
Abstract
Clinical recovery after sport-related concussion varies as a function of pre-injury and acute factors. Whether, or the extent to which, concussion history is associated with clinical outcome after sport-related concussion is uncertain, because research has produced mixed findings. The present study aimed to assess whether a history of previous concussions was associated with prolonged clinical recovery after a subsequent sport-related concussion. The sample comprised 780 adolescent student athletes (mean age = 16.3, standard deviation = 1.3 years; 56.8% boys, 43.2% girls) whose school participated in the Maine Concussion Management Initiative (MCMI). Survival analyses were used to compare recovery times among adolescents with a history of 0, 1, or ≥2 previous concussions after a subsequent sport-related concussion. The two primary outcomes of interest were the number of days to return to school and sports. There were no statistically significant differences in total time to return to school and sports, or the proportion of adolescents who returned to school and sports at most intervals (e.g., 7, 14, 28 days), between those with 0, 1, or ≥2 previous concussions. A greater proportion of adolescents, however, with a history of ≥2 previous concussions remained out of sports at 28 days compared with those with no previous concussions (23.5% vs. 12.7%; odds ratio [OR] = 2.10, 95% confidence interval [CI] 1.18–3.73). Having sustained prior concussions was not associated with time to return to school after a subsequent sport-related concussion. A greater proportion of adolescents, however, with two or more previous concussions experienced a prolonged return to sports. Further research is warranted to identify risk factors for worse outcomes among the subset of adolescents with a history of multiple previous concussions who experience prolonged recoveries.
Introduction
Between 2009 and 2014, every state in the United States passed a law relating to youth concussions. 1,2 School districts across the United States have implemented policies and procedures for academic accommodations and return to school-sponsored sports for students who sustain concussions. 3 Just more than one in 10 (12.2%) middle-school student athletes report having a history of at least one previous concussion, 2.4% report having sustained two or more previous concussions, and 1.2% report having a history of three or more previous concussions. 4 Rates are modestly higher among high school athletes with 14.9% reporting at least one previous concussion, 4.3% reporting having two or more, and 1.5% reporting three or more previous concussions. 5
There is considerable concern about youth who sustain multiple concussions, and whether they will take longer to recover from a subsequent concussion. In fact, it is widely believed that youth with a history of concussion are at increased risk for worse outcome after a future concussion. The Centers for Disease Control and Prevention (CDC) HEADS UP website indicates that post-concussion syndrome (i.e., persistent symptoms or prolonged recovery) occurs rarely after a single concussion and is most common among those who have experienced multiple previous concussions. 6 Moreover, the CDC guideline for diagnosing and managing pediatric mild traumatic brain injury recommends that clinicians counsel youth and caregivers that recovery might be delayed in those with a history of prior injury. 7
The strength of the evidence, however, supporting such authoritative statements and whether, or the extent to which, previous concussions are, in fact, associated with worse outcome from a subsequent sport-related concussion is unclear. A recent systematic review identified 51 studies examining whether children and adolescents with a history of concussion experience worse clinical outcome after a subsequent sport-related concussion. 8 There were 26,643 concussed youth included in these studies and a median of 36% had a past history of concussion. The studies were conducted in a variety of settings (although predominantly specialty concussion clinics), examined diverse outcomes and used different research and analytic designs. Most studies (72.5%) did not identify a statistically significant association between prior concussions and worse clinical outcome from a subsequent injury, 11.8% reported that those with past concussions had worse clinical outcome, 13.7% reported mixed findings, and one study (2.0%) noted that those with prior concussions had better clinical outcome. The authors concluded that the literature to date does not provide clear evidence that children and adolescents with a personal history of concussions are at increased risk for worse clinical outcome after their next concussion—although several important methodological limitations in the extant literature were identified that precluded definitive conclusions.
