
Abstract
Graded exertion testing (GXT) is an important tool for concussion management, as it is used to personalize post-concussion exercise prescription and return athletes to sport. However, most GXT requires expensive equipment and in-person supervision. Our objective was to assess the safety and feasibility of the
Introduction
Graded exertion testing (GXT) is quickly becoming a cornerstone of concussion management. 1 GXT can determine an individualized symptom exacerbation threshold for patients experiencing exercise intolerance, with aerobic exercise then prescribed for 20–30 min/day, 5–7 days/week at 80–90% of the heart rate at symptom exacerbation during the GXT. 2,3 Further, GXT is often used in the context of determining recovery status and readiness to return to sport, with individuals required to perform vigorous exercise without symptom recurrence prior to medical clearance. 1 The Buffalo Concussion Treadmill Test (BCTT) is the most widely used GXT for patients with concussion, 2 with stationary cycling 4,5 and dynamic/agility 6 GXT also available. However, current GXT protocols require expensive equipment and/or direct, in-person supervision from health care professionals.
The utilization of telehealth services has rapidly increased in the wake of the COVID-19 pandemic and telehealth approaches are likely to remain an integral part of health care services because they reduce barriers to care and improve health care access in rural locations. 7,8 Concussion diagnosis and management is centered on a wide variety of clinical assessments beyond GXTs, including a neurological exam, symptom reporting, and cognitive, balance, cervical spine, and visual/vestibular assessments. Although many concussion assessments have been adapted to fit virtual formats, 9,10 current GXTs remain unsuitable for telehealth services or even select in-person clinical settings without the space or funding to support the necessary exercise equipment. Thus, there is a need to develop telehealth-compatible GXTs to increase the implementation of this important concussion management assessment across a variety of clinical settings and to ensure patients are receiving current best practice in clinical care and management.
The
Thus, the MOVE protocol was designed to be an equipment-free, progressively intense, developmentally appropriate for children, and telehealth compatible exertion protocol. Our primary objective was to assess the safety and feasibility of the MOVE protocol in healthy children and children with subacute concussion. Our second objective was to compare heart rate, perceived exertion, and symptom presentation outcomes between the MOVE protocol and BCTT in children with subacute concussion. We hypothesized that the MOVE protocol would be safe and feasible for all participants and that heart rate and rate of perceived exertion (RPE) would increase throughout the test in a manner similar to the BCTT. Healthy children and children with subacute concussion were selected to first assess safety and feasibility of this novel GXT in lower-risk groups; future research will focus on more acute and symptomatic concussion groups.
Methods for Healthy Children
A convenience sample of healthy, uninjured children aged 5–17 years was recruited through research flyers distributed across the Facebook and Twitter accounts of research team members. Inclusion criteria were: 1) sufficient cardiovascular health to participate in exertion testing as evidenced by answering “no” to the seven screening items on the Physical Activity Readiness Questionnaire 13 ; 2) proficiency in English or French; and 3) technological requirements associated with virtual testing, namely access to a device with a webcam, microphone, and Internet. Youth were excluded if they: 1) were experiencing any injury or illness that precluded exertion testing; 2) had sustained any concussions within the past year; or 3) had sustained any prior concussion with unresolved symptoms regardless of time since injury. Parental consent and youth assent were collected prior to protocol initiation. This study was approved by the ethics committee of the Centre for Interdisciplinary Research in Rehabilitation (CRIR #1483-0520).
Participants and procedures
Twenty children were recruited between December 2020 and February 2021 (Table 1). Participants completed the MOVE protocol in their home during a single test session, with a 5-min follow-up session completed the next day to gather additional safety outcomes. The MOVE protocol was completed over Zoom Enterprise, a safe and secure video call platform. Immediately prior to protocol initiation, all participants provided demographic information and received an orientation session. This included standardized instructions on how to measure manual pulse; an explanation, demonstration, and corrections (if needed) for all exercises; and a discussion regarding protocol safety, with the parent or legal guardian present throughout the orientation session.
Descriptive Statistics for Participant Characteristics
Bold values in the P-value column indicate statistically significant findings.
Any condition refers to self-reporting one or more of the pre-injury conditions listed in the table (e.g., depression, anxiety, migraine, etc.). It is a summary variable encompassing the number of participants with at least one of the pre-morbid conditions listed. Fitness relative to peers is a self-reported outcome by the participant.
ADHD, attention-deficit/hyperactivity disorder; BCTT, Buffalo Concussion Treadmill Test; IQR, interquartile range; MOVE,
The MOVE protocol includes the following exercises completed in place: Walk, Slow Jog, Moderate Jog, Fast Jog, Jumping Jacks, Quick Steps, and Burpees. Each exercise lasted 60 sec, followed by 60 sec of rest. Participants were asked to maintain the fastest pace sustainable for the entire minute. MOVE protocol sessions were conducted by physiotherapy students in their final year of training, with the clinical skills to detect medical problems and stop a session if necessary. The physiotherapy student monitored the child virtually and provided cues as needed to maintain form for each exercise, while a parent/guardian was present within the patient's home for further supervision. A brief verbal and visual description of each exercise and an overview of testing procedures is found in Supplementary Figure S1, which was provided to participants ≥24 h in advance of testing. The stopping criteria for the MOVE protocol included any adverse event that prevented the completion of testing, or any sign of concern noted by the test evaluator.
