
Abstract
The use of biomarkers in spinal cord injury (SCI) research has evolved rapidly in recent years whereby most studies focused on the acute post-injury phase. Since SCI is characterized by persisting neurological impairments, the question arises whether blood biomarkers remain altered during the subacute post-injury time. Sample collection in the subacute phase might provide a better insight in the ongoing SCI specific molecular mechanism with fewer confounding factors compared with the acute phase where, amongst other complications, individuals receive a substantial amount of medication. This study aimed to determine if the temporal dynamics of serum biomarkers of neurodegeneration differ between individuals depending on their extent of neurological recovery in the transition phase between acute and chronic SCI. We performed a secondary analysis of biomarkers in patients with SCI (n = 41) who were treated at a level I trauma center in Germany. Patients with cervical or thoracic SCI regardless of injury severity were included. Blood samples were collected in the acute phase (1-4 days post-injury), and after 30 and 120 days post-injury. Serum protein levels of glial fibrillary acidic protein (GFAP) and neurofilament light protein (NfL) were determined for each time-point of sample collection using R-Plex Assays (Meso Scale Discovery). Linear mixed models were used to evaluate the trajectory of GFAP and NfL over time. Fixed effects of time, neurological recovery, and injury severity, along with the recovery-by-time interaction, were included in models with random slopes and intercepts. GFAP levels increase during the first days after SCI and decrease in subacute to chronic stages. Notably, the trajectory of GFAP over time is significantly associated with the extent of neurological recovery during the transition from acute to chronic SCI with a steeper decline in individuals who recovered better. Serum levels of NfL continue to rise significantly until Day 30 followed by a decrease afterwards, independent of neurological recovery. The trajectory of serum GFAP levels qualifies as a prognostic biomarker for neurological recovery, and facilitates monitoring of disease progression in the sub-acute post-injury phase.
Introduction
Clinical examination of spinal cord injury (SCI) is extremely challenging and often unreliable in the early stages after injury. 1 An objective quantification of injury severity immediately upon admission would be of utmost interest for treating physicians to support clinical decision making from the very beginning. Since the diagnosis of SCI has proven to be difficult already in the acute phase, a prognosis of neurological recovery is even more complicated. Biomarkers that allow a quantification of the lesion severity, as well as a prognosis for recovery would create an avenue to track disease progression, monitor treatment effects of potential novel therapies for SCI, and might also create targets for future pharmacological interventions.
Previous literature postulated that the concentration of neurofilament light protein (NfL) in blood serum, as well as in cerebrospinal fluid (CSF), serves as an objective biomarker for neuro-inflammatory and neuro-degenerative processes in several central nervous system pathologies including multiple sclerosis, brain tumors, traumatic brain injury (TBI), and also SCI. 2 –10
A recent systematic review found 48 publications that reported elevated glial fibrillary acidic protein (GFAP) levels in a variety of neurological disorders including Parkinson's disease, Alzheimer's disease, multiple sclerosis, and glioblastoma among others. 11 Serum levels of both NfL and GFAP are associated with the presence and, more importantly, the activity of gliomas and brain metastases. 9 Interestingly, studies including patients with spinal cord ischemia as a complication of thoraco-abdominal aortic aneurysm repair have shown that CSF levels of GFAP were upregulated before or in parallel to symptom onset. 12,13 This is in accordance with the findings by Ahadi and colleagues, 14 as well as our previous work 7 showing that the serum concentration of GFAP is related to the presence and severity of SCI in the first 24-96 h after traumatic SCI.
Since the secondary injury cascade after SCI lasts for several weeks, 15 the expression of GFAP and NfL over time might provide important information about the molecular mechanisms of SCI.
Previous studies reported elevated levels of GFAP and NfL at different time-point in various neurological conditions. We hypothesized that by investigating the trajectory of GFAP and NfL during the transition period from acute to chronic SCI we will gain a deeper insight in the process of neurological recovery after SCI.
Accordingly, the aim of this study was to evaluate if the trajectory of our chosen biomarkers is associated with recovery of motor and sensory function during the first 4 months after traumatic SCI.