First, nine of 10 (90.2%) studies were not designed specifically, a priori, to address whether a history of prior concussions was associated with worse outcome—instead, studies often examined concussion history as a secondary variable of interest such as a demographic category or one of a number of covariates added to statistical models. Second, most studies examined prior concussion history as a binary variable (yes/no) and most often grouped youth together if they had any history of concussion (i.e., 1 or more); very limited research findings are available examining clinical outcomes among youth with multiple prior concussions (i.e., 2 or more priors, so the index concussion would be at least their third lifetime injury), which represents a major gap in the literature. Third, only two studies, of 51, assessed an academic outcome, 9,10 only one of which examined the time it took for youth to return to school. 10
Return to school is increasingly acknowledged as a critical clinical outcome among student athletes. A systematic review of 17 studies yielded findings supportive of accounting for factors such as symptomatology, age/school level, and course load to inform personalized and precision guidance for return to school after concussion. 11 Given that a full and durable return to school, without academic accommodations, is arguably the most important functional outcome for concussed children and adolescents, this represents another major gap in the literature.
The present study was designed to address important knowledge gaps. First, we studied time to return to school as a primary outcome (time to return to sports was the other primary outcome). Second, we analyzed previous concussion as a categorical (i.e., 0, 1, and ≥2 prior concussions) as opposed to a binary variable (0 or ≥1 prior concussions), and included a group with multiple prior concussions, so the index injury for which their recovery is being studied is at least their third lifetime injury. Given the relative novelty of examining prior concussion history as a nonbinary variable, this study was largely exploratory in nature. We hypothesized that there would not be an association between a history of one prior concussion and time to return to school or sports; however, we anticipated that those with two or more prior concussions might show longer times to return to school and sports.
Methods
Design
An Internet-based injury surveillance application, the Head Injury Tracker (HIT), developed by the Maine Concussion Management Initiative (MCMI) was used to record and store injury- and outcome-related data from high schools in Maine and Massachusetts, USA. The system was used by athletic trainers or other school personnel as part of their routine monitoring of annual injuries. Using these surveillance data, we conducted a naturalistic observational cohort study of recovery times among adolescents who sustained sport-related concussions. The surveillance period ran from September 2014 through January 2020.
Participants
The HIT injury surveillance database includes 846 adolescent student athletes ages 14 to 19 who sustained a sport-related concussion during the observation period. Thirty-six (4.3%) athletes were excluded because of missing dates for both recovery outcomes (days to return to school and days to return to sports). An additional 30 athletes (3.5%) were excluded because of outlier values reported for clinical recovery (> 90 days).
The final sample included 780 athletes (M = 16.3, standard deviation [SD] = 1.3 years) with a sport-related concussion. Regarding prior concussion history, 69.0% (n = 538) had no prior concussion history, 19.2% (n = 150) had one prior concussion, 8.1% (n = 63) had two prior concussions, 2.2% (n = 17) had three prior concussions, 1.2% (n = 9) had four prior concussions, 0.3% (n = 3) had five prior concussions, and 0.1% (n = 1) reported seven prior concussions. The sample included more boys (n = 443, 56.8%) than girls (n = 337, 43.2%).
For girls, the sports played at the time of injury were soccer (36.5%), spirit squad (13.9%), basketball (12.2%), field hockey (7.1%), volleyball (5.3%), lacrosse (4.5%), ice hockey (4.5%), and several other sports (16.0%). For boys, the sports played at the time of injury were football (40.4%), soccer (18.3%), basketball (9.3%), ice hockey (8.4%), lacrosse (7.7%), wrestling (4.1%), and several other sports (11.8%).
Measures
Demographic, health history, and injury information
Athletic trainers or other school personnel collect demographic and health history information from athletes, as well as data pertaining to injury characteristics (e.g., date of injury, injury scenario [sport vs. non-sport related]).
Recovery outcomes
Athletic trainers or other school personnel record information related to two primary clinical outcomes. First, they record the date adolescents return to school full time and without concussion-related accommodations. Second, they record the date adolescents return to sports (on completion of a return to play protocol). Recovery time is determined by calculating the number of days between the date of the initial injury and the respective recovery dates (return to school and sports).
Procedures
The HIT application is an online injury surveillance platform and has been described elsewhere. 12,13 Athletic trainers and affiliated school personnel are trained on the HIT application format and processes for entering deidentified concussion information. Schools that are involved in the program receive access to concussion education seminars, concussion-specific training, continuing education credits, and a small yearly stipend ($200). Institutional Review Board approval was obtained for the creation of the deidentified database and its use for research purposes.
