
Abstract
The North America Clinical Trials Network (NACTN) for Spinal Cord Injury (SCI) is a consortium of tertiary medical centers that has maintained a prospective SCI registry since 2004, and it has espoused that early surgical intervention is associated with improved outcome. It has previously been shown that initial presentation to a lower acuity center and necessity of transfer to a higher acuity center reduce rates of early surgery. The NACTN database was evaluated to examine the association between interhospital transfer (IHT), early surgery, and outcome, taking into account distance traveled and site of origin for the patient.
Data from a 15-year period of the NACTN SCI Registry were analyzed (years 2005–2019). Patients were stratified into transfers directly from the scene to a Level 1 trauma center (NACTN site) versus IHT from a Level 2 or 3 trauma facility. The main outcome was surgery within 24 hours of injury (yes/no), whereas secondary outcomes were length of stay, death, discharge disposition, and 6-month American Spinal Injury Association Impairment Scale (AIS) grade conversion. For the IHT patients, distance traveled for transfer was calculated by measuring the shortest distance between origin and NACTN hospital. Analysis was performed with Brown-Mood test and chi-square tests. Of 724 patients with transfer data, 295 (40%) underwent IHT and 429 (60%) were admitted directly from the scene of injury. Patients who underwent IHT were more likely to have a less severe SCI (AIS D; p = 0.002), have a central cord injury (p = 0.004), and have a fall as their mechanism of injury (p < 0.0001) than those directly admitted to an NACTN center. Of the 634 patients who had surgery, direct admission to an NACTN site was more likely to result in surgery within 24 hours compared with IHT patients (52% vs. 38%) (p < 0.0003). Median IHT distance was 28 miles (interquartile range [IQR] = 13–62 miles). There was no significant difference in death, length of stay, discharge to a rehab facility versus home, or 6-month AIS grade conversion rates between the two groups. Patients who underwent IHT to an NACTN site were less likely to have surgery within 24 hours of injury, compared with those directly admitted to the Level 1 trauma facility. Although there was no difference in mortality rates, length of stay, or 6-month AIS conversion between groups, patients with IHT were more likely be older with a less severe level of injury (AIS D). This study suggests there are barriers to timely recognition of SCI in the field, appropriate admission to a higher level of care after recognition, and challenges related to the management of individuals with less severe SCI.
Introduction
Traumatic spinal cord injury (SCI) can result in a significant change in functioning, quality of life, and future health for those injured and their family. 1 –4 Traumatic SCI contributes to significant health care system cost and disability burden. 4 –6 Further improving traumatic SCI care would be beneficial both on an individual and public health level. 7
Often, surgical intervention and the subsequent care for traumatic SCI requires resources only available at a higher-level trauma center (i.e., Level 1). Care for patients with SCI at higher-level trauma centers has been shown to be associated with decreased rates of complications and mortality. 8,9 Higher-level trauma centers can offer multi-disciplinary teams, intensive care units, and the ability to diagnose and treat quickly with therapies that may not be available at Level 2 and 3 trauma centers. 8,9
The first 24 hours after a traumatic injury are the most critical time for optimizing patient outcomes, as early surgical intervention is associated with improved outcomes. 9 –11 Clinical practice guidelines currently recommend that patients requiring operative care should be offered surgery within 24 hours of injury, 12 although the 24 hours cutoff is somewhat arbitrary and the benefits of surgery may extend to up to 36 hours. 13 The Surgical Timing in Acute Spinal Injury Study (STASCIS), a multi-institutional retrospective study evaluating 313 patients across six hospital systems, illustrated that of patients who received early surgery (< 24 hours), 20% had neurological recovery of two American Spinal Injury Association Impairment Scale (AIS) grades at 6 months, whereas only 9% of the later surgery group (> 24 hours) improved two AIS grades. 11,14 An additional, recent randomized controlled trial also showed patients with thoracic and lumbar SCI who had surgery earlier (< 24 hours post-injury) had greater improvement post-operatively 1 year after surgery than those who had surgery 24–72 hours post-injury. 15 Guidelines recommend that patients with SCI should be admitted to a high-level trauma center promptly, so they are able to undergo surgical intervention within 24 hours of injury, an epigram coined “Time is spine.” 8,9,12,16,17
Patients arrive at North America Clinical Trials Network (NACTN) Level 1 trauma centers either directly (e.g., by emergency medical service [EMS] from scene of injury) or by first presenting to a Level 2 or 3 trauma center and then undergoing interhospital transfer (IHT). IHT has previously been associated with delays in care, including time to surgery, and poorer patient outcomes. 18 –22 It is not fully understood how IHT and transfer distance impact the rates of early surgery and patient outcomes. Our multi-site North America Clinical Trials Network for Spinal Cord Injury (NACTN) Registry examined the association between IHT, early surgery, and outcomes. Additionally, we also explored how IHT distance impacts patient outcomes.
