
Abstract
While socioeconomic status (SES) is associated with a variety of health outcomes, the literature on the association between SES and traumatic brain injury (TBI) outcomes has not been formally summarized. This study aims to review existing literature to ascertain whether patients with low SES pre-injury have worse clinical outcomes after TBI compared with those with high SES, in high-income countries. A systematic search was conducted using the MEDLINE, Embase, and PsychINFO databases. Observational studies addressing the association between SES and TBI outcomes (mortality, functional, cognitive, and vocational outcomes) were included (published from 2000, written in English). Both pediatric and adult TBI groups were included. Thirty-two studies met the inclusion criteria. Measures of SES varied across studies. Mortality was assessed in seven studies; five reported an association between low SES and higher mortality. Five of eight studies showed an association between low SES and worse functional outcomes; results for cognitive (n = 13) and vocational outcomes (n = 10) were mixed. The results of this review suggest that SES is a variable of interest in the context of TBI outcomes and should be assessed at time of admission to assist in social work discharge planning and early mobilization of available community resources. Further work is required to better understand the impact of SES on TBI outcomes.
Introduction
Traumatic brain injury (TBI) is a leading cause of morbidity and mortality worldwide, with an estimated annual incidence of 69 millions globally. 1 Multiple factors can influence long-term outcomes after TBI, including injury-related factors (such as injury severity and additional systemic injuries) as well as demographic and contextual factors. The latter group contains several variables including age, comorbidities, and socioeconomic status (SES).
The SES can be defined as the combined economic and social status of an individual or a group unit such as a household. This is commonly measured in terms of education, income, and occupation, but additional metrics such as place of residence can also be used as proxy measures. 2,3 The SES has a bidirectional association with health, with evidence suggesting that SES influences one's ability to access healthcare resources and treatment, and develop and maintain healthy habits. Reciprocally, health can also influence SES in that health status has an impact on a person's ability to attend and succeed in schooling or work. 2
Evidence has shown that SES mediates one's ability to access relevant health services—for example, because of services being inaccessible both geographically (reduced ability to travel) and financially (unaffordable in private healthcare settings). 4,5 Acceptability of health services to patients from different SES brackets also varies with evidence that lower SES is associated with reduced engagement with health screening and preventative health initiatives, potentially because of reduced awareness and health beliefs. 6 All of these factors can influence a patient's ability to recover after TBI.
SES and TBI
Low SES has been identified as a risk factor for increased incidence of trauma and injuries, including TBI. 7,8 United Kingdom (UK)-wide data from the Trauma Audit and Research Network (TARN) showed that low SES was associated with increased 30-day mortality after minor but not major trauma. 9 A study based in Scotland investigating mortality after TBI concluded that there is no association between lower SES and increased mortality, suggesting equal access to medical treatment, or that unequal access does not influence survival outcomes in this situation. 10
On the contrary, a study based in the United States used lack of medical insurance as a proxy for assessing SES, showing that this is associated with mortality and length of hospital stay after TBI. 11 Additional studies have demonstrated links between pre-injury SES and outcomes other than mortality, such as cognitive outcomes, with mixed results. 12 –14
The SES is likely to affect different groups of patients differently depending on their wider context, healthcare systems, and other factors. Therefore, whether SES is an independent factor impacting outcomes after TBI is an important question to answer to provide better future strategies to protect patients from health inequalities or reduce health inequalities themselves. There is currently no systematic review investigating the relationship between SES and clinical outcomes after TBI.
Therefore, the purpose of this review is to synthesize the existing evidence around the association between SES and outcomes after TBI.
Methods
A systematic review of the literature was conducted using the following databases: MEDLINE, EMBASE, and PsychINFO via the Ovid platform. The PRISMA guidelines were followed when reporting the results. 15
Original research articles meeting the following criteria were included: Patients of all ages suffering from TBI, diagnosed clinically or radiographically. Report of socioeconomic status of the patients with a definition of the measurement used (such as a deprivation index or other proxy measure but excluding education of the patient alone as this is often a precursor to downstream SES metrics). Assessing outcomes after TBI, including mortality and clinical outcomes (e.g., functional neurological status (GOSE [Glasgow Outcome Scale-Extended]), cognitive or vocational outcomes). Publications in the English language with full text available. Observational research study design. Reports from high-income countries (HIC) only, defined by HIC status set out by the World Bank, based on gross national income (GNI) per capita.
16
To assess whether a country was a HIC at the time of the study, the GNI per capita threshold of the year of publication of the article was used. This was to limit the role of confounding factors such as different health system resources that could impact the results. Published from 2000 onward. This was chosen to account for the developments in management of TBI within the last 20–30 years.
The final search was performed on 16th March 2021. The full list of search terms used, and number of articles screened is available in Appendix 1 of the Supplementary Materials.
Screening process
A two-stage review process was adopted with two-reviewer (SV, MS) abstract screening followed by a single-reviewer (SV) full-text review. Data extraction was performed using a custom-made data extraction table (Appendix 2 of the Supplementary Material). The PRISMA Flow Diagram, 2020 version, describes this process. 17
Article exclusion criteria were grouped as follows:
Reason 1. Article is a published conference abstract only.