Statistical analysis
The primary aim of this study was to assess whether, or the extent to which, prior concussion history is associated with prolonged clinical recovery after a subsequent sport-related concussion. Given the distribution of prior concussion histories (i.e., range 0–7) and interest in assessing concussion history in a non-binary manner, this variable was divided into three groups: (1) those with no prior concussion history before their index concussion, (2) those with a history of one prior concussion [index concussion would be their second lifetime concussion], and (3) those with a history of two or more prior concussions [index injury would be at least their third lifetime concussion]). Mann Whitney U tests, Kruskal-Wallis tests, and chi-square tests were used to assess between-group differences among demographic variables. Spearman correlations assessed correlations among the number of prior concussions (as a continuous variable), days to return to school, and days to return to sports.
Primary analyses
Survival analyses (Kaplan Meier with log rank tests) compared recovery times between adolescents with 0, 1, or ≥2 prior concussions and were censored at 28 days. We also conducted chi-square tests to compare the proportions of youth with 0, 1, or ≥2 prior concussions who were and were not recovered at various time points (e.g., 7, 14, 21, and 28 days), with only the tests for differences at 21 days for return to school and 28 days for return to school and sports considered primary analyses of interest because they indicate prolonged recovery. We graphed ascending cumulative recovery curves to display the percentages of athletes returning to school or sport from time of injury through 30 days post-injury. Alpha levels were set at p < 0.05 for these analyses.
Secondary analyses
We conducted secondary analyses to examine group differences based on demographic variables (i.e., age, sex, history of treatment for attention deficit hyperactivity disorder [ADHD]) migraine, depression) in the proportion of adolescents who did and did not return to school at 21 days and returned to sport by 28 days, respectively, after the index concussion across prior concussion groups (0, 1, and ≥2).
The Benjamini-Hochberg procedure (BH) with a false discovery rate of 0.10 was used to correct for multiple comparisons in univariate analyses (i.e., chi-square tests, t tests). 14 Results were interpreted as significant if the test p value was smaller than the BH critical value. In total, we conducted 30 (15 for return to school and 15 for return to sports) univariate tests (m) as part of these secondary analyses. All statistical analyses were conducted using IBM SPSS Statistics 28.
Results
Descriptive data
Demographic characteristics of the sample are presented in Table 1 and descriptive statistics for days to return to school and sports are presented in Table 2. Among the full sample, girls (median = 7 days) and boys (median = 7 days) did not differ on days to return to school (U = 67,845, p = 0.25, r = -0.04, negligible effect) or days to return to sports (girls median = 15 days, boys median = 14; U = 63,926, p = 0.59, r = -0.02, negligible effect). Days to return to school was significantly positively correlated with days to return to sports (rho = 0.57, p < 0.001).
Summary of Demographic and Health History Information Between Prior Concussion History Groups
SD, standard deviation; ADHD, attention-deficit/hyperactivity disorder.
Number of Days to Return to School and Sports by Prior Concussion History
M, mean; Md, median; SD, standard deviation; IQR, interquartile range.
Students' age was not associated with days to return to school (rho = -.04, p = 0.23) nor sports (rho = -.003, p = 0.93). The total number of prior concussions was not correlated with days to return to school (rho = 0.00, p = 0.96) or sports (rho = 0.02, p = 0.59). There were no significant differences between the prior concussion history groups in the proportion of boys and girls (χ 2 (2) = 0.76, p = 0.68). The prior concussion history groups differed very slightly by age [No Prior Concussions M = 16.3, SD = 1.3, 1 Prior Concussion M = 16.4, SD = 1.2, ≥2 Prior Concussions M = 16.6, SD = 1.2; K-W χ 2 (2) = 6.56, p = 0.04].
Prior concussion history groups did not differ in terms of proportions of students with self-reported pre-injury attention-deficit/hyperactivity disorder (χ 2 (2) = 4.54, p = 0.10) or depression, (χ 2 (2) = 4.58, p = 0.10). Prior concussion history groups did differ in terms of proportions with pre-existing migraines (χ 2 (2) = 32.0, p < 0.001) such that those with two or more prior concussions were more likely to report a history of migraines than those with one prior concussion or no prior concussions.