Methods
Eighty-one individuals with acute traumatic SCI were recruited at Trauma Center Murnau (Bavaria, Germany) as part of the prospective Autoantibodies in Spinal Cord Injury Study (
For 38 out of 81 patients, blood samples were collected at three time-points (after 1-4, 30, and 120 days post-injury). Data of these 38 individuals were included in the analysis of this study and the previously published manuscript. 7 For the present study, we excluded one patient who sustained lumbar SCI, and one patient who was already classified American Spinal Injury Association (ASIA) Impairment Scale (AIS) E (normal neurological function in all sub-scores) at the first follow-up 30 days post-injury. Further, we were able to recruit an additional five patients who agreed to participate in the meantime. The total number of patients included in this analysis is therefore 41 (Table 1).
Summary of Subject Characteristics
Independent t-test between better and worse recoverers; bPearson's chi-squared test.
SD, standard deviation; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Blood samples
Two 7.5 mL serum tubes were collected at each time-point of sample collection (Days 1-4, 30, and 120). The serum tubes were stored at room temperature for 45 min followed by 1 h at 4°C, allowing the blood to clot. After that, the blood was centrifuged at 4°C, at 1500 g for 20 min and serum was aliquoted and stored at -80°C until shipped to the laboratory of the Institute of Molecular Regenerative Medicine at the Paracelsus Medical University (Salzburg, Austria) on dry ice for storage and sample analysis.
Analytical procedures
Serum levels of GFAP and NfL were measured by R-Plex singleplex assays (Meso Scale Discovery, Rockville, MD). Measurements were carried out following manufacturer's instructions, including dilution of samples and standards. The same serum aliquot was used for both biomarkers without any freezing and thawing cycles in between. The analytical methods are depicted in detail in the supplementary material of our previous study. 7
Neurological assessment
Motor and sensory function of individuals who sustained SCI was evaluated according to the International Standards for Neurological Classification of Spinal Cord Injury scale (ISNCSCI) by the American Spinal Injury Association. 17 Complete ISNCSCI and its sub-scores (upper extremity motor score (UEMS), lower extremity motor score (LEMS), pin prick sensory score (PP), and light touch sensory score (LT)) were available from all 41 patients at 30 and 120 days post-injury.
Statistical analysis
All statistical analyses and figures were compiled in R (R Core Team, 2018, version 4.0.4 running under: Windows 10 x64). Descriptive statistics for continuous variables and frequency counts for categorical variables were calculated. Pearson's chi-squared tests were applied to test the association between categorical variables. Independent t-tests were used to determine differences in continuous variables.
Temporal evolution of biomarkers during the transition from acute to chronic SCI
To create a measure for neurological recovery, the group was divided into better versus worse recoverers by median Integrated Neurological Change Score (INCS) 18 between the first follow-up 30 days post-SCI and the second follow-up 120 days post-SCI. The INCS allows us to quantify the change in neurological function between two assessments resulting in a value between -1 (worse possible change in the ISNCSCI's LT, PP, UEMS, and LEMS scores) and +1 (full neurological recovery assessable by ISNCSCI). Since less neurological recovery is to be expected in individuals with motor complete lesions, 19,20 we split the cohort by median INCS between 30 and 120 days separately for the groups AIS A+B, AIS C, and AIS D (Fig. 1). ISNCSCI assessments are often incomplete in the acute stages after injury due to concomitant injuries, or a patient's inability to comply with the examination. In order to calculate the INCS for the entire cohort, and because an assessment at a later time-point is considered a more reliable measure of function, 1 we calculated the change between Days 30 and 120.

Integrated Neurological Change Score (INCS) differs upon injury severity according to the American Spinal Injury Association (ASIA) Impairment Scale (AIS). The dashed lines represent the median INCS, which is used as cutoff between better and worse recovery in each group (AIS A + B vs. C. vs. D).
Linear mixed model (LMER) analyses were used to assess differences in serum biomarkers (GFAP, and NfL) across time and between better and worse recoverers. Fixed effects of time, neurological recovery, and injury severity, along with the recovery-by-time interaction, were included in random intercept models, which included random effects for subjects and a random slope for baseline severity using the R package lme4. 21,22 Significance of fixed effects was assessed by F-tests with a Kenward-Roger approximation of degrees of freedom using the lmerTest package. 23
Results
A total of 41 individuals were included in this study. Baseline characteristics were summarized in Table 1. In our cohort, there were no differences in age and sex between worse and better recoverers. There was a tendency for individuals with thoracic lesions to regain less function compared with those with cervical lesions, which could be due to the fact that in our cohort, individuals with thoracic lesions were more severely injured compared with patients with cervical lesions (Table 2). By using the INCS as a cutoff, we were able to discriminate between better and worse recoverers among all AIS grades thereby creating an inclusive study endpoint.