Methods
The details of the NACTN Registry methodology are described in the companion article in this issue. 23 The registry was queried for patients who were direct admissions to an NACTN center versus IHTs from a lower-level center. Demographics included age, sex, and race. Other data included injury characteristics (mechanism of injury, spinal level of injury, and central cord or conus syndromes), presenting characteristics (blood pressure, mean arterial pressure, Acute Physiology and Chronic Health Evaluation II [APACHE II] score), and comorbities. 24 The APACHE II scoring system estimates predicted intensive care unit (ICU) mortality based on patient characteristics, where a higher score is associated with higher risk of mortality. 24 Baseline AIS grade—from A (complete) to E (normal)—was assessed at baseline and at follow-up. 25 For those who underwent surgery, the evaluation performed before surgery was considered initial (baseline); those without a pre-operative AIS exam were excluded. For those who did not undergo surgery, the AIS grade measured within 7 days was considered initial. Patients who had both initial (i.e., time of injury) and 6-month AIS grade outcomes were included in the subgroup for 6-month outcomes. Central cord syndrome was defined as American Spinal Injury Association Impairment Scale (AIS) C/D cervical injuries with upper extremities weaker than lower extremities (> 10-point difference in AIS motor score), with or without variable sensory and bladder involvement. 26
Outcomes included surgery (yes/no), timing of surgery (
Statistical analysis
Summary statistics were used to present the data. The comparisons between the IHT group and direct transfer group were performed with the Brown-Mood test for continuous variables as they failed the normality test per Kolmogorov-Smirnov test. The chi-square test was used to compare categorical variables. A subset of the IHT group that traveled less than 30 miles from the transfer hospital to the NACTN site was also compared with the direct admittance group. Both 45 and 60 minutes have previously been used as cutoffs for transport time to trauma centers. 28 Our data did not include time, but instead calculated distance. The cutoff of 30 miles was chosen somewhat arbitrarily to look at those who feasibly could have been directly admitted to an NACTN, roughly within 45–60 min of travel time. All tests were two-sided with a significance level of 5%. Statistical analyses were performed in SAS 9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Participant characteristics and transfer status
There were 724 patients included in the study (see Fig. 1). About 40% presented with AIS grade A, and all patients who received surgery had a pre-operative AIS grade reported. About 40% arrived by IHT (n = 295/724) and 60% were directly admitted (n = 429/724). Participant demographics and characteristics stratified by transfer status are presented in Table 1. Female patients were more likely to arrive by IHT than direct admission (p = 0.03), but there was no difference in age between the two groups. Patients with a fall injury were more likely to arrive via IHT (p < 0.0001), whereas patients with a motor vehicle collision injury were more likely to arrive via direct admission (p < 0.0001). Patients with AIS grade D scores were more likely to arrive via IHT (p = 0.002), whereas patients with AIS grade A scores were more likely to be direct admission (p = 0.0009). Patients with lumbar injuries and those with central cord injury were more likely to arrive via IHT than direct admission (p = 0.0008 and p = 0.004, respectively).
