants were able to cross the 20 N force threshold to enter unassisted mode in at least one trial with the combination of stimulation on and active effort Supplementary Table S2. Multiple participants produced 20 N or more force during trials with stimulation off and active effort (Active-Off; Supplementary Table S2). Participant 02 passed this threshold in the highest percentage of total trials, entering unassisted cycling mode (producing 20 N or greater of force) on 50% of active (effort) trials with stimulation off. Additionally, multiple participants produced 20 N or more of force during trials when asked to put forth no effort to move (Passive-Off and Passive-On; Supplementary Table S2).
Proportion of trial in unassisted bike mode
During each trial, the MOTOmed cycle recorded the duration the participant spent in assisted mode (motor on, participant force input less than 20 N) and in unassisted mode (motor off, participant force input 20 N or more). The proportion of the total trial duration (2-min trial) spent in unassisted mode (motor off) was calculated using this data. The proportion of time spent in unassisted mode (motor off, participant force input 20 N or more) during the trial grouped by stimulation and effort is shown in Figure 1, with individual participant variation shown in Supplementary Figure S3.

Violin, whisker, and jittered data plots of the proportion of time spent in unassisted mode between the four possible combinations of stimulation present (Stim +, Stim -) and conscious pedaling effort from the participant (Effort +, Effort -).
The maximum power generated during each trial grouped by stimulation and effort is shown in Figure 2, with individual participant variation shown in Supplementary Figure S4. Where the portion of time spent in unassisted mode describes the ability of participants to sustain movement, the maximum power (watts) produced at any point during the unassisted mode of the trial reflects the strength and coordination of the movement. Power data is only collected during the unassisted mode of the trial, as the assisted mode portion of the trial has a constant speed and power production determined by the active motor. Therefore, the watts produced in unassisted mode are produced by the participants pedaling without assistance.
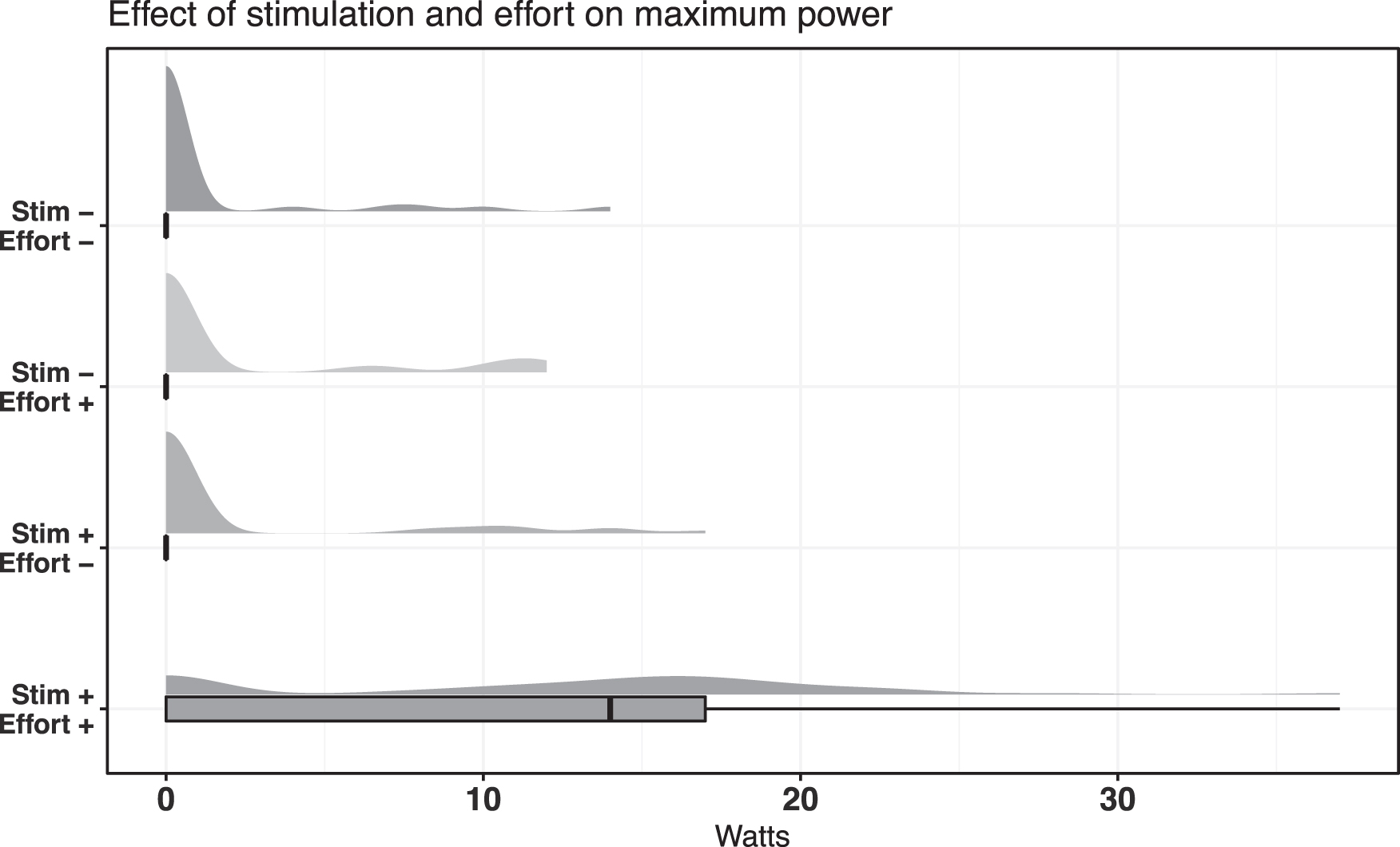
Violin, whisker, and jittered data plots of the maximum power generated in unassisted mode between the four possible combinations of stimulation present (Stim +, Stim -) and conscious pedaling effort from the participant (Effort +, Effort -).