Neurological Level of Injury Versus AIS at Day 30
Pearson's chi-squared test.
AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Linear mixed model analysis revealed a significant effect of severity (AIS D; p = 0.032), recovery (INCS above median; p = 0.02), and a significant recovery-by-time interaction effect for the serum levels of GFAP between Days 1-4 and Day 30 (p = 0.022). The group consisting of patients with better recovery had higher GFAP levels at the first time-point of sample collection (Days 1-4) compared with the worse recoverers (Fig. 2A). Serum concentrations of GFAP decreased after the initial peak with a significantly steeper decline in AIS A, B or C patients with better neurological improvement (Fig. 2D-F). GFAP levels were already quite low 30 days post-SCI in the group of better recoverers [mean (standard deviation [SD]) = 129.4 (145.5) pg/mL], while the mean (SD) serum concentration was still 1715.5 (7330.1) pg/mL in the group of worse recoverers (Fig. 2B). This interaction failed to reach statistical significance for the time period until Day 120 (p = 0.058; Table 3). While F-tests with Kenward-Roger approximation of degrees of freedom showed a significant effect of time for the trajectory of GFAP (p < 0.001), the interaction effect including all three time-points of sample collection (Days 1-4, Day 30, and Day 120) was not significant (p = 0.056). By reducing the LMER to the early injury phase (Days 1-4 until Day 30), the interaction effect in F-tests with Kenward-Roger approximation was statistically significant (p = 0.049) (Supplementary Table S1).
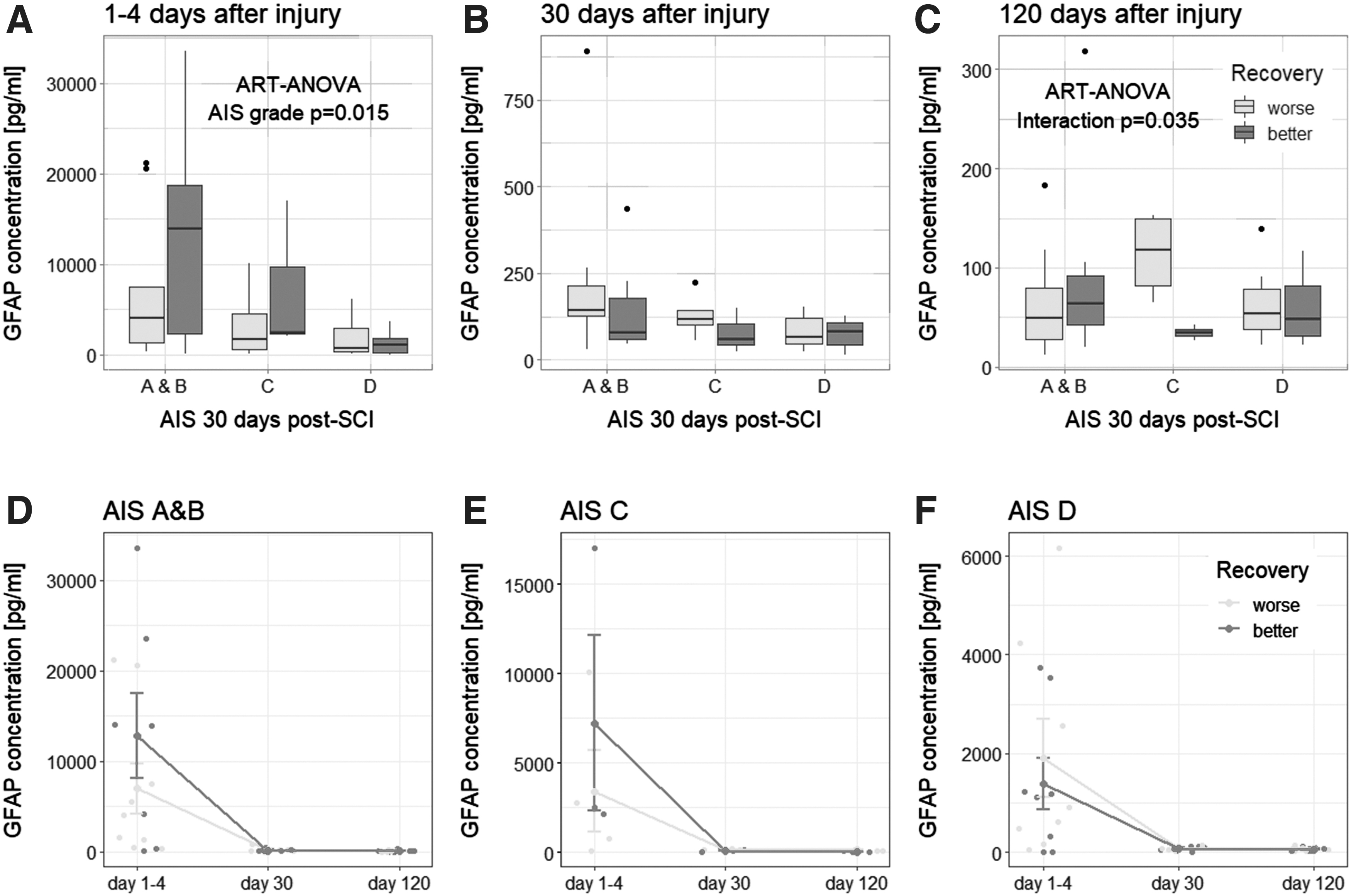
Glial fibrillary acidic protein (GFAP) between better and worse recoverers,