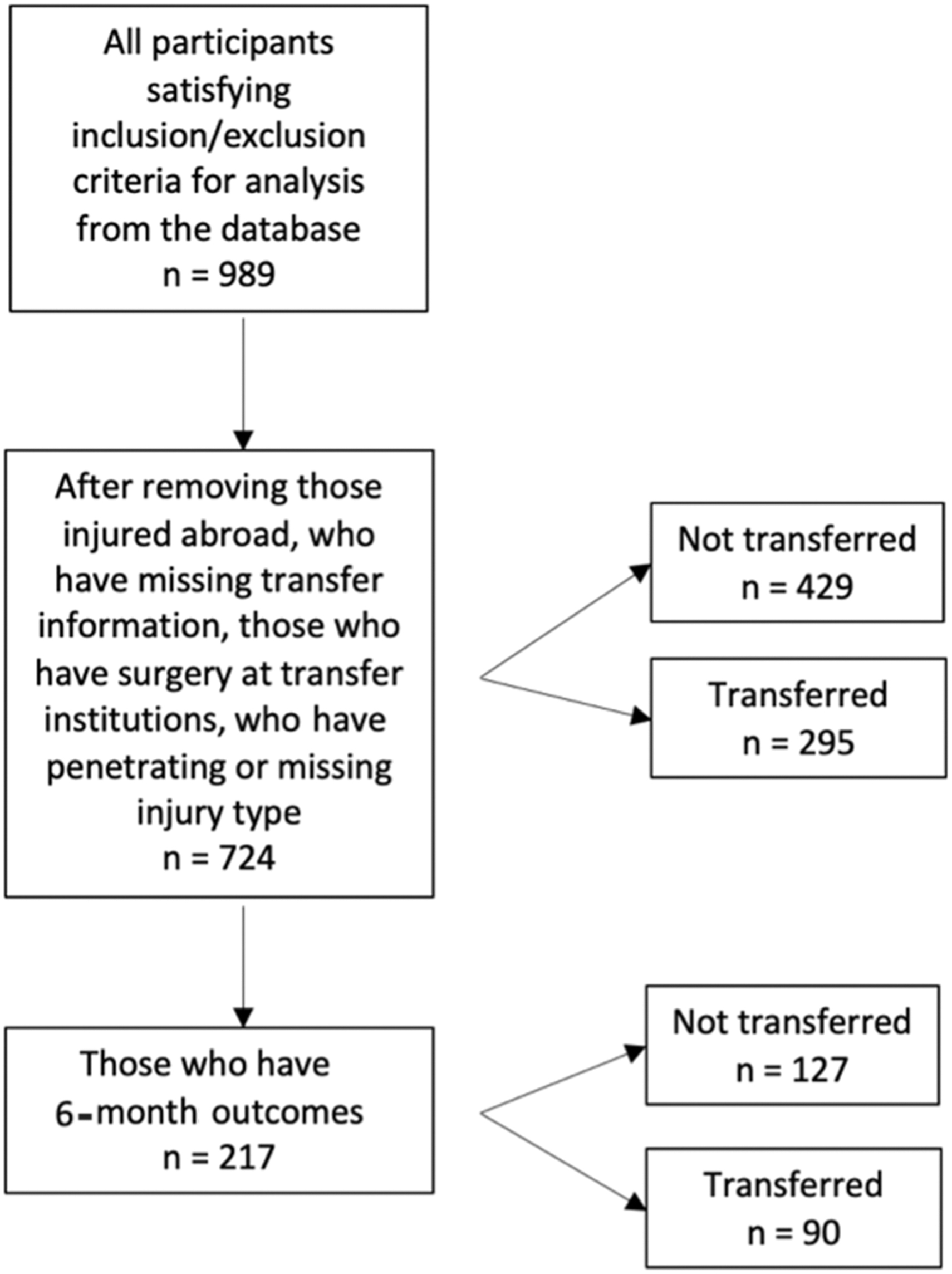
Flowchart showing the data preparation process and the participants included in this study.
Characteristics of the Participants Included in This Study Stratified by Whether They Had IHT
AIS, American Spinal Injury Association Impairment Scale; APACHE-II, Acute Physiology and Chronic Health Evaluation II; BP, blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; MVA, motor vehicle accident; SBP, systolic blood pressure.