Date of return to school was not available for 18 (2.3%) adolescents and date of return to sports was not available for 49 (6.3%) athletes. The missing outcome data did not differ between girls and boys [missing school return data: girls = 2.1%, boys = 2.5%, χ 2 (1) = 0.14, p = 0.71; missing sports return data: girls = 6.8%, boys = 5.9%, χ 2 (1) = 0.30, p = 0.59]. The missing school return data also did not differ based on prior concussion history [No Prior Concussions = 2.4%, 1 Prior Concussion = 2.0%, ≥2 Prior Concussions = 2 .2%, χ 2 (2) = .98, p = 0.95]. A greater proportion of those with a prior history of two or more prior concussions, however, were missing sports return data [No Prior Concussions = 5.2%, 1 Prior Concussion = 6.7%, ≥2 Prior Concussions = 12.0%, χ 2 (2) = 6.13, p = 0 .047].
Return to school
Cumulative recovery curves displaying the proportion of adolescents who returned to school over time based on prior concussion history are presented in Figure 1. The mean, median, and number of days until 90% of athletes returned to school are shown in Table 2. Kaplan-Meier survival analysis indicated that prior concussion groups did not differ in days to return to school [Log Rank: χ 2 (2) = 2.83, p = 0.24]. Prior concussion groups did not differ in the proportion of athletes remaining out of school at 3, 5, 7, 14, or 21 days (see Table 3). There was a statistically significant group difference, however, in the proportion of athletes who remained out of school at 28 days after injury (p = 0.03).

Days to return to school (cumulative percentage curves).
Chi-Squared Analyses Comparing the Percentage of Athletes Who Returned to School and Sports at Various Time Points Post-Injury Based on Prior Concussion History
Italics represent primary outcomes of interest (prolonged return to school/sports).
Pairwise chi-square follow-up tests revealed that a greater proportion of athletes with no prior concussions (6.1%) remained out of school at 28 days compared with those with one prior concussion (0.7%; OR = 0.11, 95% CI 0.01– 0.78). Athletes with no prior concussions did not differ significantly from those with two or more prior concussions (4.4%; OR = 0.72, 95% CI 0.25–2.08); there was no significant difference between those with two or more versus one prior concussion in the proportions of athletes who remained out of school at 28 days.
Analyses assessing for associations between demographic variables and risk for prolonged return to school (>21 days) stratified by prior concussion history are displayed in Table 4. No demographic or health history variables (age, sex, ADHD history, migraine history, and depression history) were associated with a prolonged return to school across prior concussion groups (0, 1, & ≥2) after adjusting for multiple comparisons.
Demographics of Student-Athletes With Normal Versus Prolonged Returns to School (>21 Days) and Sports (>28 Days)
Fisher's exact test p value because of a cell size <5. BH, Benjamini–Hochberg critical value, (i/m)*Q, where i is the rank, m is the total number of tests (m = 30), and Q is the false discovery rate (Q = .10); result was deemed significant if the BH correction exceeded the p value (p < BH); OR, odds ratio; CI, confdece interval.
Return to sports
Cumulative recovery curves displaying the proportion of athletes who returned to sports over time based on prior concussion history are presented in Figure 2. Because many prior studies examined concussion history in a binary way (yes or no), we also present the cumulative ascending curves for time to return to sports for those with no prior concussions and those with one or more prior concussions (Fig. 3). The mean, median, and number of days until 90% of athletes returned to sports are shown in Table 2.