Linear Mixed Model: Serum Levels of GFAP
p < 0.05; ** p < 0.01; *** p < 0.001.
GFAP, glial fibrillary acidic protein; CI, confidence interval; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
LMER also revealed a significant effect of time for the serum levels of NfL between Days 1-4 and Day 30 (p < 0.001). NfL concentration significantly increases within the first 4 weeks after injury independent of neurological recovery (Table 4; Fig. 3), although, lower levels were observed in less severely injured individuals (AIS D; p = 0.001; Table 4; Fig. 3). The fixed effect of injury severity was also significant in F-tests with Kenward-Roger approximation (p = 0.012; Supplementary Table S2).
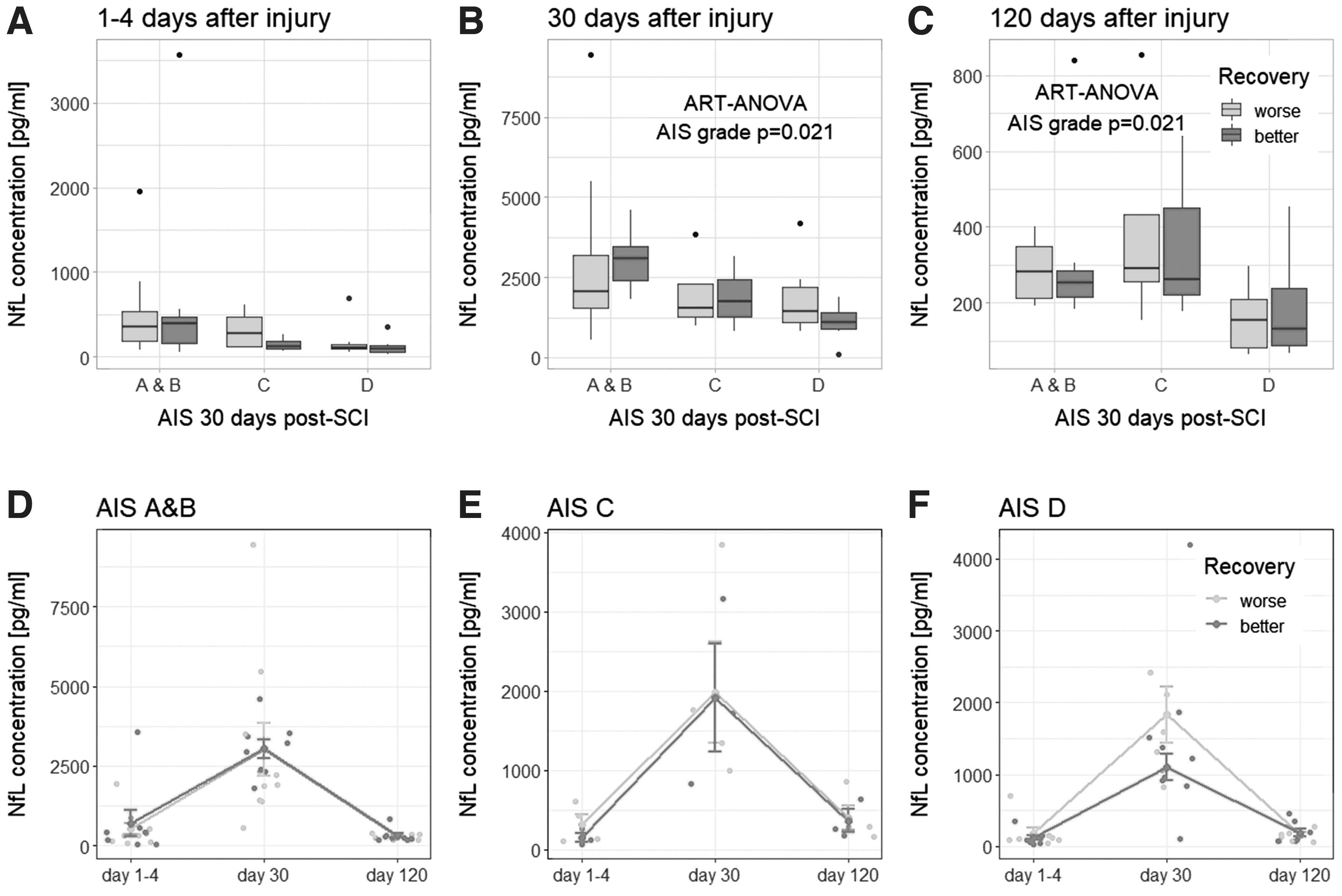
Neurofilament light protein (NfL) between better and worse recoverers,
Linear Mixed Model: Serum Levels of NfL
p < 0.05; ** p < 0.01; *** p < 0.001.
NfL, neurofilament light protein; CI, confidence interval; AIS, American Spinal Injury Association (ASIA) Impairment Scale.
Generally, serum concentrations of both biomarkers, GFAP and NfL, were significantly lower in less severely injured individuals (AIS D) compared with those with AIS A, B, and C lesions (Fig. 2 and Fig. 3).
Discussion
In this study, we focused on the relation between biomarkers and neurological recovery. The three time-points of sample collection (Days 1-4, Day 30, and Day 120) allowed us to assess the longitudinal expression of GFAP and NfL during the transition from acute to chronic SCI. The changes between Days 1-4 and Day 30 reflect the early stages of neurological recovery and are therefore particularly interesting in terms of biomarker evaluation.