Timing of surgery based on transfer status
Patients who arrived by IHT and had surgery were more likely to have surgery more than 24 hours after their injury than those directly admitted to an NACTN center (p = 0.0003, Table 2). Patients who arrived by IHT and had surgery underwent surgery a median of 36 hours post-injury (interquartile range [IQR]: 17–74) and patients who were directly admitted had a median time to surgery of 22 h post-injury (IQR: 11–56); however, this difference was not statistically significant (p = 0.053; Fig. 2).

Timing (in hours) of injury to arrival, arrival to surgery, and injury to surgery of those who arrive via direct admission versus interhospital transfer (IHT).
Surgical Treatment and Timing of Surgery Stratified by Whether Participants Were Transferred or Not
Hospital and patient outcomes analyzed according to transfer status
Patients who arrived by IHT had no difference in length of hospital stay, mortality rates, or discharge disposition compared with direct admission. Patients who were directly admitted had higher rates of cardiac complications, including cardiac arrest, myocardial infarction, shock, chronic heart failure, or dysrhythmias (p = 0.002; Table 3).
Hospitalization Outcomes for Participants Included in This Study Stratified by Whether They Were Transferred or Not
GIGU, gastrointestinal, and genitourinary; LOS, length of stay.
Six-month outcomes
Patients with 6-month outcomes (n = 217/724, 30%) were younger, more likely to identify as a race other than black or white, and less likely to have substance use as a comorbidity, but had similar injury characteristics, clinical status, and AIS grade on presentation (Table 4). There was no significant difference in AIS grade change from the time of injury to 6 months post-injury based on IHT compared with direct admission to an NACTN site. In the IHT group, 49% improved in AIS grade at 6 months compared with the initial score, 48% had no change, and 3% regressed. In the direct admission group, 46% improved their AIS grade at 6 months compared with initial score, 52% had no change, and 2% regressed. Change in AIS grade by transfer group is presented in Figure 3.
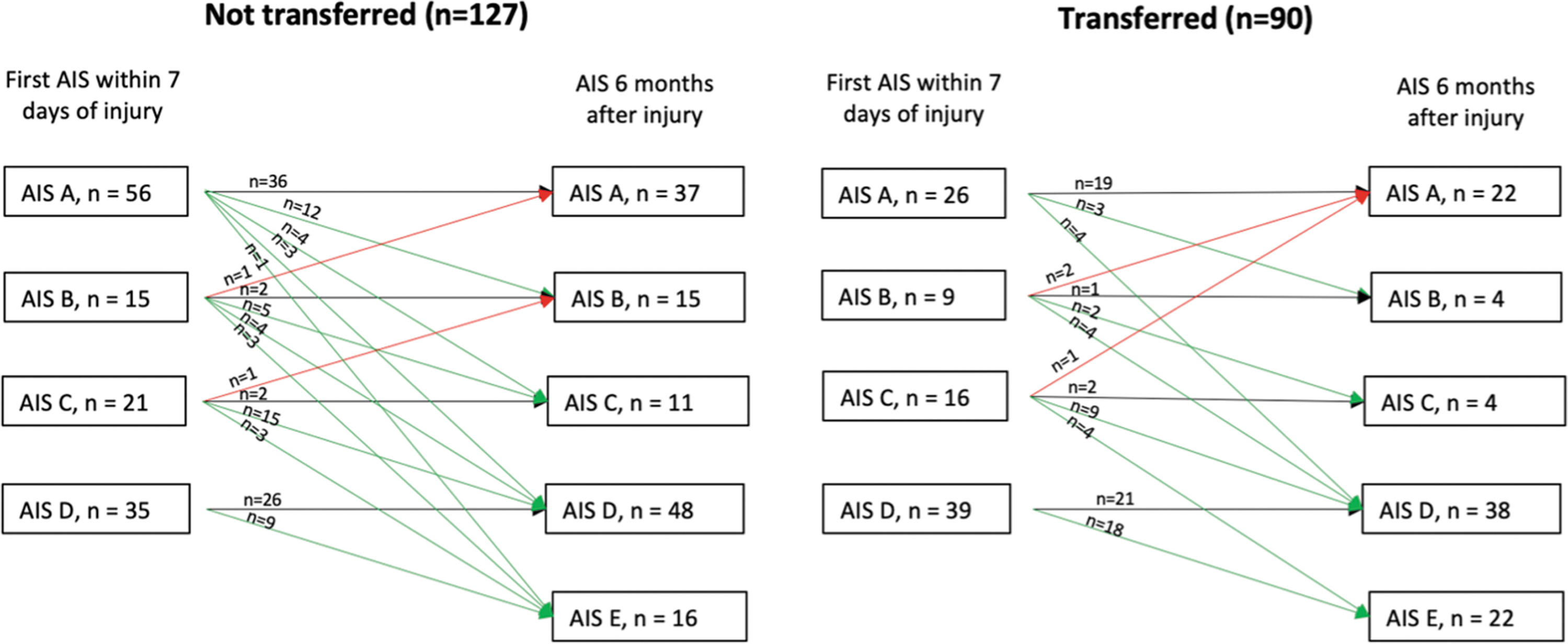
American Spinal Injury Association Impairment (AIS) scale transition from initial AIS grade within 7 days of injury to 6 months.