Outcome measures
Primary outcomes were metrics of protocol safety. Minor adverse events were defined as: 1) a fall; 2) a musculoskeletal injury not requiring medical attention (e.g., minor ankle sprain); or 3) the persistence of increased (> 10-point change) concussion-like symptoms at the 24-h follow-up. Major adverse events include: 1) a musculoskeletal injury requiring medical attention (e.g., broken limb) or 2) severe concussion-like symptoms requiring medical attention. The MOVE protocol would be considered safe if fewer than four (20%) minor and/or two major (10%) adverse events occurred. This definition was based on a study by Chan and colleagues, 14 who concluded an exercise-based intervention was safe with 10 minor (≥ 10-point symptom increase) and two major (emergency department visits for concussion symptoms) adverse events reported.
Post-Concussion Symptom Inventory (PCSI)
The PCSI is a set of developmentally appropriate concussion symptom scales for children, with three different forms based on the child's or adolescent's age. 15 All participants completed the 20-item, 7-point Guttman scale version and rated each symptom from 0 (not present) to 6 (severe). The PCSI was completed immediately prior to and 24 h following the MOVE protocol. The total symptom score (sum of all items; possible scores range from 0 to 120 with higher scores indicating more severe symptoms) was the outcome of interest.
Activity limiting symptoms
Participants were asked if any concussion-like symptoms (e.g., headache, dizziness, etc.) were affecting their ability to participate in activities of daily living. Participants rated this question from 0 (no activities are limited) to 3 (most activities are limited). This captures a broader, more functional aspect of symptom reporting not captured by the PCSI.
Global symptom scale
Participants rated their overall symptom presentation from 0 (terrific, no symptoms) to 10 (terrible, worst I ever felt). The global symptom scale was administered at rest and following every exercise throughout the MOVE protocol.
Secondary outcomes of interest included measures of protocol feasibility, including the: 1) feasibility of the remote assessment; 2) feasibility of the protocol itself; 3) feasibility of the outcome measures; and 4) progressive intensity of the protocol. Assessments used to determine progressive intensity are defined below, with remaining outcomes listed in Table 2. The a priori definition of feasibility was that at least 3 of the 4 categories would be successfully achieved in ≥80% of youth.
Feasibility Outcomes for the MOVE Protocol
A priori definitions of feasibility, all feasibility outcomes evaluated, and the success rate for both healthy and concussed participants are presented. The outcomes labeled with an asterisk were collected for each MOVE protocol stage, for an n = 140 for healthy participants and n = 105 for participants with concussion. All other categorical outcomes were collected a single time-point, for an n = 20 (healthy) or n = 15 (concussed).
Zoom is a secure, cloud-based video communications application.
MOVE,
Pulse rate
Participants, or parents of young children, manually recorded pulse as a proxy of heart rate at rest and immediately following each MOVE exercise. Manual pulse was recorded at either the wrist or neck (participant preference) for 20 sec and multiplied by 3 to capture beats per minute (bpm).
Rate of perceived exertion (RPE)
RPE was recorded using the Borg scale at rest and following each MOVE exercise on a scale ranging from 1 (rest) to 10 (maximal activity). Both verbal and pictorial versions of this scale were used to increase understanding for young children. The Borg RPE scale has been used extensively in the post-concussion GXT literature. 3,16
Protocol satisfaction
Children and their parent separately rated their overall satisfaction with the MOVE protocol from 0 (not satisfied at all) to 10 (extremely satisfied) to broadly capture how content participants and parents were with the MOVE protocol.
Statistical analysis
Descriptive statistics are provided for patient characteristics and study outcomes (Tables 1 and 3). Adverse events were evaluated using descriptive statistics (frequencies with percentages). General linear models determined the relationship between MOVE stage and normally distributed outcomes (heart rate and RPE). A repeated term was added to account for multiple observations from the same participant. Symptom outcomes were non-normally distributed. Friedman's test assessed the relationship between MOVE stage and global symptom scale ratings throughout the test, whereas the Wilcoxon signed-rank (PCSI) and McNemar (symptom limited activities) tests evaluated changes in symptom metrics gathered pre- and 24 h post-test. Remaining feasibility outcomes were assessed using Fisher tests. Post hoc comparisons were performed with Bonferroni corrections wherever appropriate; significance was set at p ≤ 0.007 to account for the seven stages of the MOVE protocol.
Descriptive Information for All Outcomes Collected Throughout the MOVE Protocol
Outcomes are presented for both healthy and concussed children by exercise stage. For the heart rate outcomes, (M) = manual pulse and (P) = Polar HR monitor. The final two stages of the MOVE protocol differed between healthy controls. Healthy controls completed Quick Step exercises during Stage 6 and Burpee exercises during Stage 7. Concussed patients completed High Knees during Stage 6, with Quick Step exercises moved to Stage 7. All other stages were identical between groups, with the specific exercises listed in the column header.