Reason 2. Article is a narrative or systematic review article, not original research.
Reason 3. Article investigates the wrong patient population. For example, if it includes all types of acquired brain injury including strokes without differentiating outcome data into a clear TBI subgroup.
Reason 4. Article assesses the wrong outcome measure. For example, investigates the incidence of TBI rather than outcomes following TBI.
Reason 5. Article does not use a defined exposure metric for socioeconomic status.
Reason 6. Article is a technical article describing a scoring algorithm without focusing on the relevant outcomes.
Reason 7. Article compares across multiple countries that are both HICs and low- and middle-income countries (LMICs).
Methodological quality assessment and level of evidence
The National Institutes of Health (NIH) Study Quality Assessment Tool for Observational Cohort and Cross-sectional studies, a validated assessment tool for observational studies, was used to evaluate study quality. 18 The GRADE system was used to assess the level of evidence pertaining to the key outcomes of interest. 19,20
TBI outcomes
Because several outcomes are of interest after TBI, the following four outcome groups were investigated separately: mortality, functional, cognitive, and vocational outcomes. The rationale for these groups is described more in details in the results. The results of this review are reported as a narrative synthesis.
Results
There were 1576 studies identified by the pre-defined search strategy, and 32 studies met the inclusion criteria (Fig. 1). Most studies reported data from an individual country, although the study by Arango-Lasprilla and associates 21 included participants recruited from 18 European countries as part of the CENTER-TBI project. The United States was the most represented country in 15 studies, followed by Australia (four studies), Norway (three studies), and The Netherlands, the United Kingdom, Canada, Israel represented in two studies each. Fourteen studies were single-center studies and 18 were multi-center studies.
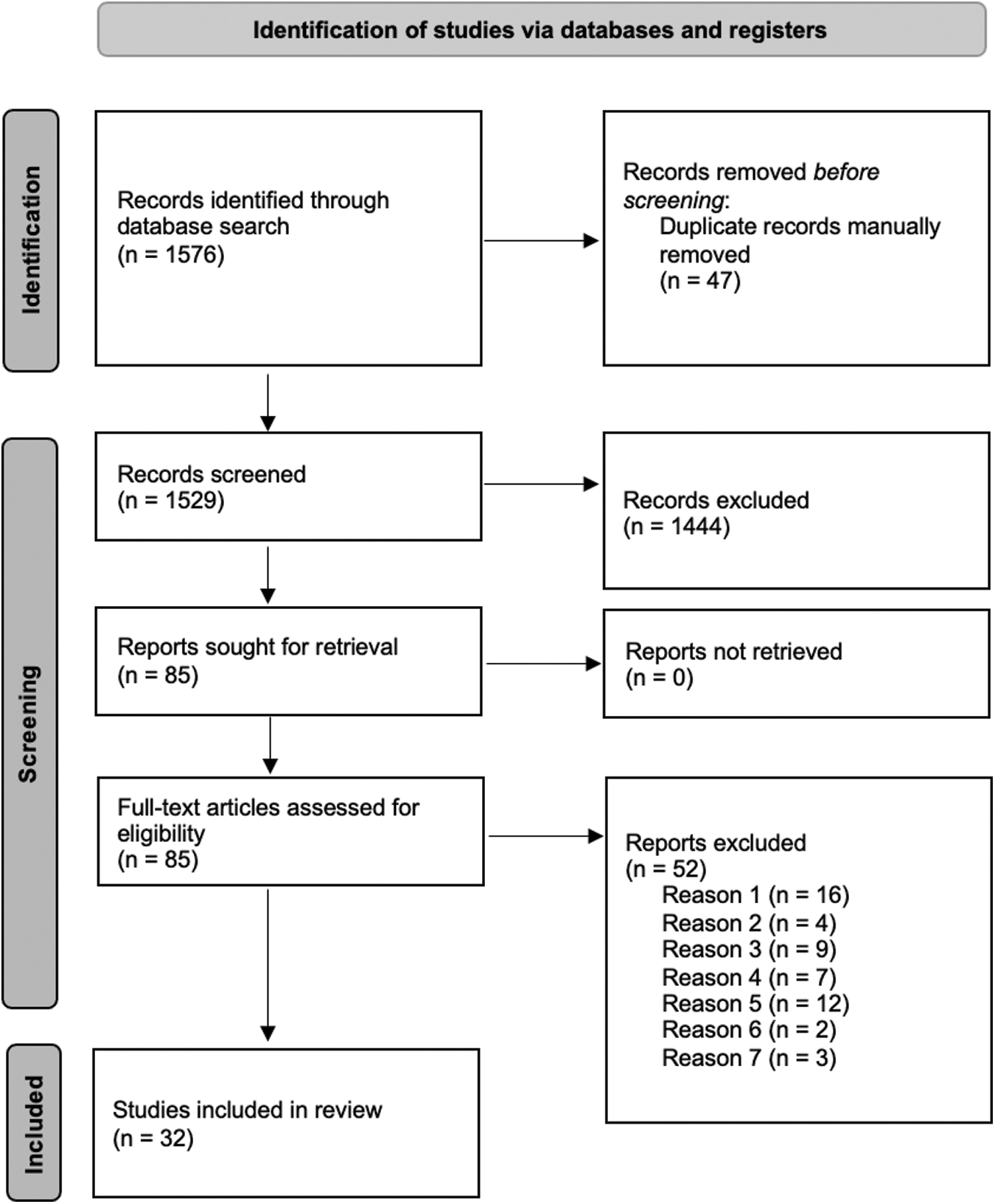
Preferred Reporting Items for Systematic reviews and Meta-Analyses ( PRISMA) diagram for this systematic review.