Clinical and Demographic Comparison of Patients with 6-Month AIS Data Compared With Those Lost to Follow-Up
AIS, American Spinal Injury Association Impairment Scale; APACHE-II, Acute Physiology and Chronic Health Evaluation II; BP, blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; MVA, motor vehicle accident; SBP, systolic blood pressure.
Impact of transfer distance
With respect to the subset of patients who arrived by IHT (n = 295/724), these patients traveled a median of 28 miles (IQR: 13–62) from the transfer site. Those who arrived by IHT at the NACTN hospital more than 24 hours after injury did not differ significantly in distance traveled (median: 25, IQR: 11–54, n = 54) compared with those who arrived by IHT within 24 hours of injury (median: 28, IQR: 13–80, n = 106), p = 0.25.
We also compared the subset of ITH patients who had a transfer distance of less than 30 miles (n = 143) with the direct admissions. Patients who arrived after IHT of less than 30 miles arrived a median of 8 hours after injury (IQR: 5–24), whereas patients who arrived via direct admission arrived a median of 1 hours post-injury (IQR: 1–2, p < 0.0001). Patients who arrived via IHT of less than 30 miles had surgery at a median of 36 hours after their injury (IQR: 17–77), whereas patients directly admitted had surgery a median of 22 hours post-injury (IQR: 11–56), although this difference was not statistically significant (p = 0.12). Patients who were transferred less than 30 miles were less likely to have surgery within 24 hours of injury (n = 47/128, 37%) compared with direct admission (n = 195/372, 52%; p = 0.002). Despite this, both groups had statistically equivalent length of stay, deaths, and discharge disposition after acute hospitalization, and in their 6-month AIS, motor, pinprick, and light touch sensation score change.
Impact of early versus late arrival to NACTN center by IHT
Of the patients who arrived by IHT, 78% (n = 222/286) arrived within 24 hours of injury and 22% (n = 64/286) arrived to the NACTN site more than 24 hours after injury (late IHT). There was no difference in age, sex, or race makeup of these two groups; however, late IHT patients were more likely to have been injured by a fall (p = 0.0009), less likely to be injured by motor vehicle collision (p = 0.004), and less likely to be AIS grade A (p = 0.0074) compared with the transfers arriving within 24 hours of injury.
Those who arrived via IHT within 24 hours had a longer length of stay (median = 14, IQR: 8–25) than late IHT patients (median = 11, IQR: 8–19; p = 0.037) but had similar rates of death and locations of discharge (rehab hospital vs. home). Late IHT patients were more likely to have GIGU complications (p = 0.0003), whereas patients who arrived via IHT within 24 hours had higher rates of pulmonary complications (p < 0.0001).