MOVE,
Results for Healthy Children
Safety Outcomes
No adverse events were reported throughout the MOVE protocol. Global symptom scale ratings significantly increased (χ 2 (7) = 60.5, p < 0.001; Fig. 1) throughout testing. Eight (40%) participants reported no symptom change throughout the MOVE protocol, two (10%) participants reported a 1- or 2-point change, and 10 (50%) participants reported a 3- or 4-point change. Global symptom scale ratings reported during the final three exercise stages were significantly higher than at rest, with increased symptoms reported following Quick Steps compared with walking (Fig. 2). When investigating pre-session to post-session (24 h later) symptom changes, concussion-like symptom scores significantly decreased over time (PCSI score pre: 1 [interquartile range (IQ): 0–2.5]; PCSI score post: 0 [IQR: 0–0]; S = 45.5, p = 0.0002). Similarly, the proportion of participants reporting “few” activities of daily living being affected by concussion-like symptoms was reduced 24 h following testing (pre: n = 2 [10%]; post: n = 1 [5%]).
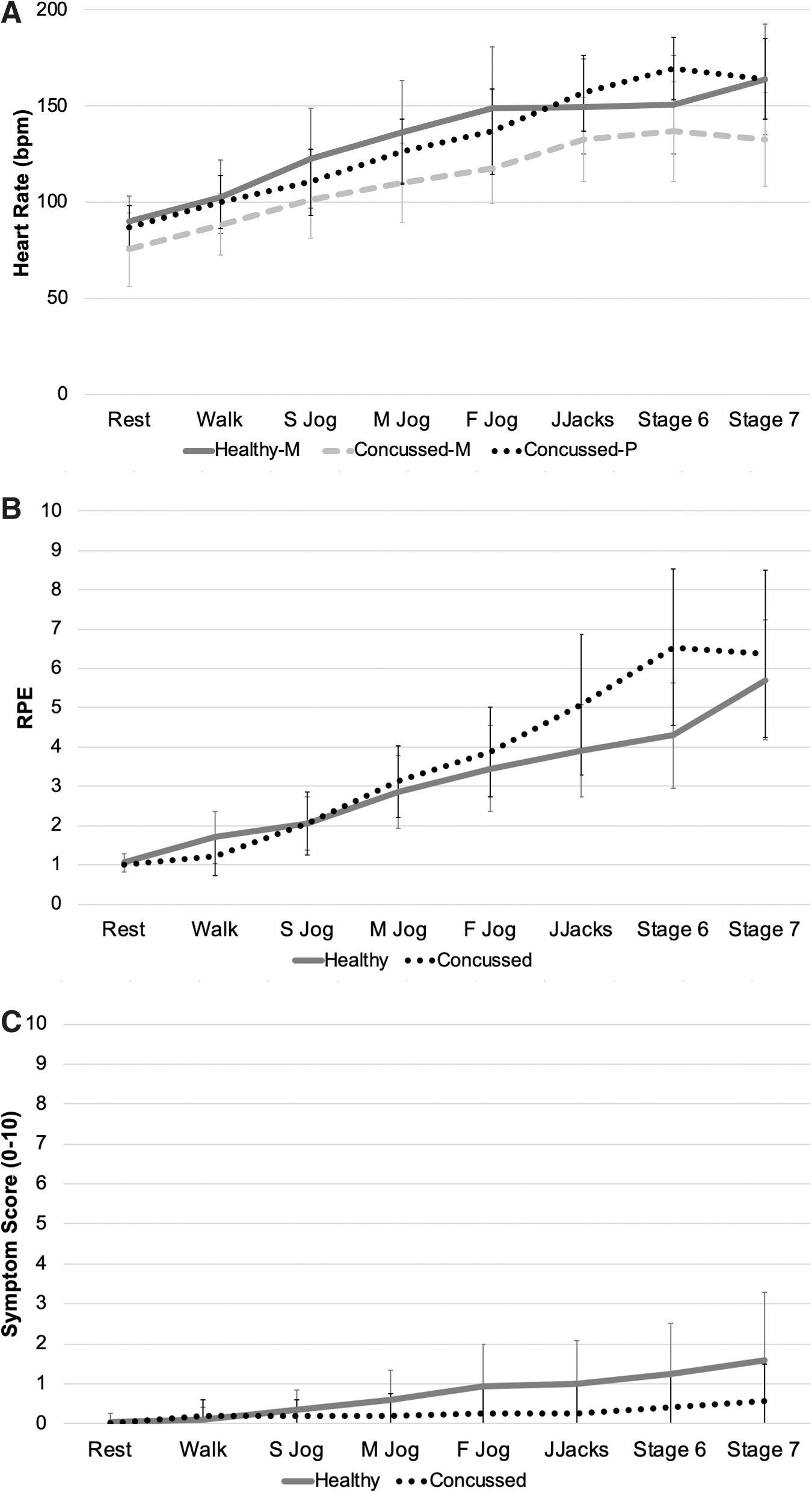
Line graphs depicting heart rate

Results of post hoc testing for heart rate, RP, and global symptom scale ratings throughout the MOVE protocol. Healthy participants are represented by the dark gray boxes in the upper right half of the matrix, whereas concussed participants are represented in the light gray and black striped boxes in the lower left half of the matrix. A filled box represents a statistically significant finding after correcting for multiple comparisons. F Jog, Fast Jog; J Jacks, Jumping Jacks; M, Medium Jog; MOVE,
Feasibility outcomes
The MOVE protocol exceeded all feasibility definitions in healthy youth (Table 2), with observed success rates ≥90% for all outcomes. Heart rate significantly increased throughout the MOVE protocol (F(7,152) = 20.9, p < 0.001, R2 = 0.491; Table 3, Fig. 1), establishing the progressive intensity of the test. In general, heart rate was not significantly different among the final four stages but was significantly higher than that observed during the initial three stages (Fig. 2). Similar findings were observed for perceived exertion, with RPE significantly increasing throughout the MOVE protocol (F(7,152) = 43.7, p < 0.001, R2 = 0.668; Table 3, Fig. 1). Participants reported a significantly higher RPE following the Burpee stage compared with all other exercises (Fig. 2). Additionally, RPEs reported during the initial three exercise stages were significantly lower than those during the remaining exercise stages. Parents (9.4 ± 0.8) and children (9.0 ± 1.0) reported high rates of satisfaction with the MOVE protocol.