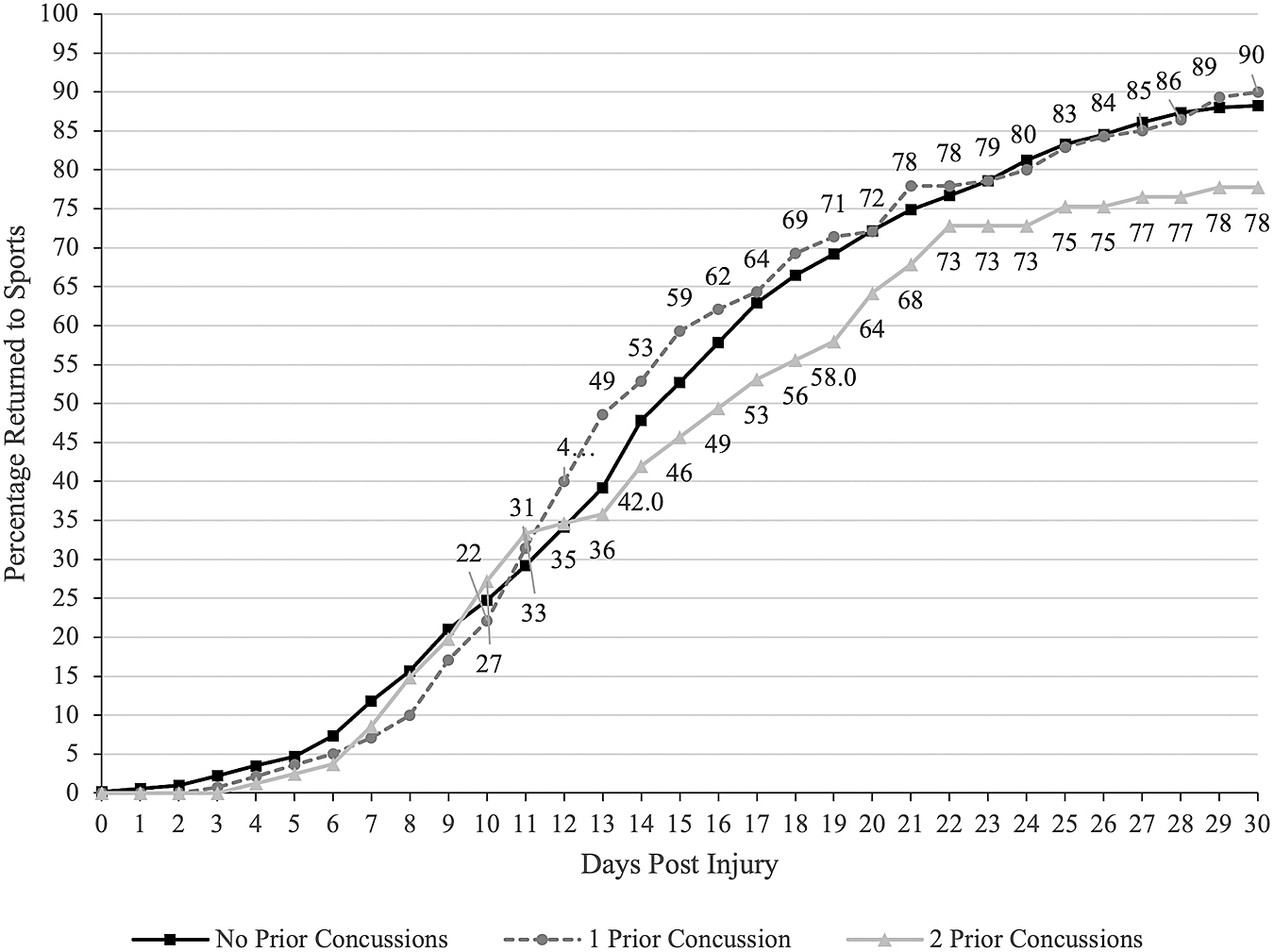
Days to return to sports (cumulative percentage curves).

Days to return to sports (cumulative percentage curves) with prior concussion coded as a binary variable (i.e., yes/no).
Kaplan-Meier survival analysis indicated that prior concussion groups did not differ in days to return to sports [Log Rank: χ 2 (2) = 3.95, p = 0.14]. Prior concussion groups did not differ in the proportion of athletes remaining out of sports at 7, 10, 14, or 21 days (see Table 3). There was a statistically significant group difference in the proportion of athletes who remained out of sports at 28 days after injury (p = 0.04). Pairwise chi-square follow-up tests revealed that a greater proportion of athletes with two or more prior concussions remained out of sports at 28 days (23.5%) compared with those with no prior concussions (12.7%; OR = 2.10, 95% CI 1.18–3.73), but did not differ significantly from those with one prior concussion (13.6%; OR = 1.95, 95% CI 0.96–3.95); there was no significant difference between those with no prior concussions versus one prior concussion in the proportions of athletes who remained out of sports beyond 28 days (OR = 1.08, 95% CI 0.6–1.86).
Analyses assessing associations between demographic variables and risk for prolonged return to sports (>28 days) stratified by prior concussion history are displayed in Table 4. There were no demographic or health history variables (age, sex, ADHD history, migraine history, and depression history) associated with a prolonged return to sports across prior concussion history groups (0, 1, & ≥2) after adjusting for multiple comparisons.