Discussion
The NACTN SCI multi-site registry examines the association between IHT, IHT distance, early surgery, and outcomes. We found the IHT and direct admit groups had differences in injury severity, such that patients admitted directly had more severe neurological deficits such as a higher percentage of patients with AIS grade A than those arriving by IHT; however, there was no difference in age between the two groups. Patients arriving by IHT were more likely to have surgery more than 24 hours after injury, but the IHT and direct admit groups had similar rates of length of stay, mortality, discharge disposition (home vs. acute rehab), and 6-month outcomes (AIS grade conversion). Importantly, this lack of difference in outcomes could be partially explained by the difference in injury severity between the two groups. The delay in surgery (> 24 hours) for the IHT group was not explained by transfer distance. IHT patients transferred less than 30 miles—who feasibly could have been direct admissions—arrived at NACTN sites a median of 8 hours post-injury compared with direct admits with a median of 1 hour, suggesting direct admission when a Level 1 trauma center is nearby could reduce delays in care.
Previous research has showed improved outcomes following SCI care at trauma centers compared with non-trauma centers, which ideally means patients who need trauma level of care should be transported directly to the nearest, appropriate level trauma center if this can be done in a safe and timely manner. 8,9,29 The 2011 National Guideline for the Field Triage of Injured Patients from the Centers for Disease Control and Prevention classified “paralysis” as an injury pattern that warrants transfer to the highest-level trauma center nearby. 30,31 These guidelines were revised in 2021 and “paralysis” was replaced by “suspected spinal injury with new motor or sensory loss” as one of the criteria prompting transit to the highest-available trauma center nearby. 32 The triage guideline change to motor and sensory loss captures a larger population of people with SCI, presumably to address the under-triage of patients with SCI with moderate levels of dysfunction. With this shift in language comes the challenge of a more complete neurological exam needed in the field by EMS to detect more subtle changes to neurological function. Unfortunately, these guidelines do not indicate specific distances or travel times required to reach a trauma center. Instead, they state that transport should be initiated to the “highest-level trauma center available within the geographic constraints of the regional trauma system.” 32
Our finding that IHT is associated with greater likelihood of delayed surgery (> 24 hours post-injury) compared with direct admissions is consistent with previous research. A recent large study using the National Trauma Data Bank of over 11,000 patients with SCI treated between 2011 and 2014 also found that presentation to a lower acuity center with subsequent necessity of IHT to a Level 1 center reduced the rates of surgery within 24 hours of injury. 18 Other research investigating why some patients with SCI have delayed surgery identified delayed interhospital transfer as one cause. 19
We found that in general IHT patients and direct admit patients had similar acute outcomes including length of stay, death, and discharge disposition, and similar 6-month neurological outcomes. In past limited studies, the findings on the effect of IHT on patient outcomes have been mixed. A study at the University of Utah—a Level 1 trauma center—comparing direct admits with patients arriving by IHT found no difference in length of stay or outcome measures of neurological functioning. 22 Patients who arrived directly were able to ambulate a further distance on the day of discharge compared with those who arrived by IHT. 22 Another study comparing patients arriving by IHT versus direct admit found that the IHT patients had increased length of stay and greater cost of care; however, patients in this study received surgery at the first site before being transferred to the higher level of care site. 20,21 Differences in sampling limit comparisons between these studies and ours. Further, in our study, directly admitted patients were more severely injured.
Previous research has found that nearly one-third of patients with traumatic SCI are under-triaged—meaning brought to a center providing a lower level of care than required for this type of injury. 31 We found that less severely injured patients (AIS grade C) and those injured by falls were disproportionately represented in the IHT group, suggesting these patients are under-triaged in the field. Similar to our findings, those of Selvarajah and colleagues showed that under-triage most likely happens in patients with moderate neurological injuries rather than in those with severe injuries. 33
Although arrival by IHT was associated with greater delay in surgical care, this delay was not explained by distance traveled. Instead, this delay may represent an intervention at outside hospitals, time required to coordinate transfer, regional differences in protocols, and time spent making the decision to recommend surgical planning. 19,34,35 We found that patients who arrived by IHT from a close distance (< 30 miles) unsurprisingly had delays in presentation compared with those who were directly admitted. Given the short distance between lower-level and Level 1 trauma centers, these patients could be transferred directly to Level 1 centers, whereas longer IHT distances may require stabilization and formal evaluation at a lower-level site first.