Twenty studies collected data prospectively, and the remainder were retrospective cohort studies. Follow-up time varied greatly between studies with some following patients only through acute hospitalization (particularly those focused on mortality), and others with follow-up intervals ranging from 3–6 months to 40 years.
The Glasgow Coma Scale (GCS) was used to assess TBI severity in all studies. Nineteen (60%) studies included participants with any TBI severity, five studies included patients with mild TBI only, 22 –26 five studies included patients with moderate or severe TBI, 27 –31 two studies included severe TBI alone, 32,33 and one study included patients with complicated mild (GCS 13–15 with CT head imaging findings) to severe TBI. 34
Sample size varied widely between studies, ranging from 34 TBI participants to 187,354 individuals. 35,36 Overall, the median population size was 163.5 (interquartile range 87 to 1724.5). Nineteen studies included adult patients alone, nine included only pediatric patients, and four studies included both groups.
Measuring SES
The most common measure of SES used in the included studies was pre-injury employment or occupation, noted in 12 of the 32 studies. 25 –28,30,31,33,37 –41 Eight studies investigating pediatric TBI populations used parental occupation as their measure of SES 13,22,23,35,42 –45 and one used the highest education level of the primary caregiver as measure of SES. 34 Four studies, all based in the United States, used medical insurance as a proxy measure for SES. 11,36,46,47
Income was used by a small number of studies: Nuno and colleagues 48 used the median family income in the zip code of residence, classified into income brackets. 48 Heffernan and coworkers 46 also used median income in the zip code based on US census data as a continuous scale by $1000 increments. Huang and associates 38 used family income status, defined as low, middle, or high-income family, as one of their SES measures, alongside employment.
The SES can also be measured through indices or composite scores incorporating multiple variables. Such indices were used in six articles included in this review and include the Carstairs and Morris Index of Deprivation, English Indices of Multiple Deprivation (IMD), New Zealand Deprivation Index 2006, and the Socioeconomic Composite Index. Two studies created their own context-specific composite scores. 29,32
TBI outcomes based on SES
The included articles reported a range of outcome measures. To allow for comparison across studies and pooling results of studies addressing similar outcomes together, outcome measures were grouped into one of four categories: mortality, functional outcomes, cognitive outcomes, and vocational outcomes. Specifically, the functional outcomes category included several measures of pertaining to global functioning, such as assessment of overall health and disability, independence with activities of daily living, GOSE, and self-reported measures of persisting symptoms and quality of life. The cognitive category included measures of cognition and neuropsychiatric symptoms, and vocational outcomes pertained to return to work.
From a methodological perspective, it is important to note that all studies used multi-variable analysis when assessing the association between variables and their outcomes.
Mortality
Seven of the 32 studies investigated mortality as one of their primary outcomes (Table 1), all of which had populations of more than 1000 individuals per study. All but one study concluded that lower SES was associated with a statistically significant increase in mortality compared with higher SES. Five studies investigated in-hospital mortality, of which three showed a significant association with SES, and one showed a significant association between SES and mortality for severe TBI only. Dunn and colleagues 49 was the only study showing no difference in the odds of in-hospital mortality based on baseline SES: in this study, more deprived patients had higher survival rates than less deprived individuals (81.2% vs. 78%, p = 0.046) in univariate analysis, but this was not significant after multi-variable analysis, potentially suggesting confounding.
Summary of Studies With Mortality as Their Outcome
SES, socioeconomic status; TBI, traumatic brain injury; SD, standard deviation; AIS, Abbreviated Injury Scale, scores 1–5 with increasing severity; CI, confidence interval; HR, hazard ratio; ISS, Injury Severity Score.
Significance column: Standard text, low SES predicts worse outcomes; italic, low SES does not predict difference in outcomes. Scores 1 - 15 with increasing severity.
Studies based in the United States used medical insurance as a proxy measure for SES. Haines and coworkers 11 showed a significant increase in mortality with lower SES for severe head injuries, when comparing privately insured versus uninsured patients, although the effect was quite small (odds ratio [OR] = 1.052, p = 0.001, confidence interval [CI] not reported). Heffernan and associates, 46 McQuistion and colleagues, 47 and Selassie and coworkers 36 used insurance status as a proxy for SES. They all showed a significantly higher mortality risk for patients with Medicare/Medicaid insurance and uninsured individuals compared with those privately insured.