Discussion
It is widely believed that children and adolescents with a personal history of concussion are at risk for worse outcome after their next concussion, and this belief is reflected in the Centers for Disease Control guideline for managing pediatric mTBI. 7 The extant literature on this topic, however, is remarkably inconsistent with this perspective—with most studies not finding an association between prior concussion and worse clinical outcome. 8 There are fundamental limitations in published studies to date—such as most studies not being designed specifically to study this topic, being underpowered and classifying concussion history as binary (i.e., yes or no)—that leave the field at a crossroads. 8
In the present study, prior concussion history, including having multiple prior concussions, did not appear to be associated with time to return to school or sports after a subsequent sport-related concussion in most of the analyses. For example, days to return to school and days to return to sports were not correlated with the number of prior concussions adolescents sustained, did not differ between youth with 0, 1, or ≥2 prior concussion (mean group difference analyses), nor did survival functions for days to recovery differ between youth with 0, 1, or ≥2 prior concussion.
There was one statistically significant finding, however, in that a greater proportion of adolescents with a history of multiple (two or more) prior concussions experienced a prolonged return to sports compared with those with no prior concussion. There were no statistically significant differences between those who did and did not experience a prolonged return to school or sports along demographic and pre-existing health factors (i.e., age, sex, history of treatment for ADHD, migraine, depression) among those with a history of two prior concussions (although we were underpowered to examine those associations well). One explanation for why it appeared to take a subgroup of those with multiple concussions (i.e., the index concussion was at least their third concussion) longer to return to sports might be more conservative medical management, whereby the athletic trainer, physician, parents, and student-athlete might be comfortable with a more gradual return to sports (or possibly even discontinuing that sport). 15 –17
There are several notable strengths to this study compared with the available literature on the topic. First, prior concussion history was not examined as a binary variable (i.e., presence or absence of any prior concussions). Rather, concussion history was divided into three categories (i.e., 0, 1, ≥2), which allowed for an investigation of whether an increasing number of concussions is associated with recovery time.
Only a small number of studies have compared outcomes among youth with no prior, one prior, and two or more prior concussions. The number of youth with two or more prior concussions has varied across these studies, ranging from six to 192 participants. 18 –22 Moreover, the median number of participants with two or more concussions was 41 across 12 studies, and only four studies that examined youth with two or more prior concussions had larger cell sizes than the present study. 20,22 –24 Second, this study not only examined days to return to sports, but also days to return to school, which has been an underresearched yet critical outcome for concussion recovery studies. Third, the study examined potential interactions between concussion history and demographic and pre-existing health factors that have been associated with clinical outcome after concussion (i.e., sex, migraines, and depression).
These results suggest that concussion history does not appear to be associated with time to return to school after a subsequent sport-related concussion. Some of the results of the present study align with broader findings suggestive of no association between prior concussion history and time to return to school and sports among both youth 8 and college-aged students in most instances. 25
For example, among college athletes, of the seven studies that examined the association between time to return to sports and prior concussion history, only two studies reported a statistically significant association. 26,27 Notably, one of the two studies speculated that more conservative management of athletes with a history of prior concussion resulted in longer times to return to sport given that there was no difference in symptom duration between athletes with and without a history of prior concussions. 28
Differences in management of athletes with no prior concussion history, however, versus a prior history of multiple concussions has not been thoroughly investigated, particularly in the context of the number of prior concussions. Overall, these findings offer some evidence that may challenge and/or call into question the routine or automatic use of more conservative management of adolescent athletes with a history of prior concussions. Research is needed, however, to better characterize the minority of youth with two or more prior concussions who experience prolonged return to sports after a subsequent sport-related concussion.