Both biomarkers showed a severity-dependent trajectory, with lower levels in less severely injured individuals. We found a significant recovery-by-time interaction effect for trajectory of serum concentrations of GFAP within the first 4 weeks post-injury.
As expected, our data showed a trend towards better neurological recovery in individuals with cervical lesions compared with those with thoracic lesions. Individuals with thoracic lesions are more severely injured (Table 2) and recover less compared with those with cervical lesions (Table 1). This has already been discussed extensively in previous literature. 24 –28 Since injury severity is highly associated with the neurological level of injury (cervical vs. thoracic), and we accounted for severity (by means of AIS) in the linear mixed model analysis as a fixed effect as well as a random slope, we did not distinguish between individuals with cervical versus thoracic lesions in our analysis.
GFAP serum concentrations are significantly higher in individuals with SCI compared with healthy controls within 4 days after injury. 7 Also, previous research found significantly higher serum levels of GFAP in patients with SCI compared with patients with vertebral fractures without SCI 24 h after injury. 14 Additionally, the expression of GFAP in CSF is severity-dependent in the early post-injury period with highest levels during the first 24 to 36 h after SCI. 29 These results indicate, that GFAP is a marker for tissue damage in the early phase after SCI.1 1,14 Our findings coincide with previous literature showing that GFAP is upregulated immediately after injury reaching a peak within few days post-SCI followed by a subsequent decrease to relatively low levels after 4 weeks (Fig. 2).