Heffernan and associates 46 showed that patients with private insurance were less likely to die compared with those with Medicare/Medicaid policies (OR = 0.68, 95% CI = 0.51 to 0.9) or uninsured (OR = 0.57, 95% CI = 0.41 to 0.78); McQuistion and colleauges 47 showed that uninsured patients were more likely to die in hospital compared with those with private insurance (OR = 1.37, 95% CI 1.27 to 1.48); and Selassie and coworkers 36 showed increased odds of mortality for patients without insurance (OR = 1.27, 95% CI 1.11 to 1.45) and indigent insurance (OR = 1.67, CI 1.48 to 1.87) compared with the privately insured group.
Functional outcomes
Eight studies addressed functional outcomes 24,25,27,29,30,33,38,50 with a wide range of population sizes (from 51 to 8630) and follow-up duration (from three months to 40 years). The outcome measures varied: (Extended Glasgow Outcome Scale), which describes longer term functional outcomes, was used as a metric in three studies 25,33,50 while other social functioning and activities of daily living (ADL) scales were used by Hoofien and coworkers, 32 Rassovsky and colleagues, 29 and Ulfarsson and associates. 33
The Patient Competency Rating Scale (PCRS) was used by van Walsem and colleagues 30 to assess competency with daily activities as reported by patients, and Yue and associates 35 used a satisfaction with life scale administered to patients at six months post-injury requiring individuals to rate items on a point-based scale. Huang and associates 38 assessed overall functioning based on being institutionalized or discharged home. Finally, Rabinowitz and coworkers 24 assessed persisting symptoms using a validated questionnaire (Rivermead Post Concussion Symptoms Questionnaire).
Results support the presence of an association between lower SES and worse functional outcomes. Five studies showed a significant link between lower SES and worse functional outcomes, including two large studies of 8630 patients by Huang and associates 38 and 1322 patients by Humphries and colleagues. 50 Huang and associates 38 showed a large increase in the odds of being institutionalized versus being discharged home for both SES exposure measures used (unemployment vs. employment: OR = 2.12, 95% CI = 1.34 to 3.34, and family income (average vs. low): OR = 2.20, CI = 1.66 to 2.92) in their multi-variable model. Humphries and colleagues 50 showed that 12-month GOSE scores worsened with increasing deprivation (increasing raw IMD scores) in their multi-variable ordinal regression model.
Two small-scale studies showed no association, with a total of 176 included patients across the two studies. 24,29 One study by Yue and coworkers 25 showed that patients who were unemployed pre-injury had lower GOSE scores at 6 months compared with those in employment (GOSE scores decreased by 0.50 points, CI = -0.88 to -0.11), but self-reported quality of life scores did not differ (Table 2).
Summary of Studies With Global Functioning Measures as Their Outcome
SES, socioeconomic status; ADL, acivities of daily living; CI confidence intrval; GOSE, Glasgow Outcome Scale Extended; SCI = socioeconomic composite index-
Significance column (significance based on p < 0.05): Standard text, low SES predicts worse outcomes; italic, low SES does not predict difference in outcomes.
SES indicator created by the authors because of the context in which the study was conducted.
Cognitive outcomes
Thirteen studies focused on cognitive and psychiatric outcomes. 13,22 –25,29,32,34,35,42 –45 Variation existed between these studies in terms of the specific metrics and scales used to assess cognitive and psychiatric outcomes. These differences make it more challenging to compare results directly across the studies and increase heterogeneity of outcome data available. Nevertheless, most studies included measures of intellectual ability such as intelligent quotient (IQ) measures and other scales of intelligence, such as the Wechsler Intelligence Scale and learning tests. Scales of behavior were used in a small subset of studies.
Finally, two studies by Ryan and colleagues investigating psychiatric conditions used tailored interviews. 13,35 Results were mixed; five studies showed no association between SES and cognitive outcomes. 13,23,29,42,43 Catroppa and colleagues 43 tested intellectual ability through a number of IQ measures, none of which showed significant differences across SES groups, both at 2- and 10-years post-injury. Five studies suggested a link between lower SES and worse outcomes, 24,32,34,44 and three showed that SES affected some cognitive domains but not others 25,35,45 (Table 3).
Summary of Studies Assessing Cognitive Outcomes
SES, socioeconomic status; CI, confidence interval.
Significance column: Standard text, low SES predicts worse outcomes; italic, low SES does not predict difference in outcomes.
The study by Wade and coworkers 34 was the only study with a large population size of 591 (all other studies had populations of 34–164 patients). This study assessed child behavior problems and showed consistently over double odds of internalizing, externalizing, and total problems for children in the lower SES group after TBI (ORs, respectively for internalizing, externalizing, and total problems: OR = 2.82, 95% CI 1.27 to 6.28; OR 2.31, CI 1.02 to 5.24, and OR = 2.90, CI 1.20 to 6.44).