Methods for Children With Concussion
Children with concussion presenting for clinical care to the Montréal Children's Hospital Concussion Clinic (MCHCC) between April and June 2021 were consecutively screened for participation. The inclusion/exclusion criteria and informed consent procedures were identical to those for healthy controls, with the exception that participants must additionally be diagnosed with a concussion by a licensed health care provider. This study was approved by the ethics committee of the McGill University Health Centre Pediatrics Board (#2021-7459).
Participants and procedures
The methods used in children with concussion largely paralleled those used in healthy youth. Here, we outline only changes to the study procedures described in healthy children. Thirty children with subacute concussion were randomly assigned to the MOVE (n = 15) or BCTT (n = 15) protocol using a computer-generated sequence with block sizes of six. Participants with subacute concussion were already scheduled to undergo GXT as part of their clinical care and included: 1) children with persisting symptoms (≥ 4 weeks post-injury) completing GXT to help establish an aerobic exercise rehabilitation program (n = 8); or 2) children determined by their treating physiotherapist to be clinically recovered at rest completing GXT as part of a clinic discharge/return-to-sport evaluation (n = 22). This cohort was selected in collaboration with our clinical partners at the MCHCC to first assess the safety and feasibility of our novel GXT in lower-risk groups prior to future implementation in more acute and symptomatic concussion groups.
MOVE protocol
Prior to the initiation of the MOVE protocol in children with subacute concussion, the research team met with our clinical partners at the MCHCC. Clinicians believed the burpee exercise was too demanding for patients experiencing vestibular problems and the movement pattern was too complex for young children generally. The decision was made to remove the Burpee stage and replace it with High Knees exercises (Supplementary Fig. S2). No other changes were made to the MOVE protocol procedures before applying it to participants with subacute concussion.
Participants with subacute concussion completed the MOVE protocol in-person out of an abundance of caution. The participant performed the MOVE protocol in the MCHCC during an already scheduled visit for clinical care. A licensed physiotherapist remained with the patient throughout testing, although they did not participate in the test administration itself. Meanwhile, a research assistant was stationed in a different room within the clinic and administered the MOVE protocol using Zoom Enterprise software. This approach allowed the research team to evaluate the safety and feasibility of the MOVE protocol administered remotely as intended, while enhancing participant safety by ensuring a licensed health care provider was present to monitor the patient and provide medical care if needed.
BCTT protocol
The BCTT was performed according to published guidelines. 3,17 Participants began walking on a treadmill at a set speed and a 0% incline. Every minute, the treadmill incline increased by 1%. Once the maximum treadmill incline of 15% was achieved, speed was increased by 0.4 mph every minute. Outcomes measures were collected every minute during the BCTT. A similar exertion test is already part of standard care at the MCHCC.
Stopping criteria
In addition to the stopping criteria described previously, both the MOVE and BCTT protocols were stopped if a patient reported a ≥3-point increase on the global symptom scale. If no symptom exacerbation or adverse events were reported, the MOVE group completed the full protocol and the BCTT group continued until they reached maximal exertion.
Outcome measures
Safety and feasibility outcomes are identical to those described above in healthy children. However, the PCSI was collected as part of routine care in the MCHCC and participants therefore completed the age-appropriate version. Thus, participants aged 5–7 years completed the 5-item (3-point Guttman scale) version, whereas participants aged 8–12 years completed the 17-item (3-point Guttman scale) version. Adolescents aged ≥13 years completed the same 20-item, 7-point Guttman Scale PCSI version completed by healthy participants. Additionally, manual pulse was unable to be collected during the BCTT; therefore, participants in the BCTT group wore a heart rate monitor (Polar Electro Oy, Kempele, Finland) throughout the protocol. For the MOVE group, heart rate outcomes were collected via manual pulse and heart rate monitor to compare findings with both the BCTT group and healthy MOVE group.