Our study has several limitations. Our data did not capture the address of where the SCI occurred, limiting our ability to determine distance from injury site to the first hospital in the case of IHT or to the NACTN site. We also did not record the method of transport (e.g., ambulance vs. helicopter/fixed wing), which may have impacted travel time. 36 Our data are also limited to patients presenting to NACTN sites, either by IHT or directly. We cannot draw conclusions about patients with SCI who reached lower-level centers and were not subsequently transferred and may have fared differently. It is also a significant limitation that we were unable to obtain a 12-month or longer final follow-up of neurological outcome in our patients. Recovery from SCI can be delayed in a significant number of patients, so there is the possibility that longer follow-up would have shown greater recovery in the directly transferred earlier decompressed patients. Our high proportion of the sample lost to follow-up limits our ability to generalize findings to all patients with SCI, although this concern is somewhat mitigated by those with 6-month data having similar demographic and clinical characteristics versus those who did not. Finally, there are other outcomes that may have been influenced by IHT but were not captured in the NACTN database, such as the cost differences between direct admission and IHT. These areas represent topics for further investigation.
Conclusions
We found that IHT is associated with a lower chance of surgical intervention within 24 hours following SCI—a time goal that has been established as key for intervention to promote the best outcomes in patients with SCI with persisting compression of the spinal cord. Appropriate triaging can help minimize delays in care and IHT. Patients with less severe neurological injuries but who require a higher level of care represent a group that could benefit from improved recognition in the field of avoiding IHT, particularly when a trauma center is close by. The traumatic SCI field may benefit from similar models of specialized emergency care such as stroke—where patients are brought to dedicated “stroke centers” for timely management. This study contributes to the goal of appropriately triaging patients with SCI so that they receive the level of care they need such as the opportunity to receive surgery within 24 hours of injury.
Footnotes
Transparency,Rigor,and Reproducibility Summary
This is a secondary analysis of a prospective study, North American Clinical Trials Network (NACTN), which was pre-registered at clinical ![]() schematizes the flow of cohort extraction. Data was de-identified. Statistical analyses were performed in SAS 9.4 (SAS Inc, Cary, NC). All the assumptions of tests and models were evaluated, and appropriate statistical methods were used, detailed in the methodology section. Data from this study is not available publicly at the moment because the original study is still ongoing. Analytical codes used in this study are not available to the public because they are commonly known methods.
schematizes the flow of cohort extraction. Data was de-identified. Statistical analyses were performed in SAS 9.4 (SAS Inc, Cary, NC). All the assumptions of tests and models were evaluated, and appropriate statistical methods were used, detailed in the methodology section. Data from this study is not available publicly at the moment because the original study is still ongoing. Analytical codes used in this study are not available to the public because they are commonly known methods.
Authors' Contributions
Margot Kelly-Hedrick: writing—original draft, conceptualization; Beatrice Ugiliweneza: formal analysis, writing—review and editing; Elizabeth G. Toups: writing—review and editing, resources, project administration; George Jimsheleishvili: writing—review and editing, project administration; Shekar N. Kurpad: writing—review and editing; Bizhan Aarabi: writing—review and editing, resources; James S. Harrop: writing—review and editing, resources; Norah Foster: writing—review and editing; Rory C. Goodwin: resources; Christopher I. Shaffrey: resources; Michael G. Fehlings: writing—review and editing, resources; Charles H. Tator: writing—review and editing; James D. Guest: writing—review and editing, resources; Chris J. Neal: writing—review and editing, resources; Muhammad M. Abd-El-Barr: writing—review and editing, conceptualization; Theresa Williamson: writing—review and editing, conceptualization.
Disclaimer
The views expressed in this article are those of the author(s) and do not necessarily reflect the official policy of the Department of Defense of the U.S. government.
Funding Information
This material is based upon work supported by the U.S. Army Medical Research Acquisition Activity under grant nos. W81XWH-07-1-0361, W81XWH-10-2-0042, and W81XWH-13-2-0040, contract no. W81XWH-16-C-0031; and the Christopher & Dana Reeve Foundation.
Author Disclosure Statement
No competing financial interests exist.