Vocational outcomes
Ten studies included vocational outcomes after TBI, all of which were investigated in adult patients only (Table 4). 26 –29,31,32,37,39 –41 Vocational outcomes primarily consisted of return to work after TBI, assessed in all 10 studies. The follow-up time at which the final assessment was completed, however, varied from six months to 14 years. Six studies showed a significant association between lower SES pre-injury, often assessed as pre-injury employment and occupation type, and employment after TBI.
Summary of Studies With Vocational Outcomes
SES, socioeconomic status; CI, confidence interval; RTW, return to work.
Significance column: Standard text, low SES predicts worse outcomes; italic, low SES does not predict difference in outcomes.
Two studies by Rassovsky and associates 29 and Grauwmeijer and colleagues 27 showed no association between SES and return to work, and both had long follow-up times of 10 years or more. 27,29 This could indicate that it takes longer for individuals with lower SES to return to work after TBI. De Koning and colleagues 26 showed a significant association between level of employment pre-injury and return-to-work at six months, but no significance at the later time point of 12 months. 26
Outcomes for pediatric patients with TBI
Most studies included in this review focused on adult TBI populations or included both older children and adults; therefore, the results up to this point present data from all included studies. This paragraph presents a closer look at those nine studies that focused solely on pediatric TBI participants. Of these, only one study had mortality as its primary outcome. 48 The remaining eight studies focused on cognitive outcomes. 13,22,23,32,34,35,42,43 The evidence was mixed, with four studies showing that family SES is not associated with differential cognitive or psychiatric outcomes after TBI, three studies showing a link between lower SES and worse cognitive outcomes, and one study showing a mixed picture with lower SES predicting worse outcomes for only some of the cognitive domains but not others. Details are provided in Appendix 3 of the Supplementary Material.
Outcomes based on TBI severity
Five studies only recruited participants with mild TBI. 22 –26 Overall, no clear association between SES and outcomes was shown in the mild TBI groups; however, the outcomes studied in these five articles varied. A further five studies included participants with moderate and severe TBI but not mild TBI. 27 –31 They all assessed functional outcomes, largely defined as post-injury employment, and also showed mixed results with a trend toward a negative association between SES and worse outcomes (three studies: lower SES associated with worse functional outcomes, two studies: neutral). Two studies only recruited participants with severe TBI, 32,33 and both showed worse outcomes for lower SES in their populations.
Assessment of quality and level of evidence
The 14-item NIH Quality Assessment Tool for Observational Cohort and Cross-sectional Studies was used to assess methodological quality. All articles scored well for the domains assessed having a clear and defined study question, and the exposure being measured before the outcome: however, based on the scoring guidelines, most studies scored a “poor” quality rating overall, and 11 scored a “fair” rating. No studies scored a “good” rating overall. Having the exposure measured more than once in the study and blinding of the assessors of the outcomes to the exposure were particularly problematic.
In regard to the variable studied (SES), however, these are unlikely to have had an impact on the quality of data reported because SES is typically relatively fixed and unlikely to have changed significantly over a short period. In addition, none of the studies reported performing a priori calculation regarding required sample size, which is important to detect differences between groups.
The GRADE quality assessment was used to assess the level of the evidence surrounding each outcome of interest (Table 5). Inconsistency, referring to unexplained heterogeneity of the results, was identified as serious for the cognitive and vocational outcomes. Serious issues with indirectness or imprecision of the evidence were not identified for these outcomes. Overall, the quality of evidence was rated as moderate for mortality: this was the outcome where studies had variable risk of bias, with some studies only having moderate risk of bias (rated as fair), and where the results were most consistent. The other three outcomes had low and very low quality of evidence, owing to high risk of bias in individual studies, as well as high levels of heterogeneity in between studies.
GRADE Level of Evidence for Each Study Outcome and Recommendations
Discussion
This review showed trends to support the hypothesis that lower SES is associated with worse outcomes after TBI. No studies showed better outcomes for lower SES groups. The mixed outcomes and heterogeneous data reported in this review, however, demonstrate that there are several challenges that should be considered when evaluating the SES of individuals with TBI that could impact study and patient outcomes.
All 32 studies included were observational. This is not surprising given the subject matter and inclusion criteria and has been shown to be the case for studies of SES in other clinical contexts. 5,51 It would not be possible to conduct randomized clinical trials to investigate SES; therefore, good quality evidence to inform clinical practice must be derived from robustly constructed, large scale observational studies.
SES measurement
The SES cannot be directly and objectively measured, but is a complex multi-dimensional context-specific construct, and measures vary according to the setting, country, or society of an individual. 52 Universally acceptable and valid metrics are difficult to establish; therefore, proxy metrics are the best method established for estimating SES.
Several measures of SES were used across the studies included in this review, frequently including occupation and employment. These can be challenging to compare between different studies and preclude meta-analysis because occupation outcomes have no set definition for research purposes (e.g., criteria used to define full-time employment may vary between studies).