Estimates from each model describe the independent effect of each variable on unassisted pedaling and maximum power produced in watts (Fig. 3). The combination of stimulation and conscious effort from participants produced the greatest positive estimate (+ 0.23) and was the only statistically significant contribution (p = 0.002). A ceiling effect of measuring the duration of active cycling was noted when participants' ability to activate the unassisted-cycling mode (20 N force input by the participant) encompassed the entire trial (2 min). Therefore, the paired outcome of maximum power was also required for further comparison between these cases. The combination of stimulation and conscious effort from participants had the greatest positive estimate on maximum power (+ 8.85 W) and was also statistically significant (p < 10−5).

There were no adverse events noted during the cycling trials, and there were no issues with participants engaging the device. All patients tolerated the stimulation and cycling without any adverse events. An example trial of motor assist cycling with and without stimulation is shown in Supplementary Videos S1 and S2.
Discussion
This study explores the feasibility and safety of motor-assist cycling for individuals with motor-complete cSCI after implantation of eSCS in the E-STAND clinical trial. Cycling was well-tolerated without any adverse events. With active, continuous stimulation and conscious effort, all participants were able to cycle without motor assistance. Our stationary cycling factorial study design demonstrated volitional movement restoration with eSCS in a diverse study population of cSCI participants.
The demographics and medical characteristics of this participant sample are diverse in comparison to other current eSCS studies. On average, people with spinal cord injury are 43 years old at initial injury and are 9 years post-injury. 12,13 Other eSCS trial cohorts have an average age of 27-31 years and an average time since injury of 6.1-6.3 years. 14,15 Participants in this study have a mean age of 38 years (SD 9.96) and a mean time since initial SCI of 7.1 years (SD 4.88). In addition, other eSCS research study cohorts require participants to undergo intensive preparatory rehabilitation, 1 -3 while our study does not. 4 Reduced barriers to participation may explain the increased age and time since injury in our study. In addition, the detection of volitional movement demonstrates that preparatory rehabilitation is not a prerequisite for discernible functional gains as demonstrated here.