There are interesting contrasts between the results of the present study of adolescent student athletes and a study conducted by Corwin and colleagues, 10 published in 2014, that reported on the same clinical outcomes (days to return to school and sports) among youth presenting to a specialty sports medicine clinic. In a sample of 247 youth presenting to a specialty clinic, the median number of days until return to school was greater across all concussion histories compared with the results of the present study. Youth with three or more prior concussions (n = 15) took a median of 105 days to return to school, compared with 33 days for those with two prior concussions (n = 22), 34 days for those with one prior concussion (n = 55), and 29 days for those with no prior concussions. In contrast, adolescent student athletes included in the present study with two or more prior concussions took a median of seven days, those with one prior concussion took six days, and those with no prior concussions took seven days. More broadly, time to return to school is within the range reported within the literature. 29,30
Differences reported by Corwin and colleagues 10 were more pronounced in relation to median days until fully cleared to return to sports. Youth with three or more prior concussions took a median of 243 days to be fully cleared, those with two or more prior concussions took a median of 158 days, and those with one prior concussion or no prior concussions took a median of 64 days. These results are in stark contrast to the present results, in which the median number of days to return to sports did not exceed 17 days across all levels of prior concussion history (i.e., 0, 1, ≥2). These divergent results highlight that youth presenting to specialty clinics represent a select group and thus research studies reporting findings from clinic-based samples likely do not generalize to the larger population of concussed student athletes.
Another finding that did not reach statistical significance, possibly due to sample size limitations, was an apparent overrepresentation of adolescents with a personal history of pre-injury depression in the prolonged recovery group among those with two or more prior concussions, as shown in Table 4. Youth with prior concussions who experienced a prolonged return to either school or sports were nearly three times more likely to report a history of depression. Depression is a well-established risk factor for worse clinical outcome after concussion. 31,32 Whether, or the extent to which, depression and prior concussion history interact represents a worthy area for future research. For example, the recurrent experience of multiple concussions and associated repeated lifestyle disruption, time held out of sports, decreased social activity during recovery, and potential increased school-related stress might be especially challenging for youth with pre-existing emotional health difficulties, leading to lengthier recovery times. Larger scale, prospective data collection efforts to adequately power analyses of subgroups of youth athletes with multiple pre-existing health conditions (i.e., multiple prior concussions and pre-existing mental health conditions) are required to advance our knowledge in this area.
Limitations
Concussion history as well as the other health history information were self-reported by adolescents. We could not verify whether the student athletes' self-reported health histories were accurate. Notably, high school student athletes are highly consistent when self-reporting their concussion history an average of two years apart. 33 Moreover, we do not have important information to better characterize concussion history, such as the mechanism, severity, recovery time of prior injuries. The use of self-report to determine concussion history and the lack of important information to better characterize prior concussions are pervasive limitations in sport-concussion outcome literature examining this topic and represent important methodological features for future investigations to improve on. 8
Further, there may have been differences in how concussions were defined/diagnosed because these data were collected during the course of routine practice with school personnel. In addition, there may have been variability among school personnel in how return to school and return to sports were defined. For example, some of the return to school dates may reflect when the student athlete returned to school in any capacity, and not when they returned to school without accommodations.
To promote data quality, training before implementing the HIT platform as well as ongoing technical support were provided to schools throughout the observation period. Last, acute post-injury assessment data were not available, and thus we were not able to characterize the severity of the index concussions.
As is the case with the majority of research reporting on prior concussion history as a continuous variable, the number of adolescents with multiple prior concussions decreases considerably with each additional prior concussion (i.e., 2 or more, 3 or more, 4 or more). 10,18,20,23,24,34 Only 1.6% of youth in the present sample reported a prior history of three or more concussions. Very few studies have examined clinical outcome among athletes with three or more prior concussions. Prior outcome studies of youth have reported 3.9%, 20 5%, 10 and 7.3% 18 of participants have a history of three or more prior concussions.
Some research among collegiate athletes suggests that a prior history of three or more concussions may represent a threshold for worse clinical outcomes. 35 -38 The same, however, has not been consistently found among youth athletes. 8 In fact, a study of nearly 2000 youth treated at a specialty clinic did not find a difference in recovery time among those with three or four or more prior concussions compared with youth with no prior concussions. 20 A study of 425 youth hockey players also did not report a difference in outcome; youth with three or more prior concussions did not take longer to return to play compared with those with no prior concussions. 18
The study with the smallest overall sample size, which also recruited from a specialty clinic, reported on a very small subgroup of only 13 youth with three or more prior concussions. 10 Among this small and seemingly highly select subgroup of youth, those with three or more prior concussions took longer to recover symptomatically and to be fully cleared, although no significant differences were found on other outcomes such as the median days to return to school full time or the percentage of youth reporting a decline in grades after their injury. 10 The limited number of participants with a history of three or more prior concussions in the present study precluded an analysis of this threshold.