Vocational outcomes in the included studies were primarily return to employment after TBI. This outcome may be biased as a marker for post-TBI success because various employers have different tolerances for leaves of absence, medical insurance coverage, and physical and cognitive requirements on return to work, regardless of TBI or other types of injury. Several studies attempted to address this issue by evaluating pre-and post-injury productivity or relative change in employment level.
An additional limitation of investigating this outcome was the definition of employment itself. This varied across studies, with some authors including those in education in the employed category 28,40 and others including them in the unemployed category. 39 Impact of age and other demographic factors on return to work are also relevant. Research shows that older individuals with TBI (>40) are less likely to return to work post-injury compared with younger individuals. 53,54 This may be related to greater ability to retrain and long-term employment prospects making employers more willing to invest in younger workers, or simply a patient's personal choice to retire early considering their injury regardless of functional rehabilitation. In addition, longer rehabilitation after TBI may have more focus on return to work for younger individuals. Taken together, this indicates that there may be multiple confounders of the relationship between pre-injury SES and employment after TBI.
Medical insurance status was also used as a proxy for SES. 11,36,46,47 This measure has the advantage of being readily available on medical records, but does not yield granular data and makes broad presumptions regarding a patient's employment or financial status based on presence or absence of insurance without regard for the vast variety of options for private and public funding available in many regions.
Results from the United States-based studies all demonstrated a correlation between lower SES, largely defined by presence or absence of insurance, and mortality risk. The difference in emergency care received after a trauma may not vary as much as outpatient or elective services, possibly confounding the association between insurance status and SES, thus biasing the interpretation of the results of these studies. On the other hand, insurance status likely has a large impact on rehabilitation services utilized after index hospitalization, thus very likely impacting some of the longer-term outcomes reported in included studies.
Several studies in entirely publicly funded medical systems also found associations between SES and outcomes, using measurements other than insurance status as proxies for SES, implying that insurance status alone is not a reliable measurement of SES, with variation existing within broad insurance groups.
Indices of deprivation were also used: Carstairs and Morris Index of Deprivation, 49 the English Index of Multiple Deprivation, 50 the New Zealand Deprivation Index, 55 and the Socioeconomic Composite Index. 24 The above indices have a key issue of providing area-level rather than individual-level deprivation scores. They also have the advantage of being context specific, because they can include tailored variables that apply to a local population or group, making them a very specific and likely more accurate measurement tool for SES. This is highly appropriate as SES is best understood within its own context; however, this can make wider comparison across populations more challenging.
Outcomes measurement
The outcomes evaluated in SES studies are also quite heterogeneous and susceptible to a variety of factors that could impact reported results. Most studies evaluating mortality reported in-hospital mortality without looking at 6- or 12-month relative risk of mortality, which could be impacted by several SES factors.
Functional outcomes can also be quite variable depending on the tool used and timeline studied. This review found that low SES appears to be correlated with poor functional outcomes, but specific outcomes measured can impact the data reported. For example, Huang and associates 38 demonstrated a significant relationship between family income and functional outcome that they defined as discharge destination to home or long-term facility. This study was conducted robustly, but a key limitation is the lack of information regarding caregiver status, outside assistance by home-care nursing staff, and level of independence at home, because this could vary from being completely independent to requiring assistance for most ADL.
This outcome is also limiting because families of higher SES would likely have a better ability to care for injured family members at home through the financial means to hire home-care nursing staff or potentially taking extended leave from work to care for patients during the recovery period, a luxury that is often not available to those of non-professional or hourly workers in many locations. Thus, discharge destination is likely a poor representation of true recovery and lacks detailed stratification regarding expected outcomes.
Other measurements of functional outcomes, such as level of independence and self-reported symptom and satisfaction scores have similar challenges. Analogous to the indices used as SES measurement, functional outcomes are a factor of their own societal context, linked to personal values, social dynamics, and cultural beliefs. This raises a challenge relating to the need to achieve a trade-off between using locally developed and meaningful metrics of functional outcomes and utilizing standardized measurements of outcomes such as GOSE that may be less specific but easier to compare between varied patient populations.
Cognitive outcomes, too, are highly susceptible to variations in measurement, reporting, and context-specific expectations. Cohen-Zimerman and colleagues 44 showed a significant association between childhood SES and intelligence scores years after injury (higher SES, higher intelligence scores). .The authors also noted, however, a similar significant association between SES and intelligence overall both in the controls and TBI groups, suggesting that the link between intelligence and SES exists even in the absence of a brain injury. They postulate that this may be explained by the theory of cognitive reserve, stating that pre-morbid cognitive enrichment (such as years of education, access to resources, and a stimulating environment) plays a neuroprotective role in modulating the effects of a subsequent brain injury. 56,57
Measures of intelligence are inherently flawed by biases and the context and cohort against which they are compared, making it challenging to conduct studies with varied patient populations. In addition, intellectual outcomes may not be the only measurement of consequence when evaluating cognitive impact of TBI; Yue and coworkers 25 showed that lower SES predicted higher psychological distress scores but no difference in neurocognitive domains. The authors considered whether there may be an element of confounding in that unemployment and more challenging social situations may themselves be a predictive factor of distress even in the absence of brain injury, drawing similar conclusions to the aforementioned complexity of this outcome paradigm. Psychological distress, however, is an important consideration for developing children, even in the absence of intellectual impairment.