Statistical analysis
Statistical approaches for safety and feasibility outcomes were identical to those described for healthy youth. To compare performance between MOVE and BCTT protocols, independent sample t-tests or Mann-Whitey U tests were conducted using change scores (i.e., scores at protocol termination minus scores at rest prior to protocol initiation) for heart rate, RPE, and global symptom scale ratings. Bland-Altman plots, Pearson's correlation coefficients, and paired sample t-tests were conducted to evaluate systematic bias between manual and monitor-based heart rate outcomes in the MOVE group. Due to the differences in the protocol and injury status of the participants, MOVE protocol findings were not statistically compared between healthy controls and patients with concussion. However, descriptive statistics and data visualizations are presented to highlight similarities across cohorts.
Results for Children With Concussion
Demographic Information
No significant differences were observed between MOVE and BCTT groups for any demographic variables. Compared with healthy youth, participants with subacute concussion less frequently reported French as their primary language (p < 0.001), had higher total symptom scores on the PCSI (p = 0.003), and were more likely to report a prior history of concussion (p = 0.006, Table 1).
Safety outcomes
No adverse events were reported during either the MOVE or BCTT protocol. Three (20%) BCTT and zero (0%) MOVE assessments were stopped early (p = 0.22). BCTT assessments were stopped due to symptom exacerbation (n = 1), inability to maintain necessary walking speed (n = 1), and calf cramps (n = 1). Participants with subacute concussion experienced small but statistically significant increases (χ 2 (7) = 16.7, p = 0.019) in global symptom scale ratings throughout each GXT (Table 3, Fig. 1). Ten (66.7%) participants reported no symptom increases on the global symptom scale, 4 (26.7%) participants reported a 1-point increase, and 1 (6.6%) participant reported a 2-point increase. For the BCTT, 11 (73.3%) participants reported no symptom increase, 2 (13.3%) participants reported a 1-point increase, and 1 (6.7%) participant each reported a 2-point and 3-point increase. Symptom changes did not differ between the MOVE (median = 0 [IQR: 0–1]) and BCTT protocols (median = 0 [IQR: 0–1]; Z = 0.18, p = 0.86; Fig. 3). Only 7 (46.7%) MOVE and 5 (33.3%) BCTT participants completed the 24-h follow-up. PSCI scores generally decreased (MOVE: −5 [IQR: −9, 0]; BCTT: 0 [IQR: −1, 0]) at follow-up, but changes were not statistically significant (p = 0.24) likely due to low statistical power. The proportion of participants reporting activity limiting symptoms did not change for either group (p > 0.70).

Box-and-whisker plots depicting the change (maximum minus minimum values recorded throughout each protocol) for HR
Feasibility outcomes and comparison between GXTs
The MOVE protocol exceeded feasibility definitions (Table 2), with observed success rates >91% for all outcomes. Heart rate significantly increased throughout the MOVE protocol when using manual (F(7,98) = 11.9, p < 0.001, R2 = 0.460) and monitor-based (F(7,110) = 44.1, p < 0.001, R2 = 0.737; Table 3, Fig. 1) measurements, establishing the MOVE protocol as a progressively intense GXT. Post hoc analyses were similar to healthy controls, with heart rates for the final three exercise stages significantly higher than all preceding stages (Fig. 2). Similar patterns were observed for the BCTT (F(19,183) = 9.91, p < 0.001, R2 = 0.507). The change in heart rate throughout the MOVE (82.4 ± 17.9 bpm) and BCTT (72.1 ± 23.0 bpm) protocols were not significantly different (t(28) = 1.36, p = 0.18, Fig. 3). RPE also significantly increased during both the MOVE (F(7,111) = 38.2, p < 0.001, R2 = 0.707; Table 3, Fig. 1) and BCTT protocols (F(19,188) = 4.98, p < 0.001, R2 = 0.335) and the change scores did not differ between groups (MOVE: 5.87 ± 1.92, BCTT: 5.07 ± 2.34, t(28) = 1.02, p = 0.32; Fig. 2). Post hoc analyses were nearly identical to the heart rate outcomes, with the RPE for the final three stages significantly higher than rest, walk in place, Slow Jog, and Medium Jog exercises (Fig. 2). Parents (9.3 ± 1.1) and children (9.2 ± 1.5) reported high rates of satisfaction with the MOVE protocol.
Manual pulse vs. heart rate monitor comparison
Systematic bias was observed between heart rate measurements collected via manual pulse and monitors. Although outcomes were strongly correlated across methods (r = 0.753, p < 0.0001), heart rate measurements captured via monitors were significantly higher than those captured via manual pulse (mean difference: 19.6 bpm [95% confidence interval (CI): 15.4-23.7], t(106) = −9.41, p < 0.001, Fig. 4).