Last, the HIT platform includes only a small number of demographic variables. Consequently, we could not assess for interactions between prior concussion history and possible contributors to clinical outcome such as race, ethnicity, and social determinants of health. Emerging research suggests these factors may contribute to disparities in concussion care and outcome and warrant further assessment in future studies. 39,40
Conclusions
The results of the present study are mixed, and they do not provide strong support for the belief that prior concussions are a risk factor for worse clinical outcome after the next concussion in high school students. There was no meaningful difference across the groups in how long it took them to return to school, and for most of the statistical analyses, the groups also did not differ on time to return to sports. Prior studies classified concussion history as binary, and as seen in Figure 3, the cumulative ascending curves for time to return to sports overlapped considerably. With that said, a greater proportion of adolescents with two or more prior concussions showed a prolonged return to sports compared with those with no prior concussions, although it is unknown whether this difference represents a biopsychosocial vulnerability from prior concussions, differences in clinical management, or some other factor(s). Further research is needed to determine whether there are other vulnerability factors in the subgroup of youth who sustain multiple concussion that confer risk for worse outcome.
Footnotes
Acknowledgments
The data were gathered as part of the Maine Concussion Management Initiative (MCMI) under the direction of principal investigator Dr. Paul Berkner. The MCMI was funded in part by the Goldfarb Center for Public Policy and Civic Engagement at Colby College, and the Bill and Joan Alfond Foundation (PI: Berkner). The authors thank the Maine Athletic Trainers Association for their collaboration with the MCMI.
Authors' Contributions
CG helped conceptualize the study, helped conduct the literature review, conducted the statistical analyses, created the tables and figures, and drafted the manuscript. GI helped conceptualize the study, helped conduct the literature review, helped conceptualize the statistical analyses, and edited drafts of the manuscript. RZ critically reviewed and edited the manuscript. PB helped design and coordinate data collection, wrote the IRB, conceptualized the injury surveillance program, investigated database questions, and edited the manuscript. NC assisted with conceptualizing the study and statistical analyses, helped conduct the literature review, supervised the analyses, and edited drafts of the manuscript. All authors reviewed and approved the final manuscript.
Transparency,Rigor,and Reproducibility Summary
The study design and analytic plan were not preregistered. This study conducted analyses on prospectively collected injury surveillance data from high school students whose schools participated in the Maine Concussion Management Initiative (MCMI). Data analyses were conducted using SPSS (version 28.0). Primary statistical tests included Kaplan Meier with log rank tests and chi-square tests. For secondary analyses, that included multiple comparisons, we implemented the Benjamini-Hochberg procedure to partially mitigate Type I error. Additionally, cell sizes for several of secondary analyses were not sufficiently powered to detect statistically significant associations. We plan to conduct replication studies with updated high school MCMI data and in a college population.
Funding Information
This study was funded in part by the National Football League for a program of research entitled “The Spectrum of Concussion: Predictors of Clinical Recovery, Treatment and Rehabilitation, and Possible Long-Term Effects” (PI: Iverson). NC acknowledges support from the Louis V. Gerstner III Research Scholar Award. GI acknowledges unrestricted philanthropic support from the Mooney-Reed Charitable Foundation, Heinz Family Foundation, Boston Bolts, ImPACT® Applications, Inc., National Rugby League, and the Schoen Adams Research Institute at Spaulding Rehabilitation. None of the above entities were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Author Disclosure Statement
CG and PB declare that they have no competing interests.
RZ has received salary support from the Harvard Integrated Program to Protect and Improve the Health of National Football League Players Association Members. He serves on the Scientific Advisory Board of Myomo, Oxeia Pharma, and ElMInda.
GI has been reimbursed by the government, professional scientific bodies, and commercial organizations for discussing or presenting research relating to MTBI and sport-related concussion at meetings, scientific conferences, and symposiums. He has a clinical practice in forensic neuropsychology, including expert testimony, involving individuals who have sustained mild TBIs (including athletes). He has received research support from test publishing companies in the past, including ImPACT® Applications Systems, Psychological Assessment Resources, and CNS Vital Signs. He has received research support from the Harvard Integrated Program to Protect and Improve the Health of NFLPA Members. He serves as a scientific advisor for NanoDx™, Sway Medical, Inc., and Highmark, Inc.
NC has a clinical practice in forensic neuropsychology involving individuals who have sustained mild TBIs.