Study designs
The size of the studies evaluated in this review varied and likely had an impact on reported findings. The studies evaluating the association between SES and mortality had a mean of 49,047 participants (range 2932 to 187,354), while the studies reporting on functional outcomes were smaller overall and findings were stratified by cohort size; the two studies that had large populations of greater than 1000 patients found there was an association between SES and poor functional outcomes 38,50 while those that were smaller demonstrated no link with outcomes.
Similar results were reported for cognitive outcomes. Both studies that evaluated the cognitive outcomes in children after TBI reported a relationship between SES and poor outcomes, but the estimates of the associations were imprecise, likely because of the small sample size of both studies (40 and 70 individuals, respectively). 42,43 Thus, a lack of association between SES and poor outcomes found in some studies could be because of underpowered studies; frequently these were the studies measuring complex psychosocial concepts that required multi-faceted evaluation and long-term follow up.
All studies used multi-variable analysis when studying the association between variables of interest and outcomes; a number of studies reported both univariable and multi-variable models, and in this case, the results included in this review represent the multi-variable analysis, because these adjust for other factors. This demonstrates that the authors attempted to account for other variables that may influence the results of their studies.
Implications for clinical practitioners
This work supports the hypothesis that SES is a variable of interest in the context of TBI outcomes. It flags that patients with TBI falling into the low SES category may require individualized and targeted interventions during their recovery to help them achieve similar outcomes to the higher-SES group, a concept that has been identified across diverse areas of clinical medicine. 58 –60
Societal changes are likely required to reduce socioeconomic inequalities, and healthcare professionals are a key professional group to initiate changes pertinent to the patient populations they treat. 61 The SES sits within the domain of the social determinants of health, contributing to the social gradient of health, a concept describing how one's position within society influences health. 62 A wider implication is therefore to advocate on behalf of vulnerable patient groups such as those with TBI.
The SES may be an upstream factor affecting an individual's ability to access health services because of lack of awareness of services available, physical challenges in reaching those (such as unavailable resources, distance, cost), weaker support networks to support one during the illness journey. These factors may therefore be part of the pathway linking SES to health outcomes. Therefore, addressing SES may be the correct strategy to reducing societal inequalities and could result in more equal access to care.
For instance, patients with TBI from lower SES could be offered targeted follow-up for early identification of complications and to facilitate an environment conducive to recovery, particularly regarding ability to participate in rehabilitation programs (such as childcare at physical therapy clinics or expanded paid time off from employment for doctors' appointments) and skills workshops for those required to change professions because of limitations from their injuries.
It is likely that those with prior unemployment, precarious employment, or low skilled jobs will require more targeted employment development training as part of their rehabilitation. Because TBI frequently affects young individuals, focusing on employment post-TBI is essential to reduce the overall loss of earning from a working-age population. Similarly, further resources could be allocated to community-based interventions in areas of greater need, to support patients locally, and strengthen their support networks.
Incorporating assessments of a patient's socioeconomic setting in early assessments could help to identify patients at risk of having worse outcomes during their initial hospital admission, allowing for resources and appropriate services to be mobilized to support them. In addition, a greater understanding of how SES affects outcomes could help establish more targeted prevention strategies in the community, such as more frequent teaching about and advocating for safety measures like bicycle helmets and seat belts in low SES areas.
At a practical level, this work suggests that taking time to ascertain a patient's sociodemographic circumstances could be crucial to facilitate targeted care in the rehabilitation after TBI. It could also be useful for designing robust prediction models for patient outcomes or strengthening existing models with SES information and instituting more specific preventative measures after injury.
Recommendations for future work
The findings of this review should be corroborated by large scale, longitudinal studies of SES and TBI in a range of healthcare settings. Understanding how the impact of SES on outcomes changes based on the health system it is studied in will be beneficial to identify protective factors as well as health system characteristics that are driving inequalities. Measuring SES in health research is challenging because of the heterogeneity of metrics available, and as suggested by Oakes and associates, 52 new efforts should be made in conjunction with epidemiologists and experts to reach a consensus and identify widely accepted and reproducible measures. This would also facilitate quantitative pooling of results from multiple studies through meta-analysis.
While shorter follow-up duration may be suitable to investigate in-hospital mortality, longer follow-up times are required to evaluate cognitive and vocational sequelae of TBI, particularly in pediatric populations. Future studies should allocate resources to longer-term longitudinal follow-up to detect changes that may become apparent years after the initial injury.