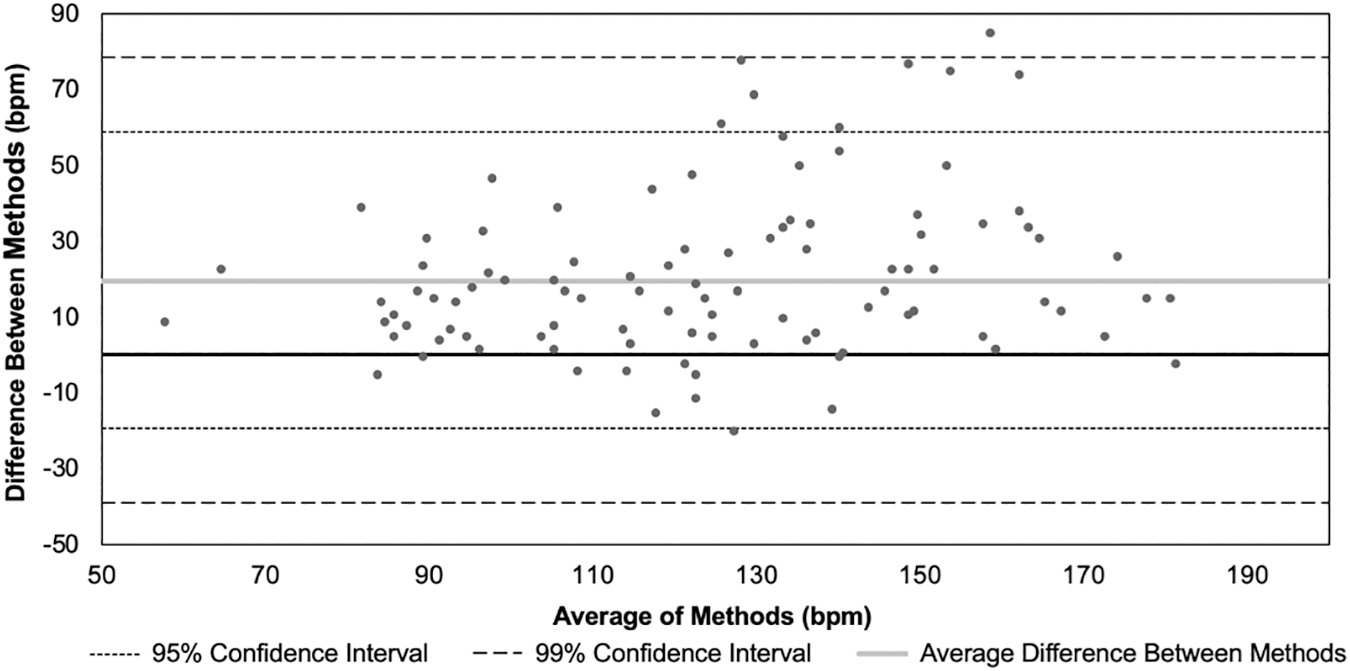
Bland-Altman plot comparing agreement between heart rate measurements gathered via manual pulse and Polar heart rate monitors. Systematic bias was observed, with heart rate monitor values an average of 19.6 bpm (95% CI: 15.4-23.7) higher than manual pulse measurements.
Discussion
The MOVE protocol is a safe and feasible telehealth compatible GXT in healthy youth and youth with subacute concussion. No adverse events occurred throughout the study, all feasibility outcomes were achieved, the protocol was well tolerated and performed similarly to the BCTT, and satisfaction ratings from parents and children were high. Out of abundance of caution for the initial testing of the MOVE protocol, children with subacute concussion were tested in-person at a follow-up clinical visit. A pseudo-virtual administration, whereby the test administrator conducted the MOVE protocol over Zoom from a different room in the clinic, was used to best approximate a telehealth administration while maximizing safety by having licensed health care providers nearby. Children with concussion were either in subacute stages of recovery at the time of testing or were clinically recovered and undergoing GXT as part of a clearance to return-to-sport evaluation. Future studies must assess fully virtual administrations of the MOVE protocol and include acutely concussed participants to further assess the protocol's potential to guide aerobic exercise rehabilitation prescriptions in telehealth contexts.
Beyond eliminating equipment and in-person administration, the MOVE protocol offers several advantages over existing GXTs used in concussion management. The full MOVE protocol consistently takes 14 min to complete, whereas the BCTT is terminated at maximal effort. Our clinical partners (physiotherapists at our local pediatric concussion specialty clinic) noted that the variability in BCTT administration length, taking upwards of 20 min for highly trained athletes, made it difficult to manage appointments, particularly if a patient arrived late or the clinician had consecutive clients. The BCTT is performed at set speeds and inclines, 2 which can be too advanced for sedentary patients, too fast for very small children, or, for the initial stages, too mild for very fit patients. The pace of MOVE protocol exercises can be adjusted to match the fitness and motor proficiency of each patient. However, it was noted that some young children (≤ 8 years of age) struggled to maintain focus during the MOVE protocol, moved out of camera range for brief periods of time, and had difficulty performing the High Knees exercises. Thus, the MOVE protocol provides several benefits compared with traditional GXTs, but also has some limitations, particularly when working with young children remotely.
Half (50%) of the healthy youth reported ≥3-point change in global symptom scale rating throughout the MOVE protocol. Symptom change was not a stopping criterion in healthy participants and our results align with previous literature illustrating that concussion-like symptoms increase immediately following exertion in uninjured individuals. 18 –20 In children with subacute concussion, only one BCTT assessment (and no MOVE assessment) was stopped due to symptom exacerbation using the ≥3-point symptom change cutoff. This finding supports prior work suggesting symptom recurrence happens infrequently (12%) in patients who are symptom free at rest. 21 This may indicate that the psychosocial context of the assessment influences the results—whereby children who have been injured conceptualize exertion, and their phenomenological experience of symptoms (and symptom “increase”), differently than children undergoing the same assessment for non-clinical reasons.