The lack of cycling performance differences by age, time since injury, spinal cord atrophy, and time since eSCS initiation may be due to the small sample size, but as the demographic variation of participants was broad, the small confidence intervals of the predictors aside from atrophy suggest that volitional movement with eSCS may be possible across a wide demographic range. All participants—including the ones with advanced age and time since injury—had some amount of cycling in unassisted mode and power generation when consciously trying to pedal with continuous eSCS active. Future eSCS research may benefit from broader inclusion criteria to better understand what cSCI population may benefit from future eSCS clinical use.
Motor-complete cSCI is associated with decreased bone density and increased impact fractures. 16 Ambulation with epidural stimulation after spinal cord injury carries significant risk, as shown in a recent body weight supported treadmill study: a 26-year-old man with a 2.5 year T4 AIS A SCI sustained a spontaneous hip fracture after a week of ambulation, further delaying study participation by 1 year. 17 The incidence rate for fragility fracture is 14% in the first 5 years and 39% in the first 15 years of spinal cord injury. 18 Participant 02, 16.8 years from his SCI, theoretically has a threefold risk of hip fracture as the individual who sustained a hip fracture in a similar study. Such participants with long term SCI and/or poor bone health can be excluded from studies of this nature proactively, but such a choice will sacrifice external validity and potential clinical applicability of this intervention. The effect of low impact cycling on bone health in SCI is controversial, 9 but high-volume FES cycling studies have shown an increase in muscle cross sectional area and a decrease in fracture threshold, suggesting that cycling after muscle conditioning may reduce fracture risk by distributing the stress burden to non-bone structures. 19
Beyond the potential benefits as an exercise platform, instrumented cycling provides real-time measurements of a functional movement without stimulation artifact, an important consideration when compared with electrophysiologic outcome metrics in the presence of a tonic source of interference. 4,20,21 Our outcome measures were chosen to characterize the movement in multiple facets and can be reproduced by future cycling research utilizing eSCS. The proportion of the trial spent in unassisted mode assesses sustainability of the participant's movement when the motor is not active and the maximum power generated reports the strength of the movements. Both these qualities of the participants' movements are of interest and are influenced by eSCS settings. Further, cycling data collection provides the possibility of remote stimulator optimization with data collection and training in clinical and home settings. Cycling has potential as an introductory rehabilitation modality or activity-based therapy that can improve exercise tolerance in cSCI patients at a higher risk of fractures 6,22 and potentially reach mobility goals formerly reserved for motor-incomplete spinal cord injury. 23 The long-term effect of the volitional component of this rehabilitation on mobility and tasks of daily living needs further study.
This study adds to the literature by demonstrating functional recovery of volitional movement with eSCS in people with motor-complete cSCI. The significant interaction between stimulation and effort when controlling for other factors is consistent with the theory that the movement generated is an organized volitional response. The factorial design of this study—accounting for both stimulation and intention to move in equal measure—addresses spastic posturing and Jendrassik-type maneuvers that confound volitional movement measures in previous studies that only compared stimulation profiles. 3,21,24 The non-zero values of the outcome measures where participants are not undergoing stimulation or trying to pedal are expected by design—non-volitional lower extremity movement, including spasticity, affects the baseline of any lower extremity task involving sustained momentum. The technical possibility that the improvement in active cycling and power generation could be due to increased spasticity was considered, but this was found to be unlikely, given previous evidence in multiple studies that stimulation decreases spasticity, 25,26 making the possibility that movement under stimulation is direct volitional control of lower limb muscles more likely.