Interestingly, in our cohort, individuals with better recovery had higher serum levels of GFAP within the first 4 days followed by a significantly steeper decline afterwards compared with worse recoverers (Fig. 2). In the group with worse neurological recovery, GFAP serum concentrations decreased only slightly after 30 days [mean (SD) = 1715.5 (7330.1) pg/mL], while in the group of individuals with better recovery GFAP levels decreased dramatically (mean (SD) = 129.4 (145.5) pg/mL). In patients with better neurological recovery, the levels of GFAP at 30 days decreased to around 1% of those at Days 1-4, while levels in worse recoverers only decreased to around 42% of the initial serum concentrations. The concentration of GFAP levels in serum reflect astrocyte damage or cell death, which is commonly considered to be a passive event. But astrocytes could be also damaged as the result of cell exhaustion after responding to the insult. Thus, the faster recovery of normal GFAP levels in good recoverers might reflect a more effective response of the astrocytes that helps to contain edema and to resolve earlier the ionic and water imbalances due to injury to the cost of losing more astrocytes/astrocyte processes at early time-points, 30 -32 rendering initial higher circulating levels of GFAP. This hypothesis, however, should be explored in future experiments.
While GFAP levels were highest at the first time-point of sample collection (1-4 days post-SCI), serum levels of NfL continue to rise within the first weeks depending on injury severity (Fig. 3). In our previous study, we found that NfL levels are already significantly different between individuals with SCI and healthy controls within the first days after injury. 7 However, an interesting observation from this longitudinal study suggests that the release of NfL into the bloodstream continues and even increases for several weeks after SCI. This supports and extends the findings by Kuhle and colleagues showing that serum NfL levels increased significantly within the first 7 days after SCI. 8 NfL has been proposed to be a marker for ongoing neurodegenerative disease progression. 33 The continued upregulation within the first weeks might be an indicator of ongoing secondary injury processes after SCI. Early NfL increases might reflect neuronal death, 32,34,35 whereas subsequent increases might reflect damage or elimination of neuronal processes during Wallerian degeneration, that takes part from days to weeks after human SCI. 36 -38
To summarize the findings of this analysis, the trajectory of serum concentrations of GFAP within the first 4 weeks after traumatic SCI is related to the extent of neurological recovery in the subsequent 3 months. Individuals with high initial levels of GFAP and a steep decline towards 30 days post-injury regained the most motor and sensory function in our cohort. Since we divided the group into better versus worse recoverers by median INCS separately depending on the initial severity (AIS A+B, C, and D) we were able to control for baseline severity in our analysis. Our findings indicate that the change in GFAP levels within the first weeks post-SCI constitutes a prognostic biomarker for neurological recovery in the sub-acute to chronic stages transition independent of injury severity. This highlights a potential clinical value of measuring acute/subacute GFAP levels to predict the further recovery in the transition period to chronic SCI.
Limitations
The main limitation of this study is that individuals with SCI often also sustain traumatic brain injury (TBI). In our study, concomitant TBI was an exclusion criterion. Biomarkers of neurodegeneration might be confounded by the presence of TBI. Generalizability of our findings is therefore limited to individuals with SCI without concomitant TBI.
Another limitation that has to be acknowledged is that the timing of the first sample collection had a range of 4 days post-injury. Accordingly, our baseline measurement might underlie variations due to the timing of sample collection.
Also, the serum concentrations of NfL showed a peak around Day 30 in our analysis. Yet, we do not know when serum levels reach their true peak. Therefore, future research should consider more frequent sample collection in the transition from acute to chronic SCI to better depict the trajectory.
Conclusion
The trajectory of serum concentrations of GFAP within the first 4 weeks is associated with neurological recovery in individuals with traumatic SCI. Therefore, serum levels of GFAP within the first 4 weeks post-injury qualify as prognostic biomarkers for neurological recovery and facilitate monitoring of disease progression in the sub-acute post-injury phase.
Footnotes
Acknowledgments
Ethics approval: All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the ethics committee of the Ethics Committee of the Bavarian Medical Board. The study was registered on the
Consent to participate: All participants provided written, informed consent.
Authors' Contributions
All authors read and approved the manuscript.
Funding Information
Author Disclosure Statement
No competing financial interest exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.