Healthy children reported a median of 1-point on the PSCI prior to the GXT, providing no “anchor” when reporting symptoms throughout testing. Their increased scores likely reflect physical effects of exertion (e.g., fatigue, mild headache), whereas participants with subacute concussion likely considered concussion-specific items when reporting symptoms throughout the GXT. Future studies should consider more specific instructions regarding symptom reporting, particularly in healthy children, to ensure increased symptoms are not due to general by-products of physical activity. Accurately capturing symptom changes is critical to establishing the specificity of the MOVE protocol to detect concussion (separating concussed from non-concussed participants) and exercise intolerance (separating concussed individuals who can and cannot complete vigorous exercise without symptom exacerbation), which can help inform clinical diagnostic and treatment decisions.
Heart rate measurements obtained via manual pulse and monitors did not agree, with monitor-recorded values approximately 20 bpm higher than manual pulse readings. Our cohort primarily included individuals with concussion clinically recovered at rest; thus, this evaluation of the MOVE protocol is more representative of using GXT to determine readiness to return to sport. Precise heart rate measurements are less relevant when using GXT to assist in return-to-play decisions. In this context, the main consideration is (a lack of) symptom recurrence during vigorous intensity exercise. Manual pulse rates or other proxies of exercise intensity such as RPE may remain adequate for this purpose. However, using GXT for post-concussion exercise prescription requires highly accurate heart rate measurements to avoid prescribing exercise therapies above the patient's symptom threshold, which may exacerbate symptoms and delay recovery efforts. 22,23
Manual pulse measurements do not have the precision required for targeted exercise prescription, but eliminating equipment that patients may not have within their home (including heart rate monitors) is important to make the MOVE protocol fully compatible with telehealth approaches. There are other methods for prescribing post-concussion exercise that do not require heart rate monitors and are generally well tolerated in children. 24 This includes approaches based on symptom-limited activities and/or RPE, which is the approach used by the MCHCC, including for symptomatic concussion participants evaluated in this study. Thus, future studies must evaluate the MOVE protocol's potential to guide post-concussion exercise in a fully virtual setting, but the nature of the approach (e.g., targeted heart rate vs. symptom- or RPE-based prescription) may depend on whether a heart rate monitor is accessible to the patient.
Limitations
Heart rate and RPE outcomes for the final two MOVE protocol stages were not significantly greater than the Jumping Jacks (Stage 5) exercise. However, children with concussion had heart rates ∼13 bpm higher during High Knees (Stage 6) exercise compared with Jumping Jacks; thus, despite the lack of statistical significance heart rate continued to increase beyond Stage 5. A similar increase was not seen for the final stage (Quick Steps). Future studies should consider reducing the MOVE protocol to six stages, as this would reduce the testing time while still maintaining an intensely demanding GXT (children were on average at 83.3% of their age-adjusted heart rate maximum at the peak of the MOVE protocol). Burpee exercises were replaced with High Knees exercise to increase the MOVE protocol's feasibility for young children and individuals with vestibular dysfunction. This change was necessitated by the policies and procedures of our clinic partner and was done to maximize patient safety and well-being. Although this change may promote the implementation of the MOVE protocol in acute settings, it limits the comparison between healthy and concussed children and may not be as ecologically valid in a return-to-play context considering the importance of visual-vestibular functioning in sport.
Children and adolescents with concussion underwent exertion testing as part of routine standard of care at the MCHCC. Most participants completed their GXT primarily for clinical discharge purposes and were predominately asymptomatic at the time of testing. Symptomatic participants were tested more than 30 days post-concussion—as such, the results might not generalize to youth tested acutely following injury. All administrations of the MOVE protocol were supervised by licensed physiotherapists or physiotherapy students in their final year of training to ensure the highest degree of participant safety. Although the concussed group was assessed using a virtual platform, they performed the MOVE protocol in-person at our local clinic. A fully virtual administration of the MOVE protocol (i.e., at-home assessment) has only been performed in healthy children at present. Thus, future studies must ensure that the MOVE protocol remains safe and feasible when administered acutely, by other health care providers, and in fully virtual settings. The PCSI outcomes for children with concussion were collected during routine clinical care and different versions were used based on the child's age. This also prevents direct comparisons between healthy and injured participants completing the MOVE protocol.