Testing intention to move also uncovers additional properties of eSCS activity. A more recent study directly comparing active and passive BWST stepping found a clinically significant difference in baseline ground reaction force and EMG activity during gait. 27 In one of our previous studies, four participants demonstrated sustained volitional movements in the absence of active stimulation during follow-up. 5
There are several limitations to this study that must be considered when interpreting the data. Motor-assist cycling was added as a study measure after participants were observed performing gross motor movements during Brain Motor Control Assessment protocols. The missing data within each participant visit was evaluated to result from technical issues with following the protocol instead of situations that could cause bias the interpretation of results such as participant discomfort, difficulty following instructions, or inability of the cycling system to interpret data successfully in these cases. However, further studies are encouraged to document the precise reasons for each incomplete factorial trial to mitigate sources of nonrandom bias more reliably. Because of the late implementation of the cycling assessment and the limited data collection window reported in this paper, no participant has completed the cycling protocol throughout their total time in the ESTAND study. Therefore, the between-participant comparison is not robust in determining the factor of duration of study participation on the outcome measures and neuroplastic changes from long term eSCS use is difficult.
In addition, several external factors shape the nature of this volitional movement. Force generated by spasticity may confound the cycling hardware's assessment of active movement. Future data collection should be more sophisticated to measure the magnitude and direction of pedal forces over the cycling period to better characterize this novel movement.
Conclusions
In this study, all participants were able to achieve active cycling with tonic stimulation and conscious effort without motor assistance. Our novel factorial study design utilizing stationary cycling demonstrates supraspinal volitional movement restoration with continuous eSCS in a diverse study population of cSCI participants. We also described useful kinematic measures which can characterize functional movement during cycling exercises in future eSCS research. Age and time since initial traumatic injury to eSCS therapy were not found to significantly impact volitional movement recovery. Further, motor-assist cycling was well-tolerated without any adverse events among all participants, regardless of initial health status and level of conditioning. Cycling has the potential to be a safe research assessment and physical therapy modality for cSCI patients utilizing eSCS who have a high risk of injury with weight bearing exercise.
Transparency, Rigor, and Reproducibility Summary
The study design and analysis plan were preregistered on January 20, 2017, at clinicaltrials.gov (NCT03026816). The analysis plan was not formally pre-registered. Actual sample size was seven participants, and the observed effect size was 23% active cycling during a trial and 8.85 Watts for the active cycling percentage and maximum power generated, respectively. Outcome assessment was unblinded. Data analysis was performed using R 4.2.0. Primary outcome measures were obtained from the MOTOmed Muvi 300 and accompanying software. The findings have not yet been replicated or externally validated. Data and analytic code are available upon request, and the manuscript is open access.
Footnotes
Acknowledgments
We would like to acknowledge Aliya Ahmadi, Dylan Sturtevant, and the rest of the ESTAND team for their contributions in performing the assessments and collecting the data for the study.
Authors' Contributions
Caleb Hoover: methodology, formal analysis, investigation, data curation, writing original draft, review and editing, funding acquisition. Willis Shuerger: software, formal analysis, resources, data curation, review and editing, visualization. David Balser: software, formal analysis, data curation, review and editing, visualization. Patricia McCracken: conceptualization, methodology, validation, investigation, resources, review and editing, funding acquisition. Thomas Murray: statistical analysis, review and editing. Leslie Morse: review and editing. Ann Parr: conceptualization, review and editing, supervision. Uzma Samadani: conceptualization, review and editing, supervision. Theoden Netoff: conceptualization, review and editing. David Darrow: conceptualization, methodology, formal analysis, investigation, resources, writing original draft, review and editing, supervision, project administration, funding acquisition.
Funding Information
This study is funded by a MN State SCI/TBI grant from the Minnesota Office of Higher Education. Devices are donated by Abbott/St. Jude.
Author Disclosure Statement
Dr. Netoff and Dr. Darrow hold equity in and serve as officers for Stim Sherpa, which has licensed optimization IP from the University of Minnesota.
For the other authors, no competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Video S1
Supplementary Video S2
Supplementary Files
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.