Agreement should be sought to use validated and standardized outcome metrics for each domain of interest. For example, it would be useful to compare the same mortality time point, such as in-hospital mortality or 30-day mortality. Similarly, with regard to global functioning measures, using outcomes scales such as the GOSE, Disability Rating Scale (DRS), or the disease specific quality of life measure Quality of Life after Brain Injury (QOLIBRI) would facilitate reproducibility across individual studies and quantitative pooling of study results in meta-analysis. 63
Limitations
Studies were heterogeneous in terms of their designs and measures of SES and outcomes used, precluding the ability to perform a meta-analysis. Specifically, the following factors result in the inability to perform meta-analysis. First, there are limited groups of studies using the same outcome measure—for example, the GOSE (three studies); however, these use the GOSE at different time points (two studies use GOSE at 12 months, one at six months), making comparison in meta-analysis difficult. 25,33,50
In addition, and more importantly, these studies measure exposure (SES) differently, which complicates quantitative comparison across studies. For example, one study uses the English Indices of Multiple Deprivation as a SES metric, 50 which is a scale dividing the population into deciles from most to least deprived, the second study uses dichotomized employment versus unemployment groups, 25 and the third uses the employed versus unemployed categories again but further subdivided into duration of unemployment. 33 Because of these multiple elements of variation, we believe that a meta-analysis with the current data is not appropriate, due to comparing studies with multiple cohorts of patients. The same can be applied to other studies with the same outcome measure such as in-hospital mortality.
The methodology of the included studies must be scrutinized, specifically with regard to confounding and interactions between variables. The role of confounding variables and mediator variables on the causal pathway linking SES to TBI outcomes needs to be considered more deeply. For example, other behaviors such as risky drinking practices and unsafe driving behaviors, which have been associated with low SES, may also contribute to poor health outcomes before or after traumatic injury. 64,65
Similarly, lower SES is associated with a higher incidence of traumatic injuries in adult and pediatric populations. 66,67 Therefore, one must be careful to interpret mortality figures in proportion to the disease incidence, which can vary for different population groups.
A high proportion of articles reviewed originated from the United States. Careful consideration must be taken of the differing insurance paradigms, regarding public versus private insurance changes subsequent to ObamaCare that occurred during the inclusion period of this study (since 2000). Using privately insured versus non-insured status as a proxy for SES could be misleading because insurance coverage is optional and under the current paradigm, many young, healthy people may choose not to pay for insurance regardless of SES.
In addition, this combined public-private system results in complex insurance schemes with many patients partially covered by both public Medicare/Medicaid and private insurance, Veterans insurance, possible add-ons to the basic public insurance, and different levels of coverage between individuals in the same household (children covered by insurance when parents are not, married adults covered by different insurance methods through their jobs requiring various levels of pay-in, deductibles, and copayments). This could be a potential confounder for outcomes published in SES literature and reported in this review.
Finally, this systematic review focuses on the impact of SES on TBI outcomes in high-income countries but excludes low- and middle-income countries. This approach was chosen to narrow the scope and obtain a more homogeneous population. Including LMICs within the same review was not deemed appropriate because differences in outcomes could be attributable to several other factors including wider differences in medical care received. This would have resulted in difficulty in differentiating between confounding factors and true association between the exposure and the outcome. Therefore, the results of this review would be relevant to high income systems alone, limiting their applicability in lower income settings. A separate review would be required to make conclusions for those settings.
Conclusion
This is the first systematic review of the association between pre-injury SES and outcomes after TBI. Using a narrative synthesis of the available evidence, trends emerged suggesting that SES is a variable of interest in TBI. The link between SES and outcomes was most robust regarding mortality and functional outcomes and more uncertain for cognitive and vocational outcomes. Further large scale, prospective, longitudinal observational studies are required to further elucidate and quantify the impact that lower SES has on clinical outcomes in the TBI population.
Notably, this review raises the point that SES should be considered as one of the relevant demographic or background factors for patients with TBI. It is important for clinicians and healthcare professionals to be aware that SES may play an important role in the clinical outcomes of patients with TBI, and actively collecting data regarding SES and considering this within a patient's clinical journey may enable early mobilization of targeted interventions for specific patient groups.
Footnotes
Authors' Contributions
S.V. designed the study protocol, J.G provided input in the protocol design. S.V. and M.S. performed the screening, data extraction and manuscript writing processes. J.G. and P.J.A.H critically revised the manuscript. All authors have read and approved the final manuscript.
Funding Information
JG was supported by the Medical Research Council (Skills Development Fellowship). For the purpose of open access, the author has applied a Creative Commons Attribution (CC BY) licence (where permitted by UKRI, ‘Open Government Licence’ or ‘Creative Commons Attribution No-derivatives' (CC BY-ND) licence may be stated instead) to any Author Accepted Manuscript version arising. PJH is supported by the NIHR (Cambridge BRC, Medtech Co-operative on Brain Injury, Global Health Research Group on Acquired Brain and Spine Injury, Senior Investigator Award) and the Royal College of Surgeons of England.
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Appendix 1
Appendix 2
Appendix 3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.