Clinical implications and future directions
GXT is becoming a cornerstone of clinical concussion management 1 ; assessments such as the MOVE protocol that reduce barriers to GXT implementation can improve clinical care and ensure more patients are receiving best-practice management approaches. The MOVE protocol can be administered and monitored virtually, making a critical concussion management tool compatible with telehealth services and alleviating potential delays in GXT due to circumstances that physically separate injured individuals and their health care providers. Further, the removal of equipment means that the MOVE protocol should be able to be performed almost anywhere, including clinical offices, hallways, hotel rooms during athletic travel, and any playing field, court, or rink. The removal of these barriers can increase the implementation of GXT across diverse clinical settings and expedite enrollment into exercise-based post-concussion treatments, which improves clinical recovery when implemented acutely. 25
Our study primarily evaluated participants who were clinically recovered at rest and undergoing GXT to receive clearance to return to sport; thus, current evidence mostly supports the MOVE protocol for assessing readiness to return to sport in asymptomatic participants. However, GXT can be used in symptomatic participants to guide post-concussion exercise prescription, as was the case for eight participants in our study. Due to differences between manual and monitor-based heart rate measurements, clinicians who wish to provide patients with a personalized heart rate zone to target during post-concussion exercise programs are highly encouraged to use a heart rate monitor. Otherwise, more generalized approaches to prescribing post-concussion exercise such as the RPE can and should be considered. 24 Manual pulse and RPE values are likely sufficient for making return-to-play or discharge decisions, which are more focused on the ability to complete intense physical activity without symptom recurrence as opposed to achieving a precise heart rate value. 1 More studies are needed to examine the safety, tolerability, feasibility, and acceptability of the MOVE protocol in concussed children and adolescents, including fully remote administration (i.e., patients are in their homes) and across different stages in the recovery process (acute, subacute, and persistent) prior to widespread clinical implementation.
Conclusions
The MOVE protocol is a safe and feasible no-equipment GXT that can be administered via telemedicine. No adverse events occurred, all feasibility criteria were met, and high levels of satisfaction were reported for the MOVE protocol. Children with subacute concussion perform similarly (i.e., changes in heart rate, rate of perceived exertion, and symptom outcomes) on the MOVE and BCTT protocols. Future studies in children with concussion must assess the fully virtual administration of the MOVE protocol, MOVE protocol safety and tolerability in children with acute concussion, and whether the MOVE protocol can be used to guide individualized exercise prescription.
Transparency, Rigor, and Reproducibility Summary
This study investigates the safety and feasibility of a novel, telehealth compatible at-home exertion protocol. This study was not formally pre-registered due to the exploratory nature of the project. The analysis plan was not formally pre-registered, but the team member with primary responsibility for the analysis certifies that the protocol submitted for ethics review pre-specified the analysis plan and study definitions of safety and feasibility. A sample size of 30 injured participants was planned based on patient availability. This sample size is in-line with prior research investigating novel exertion protocols in patients with concussion. 4,14 All patients approached agreed to participate in the study. Data collection was performed by investigators who were aware of relevant participant characteristics. The inclusion criteria and primary outcome measures are standard in the post-concussion exercise testing literature. 2,4,14 Correction for multiple comparisons was performed using Bonferroni corrections wherever appropriate. De-identified data and analytic code from this study are not available in a public archive but will be made available upon reasonable request and as allowable according to institutional review board (IRB) standards by e-mailing the corresponding author. The authors agree to provide the full content of the manuscript on request by contacting the corresponding author.
Footnotes
Acknowledgments
The authors sincerely thank Corina Alexandrescu, Émile Asselin, and Pascale Dupont for their efforts related to data collection in healthy participants.
Authors' Contributions
Elizabeth Teel conceptualized and designed the study, obtained ethics approvals, assisted with data collection, analyzed the data, interpreted results, drafted the initial manuscript, and revised the manuscript based on feedback from co-authors. Christophe Alarie conceptualized and designed the study, obtained ethics approvals, assisted with data collection, supervised research assistants, interpreted results, and critically reviewed the manuscript for important intellectual content. Nathan Cook and Grant Iverson assisted with the study design in patients with concussion, interpreted results, and critically reviewed the manuscript for important intellectual content. Bonnie Swain conceptualized and designed the study, supervised research assistants, interpreted results, and critically reviewed the manuscript for important intellectual content. Isabelle Gagnon conceptualized and designed the study, provided access to concussed patients, interpreted results, and critically reviewed the manuscript for important intellectual content.
Funding Information
All information listed in the Author Disclosure Statement are standard disclosures provided by authors about their general funding and conflicts of interest. This funding was used to support the salary of some of the authors working on this article, but again, no funding listed here was used to support the current study.
Author Disclosure Statement
Grant Iverson has a clinical and consulting practice in forensic neuropsychology, including expert testimony, involving individuals who have sustained mild traumatic brain injury (including athletes). He has received research funding from several test publishing companies, including ImPACT Applications, Inc., CNS Vital Signs, and Psychological Assessment Resources (PAR, Inc.). He has received research support from the Harvard Integrated Program to Protect and Improve the Health of NFLPA Members, and grant support from the National Football League. He serves as a scientific advisor for Sway Operations, LLC, Highmark, Inc., and for NanoDX. He acknowledges unrestricted philanthropic support from ImPACT Applications, Inc., the Mooney-Reed Charitable Foundation, the National Rugby League, and the Spaulding Research Institute for concussion research. The donors and funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication. Some authors (ET, NC, GI) were supported, in part, from a grant from the National Football League for a program of research entitled “The Spectrum of Concussion: Predictors of Clinical Recovery, Treatment and Rehabilitation, and Possible Long-Term Effects” (PI Grant Iverson). The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.